
High Inter-Rater Reliability of Manual Segmentation and Volume-Based Tractography in Healthy and Dystrophic Human Calf Muscle

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
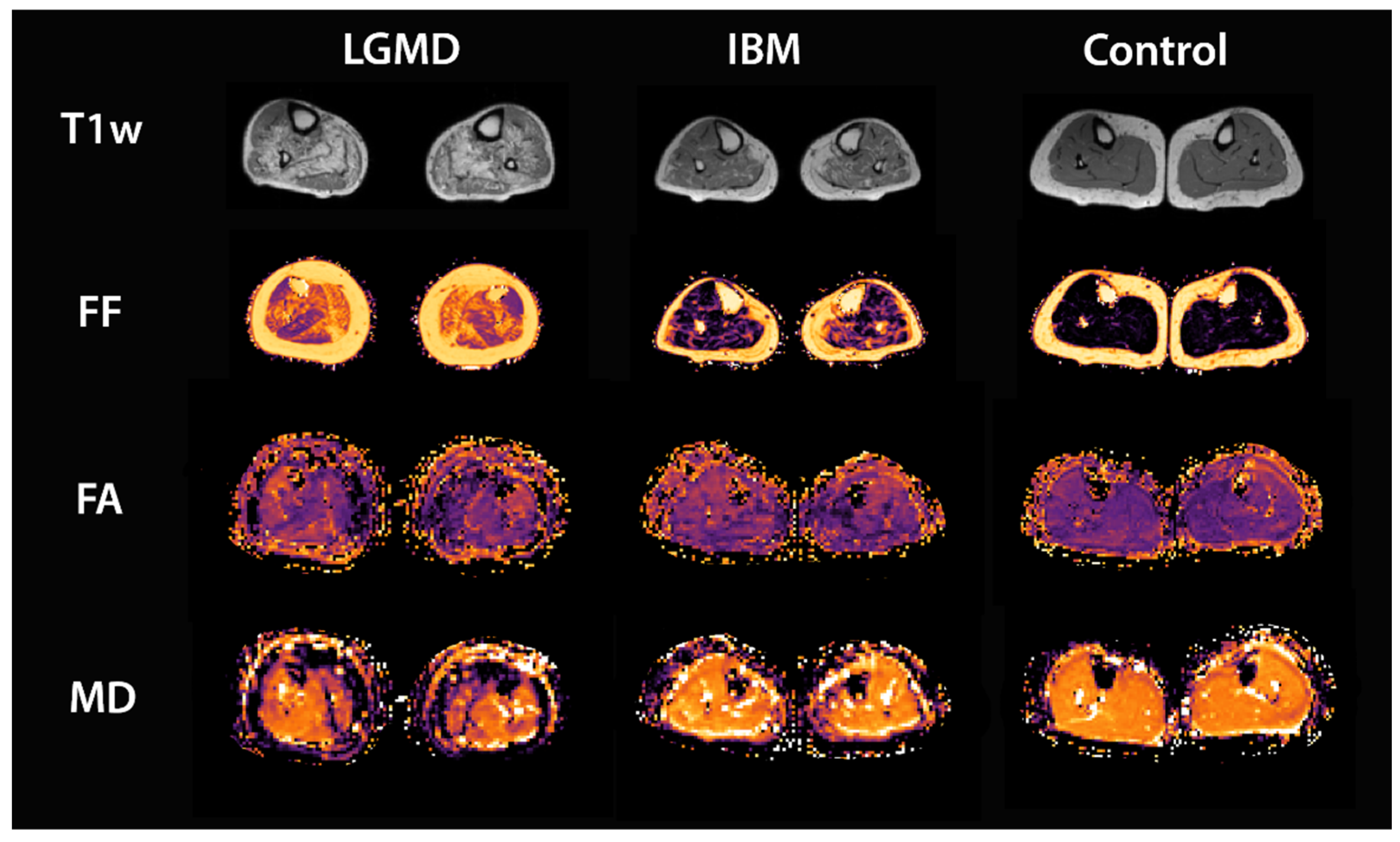
2.1. Study Population
2.2. Data Acquisition
2.3. Data Processing
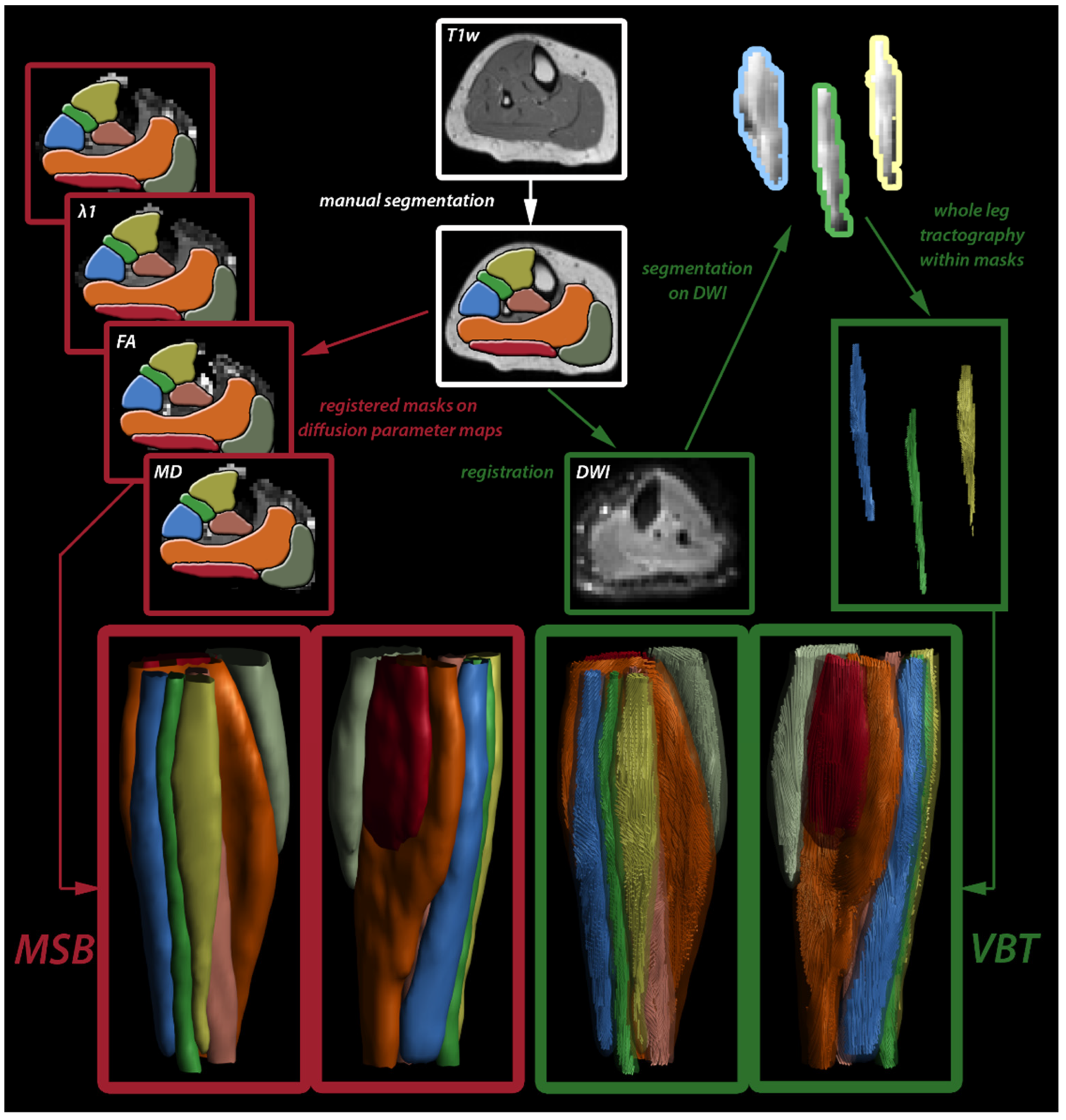
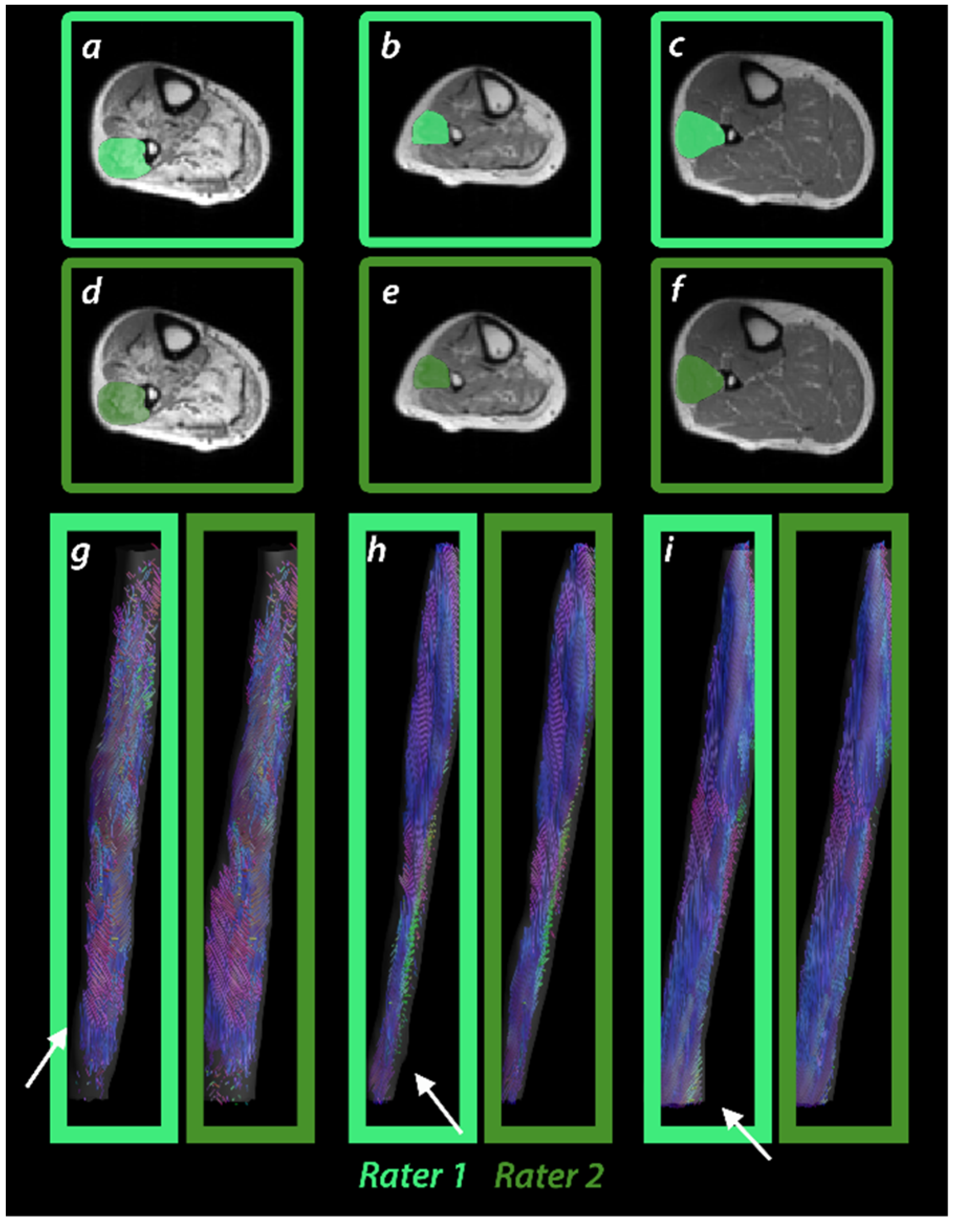
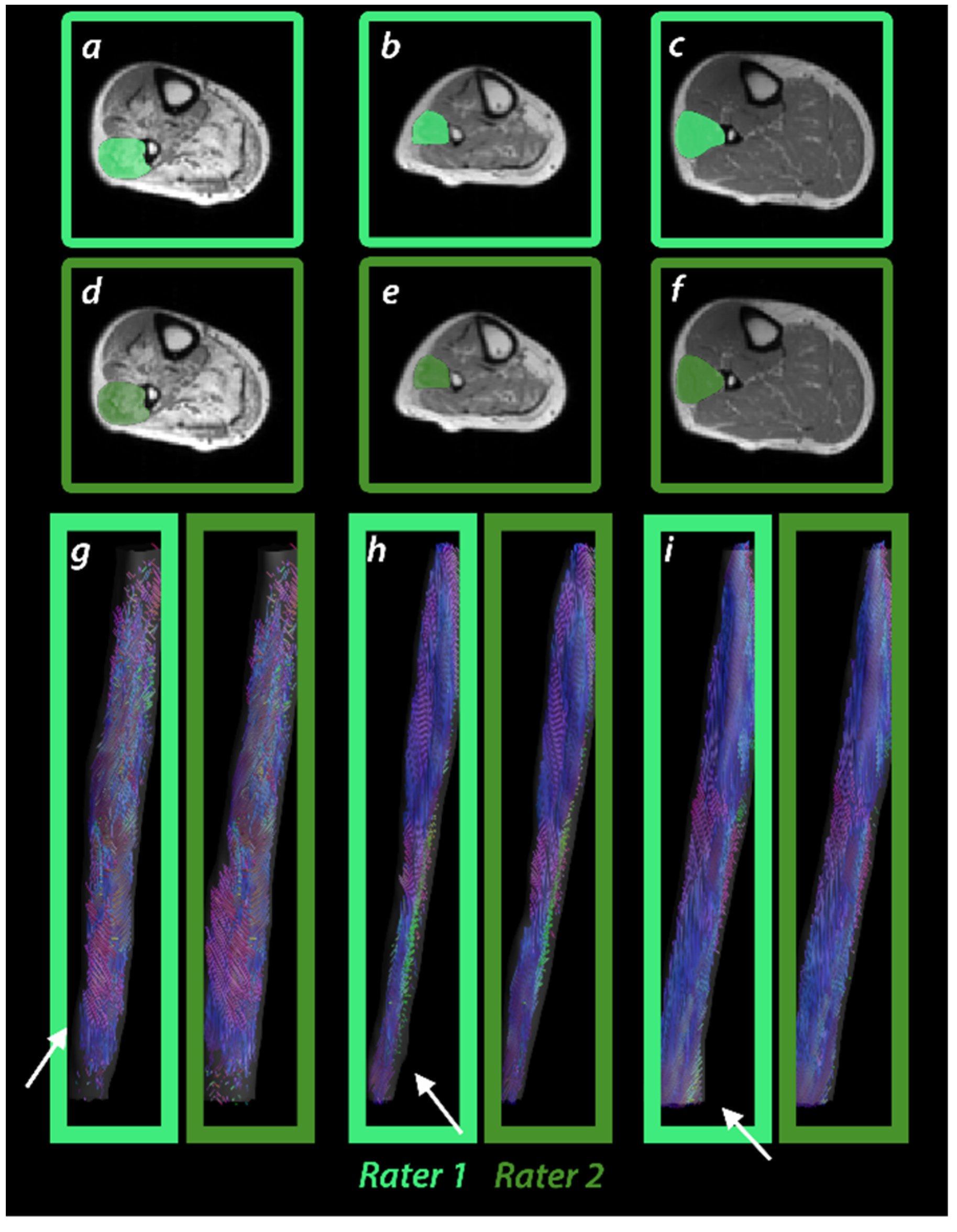
2.4. Muscle Segmentation and Tractography
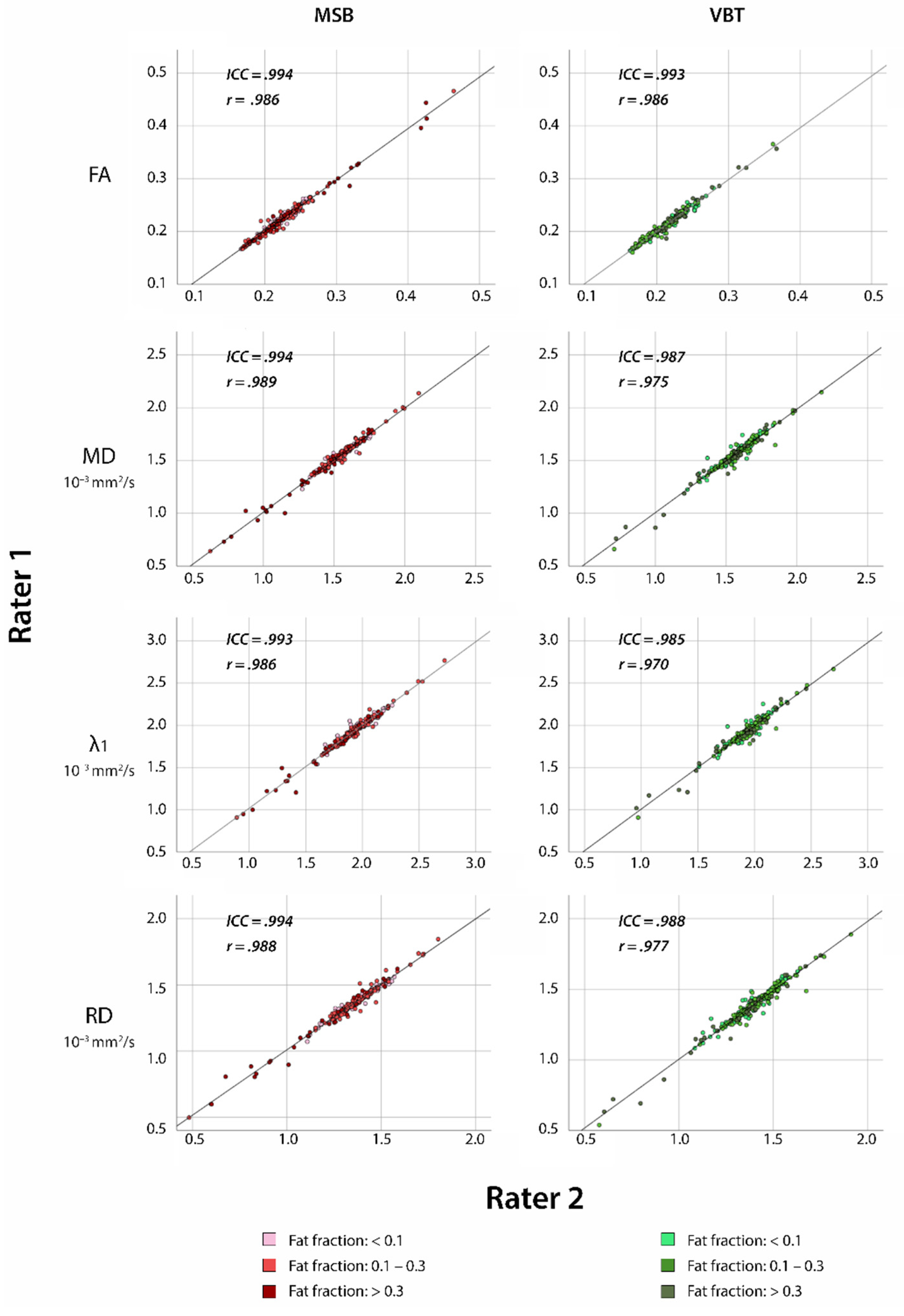
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Abbreviations:
| 3D | three-dimensional |
| CV | coefficient of variance |
| DWI | diffusion-weighted imaging |
| FA | fractional anisotropy |
| FOV | field of view |
| IBM | inclusion body myositis |
| ICC | intraclass correlation coefficient |
| LGMD | limb-girdle muscular dystrophy |
| MD | mean diffusivity |
| mDTI | muscle diffusion tensor imaging |
| MSB | manual segmentation-based analysis |
| MTL | mean tract length |
| NMD | neuromuscular diseases |
| PD | proton density-weighted |
| qMRI | quantitative magnet resonance imaging |
| RD | radial diffusivity |
| SPAIR | spectral attenuated inversion recovery |
| TD | tract density |
| TE | echo time |
| TR | repetition time |
| TSE | turbo spin-echo |
| VBT | volume-based tractography |
| Vol | volume |
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Díaz-Manera, J.; Llauger, J.; Gallardo, E.; Illa, I. Muscle MRI in muscular dystrophies. Acta Myol. 2015, 34, 95–108. [Google Scholar]
