
Cerebral CT Perfusion in Acute Stroke: The Effect of Lowering the Tube Load and Sampling Rate on the Reproducibility of Parametric Maps

 ,
, 
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
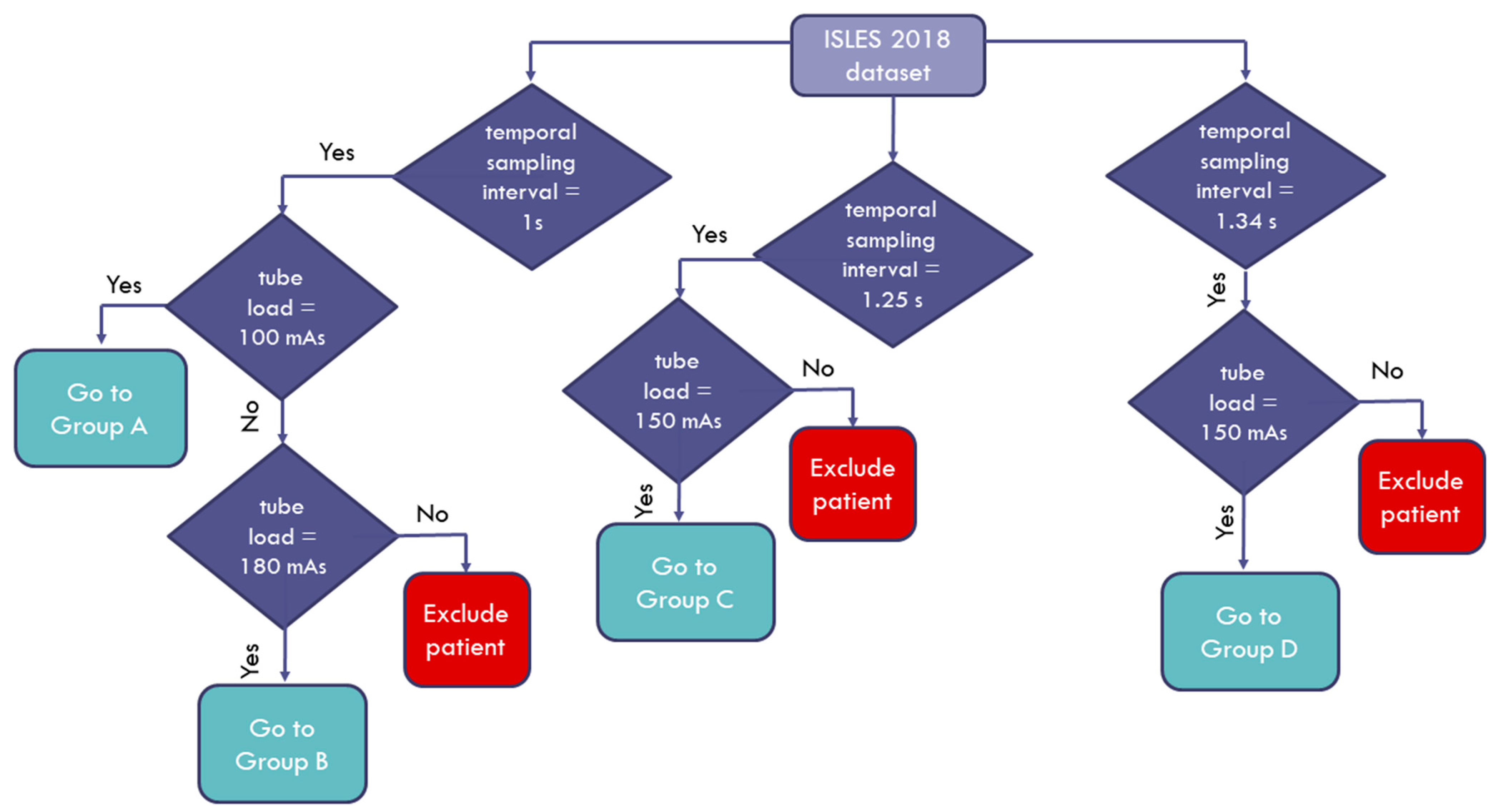
2.1. Data Description
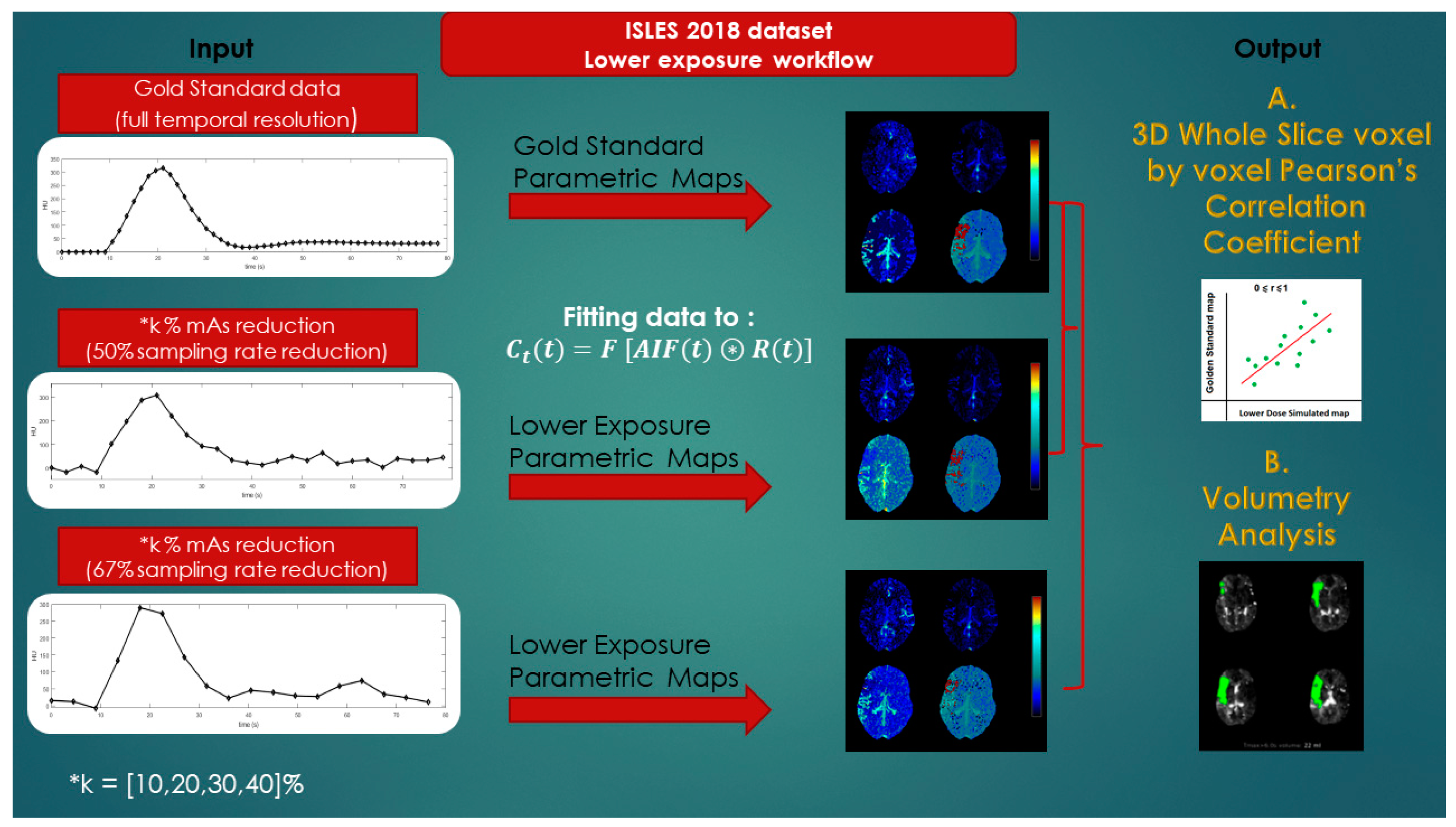
2.2. Generation of Simulated Patient Image Data Corresponding to Lower-Exposure CTP Acquisition Protocols
2.3. Quantification of Cerebral Perfusion
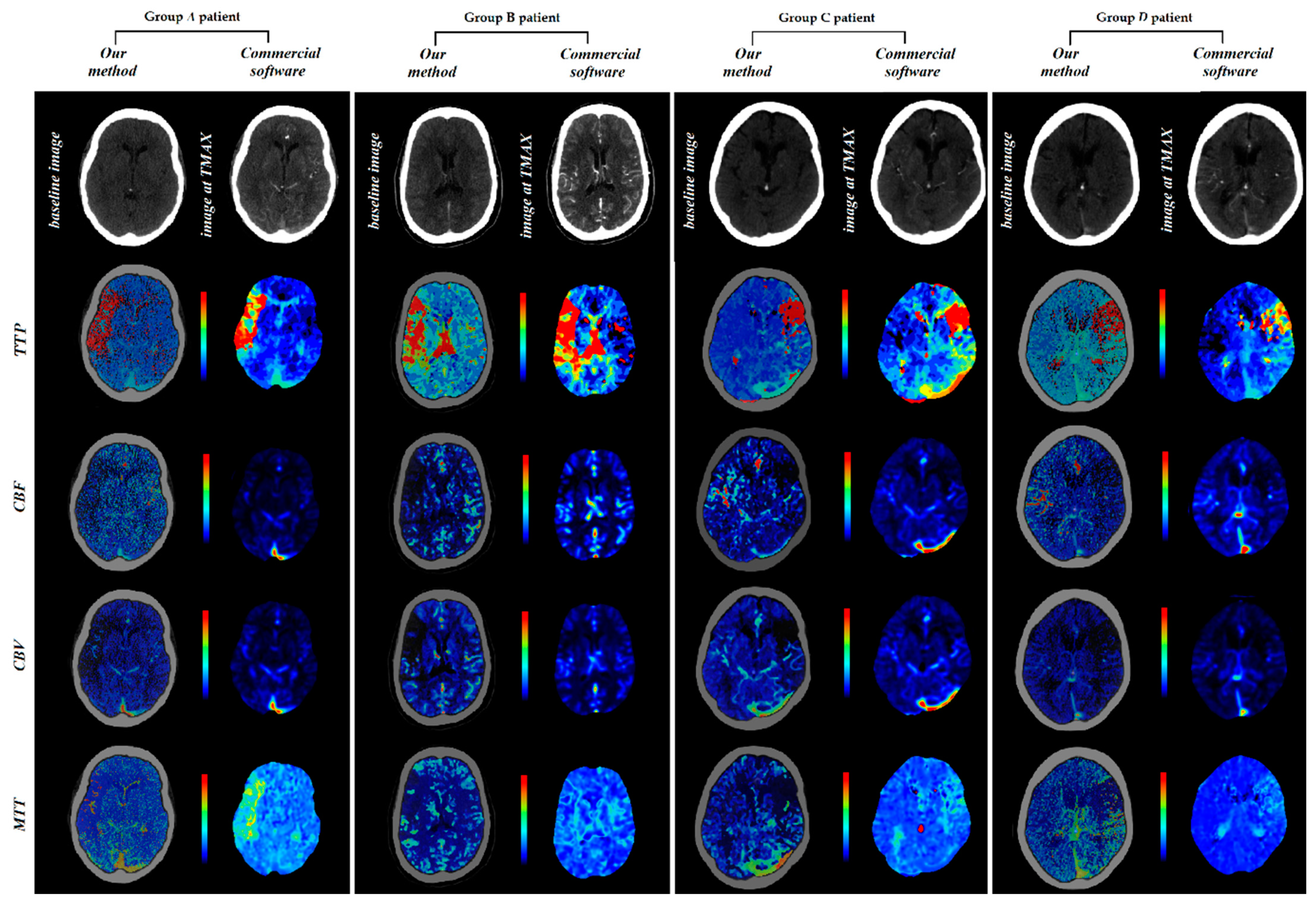
2.4. Comparison of Perfusion Parametric Maps
2.4.1. Correlation Analysis
2.4.2. Volumetric Analysis
3. Results
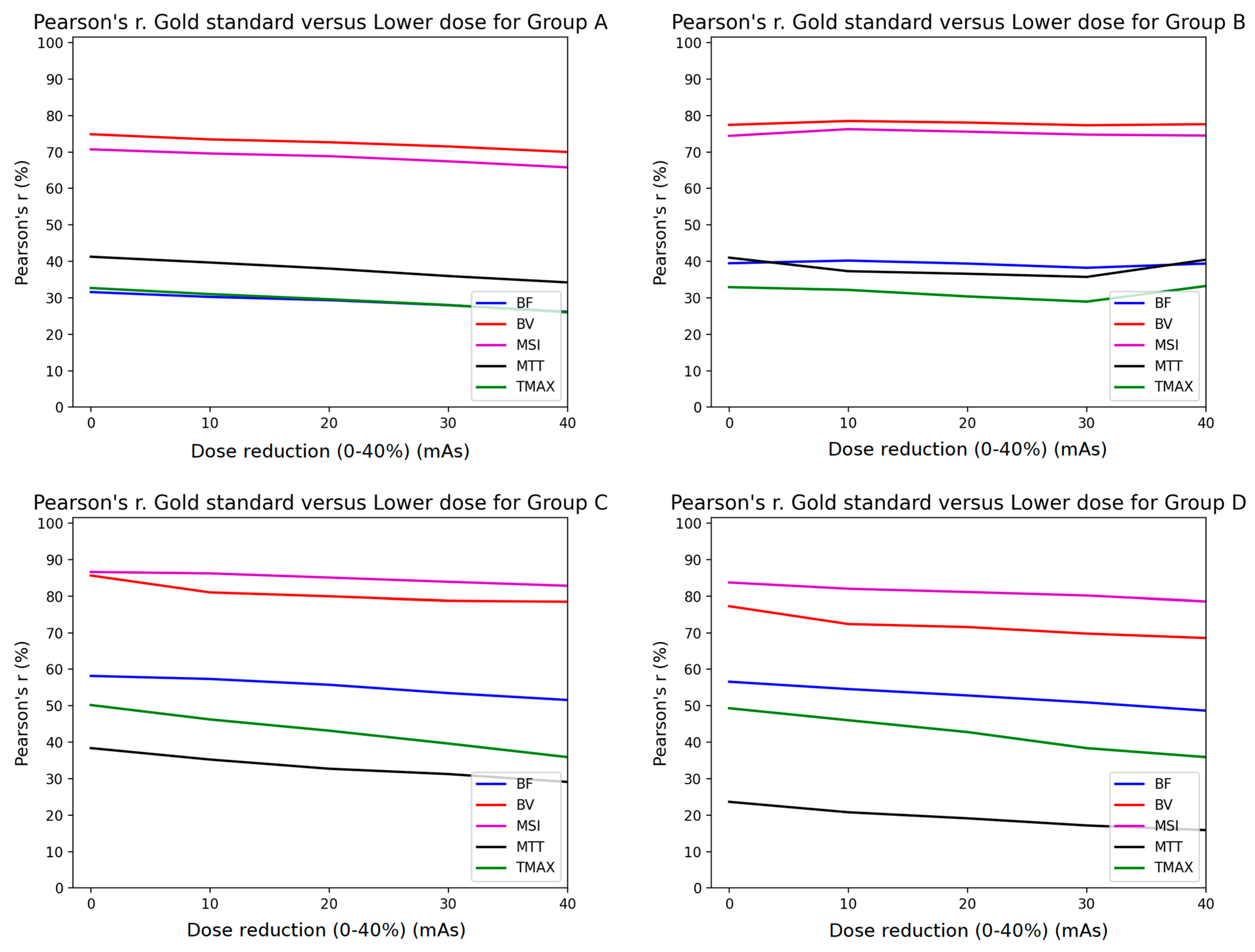
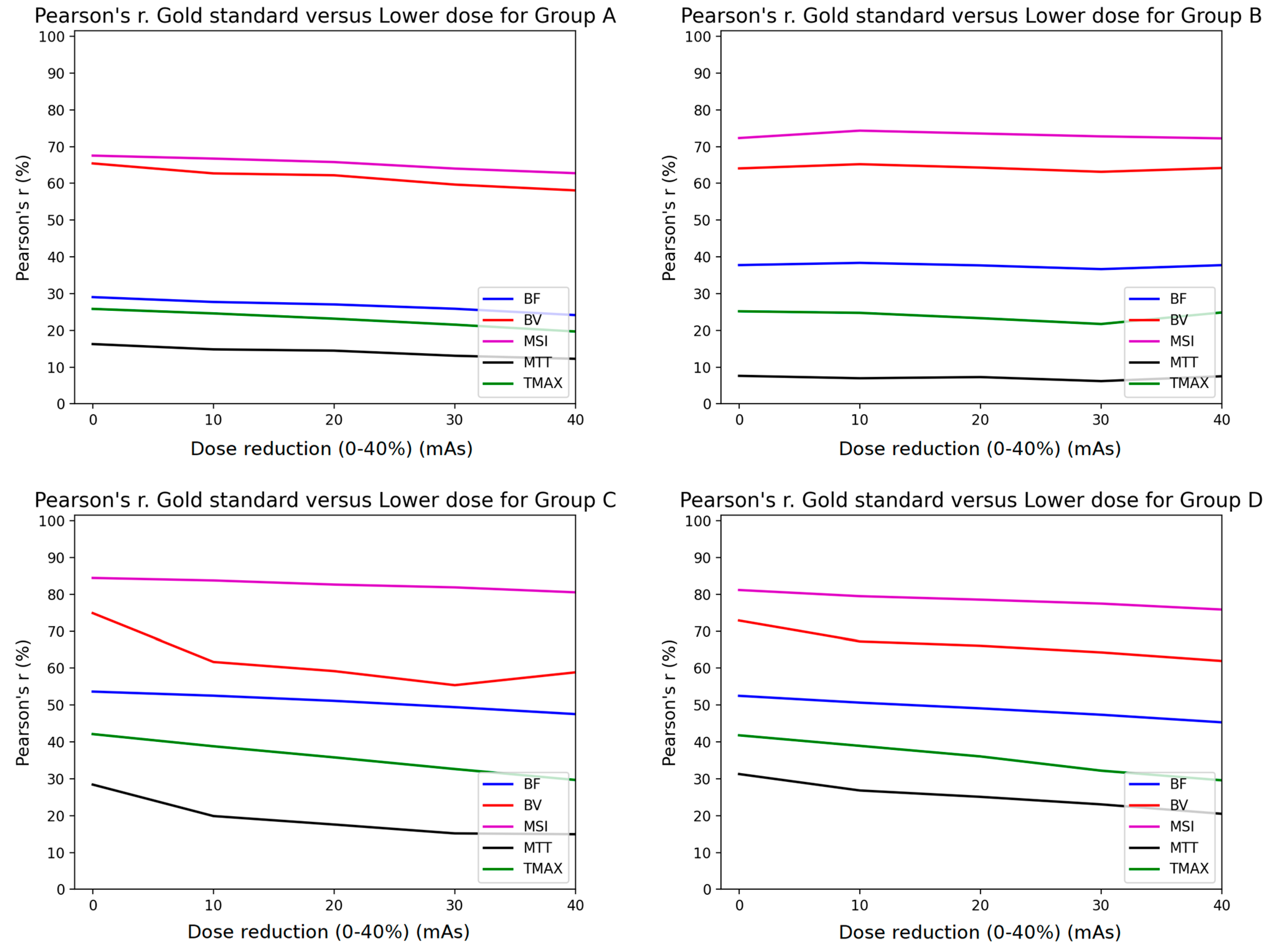
3.1. Pearson Analysis
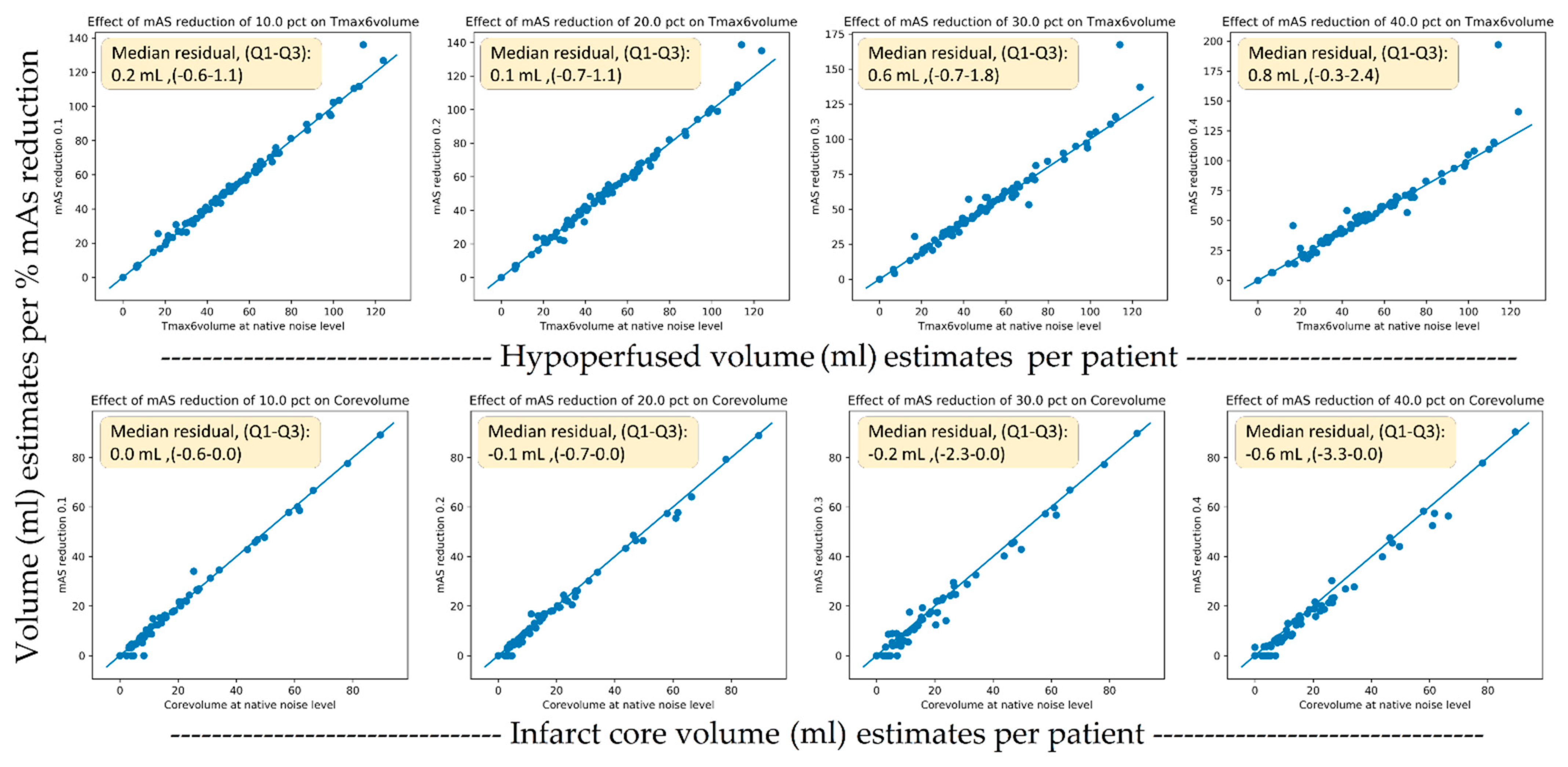
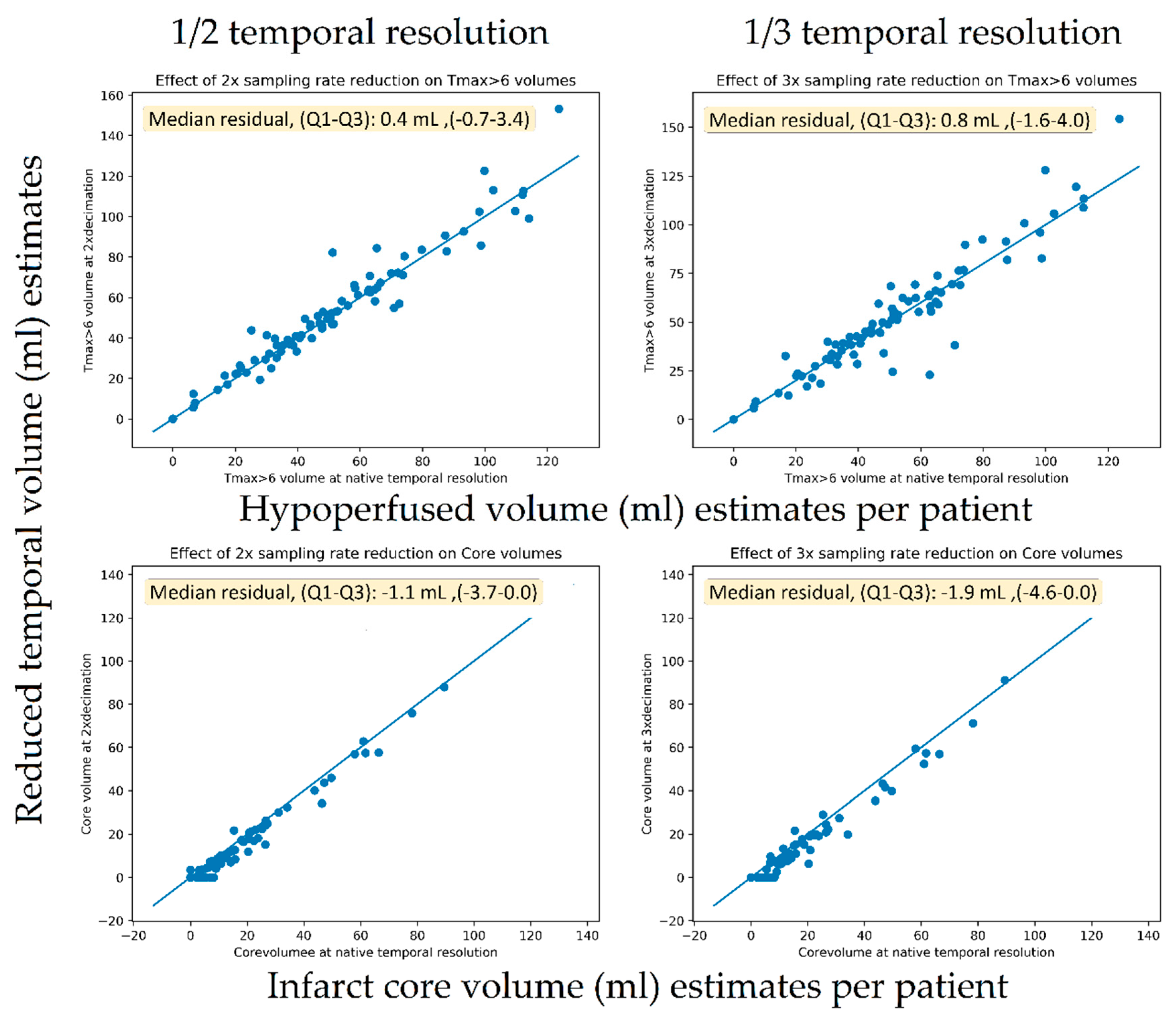
3.2. Volumetric Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIF | Arterial input function |
| ALARA | As low as reasonably achievable |
| CA | Contrast agent |
| CBF | Cerebral blood flow |
| CBV | Cerebral blood volume |
| CT | Computed tomography |
| CTP | CT perfusion |
| GSmaps | Gold standard maps |
| IQR | Interquartile range |
| MTT | Mean transit time |
| MSI | Mean slope of increase |
| ROI | Region of interest |
