
Watch and Wait Approach for Rectal Cancer Following Neoadjuvant Treatment: The Experience of a High Volume Cancer Center

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
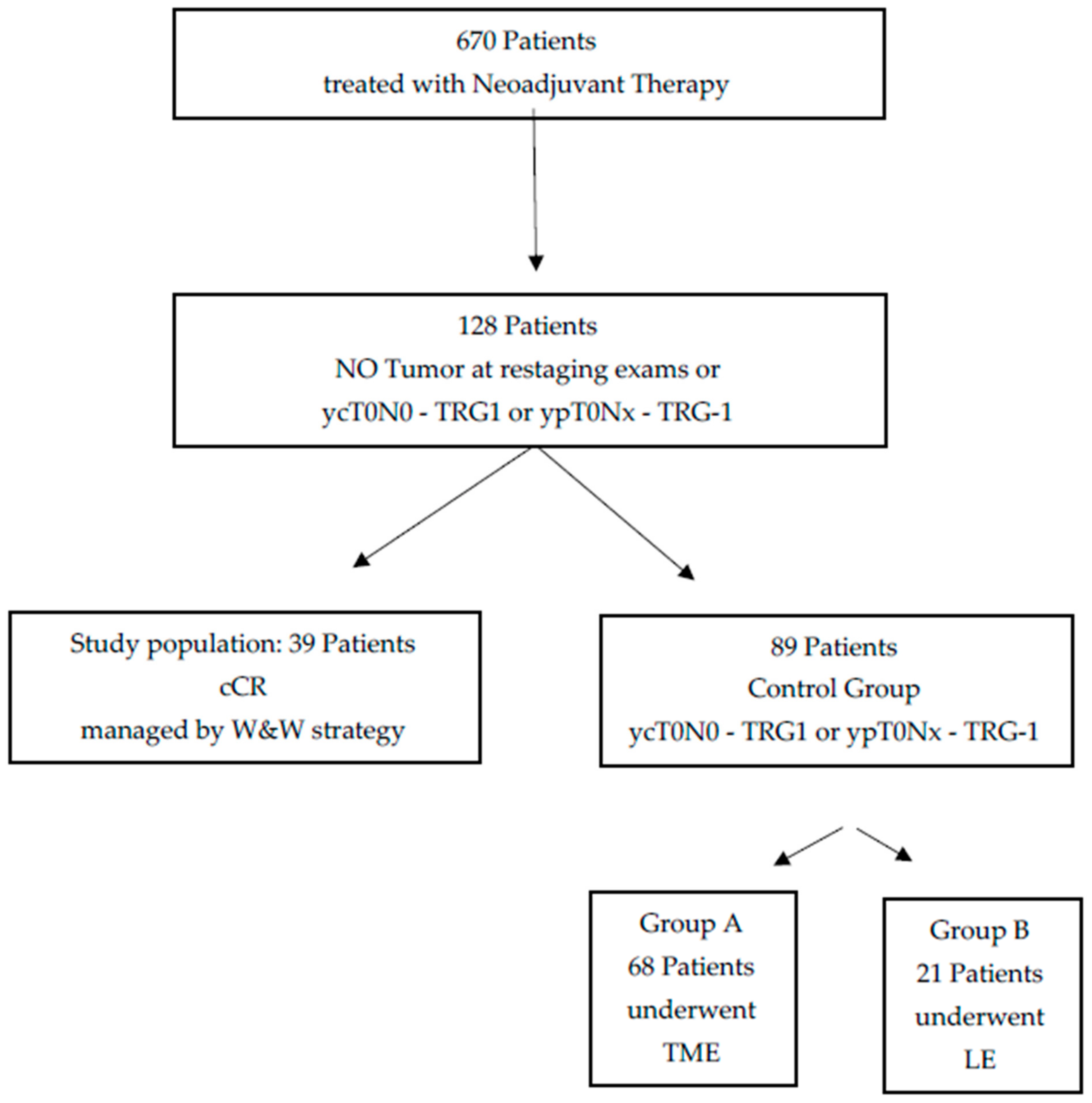
2.1. Patient Population
- (a)
- Patients with pathologically proven diagnosis of rectal cancer;
- (b)
- Patients who underwent neoadjuvant treatment such as only a short course of radiotherapy (25 Gy) or radio-chemotherapy (50 Gy with concomitant capecitabine at a daily dose of 825 mg/m2/12 h);
- (c)
- Patients who underwent digital rectal examination (DRE) and endoscopy within 15 days before treatment and who were re-evaluated after both DRE and endoscopy 8 weeks after treatment;
- (d)
- Patients who underwent magnetic resonance imaging (MRI) within 15 days before treatment and 8 weeks after the completion of neoadjuvant therapy;
- (e)
- Patients with no signs of residual tumor at restaging exams and/or histopathologic exam (ycT0N0 or ypT0—TRG1 according to Mandard [18]);
- (f)
- Patients who were followed for almost 1 year.