- Oudeman, J.; Nederveen, A.J.; Strijkers, G.J.; Maas, M.; Luijten, P.R.; Froeling, M. Techniques and applications of skeletal muscle diffusion tensor imaging: A review. J. Magn. Reson. Imaging 2016, 43, 773–788. [Google Scholar] [CrossRef]
- Schlaffke, L.; Rehmann, R.; Froeling, M.; Kley, R.; Tegenthoff, M.; Vorgerd, M.; Schmidt-wilcke, T. Diffusion Tensor Imaging of the Human Calf: Variation of Inter- and Intramuscle-Specific Diffusion Parameters. J. Magn. Reson. Imaging 2017, 46, 1137–1148. [Google Scholar] [CrossRef]
- Damon, B.M.; Froeling, M.; Buck, A.K.W.; Oudeman, J.; Ding, Z.; Nederveen, A.J.; Bush, E.C.; Strijkers, G.J. Skeletal muscle diffusion tensor-MRI fiber tracking: Rationale, data acquisition and analysis methods, applications and future directions. NMR Biomed. 2016, 31, 1252–1255. [Google Scholar] [CrossRef]
- Bolsterlee, B.; Souza, A.D.; Herbert, R.D. Reliability and robustness of muscle architecture measurements obtained using diffusion tensor imaging with anatomically constrained tractography. J. Biomech. 2019, 86, 71–78. [Google Scholar] [CrossRef]
- Forsting, J.; Rehmann, R.; Rohm, M.; Froeling, M.; Schlaffke, L. Evaluation of interrater reliability of different muscle segmentation techniques in diffusion tensor imaging. NMR Biomed. 2021, 34, 1–11. [Google Scholar] [CrossRef]
