
Predict Treatment Response by Magnetic Resonance Diffusion Weighted Imaging: A Preliminary Study on 46 Meningiomas Treated with Proton-Therapy

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. MR Imaging Techniques
2.3. Imaging Analysis
2.4. Statistical Analysis
3. Results
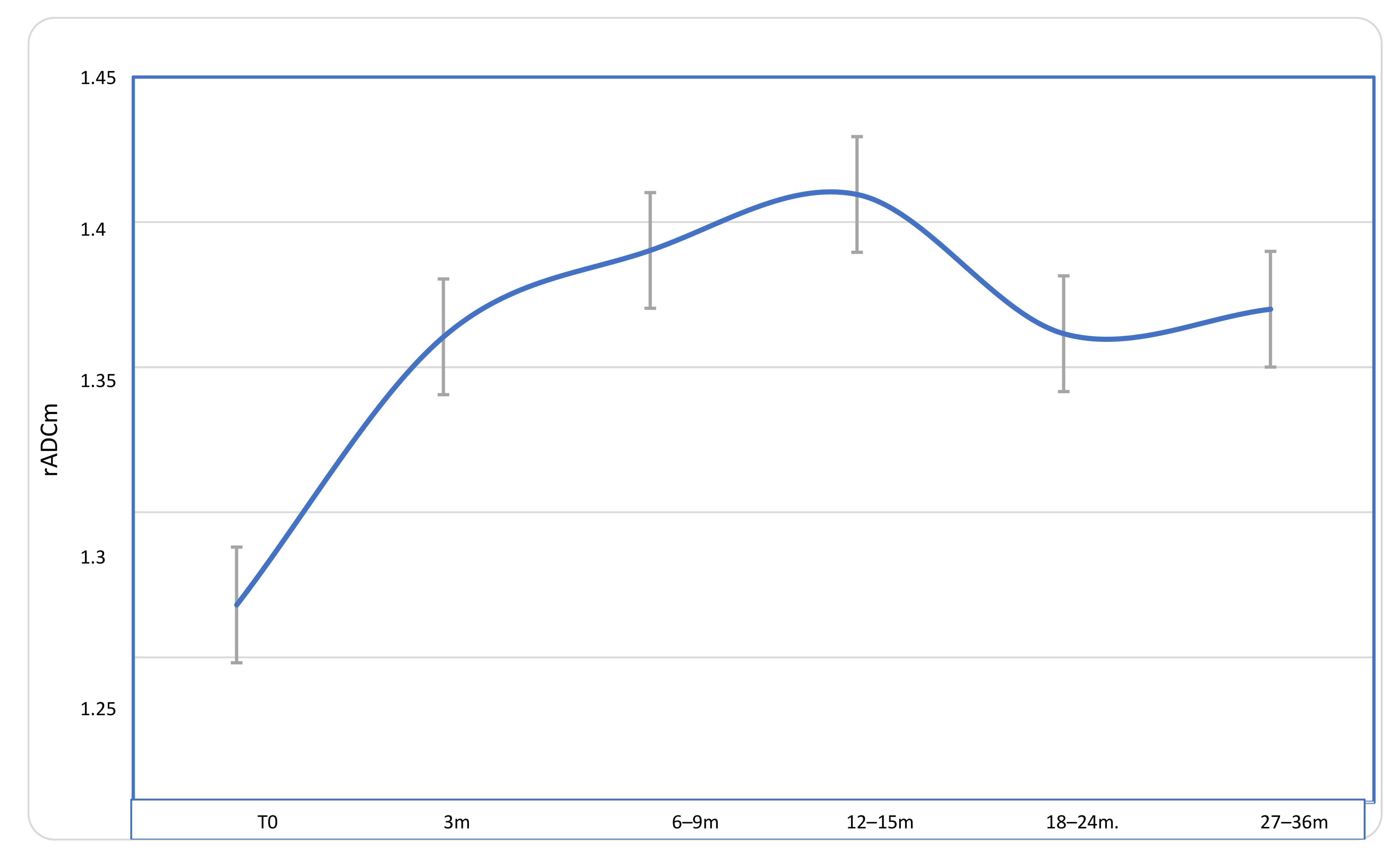
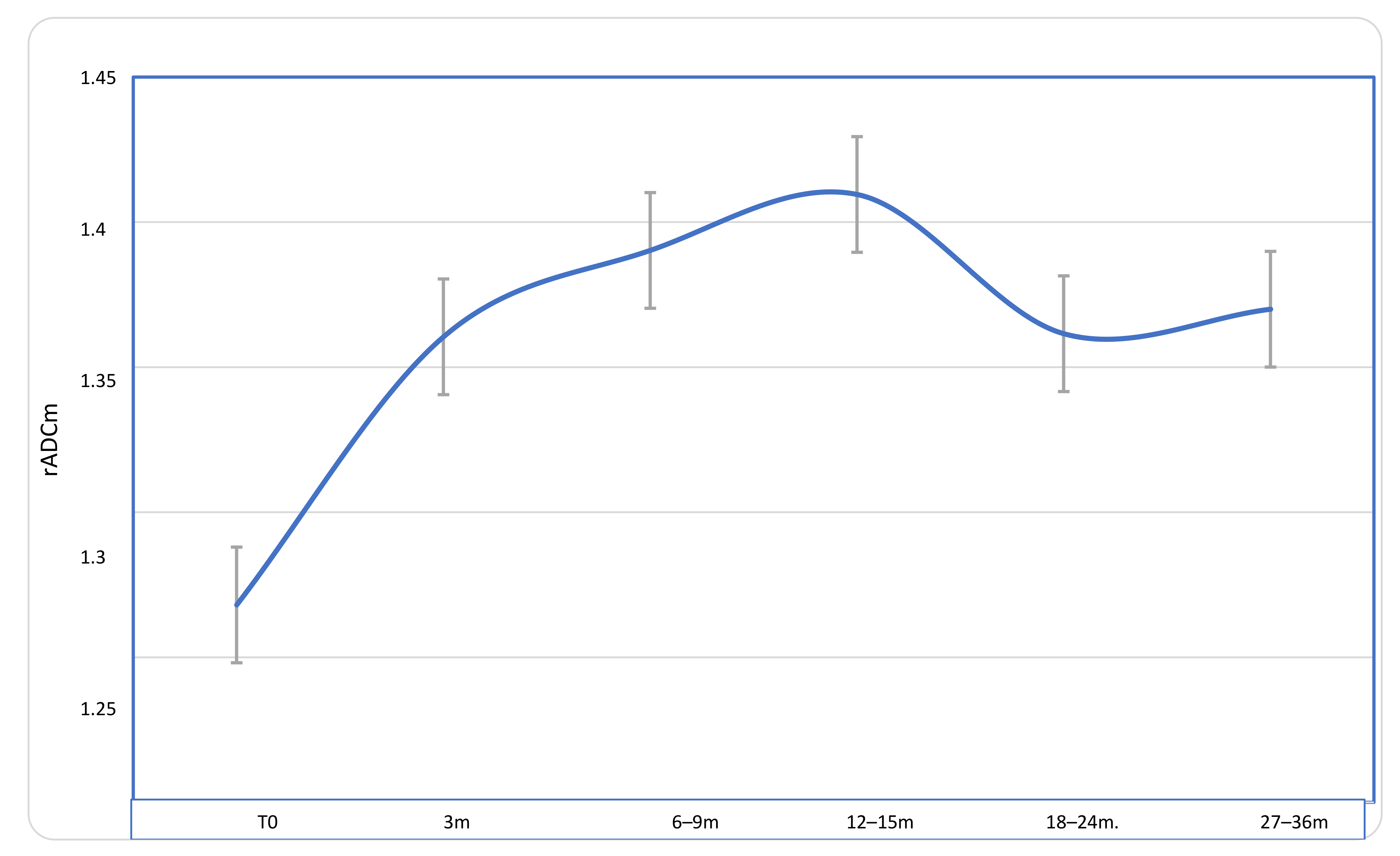
3.1. ADC Longitudinal Changes
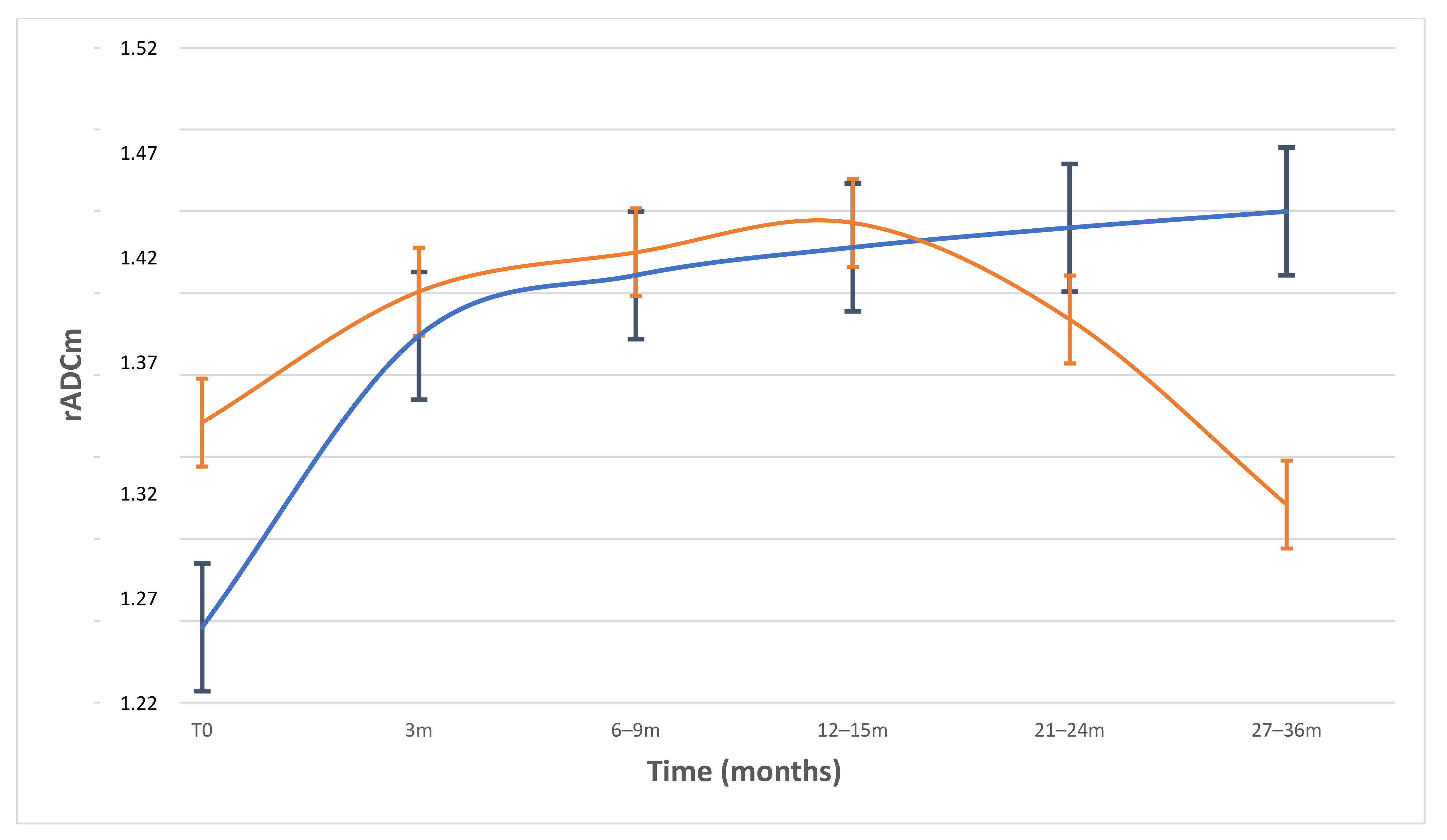
3.2. Comparison of rADCm Values among Patients Grouped by Different Volume Changes
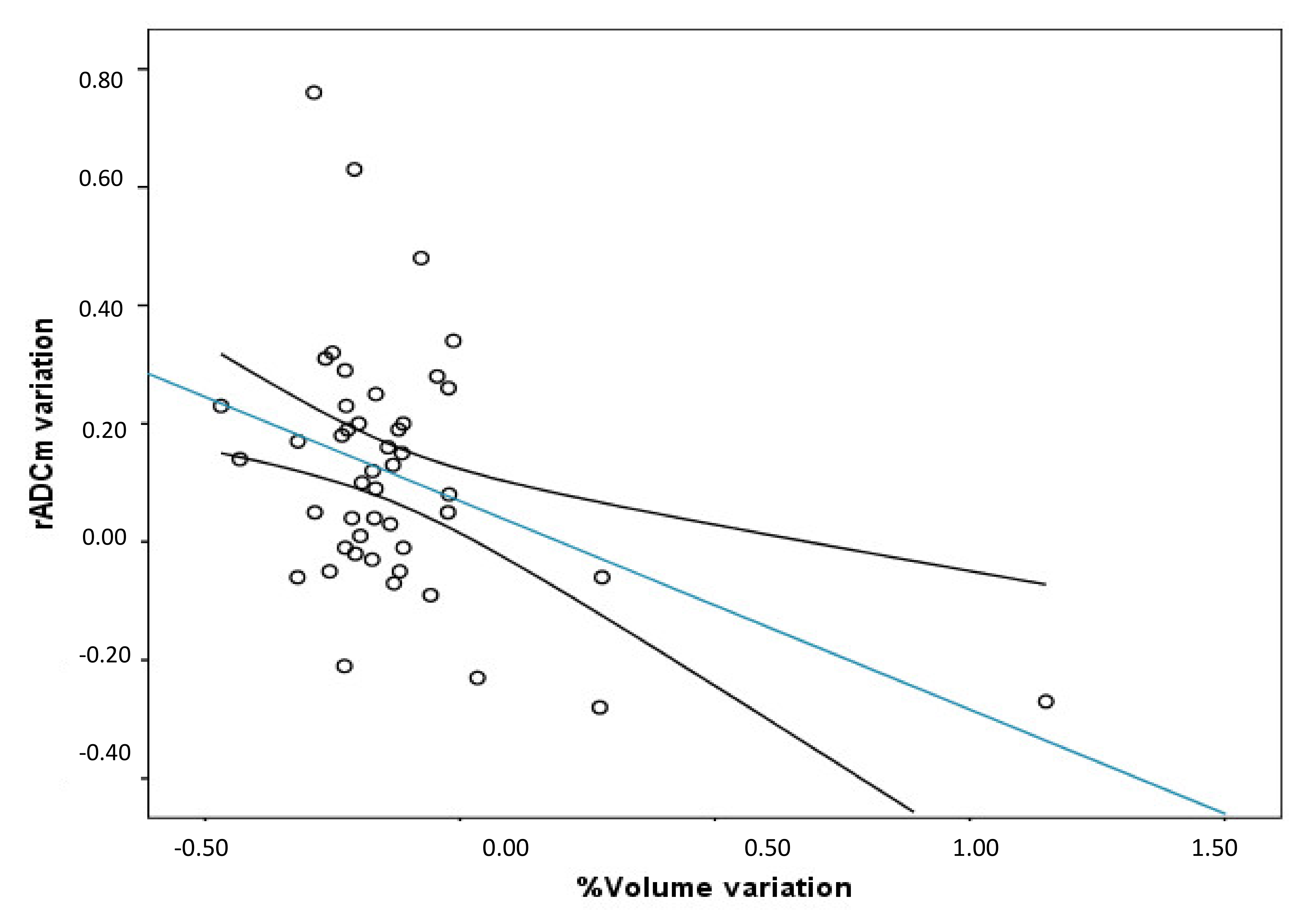
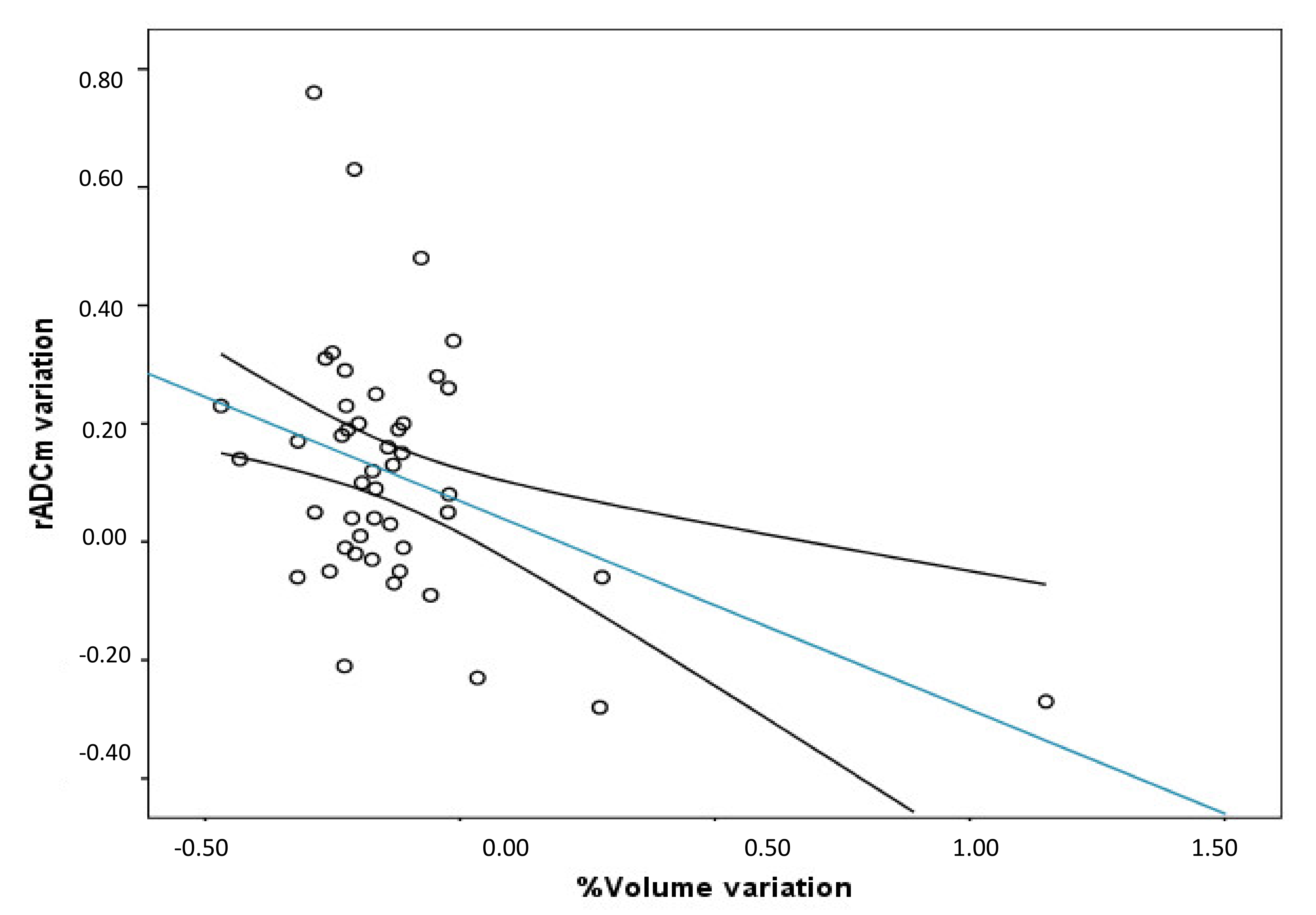
3.3. Correlations among rADCm Values, VV and Therapeutic Dose
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ogasawara, C.; Philbrick, B.D.; Adamson, D.C. Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future Directions. Biomedicines 2021, 9, 319. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Amichetti, M.; Enrici, R.M. Radiotherapy and radiosurgery for benign skull base meningiomas. Radiat. Oncol. 2009, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Brastianos, P.K.; Galanis, E.; Butowski, N.; Chan, J.W.; Dunn, I.F.; Goldbrunner, R.; Mende-Herold, C.; Ippen, M.F.; Mawrin, C.; WcDermott, M.W.; et al. Advances in multidisciplinary therapy for meningiomas. Neuro-Oncology 2019, 21, i18–i31. [Google Scholar] [CrossRef] [Green Version]