- (a)
- No accessible MRI and endoscopy study pre- or post-treatment;
- (b)
- Patients with residual tumor at restaging exams and/or histopathologic exam;
- (c)
- Unavailability for follow-up examination.
2.2. Clinical Assessment
2.3. MR Imaging Protocol
2.4. Image Analysis
- No fully normalized rectal wall (complete response);
- No fibrotic thickening of the wall without a residual mass (complete or near full response);
- Residual mass.
- -
- Yes (RD);
- -
- No (RD).
- -
- Mucin (or colloid degeneration) response in non-mucinous tumor;
- -
- Mucinous tumor without response.
3. Statistical Analysis
4. Results
4.1. Study Population
- -
- No palpable nodule on DRE in all patients;
- -
- No stenosis following proctoscopy in all patients;
- -
- A completely normal mucosa after proctoscopy in 16 patients;
- -
- A little (less than 2 cm of diameter) flat white scar at proctoscopy in 19 patients;
- -
- Teleangiectasias at the time of proctoscopy in 4 patients.
4.2. Control Group A
4.3. Control Group B
4.4. Statistical Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Freedman-Cass, D.A. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef] [Green Version]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017, 28 (Suppl. 4), iv22–iv40. [Google Scholar] [CrossRef] [PubMed]
- Spatola, C.; Privitera, G.; Milazzotto, R.; Tocco, A.; Acquaviva, G.; Marletta, F.; Marino, L.; Di Grazia, A.; Salvo, R.; Cartia, G.; et al. Trends in combined radio-chemotherapy for locally advanced rectal cancer: A survey among radiation oncology centers of Sicily region on behalf of AIRO. La Radiol. Med. 2019, 124, 671–681. [Google Scholar] [CrossRef]
- Tot Babberich, M.P.D.N.; van Groningen, J.T.; Dekker, E.; Wiggers, T.; Wouters, M.W.; Bemelman, W.A.; & Tanis, P.J. Laparoscopic conversion in colorectal cancer surgery; is there any improvement over time at a population level? Surg. Endosc. 2018, 32, 3234–3246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Fazio, V.W.; Zutshi, M.; Remzi, F.H.; Parc, Y.; Ruppert, R.; Fürst, A.; Celebrezze, J.; Galanduik, S.; Orangio, G.; Hyman, N.; et al. A Randomized Multicenter Trial to Compare Long-Term Functional Outcome, Quality of Life, and Complications of Surgical Procedures for Low Rectal Cancers. Ann. Surg. 2007, 246, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Guren, M.; Eriksen, M.T.; Wiig, J.; Carlsen, E.; Nesbakken, A.; Sigurdsson, H.; Wibe, A.; Tveit, K. Quality of life and functional outcome following anterior or abdominoperineal resection for rectal cancer. Eur. J. Surg. Oncol. EJSO 2005, 31, 735–742. [Google Scholar] [CrossRef]
- Maas, M.; Nelemans, P.J.; Valentini, V.; Das, P.; Rödel, C.; Kuo, L.-J.; A Calvo, F.; García-Aguilar, J.; Glynne-Jones, R.; Haustermans, K.; et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: A pooled analysis of individual patient data. Lancet Oncol. 2010, 11, 835–844. [Google Scholar] [CrossRef]
- Ryan, J.E.; Warrier, S.K.; Lynch, A.C.; Ramsay, R.; Phillips, W.; Heriot, A.G. Predicting pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer: A systematic review. Color. Dis. 2016, 18, 234–246. [Google Scholar] [CrossRef]
- Kong, J.C.; Guerra, G.R.; Warrier, S.K.; Lynch, A.C.; Michael, M.; Ngan, S.Y.; Phillips, W.; Ramsay, G.; Heriot, A.G. Prognostic value of tumour regression grade in locally advanced rectal cancer: A systematic review and meta-analysis. Color. Dis. 2018, 20, 574–585. [Google Scholar] [CrossRef]