- Oudeman, J.; Mazzoli, V.; Marra, M.A.; Nicolay, K.; Maas, M. A novel diffusion-tensor MRI approach for skeletal muscle fascicle length measurements. Physiol. Rep. 2016, 4, e13012. [Google Scholar] [CrossRef] [PubMed]
- Chianca, V.; Albano, D.; Messina, C.; Cinnante, C.M.; Triulzi, F.M.; Sardanelli, F.; Sconfienza, L.M. Diffusion tensor imaging in the musculoskeletal and peripheral nerve systems: From experimental to clinical applications. Eur. Radiol. Exp. 2017, 1, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahrmann, A.S.; Stott, N.S.; Besier, T.F.; Fernandez, J.W.; Handsfield, G.G. Soleus muscle weakness in cerebral palsy: Muscle architecture revealed with Diffusion Tensor Imaging. PLoS ONE 2019, 14, e0205944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otto, L.A.M.; van der Pol, W.L.; Schlaffke, L.; Wijngaarde, C.A.; Stam, M.; Wadman, R.I.; Cuppen, I.; van Eijk, R.P.A.; Asselman, F.-L.; Bartels, B.; et al. Quantitative MRI of skeletal muscle in a cross-sectional cohort of patients with spinal muscular atrophy types 2 and 3. NMR Biomed. 2020, 34, e4357. [Google Scholar] [CrossRef]
- Guo, Z.; Zhang, H.; Chen, Z.; van der Plas, E.; Gutmann, L.; Thedens, D.; Nopoulos, P.; Sonka, M. Fully automated 3D segmentation of MR-imaged calf muscle compartments: Neighborhood relationship enhanced fully convolutional network. Comput. Med. Imaging Graph. 2021, 87, 101835. [Google Scholar] [CrossRef] [PubMed]
- Ogier, A.C.; Hostin, M.-A.; Bellemare, M.-E.; Bendahan, D. Overview of MR Image Segmentation Strategies in Neuromuscular Disorders. Front. Neurol. 2021, 12, 625308. [Google Scholar] [CrossRef]