| TMAX | Time of maximum enhancement |
| TTP | Time to peak |
References
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; Berrington De González, A.; Miglioretti, D.L. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef]
- Žabić, S.; Wang, Q.; Morton, T.; Brown, K.M. A low dose simulation tool for CT systems with energy integrating detectors. Med. Phys. 2013, 40, 031102. [Google Scholar] [CrossRef]
- Frush, D.P.; Slack, C.C.; Hollingsworth, C.L.; Bisset, G.S.; Donnelly, L.F.; Hsieh, J.; Lavin-Wensell, T.; Mayo, J.R. Computer-simulated radiation dose reduction for abdominal multidetector CT of pediatric patients. Am. J. Roentgenol. 2002, 179, 1107–1113. [Google Scholar] [CrossRef]
- Mayo, J.R.; Whittall, K.P.; Leung, A.N.; Hartman, T.E.; Park, C.S.; Primack, S.L.; Chambers, G.K.; Limkeman, M.K.; Toth, T.L.; Fox, S.H. Simulated dose reduction in conventional chest CT: Validation study. Radiology 1997, 202, 453–457. [Google Scholar] [CrossRef]
- Amir, O.; Braunstein, D.; Altman, A. Dose optimization tool. In Proceedings of the Medical Imaging 2003: Visualization, Image-Guided Procedures, and Display, San Diego, CA, USA, 15–20 February 2003; 2003; Volume 5029, p. 815. [Google Scholar]