- McDonald, M.W.; Plankenhorn, D.A.; McMullen, K.P.; Henderson, M.A.; Dropcho, E.J.; Shah, M.V.; Cohen-Gadol, A.A. Proton therapy for atypical meningiomas. J. Neurooncol. 2015, 123, 123–128. [Google Scholar] [CrossRef] [Green Version]
- LaRiviere, M.J.; Santos, P.M.G.; Hill-Kayser, C.E.; Metz, J.M. Proton Therapy. Hematol. Oncol. Clin. N. Am. 2019. [Google Scholar] [CrossRef]
- Huang, R.Y.; Bi, W.L.; Weller, M.; Kaley, T.; Blakeley, J.; Dunn, I.; Galanis, E.; Preusser, M.; McDermott, M.; Rogers, L.; et al. Proposed response assessment and endpoints for meningioma clinical trials: Report from the Response Assessment in Neuro-Oncology Working Group. Neuro-Oncology 2019, 21, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glenn, C.A.; Tullos, H.J.; Sughrue, M.E. Natural history of intracranial meningiomas. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Campbell, A.; Davis, L.M.; Wilkinson, S.K.; Hesketh, R.L. Emerging Functional Imaging Biomarkers of Tumour Responses to Radiotherapy. Cancers 2019, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Camargo, A.; Schneider, T.; Liu, L.; Pakpoor, J.; Kleinberg, L.; Yousem, D.M. Pretreatment ADC Values Predict Response to Radiosurgery in Vestibular Schwannomas. AJNR Am. J. Neuroradiol. 2017, 38, 1200–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padhani, A.R.; Koh, D.M. Diffusion MR imaging for monitoring of treatment response. Magn. Reason. Imaging Clin. N. Am. 2011, 19, 181–209. [Google Scholar] [CrossRef]