- Diaz-Manera, J.; Fernandez-Torron, R.; Llauger, J.; James, M.K.; Mayhew, A.; Smith, F.E.; Moore, U.R.; Blamire, A.M.; Carlier, P.G.; Rufibach, L.; et al. Muscle MRI in patients with dysferlinopathy: Pattern recognition and implications for clinical trials. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1071–1081. [Google Scholar] [CrossRef] [Green Version]
- Keller, S.; Wang, Z.J.; Aigner, A.; Kim, A.C.; Golsari, A.C.K.A.; Kooijman, H.; Adam, G.; Yamamura, J.; Aigner, Z.J.W.A.; Golsari, A.C.K.A.; et al. Diffusion Tensor Imaging of Dystrophic Skeletal Muscle: Comparison of Two Segmentation Methods Adapted to Chemical-shift-encoded Water-fat MRI. Clin. Neuroradiol. 2019, 29, 231–242. [Google Scholar] [CrossRef]
- Schlaffke, L.; de Luca, A.; Weidlich, D.; Vaeggemose, M.; Froeling, M.; Rehmann, R.; Rohm, M.; Otto, L.A.M.; Nederveen, A.; Monte, J.; et al. Multi-center evaluation of stability and reproducibility of quantitative MRI measures in healthy calf muscles. NMR Biomed. 2019, 32, e4119. [Google Scholar] [CrossRef]
- Froeling, M. QMRTools: A Mathematica toolbox for quantitative MRI analysis. J. Open Source Softw. 2019, 4, 1204. [Google Scholar] [CrossRef]
- Tax, C.M.W.; Otte, W.M.; Viergever, M.A.; Dijkhuizen, R.M.; Leemans, A. REKINDLE: Robust extraction of kurtosis INDices with linear estimation. Magn. Reson. Med. 2015, 73, 794–808. [Google Scholar] [CrossRef]
