
Can Pre-Treatment Inflammatory Parameters Predict the Probability of Sphincter-Preserving Surgery in Patients with Locally Advanced Low-Lying Rectal Cancer?



Abstract
1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Baseline Patient and Tumor Parameters Associated with Sphincter-Preserving Surgery
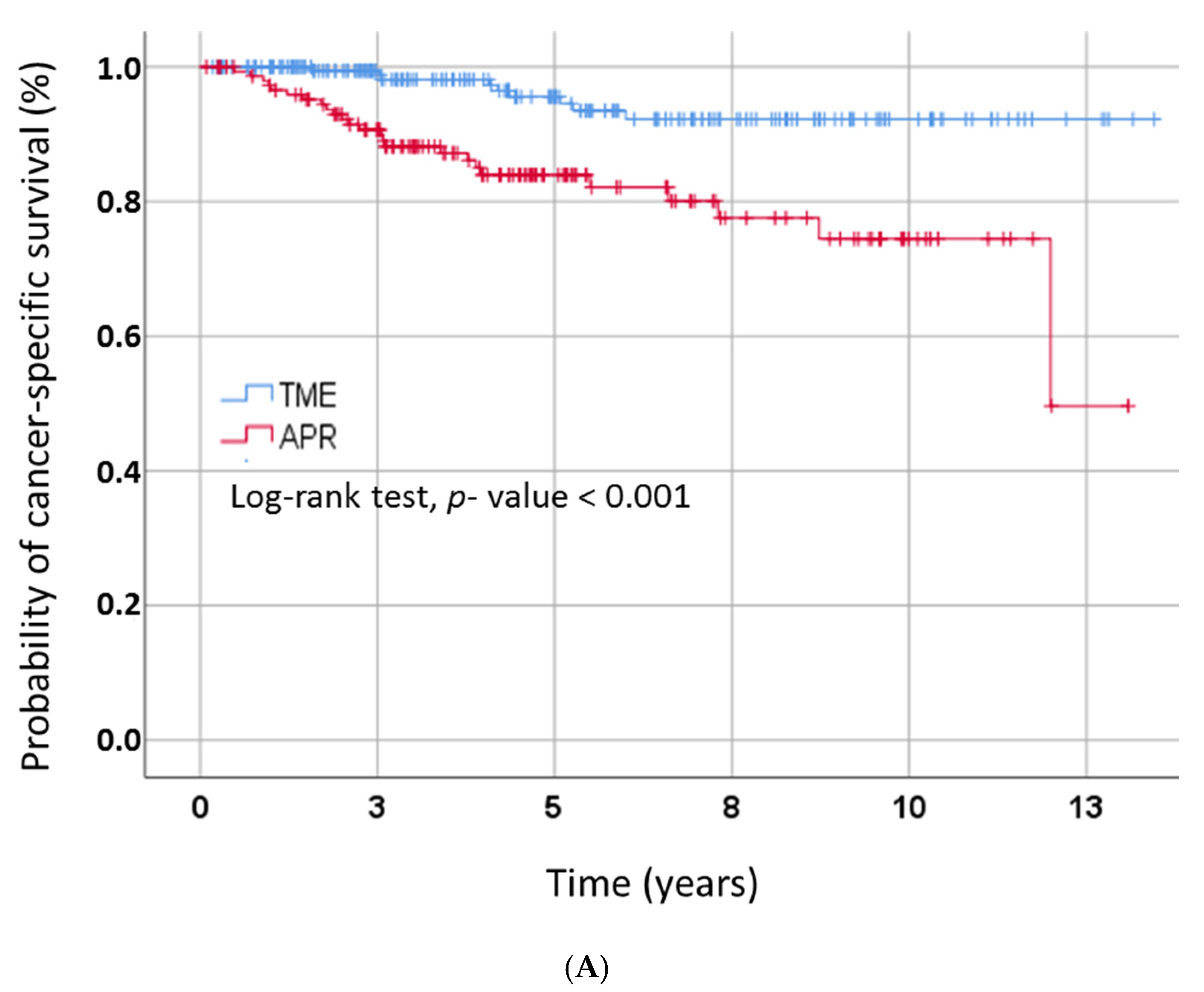
3.2. Outcome by Type of Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef]
- Akgun, E.; Ozkok, S.; Tekin, M.; Yoldas, T.; Caliskan, C.; Kose, T.; Karabulut, B.; Sezak, M.; Elmas, N.; Ozutemiz, O. The effects of chemoradiotherapy on recurrence and survival in locally advanced rectal cancers with curative total mesorectal excision: A prospective, nonrandomized study. World J. Surg. Oncol. 2017, 15, 205. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef]
- Crane, C.H.; Skibber, J.M.; Feig, B.W.; Vauthey, J.N.; Thames, H.D.; Curley, S.A.; Rodriguez-Bigas, M.A.; Wolff, R.A.; Ellis, L.M.; Delclos, M.E.; et al. Response to preoperative chemoradiation increases the use of sphincter-preserving surgery in patients with locally advanced low rectal carcinoma. Cancer 2003, 97, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.; Raissouni, S.; Price Hiller, J.; Mercer, J.; Powell, E.; MacLean, A.; Jiang, M.; Doll, C.; Goodwin, R.; Batuyong, E.; et al. Predictors of Pathologic Complete Response After Neoadjuvant Treatment for Rectal Cancer: A Multicenter Study. Clin. Colorectal Cancer 2015, 14, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Pucciarelli, S.; Bertorelle, R.; De Rossi, A.; Nitti, D. Predictive factors of the response of rectal cancer to neoadjuvant radiochemotherapy. Cancers 2011, 3, 2176–2194. [Google Scholar] [CrossRef]
- Lu, K.; Zhu, Y.; Sheng, L.; Liu, L.; Shen, L.; Wei, Q. Serum fibrinogen level predicts the therapeutic response and prognosis in patients with locally advanced rectal cancer. Hepatogastroenterology 2011, 58, 1507–1510. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Kitayama, J.; Tsuno, N.H.; Sunami, E.; Nagawa, H. Hyperfibrinogenemia after preoperative chemoradiotherapy predicts poor response and poor prognosis in rectal cancer. Int. J. Colorectal Dis. 2011, 26, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Kawai, K.; Kitayama, J.; Tsuno, N.H.; Sunami, E.; Watanabe, T. Thrombocytosis before pre-operative chemoradiotherapy predicts poor response and shorter local recurrence-free survival in rectal cancer. Int. J. Colorectal Dis. 2013, 28, 527–535. [Google Scholar] [CrossRef]
- Moureau-Zabotto, L.; Farnault, B.; de Chaisemartin, C.; Esterni, B.; Lelong, B.; Viret, F.; Giovannini, M.; Monges, G.; Delpero, J.R.; Bories, E.; et al. Predictive factors of tumor response after neoadjuvant chemoradiation for locally advanced rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 483–491. [Google Scholar] [CrossRef]
