
Radiation Dose Reduction in CT Torsion Measurement of the Lower Limb: Introduction of a New Ultra-Low Dose Protocol

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Estimation of the Effective Radiation Dose
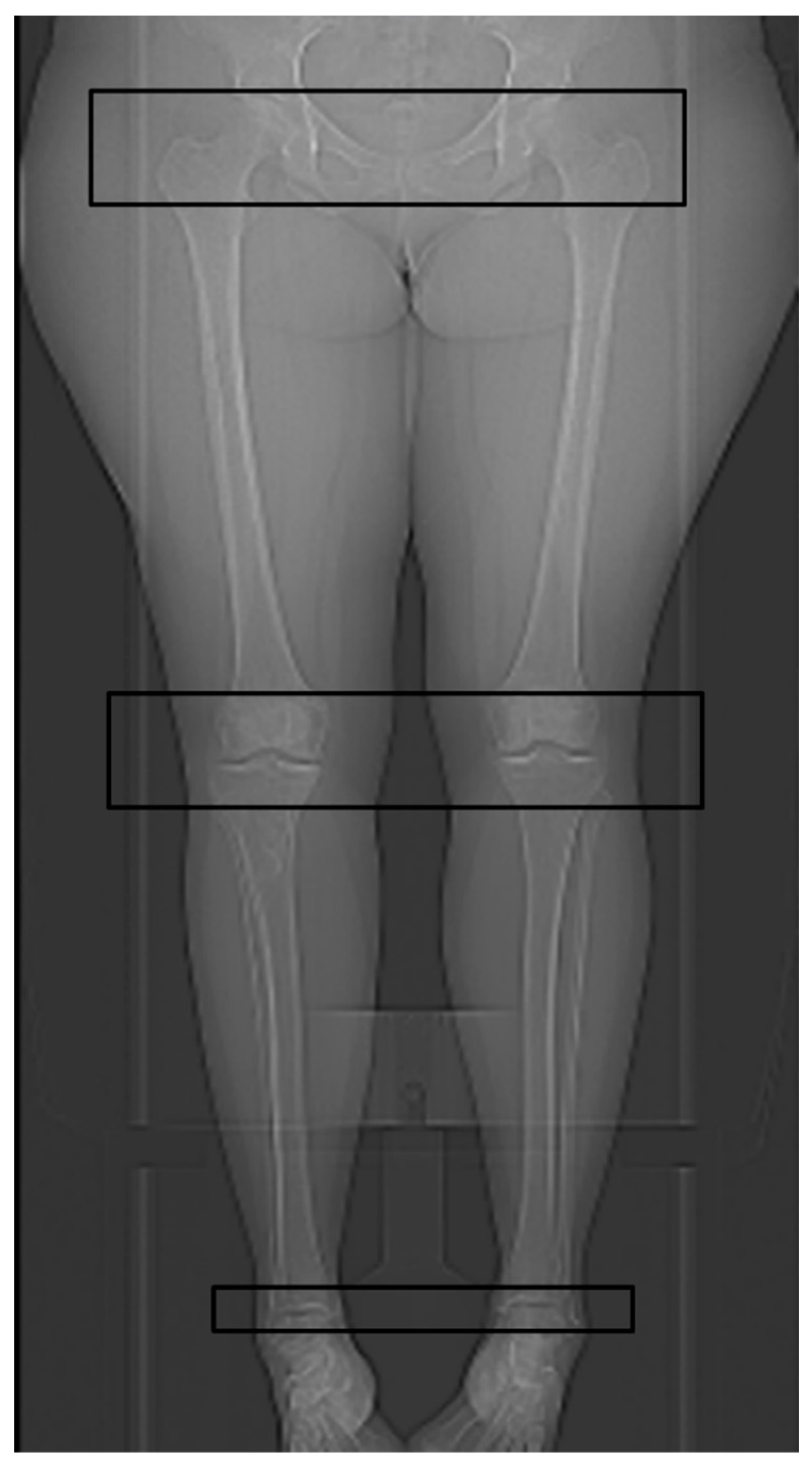
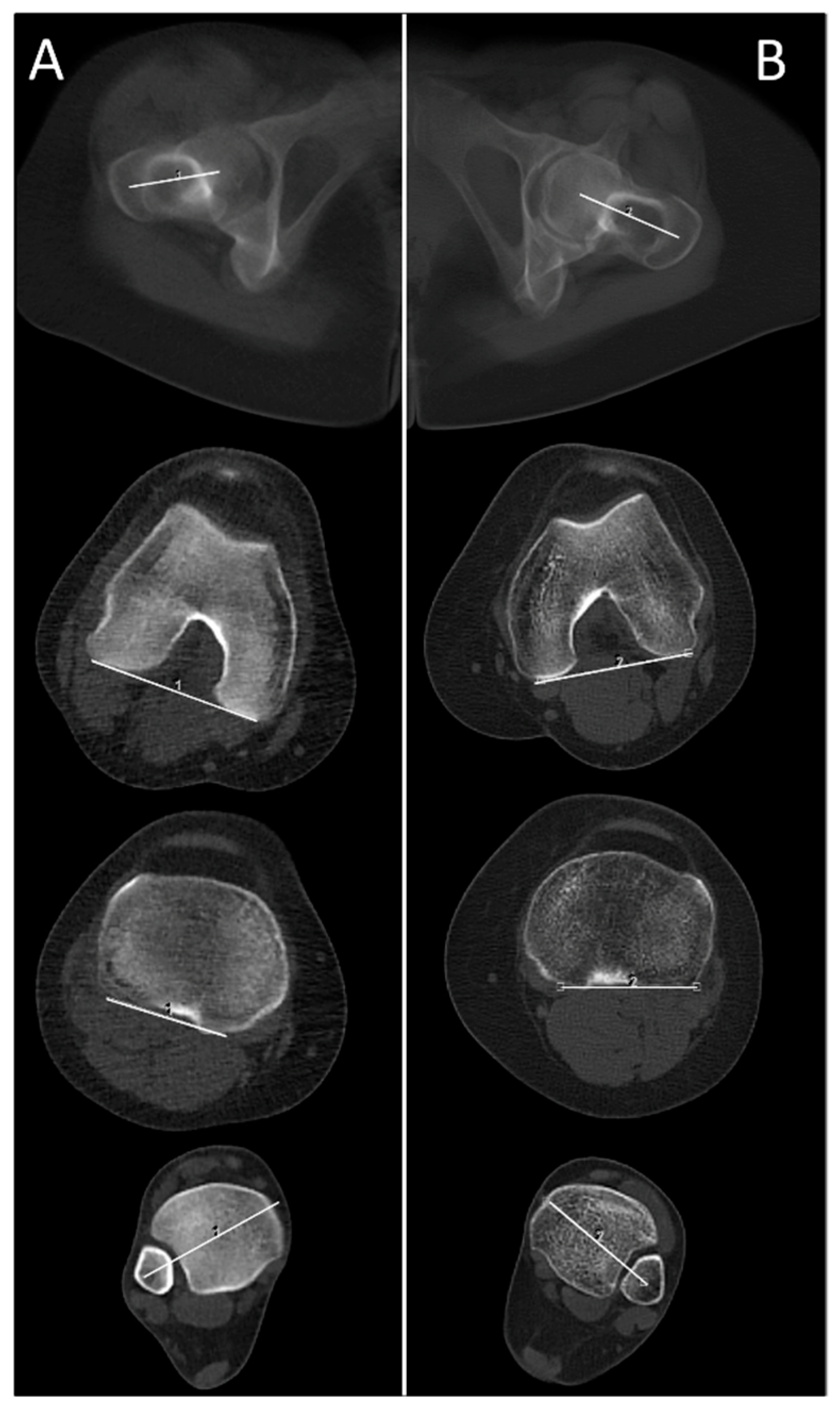
2.3. Technical Parameters of the HQ Protocol for CT Torsion Measurement of the Lower Limb
2.4. Technical Parameters of the New ULD Protocol for CT Torsion Measurement of the Lower Limb
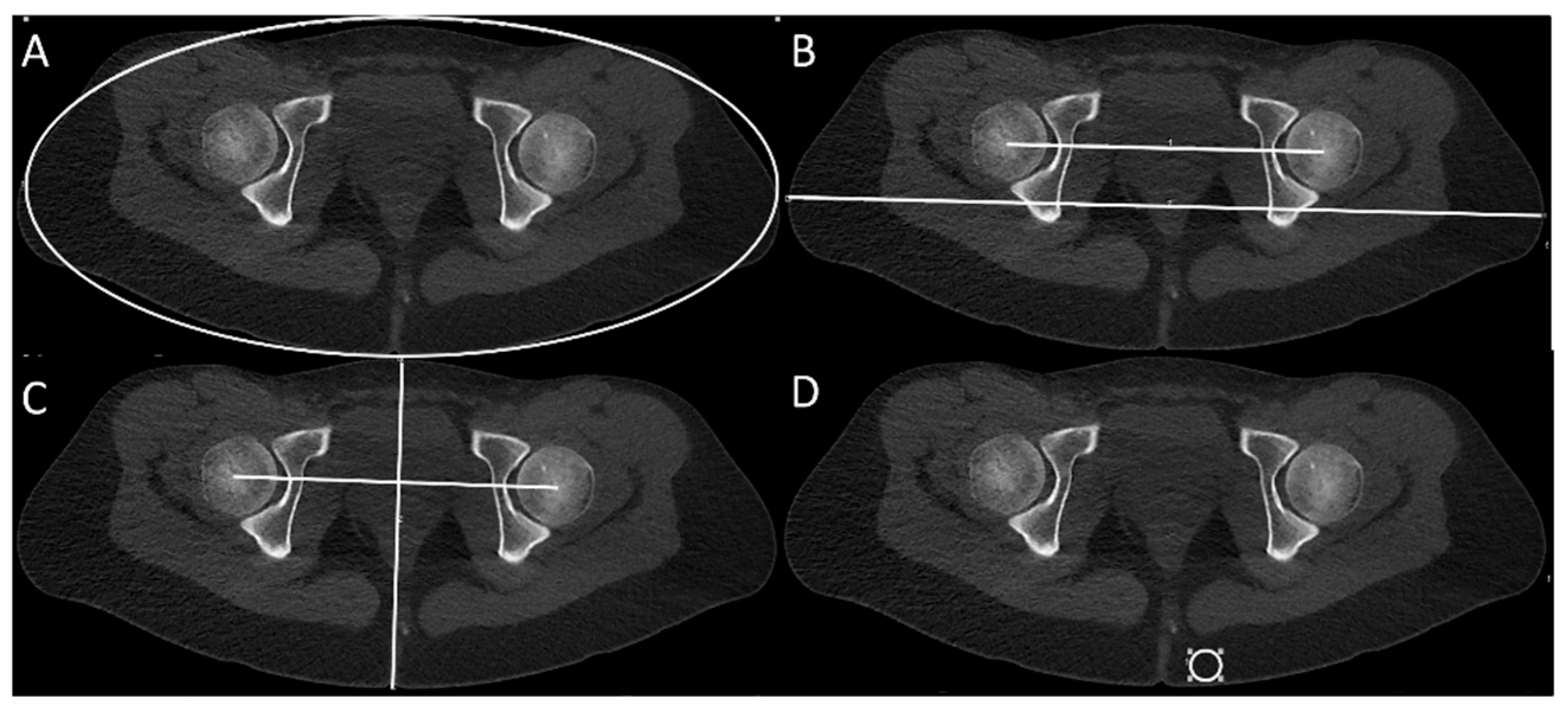
2.5. Measurement of Body Volume Parameters, CNR and DC
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations and Acronyms
| ALARA | “as low as reasonably achievable-principle” |
| AP | anterior-posterior |
| BMI | body mass index |
| CNR | contrast-to-noise ratio |
| CTDIvol | computed tomography dose index |
| DC | subjectively rated diagnostic confidence |
| DLP | dose length product |
| HQ | high-quality |
| RL | right-left |
| ROI | region of interest |
| SL | scan length |
| SOP | standard operating procedure |
| ULD | ultra-low dose |
References
- Breugem, S.J.; van Ooij, B.; Haverkamp, D.; Sierevelt, I.N.; van Dijk, C.N. No difference in anterior knee pain between a fixed and a mobile posterior stabilized total knee arthroplasty after 7.9 years. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Erkocak, O.F.; Altan, E.; Altintas, M.; Turkmen, F.; Aydin, B.K.; Bayar, A. Lower extremity rotational deformities and patellofemoral alignment parameters in patients with anterior knee pain. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3011–3020. [Google Scholar] [CrossRef]
- Karaman, O.; Ayhan, E.; Kesmezacar, H.; Seker, A.; Unlu, M.C.; Aydingoz, O. Rotational malalignment after closed intramedullary nailing of femoral shaft fractures and its influence on daily life. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Petersen, W.; Ellermann, A.; Gosele-Koppenburg, A.; Best, R.; Rembitzki, I.V.; Bruggemann, G.P.; Liebau, C. Patellofemoral pain syndrome. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2264–2274. [Google Scholar] [CrossRef] [Green Version]