- Leemans, A.; Jeurissen, B.; Sijbers, J.; Jones, D.K. ExploreDTI: A graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc. Intl. Soc. Mag. Reson. Med. 2009, 17, 3537. [Google Scholar]
- Froeling, M.; Tax, C.M.W.; Vos, S.B.; Luijten, P.R.; Leemans, A. “MASSIVE” brain dataset: Multiple acquisitions for standardization of structural imaging validation and evaluation. Magn. Reson. Med. 2017, 77, 1797–1809. [Google Scholar] [CrossRef]
- Forsting, J.; Rehmann, R.; Froeling, M.; Vorgerd, M.; Tegenthoff, M.; Schlaffke, L. Diffusion tensor imaging of the human thigh: Consideration of DTI-based fiber tracking stop criteria. Magn. Reson. Mater. Phys. Biol. Med. 2020, 33, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Fieremans, E.; Lemberskiy, G.; Veraart, J.; Sigmund, E.E.; Gyftopoulos, S.; Novikov, D.S. In vivo measurement of membrane permeability and myofiber size in human muscle using time-dependent diffusion tensor imaging and the random permeable barrier model. NMR Biomed. 2017, 30, e3612. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.R.; Eng, C.M.; Smallwood, L.H.; Lieber, R.L. Are current measurements of lower extremity muscle architecture accurate? Clin. Orthop. Relat. Res. 2009, 467, 1074–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Froeling, M.; Oudeman, J.; Strijkers, G.J.; Maas, M.; Drost, M.R.; Nicolay, K.; Nederveen, A.J. Muscle Changes Detected with Diffusion-Tensor Imaging after Long-Distance Running. Radiology 2015, 274, 548–562. [Google Scholar] [CrossRef] [PubMed]