- Wallin, U.; Rothenberger, D.; Lowry, A.; Luepker, R.; Mellgren, A. CEA—A predictor for pathologic complete response after neoadjuvant therapy for rectal cancer. Dis. Colon. Rectum. 2013, 56, 859–868. [Google Scholar] [CrossRef]
- Sun, Y.; Zhang, Y.; Huang, Z.; Lin, H.; Lu, X.; Huang, Y.; Chi, P. Combination of Preoperative Plasma Fibrinogen and Neutrophil-to-Lymphocyte Ratio (the F-NLR Score) as a Prognostic Marker of Locally Advanced Rectal Cancer Following Preoperative Chemoradiotherapy. World J. Surg. 2020, 44, 1975–1984. [Google Scholar] [CrossRef] [PubMed]
- Baral, J.; Schon, M.R.; Ruppert, R.; Ptok, H.; Strassburg, J.; Brosi, P.; Kreis, M.E.; Lewin, A.; Sauer, J.; Sawicki, S.; et al. Spincter preservation after selective chemoradiotherapy of rectal cancer. Interim results of the OCUM study. Chirurg 2015, 86, 1138–1144. [Google Scholar] [CrossRef] [PubMed]
- Partl, R.; Magyar, M.; Hassler, E.; Langsenlehner, T.; Kapp, K.S. Clinical parameters predictive for sphincter-preserving surgery and prognostic outcome in patients with locally advanced low rectal cancer. Radiat. Oncol. 2020, 15, 99. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Vakkila, J.; Lotze, M.T. Inflammation and necrosis promote tumour growth. Nat. Rev. Immunol. 2004, 4, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B.; Baltz, M.L. Acute phase proteins with special reference to C-reactive protein and related proteins (pentaxins) and serum amyloid A protein. Adv. Immunol. 1983, 34, 141–212. [Google Scholar]
- Nozoe, T.; Korenaga, D.; Futatsugi, M.; Saeki, H.; Maehara, Y.; Sugimachi, K. Immunohistochemical expression of C-reactive protein in squamous cell carcinoma of the esophagus-significance as a tumor marker. Cancer Lett. 2003, 192, 89–95. [Google Scholar] [CrossRef]
- Kuper, H.; Adami, H.O.; Trichopoulos, D. Infections as a major preventable cause of human cancer. J. Intern. Med. 2000, 248, 171–183. [Google Scholar] [CrossRef]
- Wahl, L.M.; Kleinman, H.K. Tumor-associated macrophages as targets for cancer therapy. J. Natl. Cancer Inst. 1998, 90, 1583–1584. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Achyut, B.R.; Bader, D.A.; Robles, A.I.; Wangsa, D.; Harris, C.C.; Ried, T.; Yang, L. Inflammation-mediated genetic and epigenetic alterations drive cancer development in the neighboring epithelium upon stromal abrogation of TGF-beta signaling. PLoS Genet. 2013, 9, e1003251. [Google Scholar] [CrossRef]
- Mazaki, J.; Katsumata, K.; Kasahara, K.; Tago, T.; Wada, T.; Kuwabara, H.; Enomoto, M.; Ishizaki, T.; Nagakawa, Y.; Tsuchida, A. Neutrophil-to-lymphocyte ratio is a prognostic factor for colon cancer: A propensity score analysis. BMC Cancer 2020, 20, 922. [Google Scholar] [CrossRef]