- Werner, S. Anterior knee pain: An update of physical therapy. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2286–2294. [Google Scholar] [CrossRef]
- Brouwer, G.M.; van Tol, A.W.; Bergink, A.P.; Belo, J.N.; Bernsen, R.M.; Reijman, M.; Pols, H.A.; Bierma-Zeinstra, S.M. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis Rheum. 2007, 56, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Cooke, D.; Scudamore, A.; Li, J.; Wyss, U.; Bryant, T.; Costigan, P. Axial lower-limb alignment: Comparison of knee geometry in normal volunteers and osteoarthritis patients. Osteoarthr. Cartil. 1997, 5, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Eckhoff, D.G. Effect of limb malrotation on malalignment and osteoarthritis. Orthop. Clin. N. Am. 1994, 25, 405–414. [Google Scholar] [CrossRef]
- Gugenheim, J.J.; Probe, R.A.; Brinker, M.R. The effects of femoral shaft malrotation on lower extremity anatomy. J. Orthop. Trauma 2004, 18, 658–664. [Google Scholar] [CrossRef]
- Moussa, M. Rotational malalignment and femoral torsion in osteoarthritic knees with patellofemoral joint involvement. A CT scan study. Clin. Orthop. Relat. Res. 1994, 176–183. [Google Scholar]
- Sharma, L.; Song, J.; Felson, D.T.; Cahue, S.; Shamiyeh, E.; Dunlop, D.D. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA 2001, 286, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Dickschas, J.; Harrer, J.; Reuter, B.; Schwitulla, J.; Strecker, W. Torsional osteotomies of the femur. J. Orthop. Res. 2015, 33, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and natural history of acute patellar dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef]