- Franconeri, A.; Sacco, S.; Raciti, M.V.; Maggi, A.; Muzic, S.I.; Imparato, S.; Farina, L.; Bacila, A.; Paganelli, C.; Buizza, G.; et al. Intravoxel incoherent motion as a tool to detect early microstructural changes in meningiomas treated with proton therapy. Neuroradiology 2021, 1–8. [Google Scholar] [CrossRef]
- Foti, P.V.; Longo, A.; Reibaldi, M.; Russo, A.; Privitera, G.; Spatola, C.; Raffaele, L.; Salamone, V.; Farina, R.; Palmucci, S.; et al. Uveal melanoma: Quantitative evaluation of diffusion-weighted MR imaging in the response assessment after proton-beam therapy long-term follow-up. Radiol. Med. 2015, 122, 131–139. [Google Scholar] [CrossRef]
- Wolf, M.B.; Edler, C.; Tichy, D.; Röthke, M.C.; Schlemmer, H.P.; Herfarth, K.; Bonekamp, D. Diffusion-weighted MRI treatment monitoring of primary hypofractionated proton and carbon ion prostate cancer irradiation using raster scan technique. J. Magn. Reson. Imaging 2017, 46, 850–860. [Google Scholar] [CrossRef]
- Hou, P.; Zhu, K.H.; Park, P.C.; Li, H.; Mahajan, A.; Grosshans, D.R. Proton Therapy for Juvenile Pilocytic Astrocytoma: Quantifying Treatment Responses by Magnetic Resonance Diffusion Tensor Imaging. Int. J. Part. Ther. 2017, 3, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afaq, A.; Andreou, A.; Koh, D.M. Diffusion-weighted magnetic resonance imaging for tumour response assessment: Why, when and how? Cancer Imaging 2010, 10, S179. [Google Scholar] [CrossRef]