- Benson, T.M.; De Man, B.K.B. Synthetic CT noise emulation in the raw data domain. In Proceedings of the IEEE Nuclear Science Symposium Conference Record, Knoxville, TN, USA, 30 October–6 November 2010; pp. 3169–3171. [Google Scholar]
- Afat, S.; Brockmann, C.; Nikoubashman, O.; Müller, M.; Thierfelder, K.M.; Brockmann, M.A.; Nikolaou, K.; Wiesmann, M.; Kim, J.H.; Othman, A.E. Diagnostic accuracy of simulated low-dose perfusion CT to detect cerebral perfusion impairment after aneurysmal subarachnoid hemorrhage: A retrospective analysis. Radiology 2018, 287, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Othman, A.E.; Brockmann, C.; Yang, Z.; Kim, C.; Afat, S.; Pjontek, R.; Nikobashman, O.; Brockmann, M.A.; Kim, J.H.; Wiesmann, M. Effects of radiation dose reduction in volume perfusion CT imaging of acute ischemic stroke. Eur. Radiol. 2015, 25, 3415–3422. [Google Scholar] [CrossRef] [PubMed]
- Wintermark, M.; Smith, W.S.; Ko, N.U.; Quist, M.; Schnyder, P.; Dillon, W.P. Dynamic perfusion CT: Optimizing the temporal resolution and contrast volume for calculation of perfusion CT parameters in stroke patients. Am. J. Neuroradiol. 2004, 25, 720–729. [Google Scholar]
