
Shortening the Time of the Identification and Antimicrobial Susceptibility Testing on Positive Blood Cultures with MALDI-TOF MS


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection and Culture
2.2. Subculture and Identification of Bacterial Samples
2.3. The AST Using the BD PhenixTM M50 Automated Microbiology System
2.4. Short-Term Incubation Process
2.5. Quality Control
2.6. Statistical Analysis
3. Results
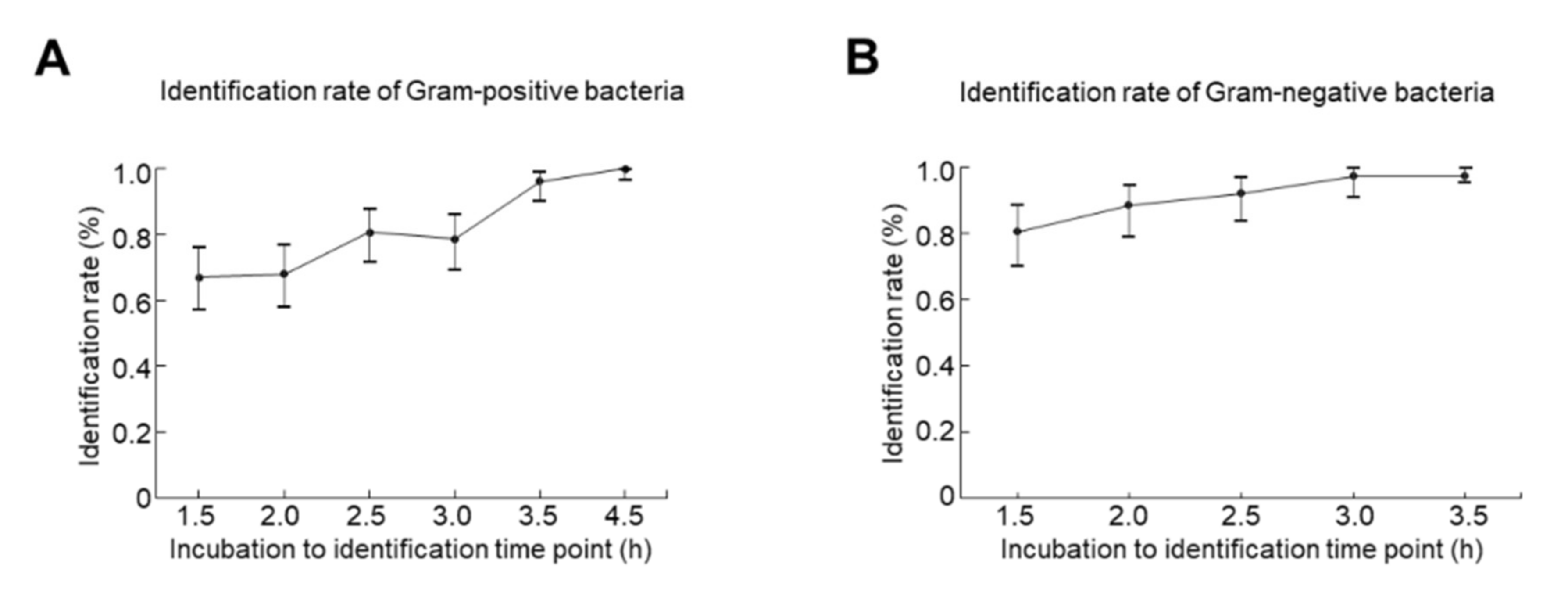
3.1. The Optimal Incubation Time for ID
3.2. The Short-Term Incubation on the M50 AST Panels Showed High Category Agreements Compared to the Conventional Disk Method
3.3. Short-Term Incubation on the Disk Diffusion AST and the BD PhoenixTM M50 AST Panels Showed High Category Agreements Compared to Overnight Incubation Colonies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care, T. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- Huang, C.Y.; Daniels, R.; Lembo, A.; Hartog, C.; O’Brien, J.; Heymann, T.; Reinhart, K.; Nguyen, H.B.; Sepsis Survivors Engagement, P. Life after sepsis: An international survey of survivors to understand the post-sepsis syndrome. Int. J. Qual. Health Care 2019, 31, 191–198. [Google Scholar] [CrossRef]
- Plevin, R.; Callcut, R. Update in sepsis guidelines: What is really new? Trauma Surg. Acute Care Open 2017, 2, e000088. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Leibovici, L.; Shraga, I.; Drucker, M.; Konigsberger, H.; Samra, Z.; Pitlik, S.D. The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection. J. Intern. Med. 1998, 244, 379–386. [Google Scholar] [CrossRef]
- Park, H.; Jang, K.J.; Jang, W.; Park, S.H.; Park, J.Y.; Jeon, T.J.; Oh, T.H.; Shin, W.C.; Choi, W.C.; Sinn, D.H. Appropriate empirical antibiotic use and 30-d mortality in cirrhotic patients with bacteremia. World J. Gastroenterol. 2015, 21, 3587–3592. [Google Scholar] [CrossRef]
- Tabak, Y.P.; Vankeepuram, L.; Ye, G.; Jeffers, K.; Gupta, V.; Murray, P.R. Blood Culture Turnaround Time in U.S. Acute Care Hospitals and Implications for Laboratory Process Optimization. J. Clin. Microbiol. 2018, 56, e00500-18. [Google Scholar] [CrossRef] [PubMed]