- Papaevangelou, E.; Almeida, G.S.; Jamin, Y.; Robinson, S.P.; deSouza, N.M. Diffusion-weighted MRI for imaging cell death after cytotoxic or apoptosis-inducing therapy. Br. J. Cancer 2015, 112, 1471–1479. [Google Scholar] [CrossRef] [PubMed]
- Dzik-Jurasz, A.; Domenig, C.; George, M.; Wolber, J.; Padhani, A.; Brown, G.; Doran, D. Diffusion MRI for prediction of response of rectal cancer to chemoradiation. Lancet 2002, 360, 307–308. [Google Scholar] [CrossRef]
- Sun, Y.S.; Zhang, X.P.; Tang, L.; Ji, J.F.; Gu, J.; Cai, Y.; Zhang, X.Y. Locally advanced rectal carcinoma treated with preoperative chemotherapy and radiation therapy: Preliminary analysis of diffusion-weighted MR imaging for early detection of tumor histopathologic downstaging. Radiology 2010, 254, 170–178. [Google Scholar] [CrossRef]
- Oh, J.; Henry, R.G.; Pirzkall, A.; Lu, Y.; Li, X.; Catalaa, I.; Chang, S.; Dillon, W.P.; Nelson, S.J. Survival analysis in patients with glioblastoma multiforme: Predictive value of choline-to-N-acetylaspartate index, apparent diffusion coefficient, and relative cerebral blood volume. J. Magn. Reson. Imaging 2004, 19, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Zhang, X.P.; Sun, Y.S.; Tang, L.; Shen, L. Apparent diffusion coefficient: Potential imaging biomarker for prediction and early detection of response to chemotherapy in hepatic metastases. Radiology 2008, 248, 894–900. [Google Scholar] [CrossRef]