- Rega, D.; Pecori, B.; Scala, D.; Avallone, A.; Pace, U.; Petrillo, A.; Aloj, L.; Tatangelo, F.; Delrio, P. Evaluation of Tumor Response after Short-Course Radiotherapy and Delayed Surgery for Rectal Cancer. PLoS ONE 2016, 11, e0160732. [Google Scholar] [CrossRef]
- Dattani, M.; Heald, R.J.; Goussous, G.; Broadhurst, J.; Julião, G.P.S.; Habr-Gama, A.; Perez, R.O.; Moran, B.J. Oncological and Survival Outcomes in Watch and Wait Patients With a Clinical Complete Response After Neoadjuvant Chemoradiotherapy for Rectal Cancer: A Systematic Review and Pooled Analysis. Ann. Surg. 2018, 268, 955–967. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.G.; Malcomson, L.; Emsley, R.; Gollins, S.; Maw, A.; Myint, A.S.; Rooney, P.S.; Susnerwala, S.; Blower, A.; Saunders, M.P.; et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): A propensity-score matched cohort analysis. Lancet Oncol. 2016, 17, 174–183. [Google Scholar] [CrossRef]
- Dossa, F.; Chesney, T.R.; Acuna, S.; Baxter, N.N. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 501–513. [Google Scholar] [CrossRef]
- Martens, M.H.; Maas, M.; Heijnen, L.A.; Lambregts, D.M.; Leijtens, J.W.; Stassen, L.P.; Beets, G.L. Long-term Outcome of an Organ Preservation Program After Neoadju-vant Treatment for Rectal Cancer. J. Natl. Cancer Inst. 2016, 108, djw171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karagkounis, G.; Liska, D.; Kalady, M.F. Conditional Probability of Survival after Neoadjuvant Chemo-radiation and Proctectomy for Rectal Cancer: What Matters and When. Dis Colon Rectum. 2019, 62, 33–39. [Google Scholar] [CrossRef]
- Bertocchi, E.; Barugola, G.; Nicosia, L.; Mazzola, R.; Ricchetti, F.; Dell’Abate, P.; Alongi, F.; Ruffo, G. A comparative analysis between radiation dose intensification and conventional fractionation in neoadjuvant locally advanced rectal cancer: A monocentric prospective observational study. La Radiol. Med. 2020, 125, 990–998. [Google Scholar] [CrossRef]
- Mandard, A.M.; Dalibard, F.; Mandard, J.C.; Marnay, J.; Henry-Amar, M.; Petiot, J.F.; Gignoux, M. Pathologic assessment of tumor regres-sion after preoperative chemoradiotherapy of esophageal carcinoma: Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Barina, A.; de Paoli, A.; Delrio, P.; Guerrieri, M.; Muratore, A.; Bianco, F.; Vespa, D.; Asteria, C.; Morpurgo, E.; Restivo, A.; et al. Rectal spar-ing approach after preoperative radio- and/or chemotherapy (RESARCH) in patients with rectal cancer: A multicentre ob-servational study. Tech. Coloproctol. 2017, 21, 633–640. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018, 29 (Suppl. 4), iv263. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.sirm.org/ (accessed on 1 June 2021).
- Dworak, O.; Keilholz, L.; Hoffmann, A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int. J. Colorectal. Dis. 1997, 12, 19–23. [Google Scholar] [CrossRef]
- Fusco, R.; Granata, V.; Sansone, M.; Rega, D.; Delrio, P.; Tatangelo, F.; Romano, C.; Avallone, A.; Pupo, D.; Giordano, M.; et al. Validation of the standardized index of shape tool to analyze DCE-MRI data in the assessment of neo-adjuvant therapy in locally advanced rectal cancer. La Radiol. Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Available online: www.uicc.org (accessed on 1 June 2021).