- Jagodzinski, M.; Niemeyer, P.; Zeichen, J.; Balcarek, P. German Society for Trauma Surgery S1-Guideline: Patellar Dislocation; AWMF: Berlin, Germany, 2014. [Google Scholar]
- Grisch, D.; Dreher, T. Torsion and torsional development of the lower extremities. Orthopade 2019, 48, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.J.; Tachdjian, M.O.; Poznanski, A.K.; Dias, L.S. CT determination of femoral torsion. AJR Am. J. Roentgenol. 1981, 137, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Widjaja, P.M.; Ermers, J.W.; Sijbrandij, S.; Damsma, H.; Klinkhamer, A.C. Technique of torsion measurement of the lower extremity using computed tomography. J. Comput. Assist. Tomogr. 1985, 9, 466–470. [Google Scholar] [CrossRef]
- Berrington de Gonzalez, A.; Mahesh, M.; Kim, K.P.; Bhargavan, M.; Lewis, R.; Mettler, F.; Land, C. Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch. Intern. Med. 2009, 169, 2071–2077. [Google Scholar] [CrossRef]
- Brenner, D.J. Slowing the increase in the population dose resulting from CT scans. Radiat. Res. 2010, 174, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Kalra, M.K.; Maher, M.M.; Toth, T.L.; Hamberg, L.M.; Blake, M.A.; Shepard, J.A.; Saini, S. Strategies for CT radiation dose optimization. Radiology 2004, 230, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Mettler, J.A.; Griffin, L. Muscular endurance training and motor unit firing patterns during fatigue. Exp. Brain Res. 2016, 234, 267–276. [Google Scholar] [CrossRef]
- Keller, G.; Afat, S.; Ahrend, M.D.; Springer, F. Diagnostic accuracy of ultra-low-dose CT for torsion measurement of the lower limb. Eur. Radiol. 1007. [Google Scholar] [CrossRef]