- Osih, R.B.; McGregor, J.C.; Rich, S.E.; Moore, A.C.; Furuno, J.P.; Perencevich, E.N.; Harris, A.D. Impact of empiric antibiotic therapy on outcomes in patients with Pseudomonas aeruginosa bacteremia. Antimicrob. Agents Chemother. 2007, 51, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Jakovljev, A.; Bergh, K. Development of a rapid and simplified protocol for direct bacterial identification from positive blood cultures by using matrix assisted laser desorption ionization time-of- flight mass spectrometry. BMC Microbiol. 2015, 15, 258. [Google Scholar] [CrossRef][Green Version]
- Idelevich, E.A.; Schüle, I.; Grünastel, B.; Wüllenweber, J.; Peters, G.; Becker, K. Rapid identification of microorganisms from positive blood cultures by MALDI-TOF mass spectrometry subsequent to very short-term incubation on solid medium. Clin. Microbiol. Infect. 2014, 20, 1001–1006. [Google Scholar] [CrossRef]
- Bhatti, M.M.; Boonlayangoor, S.; Beavis, K.G.; Tesic, V. Rapid identification of positive blood cultures by matrix-assisted laser desorption ionization-time of flight mass spectrometry using prewarmed agar plates. J. Clin. Microbiol. 2014, 52, 4334–4338. [Google Scholar] [CrossRef] [PubMed]
- Barnini, S.; Brucculeri, V.; Morici, P.; Ghelardi, E.; Florio, W.; Lupetti, A. A new rapid method for direct antimicrobial susceptibility testing of bacteria from positive blood cultures. BMC Microbiol. 2016, 16, 185. [Google Scholar] [CrossRef]
- Romero-Gomez, M.P.; Gomez-Gil, R.; Pano-Pardo, J.R.; Mingorance, J. Identification and susceptibility testing of microorganism by direct inoculation from positive blood culture bottles by combining MALDI-TOF and Vitek-2 Compact is rapid and effective. J. Infect. 2012, 65, 513–520. [Google Scholar] [CrossRef]
- Gherardi, G.; Angeletti, S.; Panitti, M.; Pompilio, A.; Di Bonaventura, G.; Crea, F.; Avola, A.; Fico, L.; Palazzo, C.; Sapia, G.F.; et al. Comparative evaluation of the Vitek-2 Compact and Phoenix systems for rapid identification and antibiotic susceptibility testing directly from blood cultures of Gram-negative and Gram-positive isolates. Diagn Microbiol. Infect. Dis. 2012, 72, 20–31. [Google Scholar] [CrossRef]
- Machen, A.; Drake, T.; Wang, Y.F. Same day identification and full panel antimicrobial susceptibility testing of bacteria from positive blood culture bottles made possible by a combined lysis-filtration method with MALDI-TOF VITEK mass spectrometry and the VITEK2 system. PLoS ONE 2014, 9, e87870. [Google Scholar] [CrossRef] [PubMed]
- Sparbier, K.; Lange, C.; Jung, J.; Wieser, A.; Schubert, S.; Kostrzewa, M. MALDI biotyper-based rapid resistance detection by stable-isotope labeling. J. Clin. Microbiol. 2013, 51, 3741–3748. [Google Scholar] [CrossRef]