- Rehmann, R.; Froeling, M.; Rohm, M.; Forsting, J.; Kley, R.A.; Schmidt-Wilcke, T.; Karabul, N.; Tegenthoff, M.; Vorgerd, M.; Schlaffke, L. Muscle Diffusion tensor imaging reveals changes in non-fat infiltrated muscles in late-onset Pompe disease. Muscle Nerve 2020, 62, 541–549. [Google Scholar] [CrossRef]
- Barp, A.; Carraro, E.; Albamonte, E.; Salmin, F.; Lunetta, C.; Pietro, G.; Messina, C.; Albano, D.; Chianca, V.; Maria, L.; et al. Muscle MRI in two SMA patients on nusinersen treatment: A two years follow-up. J. Neurol. Sci. 2020, 417, 117067. [Google Scholar] [CrossRef]
- Sinha, U.; Csapo, R.; Malis, V.; Xue, Y.; Sinha, S. Age-related differences in diffusion tensor indices and fiber architecture in the medial and lateral gastrocnemius. J. Magn. Reson. Imaging 2015, 41, 941–953. [Google Scholar] [CrossRef] [Green Version]
- Sinha, U.; Malis, V.; Csapo, R.; Moghadasi, A.; Kinugasa, R.; Sinha, S. Age-Related Differences in Strain Rate Tensor of the Medial Gastrocnemius Muscle During Passive Plantarflexion and Active Isometric Contraction Using Velocity Encoded MR Imaging: Potential Index of Lateral Force Transmission. Magn. Reson. Med. 2015, 73, 1852–1863. [Google Scholar] [CrossRef] [Green Version]
- Secondulfo, L.; Ogier, A.C.; Monte, J.R.; Aengevaeren, V.L.; Bendahan, D.; Nederveen, A.J.; Strijkers, G.J.; Hooijmans, M.T. Supervised segmentation framework for evaluation of diffusion tensor imaging indices in skeletal muscle. NMR Biomed. 2021, 34, e4406. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