- Howard, R.; Kanetsky, P.A.; Egan, K.M. Exploring the prognostic value of the neutrophil-to-lymphocyte ratio in cancer. Sci. Rep. 2019, 9, 19673. [Google Scholar] [CrossRef]
- Zhou, X.; Du, Y.; Huang, Z.; Xu, J.; Qiu, T.; Wang, J.; Wang, T.; Zhu, W.; Liu, P. Prognostic value of PLR in various cancers: A meta-analysis. PLoS ONE 2014, 9, e101119. [Google Scholar] [CrossRef] [PubMed]
- Chiang, S.F.; Hung, H.Y.; Tang, R.; Changchien, C.R.; Chen, J.S.; You, Y.T.; Chiang, J.M.; Lin, J.R. Can neutrophil-to-lymphocyte ratio predict the survival of colorectal cancer patients who have received curative surgery electively? Int. J. Colorectal Dis. 2012, 27, 1347–1357. [Google Scholar] [CrossRef]
- Li, X.; Dai, D.; Chen, B.; Tang, H.; Xie, X.; Wei, W. The value of neutrophil-to-lymphocyte ratio for response and prognostic effect of neoadjuvant chemotherapy in solid tumors: A systematic review and meta-analysis. J. Cancer 2018, 9, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Seruga, B.; Ocana, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef]
- Sun, Z.; Yu, X.; Wang, H.; Ma, M.; Zhao, Z.; Wang, Q. Factors affecting sphincter-preserving resection treatment for patients with low rectal cancer. Exp. Ther. Med. 2015, 10, 484–490. [Google Scholar] [CrossRef]
- Cong, Z.J.; Hu, L.H.; Xing, J.J.; Zhang, W.; Fu, C.G.; Yu, E.D.; Zhong, M. Risk factors associated with sphincter-preserving resection in patients with low rectal cancer. Int. Surg. 2014, 99, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.T.; Heneghan, H.M.; Winter, D.C. Systematic review of outcomes after intersphincteric resection for low rectal cancer. Br. J. Surg. 2012, 99, 603–612. [Google Scholar] [CrossRef]
- Temple, L.K.; Romanus, D.; Niland, J.; Veer, A.T.; Weiser, M.R.; Skibber, J.; Wilson, J.; Rajput, A.; Benson, A.; Wong, Y.N.; et al. Factors associated with sphincter-preserving surgery for rectal cancer at national comprehensive cancer network centers. Ann. Surg. 2009, 250, 260–267. [Google Scholar] [CrossRef]
- Purves, H.; Pietrobon, R.; Hervey, S.; Guller, U.; Miller, W.; Ludwig, K. Relationship between surgeon caseload and sphincter preservation in patients with rectal cancer. Dis. Colon. Rectum. 2005, 48, 195–202; discussion 202–204. [Google Scholar] [CrossRef] [PubMed]
- De Caluwe, L.; Van Nieuwenhove, Y.; Ceelen, W.P. Preoperative chemoradiation versus radiation alone for stage II and III resectable rectal cancer. Cochrane Database Syst. Rev. 2013, 2. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Elbers, H.; Askoxylakis, V.; Motschall, E.; Bork, U.; Buchler, M.W.; Weitz, J.; Koch, M. Neoadjuvant radiotherapy for rectal cancer: Meta-analysis of randomized controlled trials. Ann. Surg. Oncol. 2013, 20, 4169–4182. [Google Scholar] [CrossRef]