- Alagic, Z.; Bujila, R.; Enocson, A.; Srivastava, S.; Koskinen, S.K. Ultra-low-dose CT for extremities in an acute setting: Initial experience with 203 subjects. Skeletal Radiol. 2020, 49, 531–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brink, M.; Steenbakkers, A.; Holla, M.; de Rooy, J.; Cornelisse, S.; Edwards, M.J.; Prokop, M. Single-shot CT after wrist trauma: Impact on detection accuracy and treatment of fractures. Skeletal Radiol. 2019, 48, 949–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konda, S.R.; Goch, A.M.; Leucht, P.; Christiano, A.; Gyftopoulos, S.; Yoeli, G.; Egol, K.A. The use of ultra-low-dose CT scans for the evaluation of limb fractures: Is the reduced effective dose using ct in orthopaedic injury (REDUCTION) protocol effective? Bone Joint J. 2016, 98-B, 1668–1673. [Google Scholar] [CrossRef]
- Mansfield, C.; Ali, S.; Komperda, K.; Zhao, H.; Rehman, S. Optimizing Radiation Dose in Computed Tomography of Articular Fractures. J. Orthop. Trauma 2017, 31, 401–406. [Google Scholar] [CrossRef]
- Yi, J.W.; Park, H.J.; Lee, S.Y.; Rho, M.H.; Hong, H.P.; Choi, Y.J.; Kim, M.S. Radiation dose reduction in multidetector CT in fracture evaluation. Br. J. Radiol. 2017, 90, 20170240. [Google Scholar] [CrossRef]
- Akagi, M.; Nakamura, Y.; Higaki, T.; Narita, K.; Honda, Y.; Zhou, J.; Yu, Z.; Akino, N.; Awai, K. Deep learning reconstruction improves image quality of abdominal ultra-high-resolution CT. Eur. Radiol. 2019, 29, 6163–6171. [Google Scholar] [CrossRef]
- Hong, J.H.; Park, E.A.; Lee, W.; Ahn, C.; Kim, J.H. Incremental Image Noise Reduction in Coronary CT Angiography Using a Deep Learning-Based Technique with Iterative Reconstruction. Korean J. Radiol. 2020, 21, 1165–1177. [Google Scholar] [CrossRef] [PubMed]
- Wolterink, J.M.; Leiner, T.; Viergever, M.A.; Isgum, I. Generative Adversarial Networks for Noise Reduction in Low-Dose CT. IEEE Trans. Med. Imaging 2017, 36, 2536–2545. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HQ Protocol | ULD Protocol | p-Value | |
|---|---|---|---|
| N | 30 | 30 | - |