- CLSI. Verification of Commercial Microbial Identification and Antimicrobial Susceptibility Testing Systems, 1st ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2015. [Google Scholar]
- Opota, O.; Croxatto, A.; Prod’hom, G.; Greub, G. Blood culture-based diagnosis of bacteraemia: State of the art. Clin. Microbiol. Infect. 2015, 21, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Teng, C.B.; Cunningham, S.A.; Ihde, S.M.; Steckelberg, J.M.; Moriarty, J.P.; Shah, N.D.; Mandrekar, J.N.; Patel, R. Randomized Trial of Rapid Multiplex Polymerase Chain Reaction-Based Blood Culture Identification and Susceptibility Testing. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 1071–1080. [Google Scholar] [CrossRef]
- Felsenstein, S.; Bender, J.M.; Sposto, R.; Gentry, M.; Takemoto, C.; Bard, J.D. Impact of a Rapid Blood Culture Assay for Gram-Positive Identification and Detection of Resistance Markers in a Pediatric Hospital. Arch. Pathol. Lab. Med. 2016, 140, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Sauer, S.; Kliem, M. Mass spectrometry tools for the classification and identification of bacteria. Nat. Rev. Microbiol. 2010, 8, 74–82. [Google Scholar] [CrossRef]
- Verroken, A.; Defourny, L.; Lechgar, L.; Magnette, A.; Delmée, M.; Glupczynski, Y. Reducing time to identification of positive blood cultures with MALDI-TOF MS analysis after a 5-h subculture. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Altun, O.; Botero-Kleiven, S.; Carlsson, S.; Ullberg, M.; Ozenci, V. Rapid identification of bacteria from positive blood culture bottles by MALDI-TOF MS following short-term incubation on solid media. J. Med. Microbiol. 2015, 64, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.N.; Lai, C.H.; Chen, Y.H.; Chang, L.L.; Lu, P.L.; Tsai, S.S.; Lin, H.L.; Lin, H.H. Characteristics and outcomes of polymicrobial bloodstream infections in the emergency department: A matched case-control study. Acad. Emerg. Med. 2010, 17, 1072–1079. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Short-Term Culture Followed by MALDI-TOF MS [n (%)] | Conventional | ||||||
|---|---|---|---|---|---|---|---|
| Organism | 1.5 h | 2 h | 2.5 h | 3 h | 3.5 h | 4.5 h | >24 h |
| Staphylococcus spp. | 24 (54.4%) | 29 (65.9%) | 30 (68.2%) | 37 (84.1%) | 40 (90.9%) | 44 (100%) | 44 |