- Koh, D.M.; Scurr, E.; Collins, D.; Kanber, B.; Norman, A.; Leach, M.O.; Husband, J.E. Predicting response of colorectal hepatic metastasis: Value of pretreatment apparent diffusion coefficients. AJR Am. J. Roentgenol. 2007, 188, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bai, R.; Sun, H.; Liu, H.; Zhao, X.; Li, Y. Diffusion-weighted imaging in predicting and monitoring the response of uterine cervical cancer to combined chemoradiation. Clin. Radiol. 2009, 64, 1067–1074. [Google Scholar] [CrossRef]
- McMahon, S.J. Proton RBE models: Commonalities and differences. Phys. Med. Biol. 2021, 66, 04NT02. [Google Scholar] [CrossRef]
- Tommasino, F.; Durante, M. Proton Radiobiology. Cancers 2015, 7, 353. [Google Scholar] [CrossRef] [PubMed]
- Pinzi, V.; Bisogno, I.; Ciusani, E.; Canazza, A.; Calatozzolo, C.; Vetrano, I.G.; Pasi, F.; de Martin, E.; Fumagalli, M.L.; Nano, R.; et al. In vitro assessment of radiobiology of meningioma: A pilot study. J. Neurosci. Methods 2019, 311, 288–294. [Google Scholar] [CrossRef]
- Sanverdi, S.E.; Ozgen, B.; Oguz, K.K.; Mut, M.; Dolgun, A.; Soylemezoglu, F.; Cila, A. Is diffusion-weighted imaging useful in grading and differentiating histopathological subtypes of meningiomas? Eur. J. Radiol. 2012, 81, 2389–2395. [Google Scholar] [CrossRef]