| Age at time of CT (yrs.) # | 40.4 ± 15.9 | 38.8 ±15.8 | 0.784 |
| Gender (male/female) | 17/13 | 16/14 | 0.795 |
| BMI (kg/m2) # | 29.1 ± 5.4 | 28.7 ± 6.0 | 0.777 |
| Body area at femoral head level; (cm2) # | 738.8 ± 130.2 | 723.6 ± 131.8 | 0.515 |
| Ratio area/distance femoral heads # | 4.1 ± 0.7 | 4.1 ± 0.7 | 0.819 |
| Max. RL body diameter at femoral head level (mm) # | 388.8 ± 36.5 | 393.6 ± 31.4 | 0.344 |
| Ratio max. RL diameter/distance femoral heads # | 2.2 ± 0.3 | 2.2 ± 0.2 | 0.762 |
| max. AP body diameter at femoral head level (mm) # | 219.4 ± 28.8 | 219.3 ± 30.6 | 0.923 |
| Ratio max. AP diameter/distance femoral heads # | 1.2 ± 0.2 | 1.2 ± 0.2 | 0.900 |
| BMI (p-Value; Equational Fit) | Correlation Coefficient (r2) | |
|---|---|---|
| Body area | <0.001 (linear fit) | 0.73 |
| Ratio area/distance femoral heads | <0.001 (linear fit) | 0.74 |
| Max. RL body diameter | <0.001 (linear fit) | 0.48 |
| Ratio max. RL diameter/distance femoral heads | <0.001 (linear fit) | 0.33 |
| Max. AP body diameter | <0.001 (linear fit) | 0.77 |
| Ratio max. AP diameter/distance femoral heads | <0.001 (linear fit) | 0.67 |
| HQ Protocol | ULD Protocol | p-Value | |
|---|---|---|---|
| CNR # | 19.8 ± 3.6 | 17.6 ± 4.1 | 0.033 |
| CTDIvol hip (mGy) * | 17.1 (9.5–35.7) | 0.8 (0.6–1.5) | <0.001 |
| CTDIvol knee (mGy) * | 6.2 (3.6–13.5) | 0.2 (0.2–0.4) | <0.001 |
| CTDIvol ankle (mGy) * | 6.4 (3.8–6.5) | 0.2 (0.2–0.2) | <0.001 |
| DLP hip (mGycm) * | 279.5 (125–596) | 10 (7–20) | <0.001 |
| DLP knee (mGycm) * | 98.5 (48–219) | 2.5 (2–5) | <0.001 |
| DLP ankle (mGycm) * | 78 (43–104) | 2 (1–2) | <0.001 |
| DLP total (mGycm) * | 457 (251–851) | 15 (11–26) | <0.001 |
| mSv hip * | 3.79 (1.44–11.7) | 0.15 (0.08–0.69) | <0.001 |
| mSv knee * | 0.90 (0.03–2.76) | 0.03 (<0.01–0.11) | <0.001 |
| mSv ankle * | 0.05 (0.01–0.07) | <0.01 (<0.01–<0.01) | <0.001 |