- Wiesmann, M.; Berg, S.; Bohner, G.; Klingebiel, R.; Schöpf, V.; Stoeckelhuber, B.M.; Yousry, I.; Linn, J.; Missler, U. Dose reduction in dynamic perfusion CT of the brain: Effects of the scan frequency on measurements of cerebral blood flow, cerebral blood volume, and mean transit time. Eur. Radiol. 2008, 18, 2967–2974. [Google Scholar] [CrossRef] [PubMed]
- Cereda, C.W.; Christensen, S.; Campbell, B.C.; Mishra, N.K.; Mlynash, M.; Levi, C.; Straka, M.; Wintermark, M.; Bammer, R.; Albers, G.W.; et al. A benchmarking tool to evaluate computer tomography perfusion infarct core predictions against a DWI standard. J. Cereb. Blood Flow Metab. 2016, 36, 1780–1789. [Google Scholar] [CrossRef]
- Maier, O.; Menze, B.H.; von der Gablentz, J.; Häni, L.; Heinrich, M.P.; Liebrand, M.; Winzeck, S.; Basit, A.; Bentley, P.; Chen, L.; et al. ISLES 2015—A public evaluation benchmark for ischemic stroke lesion segmentation from multispectral MRI. Med. Image Anal. 2017, 35, 250–269. [Google Scholar] [CrossRef]
- Winzeck, S.; Hakim, A.; McKinley, R.; Pinto, J.A.A.D.S.R.; Alves, V.; Silva, C.; Pisov, M.; Krivov, E.; Belyaev, M.; Monteiro, M.; et al. ISLES 2016 and 2017-Benchmarking Ischemic Stroke Lesion Outcome Prediction Based on Multispectral MRI. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Britten, A.J.; Crotty, M.; Kiremidjian, H.; Grundy, A.; Adam, E.J. The addition of computer simulated noise to investigate radiation dose and image quality in images with spatial correlation of statistical noise: An example application to X-ray CT of the brain. Br. J. Radiol. 2004, 77, 323–328. [Google Scholar] [CrossRef]
- Juluru, K.; Shih, J.C.; Raj, A.; Comunale, J.P.; Delaney, H.; Greenberg, E.D.; Hermann, C.; Liu, Y.B.; Hoelscher, A.; Al-Khori, N.; et al. Effects of increased image noise on image quality and quantitative interpretation in brain CT perfusion. Am. J. Neuroradiol. 2013, 34, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Primak, A.N.; McCollough, C.H.; Bruesewitz, M.R.; Zhang, J.; Fletcher, J.G. Relationship between noise, dose, and pitch in cardiac multi–detector row CT. RadioGraphics 2006, 26, 1785–1794. [Google Scholar] [CrossRef]
- Kudo, K.; Sasaki, M.; Yamada, K.; Momoshima, S.; Utsunomiya, H.; Shirato, H.; Ogasawara, K. Differences in CT perfusion maps generated by different commercial software: Quantitative analysis by using identical source data of acute stroke patients. Radiology 2010, 254, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Zussman, B.M.; Boghosian, G.; Gorniak, R.J.; Olszewski, M.E.; Read, K.M.; Siddiqui, K.M.; Flanders, A.E. The relative effect of vendor variability in CT perfusion results: A method comparison study. Am. J. Roentgenol. 