- Mohiuddin, M.; Hayne, M.; Regine, W.F.; Hanna, N.; Hagihara, P.F.; McGrath, P.; Marks, G.M. Prognostic significance of postchemoradiation stage following preoperative chemotherapy and radiation for advanced/recurrent rectal cancers. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 1075–1080. [Google Scholar] [CrossRef]
- Steel, D.M.; Whitehead, A.S. Heterogeneous modulation of acute-phase-reactant mRNA levels by interleukin-1 beta and interleukin-6 in the human hepatoma cell line PLC/PRF/5. Biochem. J. 1991, 277, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Weinhold, B.; Bader, A.; Poli, V.; Ruther, U. Interleukin-6 is necessary, but not sufficient, for induction of the humanC-reactive protein gene in vivo. Biochem. J. 1997, 325, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Marnell, L.; Mold, C.; Du Clos, T.W. C-reactive protein: Ligands, receptors and role in inflammation. Clin. Immunol. 2005, 117, 104–111. [Google Scholar] [CrossRef]
- Kim, W.R.; Han, Y.D.; Min, B.S. C-Reactive Protein Level Predicts Survival Outcomes in Rectal Cancer Patients Undergoing Total Mesorectal Excision After Preoperative Chemoradiation Therapy. Ann. Surg. Oncol. 2018, 25, 3898–3905. [Google Scholar] [CrossRef]
- Singh, P.P.; Zeng, I.S.; Srinivasa, S.; Lemanu, D.P.; Connolly, A.B.; Hill, A.G. Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak after colorectal surgery. Br. J. Surg. 2014, 101, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ethier, J.L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wang, H.; Yan, A.; Wang, H.; Li, X.; Liu, J.; Li, W. Pretreatment neutrophil to lymphocyte ratio in determining the prognosis of head and neck cancer: A meta-analysis. BMC Cancer 2018, 18, 383. [Google Scholar] [CrossRef] [PubMed]
- Yodying, H.; Matsuda, A.; Miyashita, M.; Matsumoto, S.; Sakurazawa, N.; Yamada, M.; Uchida, E. Prognostic Significance of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Oncologic Outcomes of Esophageal Cancer: A Systematic Review and Meta-analysis. Ann. Surg. Oncol. 2016, 23, 646–654. [Google Scholar] [CrossRef]
- Dong, Y.W.; Shi, Y.Q.; He, L.W.; Su, P.Z. Prognostic significance of neutrophil-to-lymphocyte ratio in rectal cancer: A meta-analysis. Onco. Targets Ther. 2016, 9, 3127–3134. [Google Scholar]