| Staphylococcus aureus | 18 | 19 | 19 | 22 | 22 | 22 | 22 |
| Staphylococcus capitis | 2 | 2 | 3 | 3 | 3 | 7 | 7 |
| Staphylococcus caprae | 1 | 2 | 0 | 2 | 2 | 2 | 2 |
| Staphylococcus epidermidis | 3 | 5 | 5 | 5 | 7 | 7 | 7 |
| Staphylococcus hominis | 0 | 1 | 2 | 2 | 2 | 2 | 2 |
| Staphylococcus warneri | 0 | 0 | 1 | 3 | 4 | 4 | 4 |
| Enterococcus spp. | 25 (86.2%) | 27 (93.1%) | 29 (100%) | 29 (100%) | 29 (100%) | 29 (100%) | 29 |
| Enterococcus faecalis | 13 | 13 | 14 | 14 | 14 | 14 | 14 |
| Enterococcus faecium | 11 | 13 | 14 | 14 | 14 | 14 | 14 |
| Enterococcus gallinarum | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Streptococcus spp. | 20 (66.7%) | 14 (46.7%) | 24 (80.0%) | 15 (50.0%) | 30 (100%) | 30 (100%) | 30 |
| Streptococcus agalactiae | 9 | 9 | 9 | 9 | 9 | 9 | 9 |
| Streptococcus anginosus | 1 | - | 2 | - | 4 | 4 | 4 |
| Streptococcus constellatus | 2 | - | 0 | - | 4 | 4 | 4 |
| Streptococcus dysgalactiae | 3 | - | 7 | - | 7 | 7 | 7 |
| Streptococcus gallolyticus | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Streptococcus oralis | 0 | 0 | 1 | 1 | 1 | 1 | 1 |
| Streptococcus salivarius | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Streptococcus suis | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total | 69 (67.0%) | 70 (68.0%) | 83 (80.6%) | 81 (78.6%) | 99 (96.1%) | 103 (100%) | 103 (100%) |
| Short-Term Incubation Followed by MALDI-TOF MS | Conventional | |||||
|---|---|---|---|---|---|---|
| Organism | 1.5 h | 2 h | 2.5 h | 3 h | 3.5 h | >24 h |
| Enterobacterales | ||||||
| Citrobacter spp. | 3 (75.0%) | 3 (75.0%) | 3 (75.0%) | 4 (100%) | 4 (100%) | 4 |
| Citrobacterbraakii | 0 | 0 | 0 | 1 | 1 | 1 |
| Citrobacterkoseri | 3 | 3 | 3 | 3 | 3 | 3 |
| Enterobacter spp. | ||||||
| Enterobacter cloacae | 3 (75.0%) | 3 (75.0%) | 4 (100%) | 4 (100%) | 4 (100%) | 4 |
| Escherichia spp. | 17 (77.3%) | 21 (95.5%) | 22 (100%) | 22 (100%) | 22 (100%) | 22 |
| Escherichia coli | 17 | 21 | 22 | 22 | 22 | 22 |
| Klebsiella spp. | 10 (83.3%) | 11 (91.7%) | 12 (100%) | 12 (100%) | 12 (100%) | 12 |
| Klebsiellaaerogenes | 2 | 2 | 2 | 2 | 2 | 2 |
| Klebsiellaoxytoca | 3 | 3 | 4 | 4 | 4 | 4 |
| Klebsiella pneumoniae | 5 | 6 | 6 | 6 | 6 | 6 |
| Leclercia spp. | 3 (100%) | 3 (100%) | 3 (100%) | 3 (100%) | 3 (100%) | 3 |
| Leclerciaadecarboxylata | 3 | 3 | 3 | 3 | 3 | 3 |
| Morganella spp. | 4 (100%) | 4 (100%) | 4 (100%) | 4 (100%) | 4 (100%) | 4 |
