
4D Doppler Ultrasound in High Grade Serous Ovarian Cancer Vascularity Evaluation—Preliminary Study

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alcázar, J.L.; Guerriero, S.; Laparte, C.; Ajossa, S.; Jurado, M. Contribution of power Doppler blood flow mapping to gray-scale ultrasound for predicting malignancy of adnexal masses in symptomatic and asymptomatic women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 155, 99–105. [Google Scholar] [CrossRef]
- Alcázar, J.L.; Prka, M. Evaluation of two different methods for vascular sampling by three-dimensional power Doppler angi-ography in solid and cystic-solid adnexal masses. Ultrasound Obstet. Gynecol. 2009, 33, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, S.; Saba, L.; Alcazar, J.L.; Pascual, M.A.; Ajossa, S.; Perniciano, M.; Piras, A.; Sedda, F.; Peddes, C.; Fabbri, P.; et al. Past, present and future ultrasonographic techniques for analyzing ovarian masses. Women’s Health 2015, 11, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Sladkevicius, P.; Jokubkiene, L.; Timmerman, D.; Fischerova, D.; Van Holsbeke, C.; Franchi, D.; Savelli, L.; Epstein, E.; Fruscio, R.; Kaijser, J.; et al. Vessel morphology depicted by three-dimensional power Doppler ultrasound as second-stage test in adnexal tumors that are difficult to classify: Prospective diagnostic accuracy study. Ultrasound Obstet. Gynecol. 2021, 57, 324–334. [Google Scholar] [CrossRef]
- Silvestre, L.; Martins, W.P.; Candido-Dos-Reis, F.J. Limitations of three-dimensional power Doppler angiography in preoperative evaluation of ovarian tumors. J. Ovarian Res. 2015, 8, 47. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Utrilla-Layna, J.; Alcázar, J.L.; Aubá, M.; Laparte, C.; Olartecoechea, B.; Errasti, T.; Juez, L.; Mínguez, J.Á.; Guerriero, S.; Jurado, M. Performance of three-dimensional power Doppler angiography as third-step assessment in differential diagnosis of adnex-al masses. Ultrasound Obstet. Gynecol. 2015, 45, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Jurado, M. Three-dimensional ultrasound for assessing women with gynecological cancer: A systematic review. Gynecol. Oncol. 2011, 120, 340–346. [Google Scholar] [CrossRef]
- Kudla, M.J.; Timor-Tritsch, I.E.; Hope, J.M.; Monteagudo, A.; Popiolek, D.; Monda, S.; Lee, C.J.; Arslan, A.A. Spherical tissue sampling in 3-dimensional power Doppler angiography: A new approach for evaluation of ovarian tumors. J. Ultrasound Med. 2008, 27, 425–433. [Google Scholar] [CrossRef]
- Meys, E.M.; Kaijser, J.; Kruitwagen, R.F.; Slangen, B.F.; Van Calster, B.; Aertgeerts, B.; Verbakel, J.Y.; Timmerman, D.; Van Gorp, T. Sub-jective assessment versus ultrasound models to diagnose ovarian cancer: A systematic review and meta-analysis. Eur. J. Cancer 2016, 58, 17–29. [Google Scholar] [CrossRef]
- Sladkevicius, P.; Valentin, L. Interobserver agreement in describing the ultrasound appearance of adnexal masses and in calcu-lating the risk of malignancy using logistic regression models. Clin. Cancer Res. 2015, 21, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Kudla, M.J.; Alcázar, J.L. Spatiotemporal image correlation using high-definition flow: A new method for assessing ovarian vascularization. J. Ultrasound Med. 2010, 29, 1469–1474. [Google Scholar] [CrossRef]