- Kim, T.G.; Park, W.; Kim, H.; Choi, D.H.; Park, H.C.; Kim, S.H.; Cho, Y.B.; Yun, S.H.; Kim, H.C.; Lee, W.Y.; et al. Baseline neutrophil-lymphocyte ratio and platelet-lymphocyte ratio in rectal cancer patients following neoadjuvant chemoradiotherapy. Tumori 2019, 105, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Portale, G.; Cavallin, F.; Valdegamberi, A.; Frigo, F.; Fiscon, V. Platelet-to-Lymphocyte Ratio and Neutrophil-to-Lymphocyte Ratio Are Not Prognostic Biomarkers in Rectal Cancer Patients with Curative Resection. J. Gastrointest. Surg. 2018, 22, 1611–1618. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Zhu, Y.; Wu, W.; Zhang, L.; Ju, H.; Fan, Y.; Zhu, Y.; Luo, J.; Liu, P.; Zhou, N.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Locally Advanced Rectal Cancer Treated with Neoadjuvant Chemoradiotherapy. Med. Sci. Monit. 2017, 23, 315–324. [Google Scholar] [CrossRef]
- Pellino, G.; Gallo, G.; Pallante, P.; Capasso, R.; De Stefano, A.; Maretto, I.; Malapelle, U.; Qiu, S.; Nikolaou, S.; Barina, A.; et al. Noninvasive Biomarkers of Colorectal Cancer: Role in Diagnosis and Personalised Treatment Perspectives. Gastroenterol. Res. Pract. 2018, 2018, 2397863. [Google Scholar] [CrossRef] [PubMed]
- Thierry, A.R.; Mouliere, F.; El Messaoudi, S.; Mollevi, C.; Lopez-Crapez, E.; Rolet, F.; Gillet, B.; Gongora, C.; Dechelotte, P.; Robert, B.; et al. Clinical validation of the detection of KRAS and BRAF mutations from circulating tumor DNA. Nat. Med. 2014, 20, 430–435. [Google Scholar] [CrossRef]
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.; et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.; Pucciarelli, S.; Enzo, M.V.; Del Bianco, P.; Briarava, M.; Bedin, C.; Maretto, I.; Friso, M.L.; Lonardi, S.; Mescoli, C.; et al. Circulating cell-free DNA: A promising marker of pathologic tumor response in rectal cancer patients receiving preoperative chemoradiotherapy. Ann. Surg. Oncol. 2011, 18, 2461–2468. [Google Scholar] [CrossRef] [PubMed]
- Altomare, D.F.; Picciariello, A.; Rotelli, M.T.; De Fazio, M.; Aresta, A.; Zambonin, C.G.; Vincenti, L.; Trerotoli, P.; De Vietro, N. Chemical signature of colorectal cancer: Case-control study for profiling the breath print. BJS Open 2020, 4, 1189–1199. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | n (Missing %) | n (%) * or Median Value (Mean ± SD) |
|---|---|---|
| Sex | 363 (0%) | |
| Male | 249 (68.6%) | |
| Female | 114 (31.4%) | |
| Age (years) | 363 (0%) | |
| ≤60 | 131 (36.1%) | |
| >60 | 232 (63.9%) | |
| Smoking | 316 (12.9%) | |
| No | 268 (84.8%) | |
| Yes | 48 (15.2%) | |
| Karnofsky performance status | 234 (35.5%) | |
| ≤80% | 20 (8.5%) | |
| >80% | 214 (91.5%) | |
| Clinical T-size | 363 (0%) | |
| cT 1/2 | 23 (6.3%) | |
| cT 3 | 293 (80.7%) | |
| cT 4 | 47 (13.0%) | |
| Clinical nodal involvement | 363 (0%) | |
| cN0 | 153 (42.1%) | |
| cN+ | 210 (57.9%) | |
| Clinical stage | 363 (0%) | |
| I | 12 (3.3%) | |
| II | 141 (38.8%) | |
| III | 210 (57.9%) | |
| Histopathological subtype | 363 (0%) | |
| Adenocarcinoma | 340 (93.7%) | |
| Adenocarcinoma (mucinous) | 23 (6.3%) | |