- Hakyemez, B.; Yildirim, N.; Gokalp, G.; Erdogan, C.; Parlak, M. The contribution of diffusion-weighted MR imaging to distinguishing typical from atypical meningiomas. Neuroradiology 2006. [Google Scholar] [CrossRef]
- Yamasaki, F.; Kurisu, K.; Satoh, K.; Arita, K.; Sugiyama, K.; Ohtaki, M.; Takaba, J.; Tominaga, A.; Hanawa, R.; Yoshioka, H.; et al. Apparent diffusion coefficient of human brain tumors at MR imaging. Radiology 2005, 235, 985–991. [Google Scholar] [CrossRef]
- Surov, A.; Meyer, H.J.; Wienke, A. Correlation between apparent diffusion coefficient (ADC) and cellularity is different in several tumors: A meta-analysis. Oncotarget 2017, 8, 59492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surov, A.; Hamerla, G.; Meyer, H.J.; Winter, K.; Schob, S.; Fiedler, E. Whole lesion histogram analysis of meningiomas derived from ADC values. Correlation with several cellularity parameters, proliferation index KI 67, nucleic content, and membrane permeability. Magn. Reson. Imaging 2018, 51, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Thoeny, H.C.; Ross, B.D. Predicting and monitoring cancer treatment response with diffusion-weighted MRI. J. Magn. Reson. Imaging 2010, 32, 2–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawashima, M.; Suzuki, S.O.; Ikezaki, K.; Matsushima, T.; Fukui, M.; Iwaki, T. Different responses of benign and atypical meningiomas to gamma-knife radiosurgery: Report of two cases with immunohistochemical analysis. Brain Tumor Pathol. 