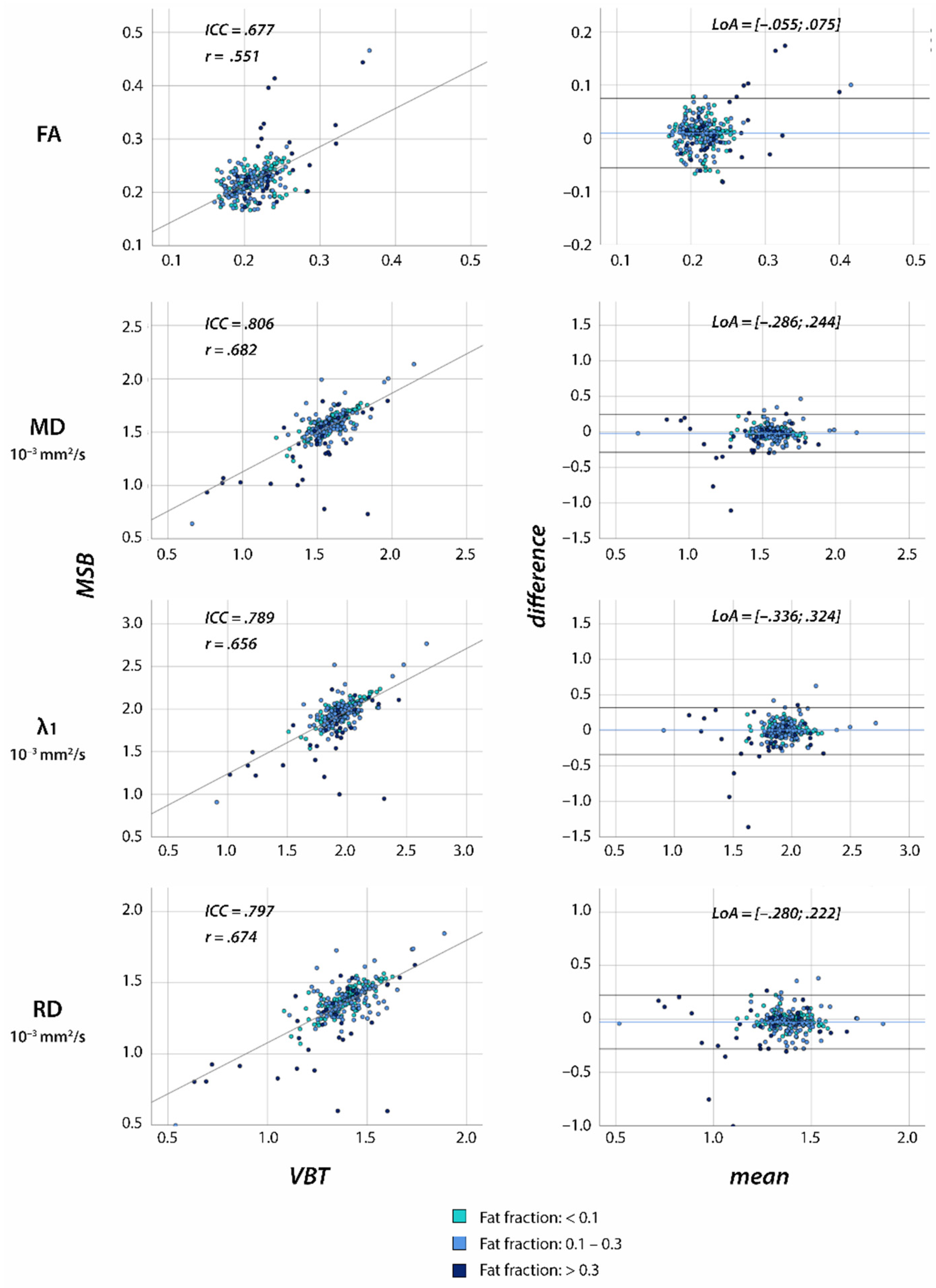
| MSB | VBT | Paired t-Tests | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | CV | Mean | SD | CV | |||||
| Healthy controls n = 20 | FA | 0.22 | ± | 0.03 | 0.13 | 0.21 | ± | 0.03 | 0.12 | <0.001 |
| MD | 1.58 | ± | 0.10 | 0.06 | 1.60 | ± | 0.12 | 0.08 | 0.005 | |
| λ1 | 1.97 | ± | 0.12 | 0.06 | 1.98 | ± | 0.14 | 0.07 | 0.551 | |
| RD | 1.39 | ± | 0.10 | 0.07 | 1.42 | ± | 0.12 | 0.08 | <0.001 | |
| TD | 25.61 | ± | 2.45 | 0.10 | ||||||
| MTL | 60.27 | ± | 26.66 | 0.44 | ||||||
| Vol | 158.9 | ± | 132.0 | 0.83 | ||||||
| NMD n = 18 | FA | 0.22 | ± | 0.04 | 0.17 | 0.21 | ± | 0.03 | 0.14 | <0.001 |
| MD | 1.54 | ± | 0.18 | 0.11 | 1.57 | ± | 0.16 | 0.10 | 0.025 | |
| λ1 | 1.92 | ± | 0.21 | 0.11 | 1.93 | ± | 0.19 | 0.10 | 0.621 | |
| RD | 1.35 | ± | 0.16 | 0.12 | 1.38 | ± | 0.15 | 0.11 | <0.001 | |
| TD | 24.85 | ± | 2.81 | 0.11 | ||||||
| MTL | 53.45 | ± | 26.99 | 0.50 | ||||||
| Vol | 156.5 | ± | 135.8 | 0.87 | ||||||
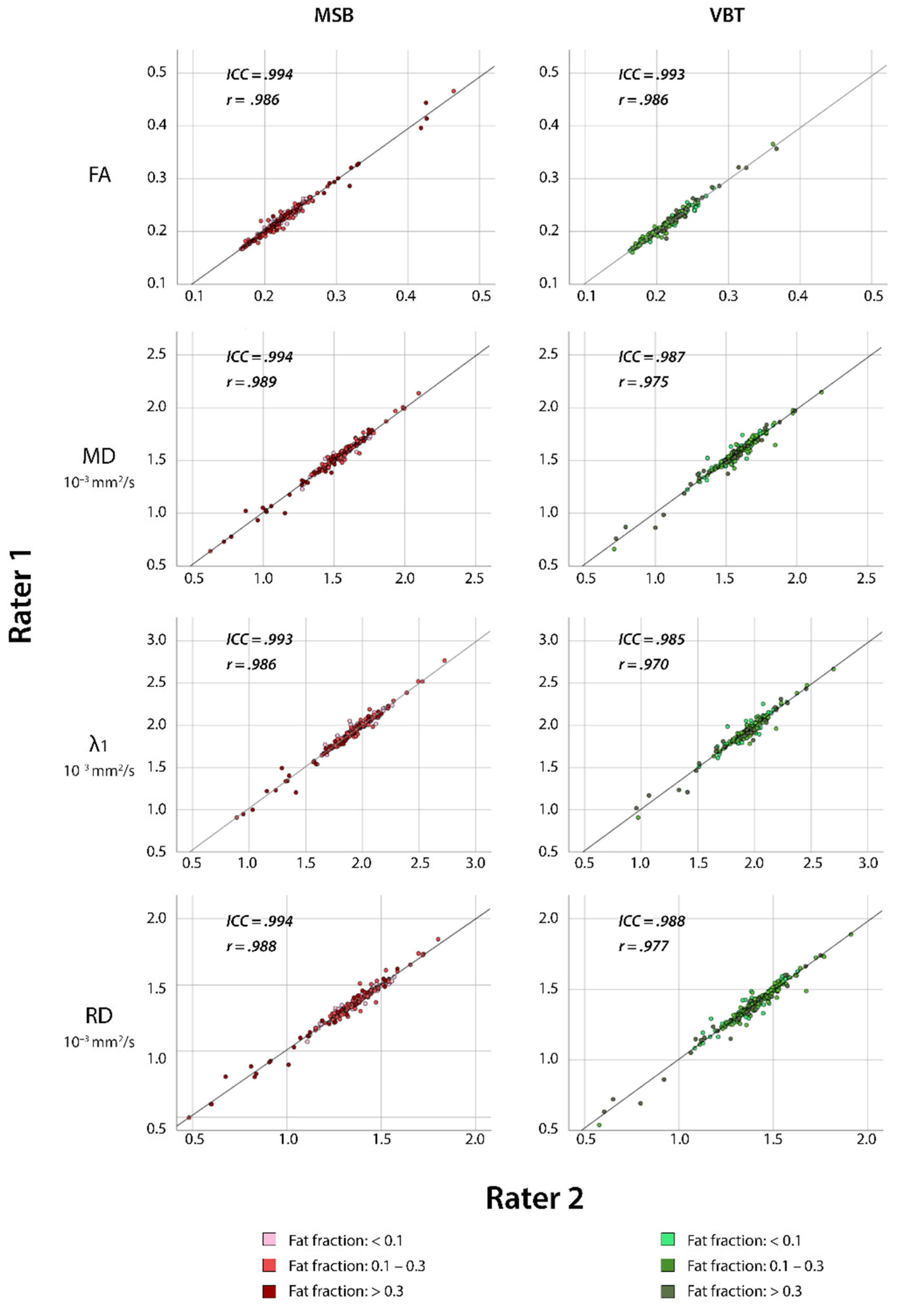
| MSB | VBT | |||||
|---|---|---|---|---|---|---|
| ICC | Cronbach’s α | ICC | Cronbach’s α | |||
| Healthy controls n = 20 | FA | 0.991 | 0.991 | 0.972 | 0.972 | |
| MD | 0.995 | 0.995 | 0.985 | 0.985 | ||
| λ1 | 0.992 | 0.993 | 0.980 | 0.980 | ||
| RD | 0.993 | 0.994 | 0.983 | 0.983 | ||