| Morganellamorganii | 4 | 4 | 4 | 4 | 4 | 4 |
| Proteus spp. | 3 (100%) | 3 (100%) | 3 (100%) | 3 (100%) | 3 (100%) | 3 |
| Proteus mirabilis | 3 | 3 | 3 | 3 | 3 | 3 |
| Salmonella spp. | 3 (50.0%) | 4 (66.7%) | 5 (83.3%) | 6 (100%) | 6 (100%) | 6 |
| Salmonella spp. | 3 | 4 | 5 | 6 | 6 | 6 |
| Serratia spp. | 2 (66.7%) | 2 (66.7%) | 2 (66.7%) | 1 (33.3%) | 1 (33.3%) | 3 |
| Serratiamarcescens | 2 | 2 | 2 | 1 | 1 | 2 |
| Serratiaureilytica | 0 | 0 | 0 | 0 | 0 | 1 |
| Subtotal | 48 (78.7%) | 54 (88.5%) | 58 (95.1%) | 59 (96.7%) | 59 (96.7%) | 61 |
| Non-Enterobacterales | ||||||
| Acinetobacter spp. | 6 (100%) | 5 (83.3%) | 5 (83.3%) | 6 (100%) | 6 (100%) | 6 |
| Acinetobacter baumannii | 4 | 3 | 3 | 4 | 4 | 4 |
| Acinetobacter johnsonii | 2 | 2 | 2 | 2 | 2 | 2 |
| Aeromonas spp. | 2 (100%) | 2 (100%) | 2 (100%) | 2 (100%) | 2(100%) | 2 |
| Aeromonascaviae | 1 | 1 | 1 | 1 | 1 | 1 |
| Aeromonashydrophila | 1 | 1 | 1 | 1 | 1 | 1 |
| Pseudomonas spp. | 4 (66.7%) | 5 (83.3%) | 4 (66.7%) | 6 (100%) | 6 (100%) | 6 |
| Pseudomonas aeruginosa | 4 | 5 | 4 | 6 | 6 | 6 |
| Stenotrophomonas spp. | 2 (100%) | 2 (100%) | 2 (100%) | 2 (100%) | 2 (100%) | 2 |
| Stenotrophomonasmaltophilia | 2 | 2 | 2 | 2 | 2 | 2 |
| Subtotal | 14(87.5%) | 14 (87.5%) | 13 (81.3%) | 16 (100%) | 16 (100%) | 16 |
| Total | 62 (80.5%) | 68 (88.3%) | 71 (92.2%) | 75 (97.4%) | 75 (97.4%) | 77 |
| Antimicrobial Agent | Category Agreement | Very Major Error | Major Error | Minor Error | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | All-CoNS | All | All-CoNS | All | All-CoNS | All | All-CoNS | All | All-CoNS | |||||||||
| n | % | n | % | n/Resistant | % | n/Resistant | % | n/Susceptible | % | n/Susceptible | % | n/Total | % | n/Total | % | n | % | |
| Ampicillin | 29 | 100 | 29 | 100 | 0/14 | 0 | 0/14 | 0 | 0/15 | 0 | 0/15 | 0 | 0/29 | 0 | 0/29 | 0 | 29 | 29 |
| Clindamycin | 38 | 86.4 | 21 | 95.5 | 2/13 | 15.4 | 0/4 | 0 | 3/31 | 9.7 | 0/18 | 0 | 1/44 | 2.3 | 1/22 | 4.5 | 44 | 22 |
| Fusidic Acid | 39 | 88.6 | 22 | 100 | 4/7 | 57.1 | 0/0 | 0 | 1/37 | 2.7 | 0/22 | 0 | 0/44 | 0 | 0/22 | 0 | 44 | 22 |
| Gentamicin | 33 | 75.0 | 20 | 90.9 | 2/19 | 10.5 | 0/9 | 0 | 5/23 | 21.7 | 1/12 | 8.3 | 4/44 | 9.1 | 1/22 | 4.5 | 44 | 22 |
| Gentamicin-Synergy | 28 | 96.6 | 28 | 96.6 | 0/8 | 0 | 0/8 | 0 | 1/21 | 4.8 | 1/21 | 4.8 | 0/29 | 0 | 0/29 | 0 | 29 | 29 |