2001, 18, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Swartz, J.E.; Pothen, A.J.; Stegeman, I.; Willems, S.M.; Grolman, W. Clinical implications of hypoxia biomarker expression in head and neck squamous cell carcinoma: A systematic review. Cancer Med. 2015, 4, 1101–1116. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.C.; Yang, S.C.; Chen, Y.F.; Tseng, H.M.; My, P.C. Simultaneous assessment of cerebral blood volume and diffusion heterogeneity using hybrid IVIM and DK MR imaging: Initial experience with brain tumors. Eur. Radiol. 2017, 27, 306–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients/MN | 44/46 | |
| Mean age ± SD | 65 ± 13.2 | |
| Sex (%) | M | 13 (29.5 %) |
| F | 33 (70.5 %) | |
| MN type (%) | 26 WHO I; 13 WHO II; 1 WHO III; | |
| MN Location | Convexity | 13 |
| Skull base: | ||
| Cavernous sinus | 13 | |
| other (petroclival, sphenoid) | 20 | |
| T0 | 3 m | 6–9 m | 12–15 m | 21–24 m | 27–36 m | |
|---|---|---|---|---|---|---|
| rADC mean ± SD | 1.268 ± 0.245 | 1.360 ± 0.214 | 1.390 ± 0.224 | 1.409 ± 0.239 | 1.364 ± 0.251 | 1.378 ± 0.283 |
| Groups | n | % | % of Volume Variation from Baseline to Last Follow-Up Exam (mean ± SD) | Pretreatment rADCm Values | % of rADCm Increase at 3 Months |
|---|---|---|---|---|---|
| Overall population | 46 | 100 | −12.54 ± 23.45 | 1.26 ± 0.24 | 8 |
| Group-1 | 18 | 39,2 | −26.3 ± 7.7 | 1.16 ± 0.20 | 16.3 |