| NMD n = 18 | FA | 0.993 | 0.993 | 0.985 | 0.985 | |
| MD | 0.995 | 0.995 | 0.989 | 0.989 | ||
| λ1 | 0.994 | 0.994 | 0.988 | 0.988 | ||
| RD | 0.994 | 0.994 | 0.988 | 0.989 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsting, J.; Rohm, M.; Froeling, M.; Güttsches, A.-K.; Vorgerd, M.; Schlaffke, L.; Rehmann, R. High Inter-Rater Reliability of Manual Segmentation and Volume-Based Tractography in Healthy and Dystrophic Human Calf Muscle. Diagnostics 2021, 11, 1521. https://doi.org/10.3390/diagnostics11091521
Forsting J, Rohm M, Froeling M, Güttsches A-K, Vorgerd M, Schlaffke L, Rehmann R. High Inter-Rater Reliability of Manual Segmentation and Volume-Based Tractography in Healthy and Dystrophic Human Calf Muscle. Diagnostics. 2021; 11(9):1521. https://doi.org/10.3390/diagnostics11091521
Chicago/Turabian StyleForsting, Johannes, Marlena Rohm, Martijn Froeling, Anne-Katrin Güttsches, Matthias Vorgerd, Lara Schlaffke, and Robert Rehmann. 2021. "High Inter-Rater Reliability of Manual Segmentation and Volume-Based Tractography in Healthy and Dystrophic Human Calf Muscle" Diagnostics 11, no. 9: 1521. https://doi.org/10.3390/diagnostics11091521
APA StyleForsting, J., Rohm, M., Froeling, M., Güttsches, A.-K., Vorgerd, M., Schlaffke, L., & Rehmann, R. (2021). High Inter-Rater Reliability of Manual Segmentation and Volume-Based Tractography in Healthy and Dystrophic Human Calf Muscle. Diagnostics, 11(9), 1521. https://doi.org/10.3390/diagnostics11091521