| Tumor grade | 362 (0.6%) | |
| G1 | 24 (6.6%) | |
| G2 | 312 (86.2%) | |
| G3 | 26 (7.2%) | |
| Erythrocyte count (T/l) | 357 (1.7%) | 4.6 (4.6 ± 0.6) |
| Leucocyte count (G/l) | 358 (1.4%) | 7.2 (7.7 ± 4.6) |
| Hemoglobin | 357 (1.7%) | 13.7 (13.4 ± 1.9) |
| Thrombocyte | 358 (1.4%) | 266 (279.8 ± 92.3) |
| Absolute neutrophil value | 345 (4.9%) | 4.8 (5.1 ± 1.8) |
| Absolute lymphocyte value | 348 (4.1%) | 1.5 (1.6 ± 0.5) |
| CRP value (mg/L) | 335 (7.7%) | |
| ≤5 | 232 (69.3%) | |
| >5 | 103 (30.7%) | |
| Neutrophil-to-lymphocyte ratio | 343 (5.5%) | |
| ≤3 | 168 (46.3%) | |
| >3 | 195 (53.7%) | |
| Platelet-to-lymphocyte ratio | 347 (4.4%) | |
| <150 | 121 (34.9%) | |
| 150–300 | 191 (55.0%) | |
| >300 | 35 (10.1%) | |
| Radiation dose (fraction/total) | 363 (0%) | |
| 1.8/45 Gy | 91 (25.1%) | |
| 2/46 Gy | 272 (74.9%) | |
| Chemotherapy | 363 (0%) | |
| 5-Fluorouracil | 267 (73.6%) | |
| Capecitabine | 96 (26.4%) |
| Parameter | Sphincter Preservation, n (%) or Mean Value ± SD | Abdominoperineal Resection, n (%) or Mean Value ± SD) | p-Value |
|---|---|---|---|
| Sex | 0.167 | ||
| Male | 138 (65.7%) | 111 (72.5%) | |
| Female | 72 (34.3%) | 42 (27.5%) | |
| Age (years) | 0.007 | ||
| ≤60 | 88 (41.9%) | 43 (28.1%) | |
| >60 | 122 (58.1%) | 110 (71.9%) | |
| Smoking | 0.311 | ||
| No | 152 (83.1%) | 116 (87.2%) | |
| Yes | 31 (16.9%) | 17 (12.8%) | |
| Karnofsky performance status | 0.149 | ||
| ≤80% | 8 (6.2%) | 12 (11.5%) | |
| >80% | 122 (93.8%) | 92 (88.5%) | |
| Clinical T-size | 0.002 | ||
| cT 1–3 | 193 (91.9%) | 123 (80.4%) | |
| cT 4 | 17 (8.1%) | 30 (19.6%) | |
| Clinical nodal involvement | 0.912 | ||
| cN0 | 88 (41.9%) | 65 (42.5%) | |
| cN+ | 122 (58.1%) | 88 (57.5%) | |
| Clinical stage | 0.912 | ||
| I/II * | 88 (41.9%) | 65 (42.5%) | |
| III | 122 (58.1%) | 88 (57.5%) | |
| Histopathological subtype | 0.066 | ||
| Adenocarcinoma | 201 (95.7%) | 139 (90.8%) | |
| Adenocarcinoma (mucinous) | 9 (4.3%) | 14 (9.2%) | |
| Tumor grade | 0.054 | ||
| G1 | 16 (7.7%) | 8 (5.3%) | |
| G2 | 184 (88.0%) | 128 (84.2%) | |
| G3 | 9 (4.3%) | 16 (10.5%) | |
| Erythrocyte count (T/l) | 4.7 ± 0.5 | 4.6 ± 0.8 | 0.327 |
| Leucocyte count (G/l) | 7.8 ± 5.8 | 7.6 ± 2.3 | 0.793 |
| Hemoglobin | 13.6 ± 1.8 | 13.2 ± 1.9 | 0.040 |
| Thrombocyte | 276 ± 93 | 284 ± 90 | 0.407 |
| Absolute neutrophil value | 4.9 ± 1.7 | 5.2 ± 1.9 | 0.126 |
| Absolute lymphocyte value | 1.6 ± 0.5 | 1.6 ± 0.6 | 0.276 |
| CRP value (mg/L) | <0.001 | ||
| ≤5 | 152 (77.6%) | 80 (57.65) | |
| >5 | 44 (22.4%) | 59 (42.4%) | |
| Neutrophil-to-lymphocyte ratio | 0.061 | ||
| ≤3 | 106 (50.5%) | 62 (40.5%) | |
| >3 | 104 (49.5%) | 91 (49.5%) | |
| Platelet-to-lymphocyte ratio | 0.114 | ||
| <150 | 78 (38.6%) | 43 (29.7%) | |