| Minocycline | 42 | 95.5 | 22 | 100 | 1/1 | 100 | 0/0 | 0 | 0/41 | 0 | 0/21 | 0 | 1/44 | 2.3 | 0/22 | 0 | 44 | 22 |
| Oxacillin | 22 | 100 | 22 | 100 | 0/10 | 0 | 0/10 | 0 | 0/12 | 0 | 0/12 | 0 | 0/22 | 0 | 0/22 | 0 | 22 | 22 |
| Penicillin G | 63 | 98.4 | 48 | 98.0 | 0/48 | 0 | 0/33 | 0 | 1/16 | 6.3 | 1/16 | 6.3 | 0/64 | 0 | 0/49 | 0 | 64 | 49 |
| Teicoplanin | 69 | 95.8 | 49 | 96.1 | 0/9 | 0 | 0/9 | 0 | 2/63 | 2.3 | 1/42 | 2.4 | 1/72 | 1.4 | 1/51 | 2.0 | 72 | 51 |
| Trimethoprim-Sulfamethoxazole | 36 | 81.8 | 20 | 90.9 | 2/7 | 28.6 | 0/2 | 0 | 5/36 | 13.9 | 2/20 | 10.0 | 1/44 | 2.3 | 0/22 | 0 | 44 | 22 |
| Vancomycin | 28 | 96.6 | 28 | 96.6 | 0/10 | 0 | 0/10 | 0 | 1/19 | 5.3 | 1/19 | 5.3 | 0/29 | 0 | 0/29 | 0 | 29 | 29 |
| Total | 427 | 91.8 | 309 | 96.9 | 11/146 | 7.5 | 0/99 | 0 | 19/314 | 6.1 | 7/218 | 3.2 | 8/465 | 1.7 | 3/319 | 0.9 | 465 | 319 |
| Antimicrobial Agent | Category Agreement | Very Major Error | Major Error | Minor Error | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n/Resistant | % | n/Susceptible | % | n/total | % | n | |
| Ampicillin | 16 | 100 | 0/0 | 0 | 0/16 | 0 | 0/16 | 0 | 16 |
| Ceftriaxone | 29 | 96.7 | 0/0 | 0 | 1/30 | 3.3 | 0/30 | 0 | 30 |
| Clindamycin | 28 | 93.3 | 0/9 | 0 | 2/21 | 9.5 | 0/30 | 0 | 30 |
| Penicillin G | 16 | 100 | 0/0 | 0 | 0/16 | 0 | 0/16 | 0 | 16 |
| Vancomycin | 30 | 100 | 0/0 | 0 | 0/30 | 0 | 0/3 | 0 | 30 |
| Total | 119 | 97.5 | 0/9 | 0 | 3/113 | 2.7 | 0/122 | 0 | 122 |
| Antimicrobial Agent | Category Agreement | Very Major Error | Major Error | Minor Error | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n/Resistant | % | n/Susceptible | % | n/Total | % | n | |
| Amikacin | 17 | 94.4 | 0/4 | 0 | 0/14 | 0 | 1/18 | 5.6 | 18 |
| Ampicillin | 54 | 88.5 | 1/45 | 2.2 | 3/14 | 21.4 | 3/61 | 4.9 | 61 |
| Cefazolin | 46 | 83.6 | 3/33 | 9.1 | 1/11 | 9.1 | 5/55 | 9.1 | 55 |
| Ceftazidime | 67 | 89.3 | 0/17 | 0 | 0/55 | 0 | 8/75 | 10.7 | 75 |
| Ceftriaxone | 63 | 100 | 0/14 | 0 | 0/49 | 0 | 0/63 | 0 | 63 |
| Ciprofloxacin | 26 | 100 | 0/16 | 0 | 0/9 | 0 | 0/26 | 0 | 26 |
| Colistin | 0 | 0 | 0/0 | 0 | 0/0 | 0 | 0/0 | 0 | 0 |
| Ertapenem | 54 | 94.7 | 0/0 | 0 | 1/54 | 1.9 | 2/57 | 3.5 | 57 |
| Gentamicin | 66 | 98.5 | 0/10 | 0 | 1/57 | 1.8 | 0/67 | 0 | 67 |
| Levofloxacin | 8 | 80.0 | 0/0 | 0 | 0/10 | 0 | 2/10 | 20.0 | 10 |
| Meropenem | 14 | 100 | 0/5 | 0 | 0/9 | 0 | 0/14 | 0 | 14 |
| Minocycline | 7 | 87.5 | 1/1 | 100 | 0/4 | 0 | 0/8 | 0 | 8 |