2011, 197, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Cremers, C.H.P.; Dankbaar, J.W.; Vergouwen, M.D.I.; Vos, P.C.; Bennink, E.; Rinkel, G.J.E.; Velthuis, B.K.; van der Schaaf, I.C. Different CT perfusion algorithms in the detection of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Neuroradiology 2015, 57, 469–474. [Google Scholar] [CrossRef]
- Meier, P.; Zierler, K.L. On the theory of the indicator-dilution method for measurement of blood flow and volume. J. Appl. Physiol. 1954, 6, 731–744. [Google Scholar] [CrossRef]
- Konstas, A.A.; Goldmakher, G.V.; Lee, T.-Y.; Lev, M.H. Theoretic basis and technical implementations of CT perfusion in acute ischemic stroke, part 1: Theoretic basis. Am. J. Neuroradiol. 2009, 30, 662–668. [Google Scholar] [CrossRef]
- Østergaard, L.; Weisskoff, R.M.; Chesler, D.A.; Gyldensted, C.; Rosen, B.R. High resolution measurement of cerebral blood flow using intravascular tracer bolus passages. Part I: Mathematical approach and statistical analysis. Magn. Reson. Med. 1996, 36, 715–725. [Google Scholar] [CrossRef]
- Bivard, A.; Levi, C.; Spratt, N.; Parsons, M. Perfusion CT in acute stroke: A comprehensive analysis of infarct and penumbra. Radiology 2013, 267, 543–550. [Google Scholar] [CrossRef]
- Qing, Y. Method and System of Obtaining Improved Data in Perfusion Measurements. WIPO Patent Application PCT/AU2004/000821, 30 April 2004. [Google Scholar]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- Othman, A.E.; Afat, S.; Brockmann, C.; Nikoubashman, O.; Bier, G.; Brockmann, M.A.; Nikolaou, K.; Tai, J.H.; Yang, Z.P.; Kim, J.H.; et al. Low-Dose Volume-Perfusion CT of the Brain: Effects of Radiation Dose Reduction on Performance of Perfusion CT Algorithms. Clin. Neuroradiol. 2015, 27, 1–8. [Google Scholar] [CrossRef]
- Won Kim, C.; Kim, J.H. Realistic simulation of reduced-dose CT with noise modeling and sinogram synthesis using DICOM CT images. Med. Phys. 2014, 41, 011901. [Google Scholar] [CrossRef] [PubMed]
- Cross, N.M.; Deberry, J.; Ortiz, D. Demonstrations Diagnostic Quality of Machine Learning Algorithm for Optimization of Low-Dose Computed Tomography Data. SIIM 2017 Sci. Sess. Posters 2017, 5–7. Available online: https://cdn.ymaws.com/siim.org/resource/resmgr/siim2017/abstracts/posters-Cross.pdf (accessed on 18 June 2021).