| 150–300 | 108 (53.5%) | 83 (57.2%) | |
| >300 | 16 (7.9%) | 19 (13.1%) | |
| Radiation dose (fraction/total) | 0.740 | ||
| 1.8/45 Gy | 54 (25.7%) | 37 (24.2%) | |
| 2/46 Gy | 156 (74.3%) | 116(75.8%) | |
| Chemotherapy | 0.911 | ||
| 5-Fluorouracil | 154 (73.3%) | 113 (73.9%) | |
| Capecitabine | 56 (26.7%) | 40 (26.1%) |
| Parameter | OR | 95% CI | p-Value |
|---|---|---|---|
| Sex | |||
| Female | 1 | ||
| Male | 0.958 | 0.482–1.905 | 0.904 |
| Age | |||
| ≤60 | 1 | ||
| >60 | 2.475 | 1.249–4.903 | 0.009 |
| Karnofsky performance status | |||
| ≤80% | 1 | ||
| >80% | 0.556 | 0.1175–1.770 | 0.321 |
| Clinical T-size | |||
| cT 1–3 | 1 | ||
| cT 4 | 3.759 | 1.214–11.641 | 0.022 |
| Histopathological subtype | |||
| Adenocarcinoma | 1 | ||
| Adenocarcinoma (mucinous) | 2.198 | 0.624–7.741 | 0.220 |
| Tumor grade | |||
| G1 | 1 | ||
| G2 | 1.899 | 0.623–5.785 | 0.259 |
| G3 | 14.067 | 1.896–104.376 | 0.010 |
| Hemoglobin | 0.992 | 0.819–1.202 | 0.936 |
| Absolute neutrophil value | 0.875 | 0.707–1.082 | 0.218 |
| CRP value (mg/L) | |||
| ≤5 | 1 | ||
| >5 | 2.544 | 1.314–4.926 | 0.006 |
| Neutrophil-to-lymphocyte ratio | |||
| ≤3 | 1 | ||
| >3 | 1.392 | 0.647–2.994 | 0.397 |
| Platelet-to-lymphocyte ratio | |||
| <150 | 1 | ||
| 150–300 | 1.084 | 0.533–2.204 | 0.823 |
| >300 | 0.464 | 0.106–2.037 | 0.309 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Partl, R.; Lukasiak, K.; Stranz, B.; Hassler, E.; Magyar, M.; Stranzl-Lawatsch, H.; Langsenlehner, T. Can Pre-Treatment Inflammatory Parameters Predict the Probability of Sphincter-Preserving Surgery in Patients with Locally Advanced Low-Lying Rectal Cancer? Diagnostics 2021, 11, 946. https://doi.org/10.3390/diagnostics11060946
Partl R, Lukasiak K, Stranz B, Hassler E, Magyar M, Stranzl-Lawatsch H, Langsenlehner T. Can Pre-Treatment Inflammatory Parameters Predict the Probability of Sphincter-Preserving Surgery in Patients with Locally Advanced Low-Lying Rectal Cancer? Diagnostics. 2021; 11(6):946. https://doi.org/10.3390/diagnostics11060946
Chicago/Turabian StylePartl, Richard, Katarzyna Lukasiak, Bettina Stranz, Eva Hassler, Marton Magyar, Heidi Stranzl-Lawatsch, and Tanja Langsenlehner. 2021. "Can Pre-Treatment Inflammatory Parameters Predict the Probability of Sphincter-Preserving Surgery in Patients with Locally Advanced Low-Lying Rectal Cancer?" Diagnostics 11, no. 6: 946. https://doi.org/10.3390/diagnostics11060946
APA StylePartl, R., Lukasiak, K., Stranz, B., Hassler, E., Magyar, M., Stranzl-Lawatsch, H., & Langsenlehner, T. (2021). Can Pre-Treatment Inflammatory Parameters Predict the Probability of Sphincter-Preserving Surgery in Patients with Locally Advanced Low-Lying Rectal Cancer? Diagnostics, 11(6), 946. https://doi.org/10.3390/diagnostics11060946