- Fischer, J.; Eglinton, T.W.; Richards, S.J.; A Frizelle, F. Predicting pathological response to chemoradiotherapy for rectal cancer: A systematic review. Expert Rev. Anticancer. Ther. 2021, 21, 489–500. [Google Scholar] [CrossRef]
- Cusumano, D.; Meijer, G.; Lenkowicz, J.; Chiloiro, G.; Boldrini, L.; Masciocchi, C.; Dinapoli, N.; Gatta, R.; Casà, C.; Damiani, A.; et al. A field strength independent MR radiomics model to predict pathological complete response in locally advanced rectal cancer. La Radiol. Med. 2021, 126, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Crimì, F.; Capelli, G.; Spolverato, G.; Bao, Q.R.; Florio, A.; Rossi, S.M.; Cecchin, D.; Albertoni, L.; Campi, C.; Pucciarelli, S.; et al. MRI T2-weighted sequences-based texture analysis (TA) as a predictor of response to neoadjuvant chemo-radiotherapy (nCRT) in patients with locally advanced rectal cancer (LARC). La Radiol. Medica 2020, 125, 1–9. [Google Scholar] [CrossRef]
- Fornell-Perez, R.; Vivas-Escalona, V.; Aranda-Sanchez, J.; Gonzalez-Dominguez, M.C.; Rubio-Garcia, J.; Aleman-Flores, P.; Loro-Ferrer, J.F. Primary and post-chemoradiotherapy MRI detection of extramural venous invasion in rectal cancer: The role of diffusion-weighted imaging. Radiol. Med. 2020, 125, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.-X.; Zhang, R.; Xiao, W.-W.; Zhang, S.; Wei, M.-B.; Li, Y.-H.; Chang, H.; Xie, W.-H.; Li, L.-R.; Ding, P.-R.; et al. The watch-and-wait strategy versus surgical resection for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy. Radiat. Oncol. 2021, 16, 1–8. [Google Scholar] [CrossRef]
- Van der Valk, M.J.M.; Hilling, D.; Bastiaannet, E.; Kranenbarg, E.M.-K.; Beets, G.L.; Figueiredo, N.; Habr-Gama, A.; O Perez, R.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): An international multicentre registry study. Lancet 2018, 391, 2537–2545. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.J.; Strombom, P.; Chow, O.S.; Roxburgh, C.S.; Lynn, P.; Eaton, A.; Widmar, M.; Ganesh, K.; Yaeger, R.; Cercek, A.; et al. Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients With a Complete Response After Neoadjuvant Therapy. JAMA Oncol. 2019, 5, e185896. [Google Scholar] [CrossRef]
- Fernandez, L.M.; Julião, G.P.S.; Figueiredo, N.L.; Beets, G.L.; van der Valk, M.J.M.; Bahadoer, R.R.; E Hilling, D.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Renehan, A.G.; et al. Conditional recurrence-free survival of clinical complete responders managed by watch and wait after neoadjuvant chemoradiotherapy for rectal cancer in the International Watch & Wait Database: A retrospective, international, multicentre registry study. Lancet Oncol. 2021, 22, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Papaccio, F.; Roselló, S.; Huerta, M.; Gambardella, V.; Tarazona, N.; Fleitas, T.; Roda, D.; Cervantes, A. Neoadjuvant Chemotherapy in Locally Advanced Rectal Cancer. Cancers 2020, 12, 3611. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, T.; Ghiringhelli, F.; Boige, V.; Le Malicot, K.; Taieb, J.; Bouché, O.; Phelip, J.M.; François, E.; Borel, C.; Faroux, R.; et al. Bevaci-zumab Maintenance Versus No Maintenance During Chemotherapy-Free Intervals in Metastatic Colorectal Cancer: A Ran-domized Phase III Trial (PRODIGE 9). J. Clin. Oncol. 2018, 36, 674–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Age, Mean (Range), Years | 66, (46–84 aa) |
|---|---|
| Sex | |
| Men | 29 |
| Women | 10 |
| Height from anal verge, mean (range), cm | 6 cm (1–12 cm) |
| Clinical tumor (T) classification | |
| T2 | 12 |
| T3 | 25 |
| T4 | 2 |
| Clinical nodal (N) classification | |
| N0 | 7 |
| N+ positive | 32 |
| Neoadjuvant regimen | |
| 50 Gy with Capecitabine | 28 |
| 25 Gy | 11 |