- Wang, T.; Lei, Y.; Tian, Z.; Dong, X.; Liu, Y.; Jiang, X.; Curran, W.J.; Liu, T.; Shu, H.-K.; Yang, X. Deep learning-based image quality improvement for low-dose computed tomography simulation in radiation therapy. J. Med. Imaging 2019, 6, 043504. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhang, Y.; Zhang, W.; Liao, P.; Li, K.; Zhou, J.; Wang, G. Low-dose CT denoising with convolutional neural network. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 143–146. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | Group C | Group D | |
|---|---|---|---|---|
| Scanner Model | General Electric: LightSpeed VCT | General Electric: LightSpeed VCT | Philips: Mx 8000 IDT16 | Philips: Mx 8000 IDT16 |
| Scan length (cm) | 2–8 | 2–8 | 2.4–4.8 | 2.4–4.8 |
| Slice thickness (mm) | 5 | 5 | 13 | 13 |
| Tube voltage (KVp) | 80 | 80 | 90 | 90 |
| Tube current (mA) | 100 | 180 | 170 | 170 |
| Rotation time (s) | 1 | 1 | 0.88 | 0.88 |
| Tube load (mAs) | 100 | 180 | 150 | 150 |
| Temporal sampling interval (s) | 1 | 1 | 1.25 | 1.34 |
| Dynamic Scans | 50 | 45 | 35 | 35 |
| Number of patients | 19 | 14 | 17 | 40 |
| 1/2 Temporal Resolution | ||||||
|---|---|---|---|---|---|---|
| Perfusion Parameters | Original Protocol | 0% mAs Reduction | 10% mAs Reduction | 20% mAs Reduction | 30% mAs Reduction | 40% mAs Reduction |
| CBV (mL mL−1) | 0.361 | 0.739 | 0.756 | 0.759 | 0.772 | 0.779 |
| CBF (mL mL−1 s−1) | 0.199 | 0.182 | 0.187 | 0.19 | 0.194 | 0.196 |
| MTT (s) | 3.138 | 5.351 | 5.332 | 5.278 | 5.254 | 5.209 |
| MSI (HU/s) | 0.912 | 1.751 | 1.743 | 1.751 | 1.766 | 1.794 |
| TTP (s) | 20.346 | 17.796 | 17.872 | 17.831 | 17.814 | 17.664 |
| 1/3 Temporal Resolution | ||||||
| CBV (mL mL−1) | 0.361 | 1.22 | 1.323 | 1.336 | 1.379 | 1.431 |
| CBF (mL mL−1 s−1) | 0.199 | 0.199 | 0.204 | 0.205 | 0.209 | 0.211 |
| MTT (s) | 3.138 | 5.413 | 5.632 | 5.618 | 5.763 | 5.886 |
| MSI (HU/s) | 0.912 | 2.299 | 2.281 | 2.305 | 2.322 | 2.354 |
| TTP (s) | 20.346 | 18.908 | 18.979 | 18.94 | 18.92 | 18.796 |
| Parameter | 10% mAs Reduction | 20% mAs Reduction | 30% mAs Reduction | 40% mAs Reduction | 50% Sampling Rate Reduction | 67% Sampling Rate Reduction |
|---|---|---|---|---|---|---|
| Hypo perfusion lesion volume difference to original scan in mL (IQR) | 0.2 | 0.1 | 0.6 | 0.8 | 0.4 | 0.8 |
| (−0.6–1.1) | (−0.7–1.1) | (−0.7–1.8) | (−0.3–2.4) | (−0.7–3.4) | (−1.6–4.1) | |
| Core lesion volume difference to original scan in mL (IQR) | 0 | −0.1 | 0.6 | −0.2 | −1.1 | −1.9 |
| (−0.6–0.0) | (−0.7–0.0) | (−2.3–0.0) | (−3.3–0.0) | (−3.7–0.0) | (−4.6–0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannidis, G.S.; Christensen, S.; Nikiforaki, K.; Trivizakis, E.; Perisinakis, K.; Hatzidakis, A.; Karantanas, A.; Reyes, M.; Lansberg, M.; Marias, K. Cerebral CT Perfusion in Acute Stroke: The Effect of Lowering the Tube Load and Sampling Rate on the Reproducibility of Parametric Maps. Diagnostics 2021, 11, 1121. https://doi.org/10.3390/diagnostics11061121
Ioannidis GS, Christensen S, Nikiforaki K, Trivizakis E, Perisinakis K, Hatzidakis A, Karantanas A, Reyes M, Lansberg M, Marias K. Cerebral CT Perfusion in Acute Stroke: The Effect of Lowering the Tube Load and Sampling Rate on the Reproducibility of Parametric Maps. Diagnostics. 2021; 11(6):1121. https://doi.org/10.3390/diagnostics11061121
Chicago/Turabian StyleIoannidis, Georgios S., Søren Christensen, Katerina Nikiforaki, Eleftherios Trivizakis, Kostas Perisinakis, Adam Hatzidakis, Apostolos Karantanas, Mauricio Reyes, Maarten Lansberg, and Kostas Marias. 2021. "Cerebral CT Perfusion in Acute Stroke: The Effect of Lowering the Tube Load and Sampling Rate on the Reproducibility of Parametric Maps" Diagnostics 11, no. 6: 1121. https://doi.org/10.3390/diagnostics11061121
APA StyleIoannidis, G. S., Christensen, S., Nikiforaki, K., Trivizakis, E., Perisinakis, K., Hatzidakis, A., Karantanas, A., Reyes, M., Lansberg, M., & Marias, K. (2021). Cerebral CT Perfusion in Acute Stroke: The Effect of Lowering the Tube Load and Sampling Rate on the Reproducibility of Parametric Maps. Diagnostics, 11(6), 1121. https://doi.org/10.3390/diagnostics11061121