| Group-2 | 28 | 61.8 | −3.65 ± 25.2 | 1.29 ± 0.23 | 6.1 |
| p-value (Group 1–2) | 0.0018 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feraco, P.; Scartoni, D.; Porretti, G.; Pertile, R.; Donner, D.; Picori, L.; Amelio, D. Predict Treatment Response by Magnetic Resonance Diffusion Weighted Imaging: A Preliminary Study on 46 Meningiomas Treated with Proton-Therapy. Diagnostics 2021, 11, 1684. https://doi.org/10.3390/diagnostics11091684
Feraco P, Scartoni D, Porretti G, Pertile R, Donner D, Picori L, Amelio D. Predict Treatment Response by Magnetic Resonance Diffusion Weighted Imaging: A Preliminary Study on 46 Meningiomas Treated with Proton-Therapy. Diagnostics. 2021; 11(9):1684. https://doi.org/10.3390/diagnostics11091684
Chicago/Turabian StyleFeraco, Paola, Daniele Scartoni, Giulia Porretti, Riccardo Pertile, Davide Donner, Lorena Picori, and Dante Amelio. 2021. "Predict Treatment Response by Magnetic Resonance Diffusion Weighted Imaging: A Preliminary Study on 46 Meningiomas Treated with Proton-Therapy" Diagnostics 11, no. 9: 1684. https://doi.org/10.3390/diagnostics11091684
APA StyleFeraco, P., Scartoni, D., Porretti, G., Pertile, R., Donner, D., Picori, L., & Amelio, D. (2021). Predict Treatment Response by Magnetic Resonance Diffusion Weighted Imaging: A Preliminary Study on 46 Meningiomas Treated with Proton-Therapy. Diagnostics, 11(9), 1684. https://doi.org/10.3390/diagnostics11091684