| Piperacillin-Tazobactam | 63 | 94.0 | 0/5 | 0 | 0/57 | 0 | 4/67 | 6.0 | 67 |
| Tigecycline | 7 | 70.0 | 0/0 | 0 | 0/5 | 0 | 3/10 | 30.0 | 10 |
| Trimethoprim-Sulfamethoxazole | 15 | 93.8 | 1/5 | 20.0 | 0/11 | 0 | 0/16 | 0 | 16 |
| Total | 507 | 92.7 | 6/155 | 3.9 | 6/359 | 1.7% | 28/547 | 5.1 | 547 |
| Organisms | Category Agreement | Very Major Error | Major Error | Minor Error | ||||
|---|---|---|---|---|---|---|---|---|
| n/Total | % | n/Resistant | % | n/Susceptible | % | n/total | % | |
| Disk Diffusion Method 1 | ||||||||
| Gram-positive | ||||||||
| Non-Streptococcus | 328/342 | 95.9 | 3/104 | 2.9 | 8/236 | 3.4 | 3/342 | 0.9 |
| Streptococcus | 116/119 | 97.5 | 0/8 | 0 | 2/111 | 1.8 | 1/119 | 0.8 |
| Gram negative | 440/447 | 98.4 | 0/133 | 0 | 0/287 | 0 | 7/447 | 1.6 |
| BD Phoenix™ M50 AST 2 | ||||||||
| Gram-positive | ||||||||
| Non-Streptococcus | 1357/1420 | 95.6 | 8/551 | 1.5 | 17/820 | 2.1 | 38/1420 | 2.7 |
| Streptococcus | 370/390 | 94.9 | 2/40 | 5.0 | 10/345 | 2.9 | 8/390 | 2.1 |
| Gram-negative | 1245/1286 | 96.8 | 3/355 | 0.8 | 13/876 | 1.5 | 25/1286 | 1.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, Y.-W.; Lin, T.-C.; Chou, H.-Y.; Hung, H.-Y.; Tan, C.-K.; Wu, L.-C.; Feng, I.-J.; Shiue, Y.-L. Shortening the Time of the Identification and Antimicrobial Susceptibility Testing on Positive Blood Cultures with MALDI-TOF MS. Diagnostics 2021, 11, 1514. https://doi.org/10.3390/diagnostics11081514
Tsai Y-W, Lin T-C, Chou H-Y, Hung H-Y, Tan C-K, Wu L-C, Feng I-J, Shiue Y-L. Shortening the Time of the Identification and Antimicrobial Susceptibility Testing on Positive Blood Cultures with MALDI-TOF MS. Diagnostics. 2021; 11(8):1514. https://doi.org/10.3390/diagnostics11081514
Chicago/Turabian StyleTsai, Ya-Wen, Ting-Chia Lin, Hsiu-Yin Chou, Huei-Ya Hung, Che-Kim Tan, Li-Ching Wu, I-Jung Feng, and Yow-Ling Shiue. 2021. "Shortening the Time of the Identification and Antimicrobial Susceptibility Testing on Positive Blood Cultures with MALDI-TOF MS" Diagnostics 11, no. 8: 1514. https://doi.org/10.3390/diagnostics11081514
APA StyleTsai, Y.-W., Lin, T.-C., Chou, H.-Y., Hung, H.-Y., Tan, C.-K., Wu, L.-C., Feng, I.-J., & Shiue, Y.-L. (2021). Shortening the Time of the Identification and Antimicrobial Susceptibility Testing on Positive Blood Cultures with MALDI-TOF MS. Diagnostics, 11(8), 1514. https://doi.org/10.3390/diagnostics11081514