| mSv total * | 4.37 (2.09–13.15) | 0.17 (0.08–0.80) | <0.001 |
| Tube Voltage HQ Protocol | Tube Voltage ULD Protocol | Tube Current HQ Protocol | Tube Current ULD Protocol | |
|---|---|---|---|---|
| Hip | 120 kV | 26 × 100 kV 4 × 120 kV | 292.4 ± 110.6 mAs | 100 kV: 20 (14–27) mAs 120 kV: 21 (19–24) mAs |
| Knee | 120 kV | 80 kV | 95.0 mAs | 9 (9–20) mAs |
| Ankle | 120 kV | 80 kV | 95.0 mAs | 10 (10–10) mAs |
| HQ Protocol | ULD Protocol | p-Value | |
|---|---|---|---|
| SL hip * | 14.9 (12.8–24.6) | 13.5 (10.8–17.0) | <0.001 |
| SL knee * | 16.1 (11.5–26.3) | 12.0 (11.1–22.2) | 0.019 |
| SL ankle * | 12.2 (9.4–16.3) | 11.1 (5.6–11.1) | <0.001 |
| SL total * | 42.9 (35.5–57.4) | 36.4 (27.5–44.6) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keller, G.; Götz, S.; Kraus, M.S.; Grünwald, L.; Springer, F.; Afat, S. Radiation Dose Reduction in CT Torsion Measurement of the Lower Limb: Introduction of a New Ultra-Low Dose Protocol. Diagnostics 2021, 11, 1209. https://doi.org/10.3390/diagnostics11071209
Keller G, Götz S, Kraus MS, Grünwald L, Springer F, Afat S. Radiation Dose Reduction in CT Torsion Measurement of the Lower Limb: Introduction of a New Ultra-Low Dose Protocol. Diagnostics. 2021; 11(7):1209. https://doi.org/10.3390/diagnostics11071209
Chicago/Turabian StyleKeller, Gabriel, Simon Götz, Mareen Sarah Kraus, Leonard Grünwald, Fabian Springer, and Saif Afat. 2021. "Radiation Dose Reduction in CT Torsion Measurement of the Lower Limb: Introduction of a New Ultra-Low Dose Protocol" Diagnostics 11, no. 7: 1209. https://doi.org/10.3390/diagnostics11071209
APA StyleKeller, G., Götz, S., Kraus, M. S., Grünwald, L., Springer, F., & Afat, S. (2021). Radiation Dose Reduction in CT Torsion Measurement of the Lower Limb: Introduction of a New Ultra-Low Dose Protocol. Diagnostics, 11(7), 1209. https://doi.org/10.3390/diagnostics11071209