| Sequence | Orientation | TR/TE/FA (ms/ms/degree) | FOV (mm × mm) | Pixel Spacing | ST/Gap (mm/mm) |
|---|---|---|---|---|---|
| T1w 2D TSE | Coronal | 499/13/150 | 450 × 450 | 0.87 × 0.87 | 3/0 |
| T2w 2D TSE | Sagittal | 4820/98/150 | 250 × 250 | 0.78 × 078 | 3/0 |
| T2w 2D TSE | Axial | 3970/98/150 | 250 × 250 | 0.78 × 0.78 | 3/0 |
| SE-DW-EPI | Axial | 2700/83 | 270 × 230 | 1.70 × 1.70 | 4/0 |
| T1w FLASH 3D | Axial | 9.8/4.76/25 | 330 × 247 | 0.59 × 0.59 | 3/0 |
| T1w FLASH 3D | Axial | 9.8/4.76/25 | 330 × 247 | 0.59 × 0.59 | 3/0 |
| T1w 2D TSE | Sagittal | 538/13/150 | 250 × 250 | 0.48 × 0.48 | 3/0 |
| T1w 2D TSE | Coronal | 538/13/150 | 250 × 250 | 0.48 × 0.48 | 3/0 |
| T1w 2D TSE | Axial | 450/12/150 | 270 × 236 | 0.52 × 0.52 | 3/0 |
| Radiological Findings | ||||||||
|---|---|---|---|---|---|---|---|---|
| Radiological Response | Restricted Diffusion | EMVI Presence | Residual Lymph Nodes | Recurrence Rate | ||||
| Complete Response | Fibrotic Thickening of the Wall without a Residual Mass | Residual Mass | Diameter < 5 mm | Diameter ≥ 5 mm | ||||
| Study population N. 39) | 10/39 | 29/39 | 0/39 | 0/39 | 0/39 | 6/39 | 0/39 | 6/39 |
| Control Group A (N. 68) | 0/68 | 14/68 | 54/68 | 68/68 | 3/39 | 0/68 | 68/68 | 2/68 |
| Control Group B (N. 21) | 0/21 | 7/21 | 14/21 | 20/21 | 0/21 | 21/21 | 0/21 | 2/21 |
| p-value at chi-squared test | <0.001 | <0.001 | 0.42 | <0.001 | 0.13 | |||
| Patient | Distance from Anal Verge, cm | Initial Clinical Staging | pCRM | Neoadjuvant Treatment | Time to Regrowth | Pattern of Regrowth | Salvage Surgery | Pathology Staging | pCRM | Distant Metastases |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | T2N1 | Negative | 50 Gy + capecitabine | 30 months | Endoluminal | LAR | ypT2N0–TRG 3 | Negative | No |
| 2 | 2 | T3N1 | Negative | 50 Gy + capecitabine | 30 months | Endoluminal | LAR | ypTisN0–TRG 1 | Negative | No |
| 3 | 8 | T3N2 | Negative | 50 Gy + capecitabine | 31 months | Endoluminal | LAR | ypT2N0–TRG4 | Negative | No |
| 4 | 6 | T3N1 | Negative | 50 Gy + capecitabine | 10 months | Endoluminal | APR | ypT1N0–TRG2 | Negative | No |
| 5 | 10 | T3N1 | Negative | 25 Gy | 12 months | Endoluminal | Refused | No | ||
| 6 | 12 | T4N2 | Negative | 50 Gy + capecitabine | 12 months | Endoluminal | Refused | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rega, D.; Granata, V.; Romano, C.; D’Angelo, V.; Pace, U.; Fusco, R.; Cervone, C.; Ravo, V.; Tatangelo, F.; Avallone, A.; et al. Watch and Wait Approach for Rectal Cancer Following Neoadjuvant Treatment: The Experience of a High Volume Cancer Center. Diagnostics 2021, 11, 1507. https://doi.org/10.3390/diagnostics11081507
Rega D, Granata V, Romano C, D’Angelo V, Pace U, Fusco R, Cervone C, Ravo V, Tatangelo F, Avallone A, et al. Watch and Wait Approach for Rectal Cancer Following Neoadjuvant Treatment: The Experience of a High Volume Cancer Center. Diagnostics. 2021; 11(8):1507. https://doi.org/10.3390/diagnostics11081507
Chicago/Turabian StyleRega, Daniela, Vincenza Granata, Carmela Romano, Valentina D’Angelo, Ugo Pace, Roberta Fusco, Carmela Cervone, Vincenzo Ravo, Fabiana Tatangelo, Antonio Avallone, and et al. 2021. "Watch and Wait Approach for Rectal Cancer Following Neoadjuvant Treatment: The Experience of a High Volume Cancer Center" Diagnostics 11, no. 8: 1507. https://doi.org/10.3390/diagnostics11081507
APA StyleRega, D., Granata, V., Romano, C., D’Angelo, V., Pace, U., Fusco, R., Cervone, C., Ravo, V., Tatangelo, F., Avallone, A., Petrillo, A., & Delrio, P. (2021). Watch and Wait Approach for Rectal Cancer Following Neoadjuvant Treatment: The Experience of a High Volume Cancer Center. Diagnostics, 11(8), 1507. https://doi.org/10.3390/diagnostics11081507