- Martins, W.P.; Welsh, A.W.; Lima, J.C.; Nastri, C.O.; Raine-Fenning, N.J. The “volumetric” pulsatility index as evaluated by spatio-temporal imaging correlation (STIC): A preliminary description of a novel technique, its application to the endometrium and an evaluation of its reproducibility. Ultrasound Med. Biol. 2011, 37, 2160–2168. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ameye, L.; Jurkovic, D.; Van Holsbeke, C.; Paladini, D.; Van Calster, B.; Vergote, I.; Van Huffel, S.; et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet. Gynecol. 2008, 31, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Kudla, M.J.; Kandzia, T.; Alcázar, J.L. Comparison of two methods for calculating the mean vascularization index of ovarian stroma on the basis of spatio-temporal image correlation high-definition flow technology. Ultrasound Med. Biol. 2013, 39, 2202–2204. [Google Scholar] [CrossRef]
- Polanski, L.T.; Baumgarten, M.N.; Brosens, J.J.; Quenby, S.M.; Campbell, B.K.; Martins, W.P.; Raine-Fenning, N.J. 4-D assessment of en-dometrial vascularity using spatiotemporal image correlation: A study comparing spherical sampling and whole-tissue analysis. Ultrasound Med. Biol. 2015, 41, 2798–2805. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xuan, Z.; Wang, Y. Diagnostic value of ultrasound score, color Doppler ultrasound RI and spiral CT for ovarian tumors. Oncol. Lett. 2019, 17, 5499–5504. [Google Scholar] [CrossRef]
- Alcázar, J.L. Tumor angiogenesis assessed by three-dimensional power Doppler ultrasound in early, advanced and metastatic ovarian cancer: A preliminary study. Ultrasound Obstet. Gynecol. 2006, 28, 325–329. [Google Scholar] [CrossRef]
- Timmerman, D.; Van Calster, B.; Testa, A.; Savelli, L.; Fischerova, D.; Froyman, W.; Wynants, L.; Van Holsbeke, C.; Epstein, E.; Franchi, D.; et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am. J. Obstet. Gynecol. 2016, 214, 424–437. [Google Scholar] [CrossRef]
- Jokubkiene, L.; Sladkevicius, P.; Valentin, L. Does three-dimensional power Doppler ultrasound help in discrimination between benign and malignant ovarian masses? Ultrasound Obstet. Gynecol. 2007, 29, 215–225. [Google Scholar] [CrossRef]
- Alcázar, J.L.; Kudla, M.J. Ovarian stromal vessels assessed by spatiotemporal image correlation-high definition flow in women with polycystic ovary syndrome: A case-control study. Ultrasound Obstet. Gynecol. 2012, 40, 470–475. [Google Scholar] [CrossRef]
- Miyague, A.H.; Pavan, T.Z.; Grillo, F.W.; Teixeira, D.M.; Nastri, C.O.; Martins, W.P. Influence of attenuation on three-dimensional power Doppler indices and STIC volumetric pulsatility index: A flow phantom experiment. Ultrasound Obstet. Gynecol. 2014, 43, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Miyague, A.H.; Pavan, T.Z.; Soares, C.A.; De Catte, L.; Nastri, C.O.; Welsh, A.W.; Martins, W.P. Importance of pulse repetition fre-quency adjustment for 3- and 4-dimensional power doppler quantification. J. Ultrasound Med. 2015, 34, 2245–2251. [Google Scholar] [CrossRef]
- Miyague, A.; Rainne-Fenning, N.; Polanski, L.; Martinez, L.; Junior, E.; Pavan, T.; Martins, W. Assessing the repeatability of 3D doppler indices obtained by static 3D and stic power doppler: A combined in vitro/in vivo flow phantom study. Ultrasound Med. Biol. 2013, 39, S31. [Google Scholar] [CrossRef]
- Soares, C.A.; Pavan, T.Z.; Miyague, A.H.; Kudla, M.; Martins, W.P. Influence of pulse repetition frequency on 3-D power doppler quantification. Ultrasound Med. Biol. 2016, 42, 2887–2892. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.R.; Martins, W.P.; Soares, C.A.M.; Miyague, A.H.; Kudla, M.J.; Pavan, T.Z. Understanding the influence of flow velocity, wall motion filter, pulse repetition frequency, and aliasing on power doppler image quantification. J. Ultrasound Med. 2018, 37, 255–261. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, J.M.; Kim, Y.J.; Lee, J.Y.; Han, J.K.; Choi, B.I. High-definition flow Doppler ultrasonographic technique to assess hepatic vasculature compared with color or power Doppler ultrasonography: Preliminary experience. J. Ultrasound Med. 2008, 27, 1491–1501. [Google Scholar] [CrossRef]
- Kudla, M.J.; Alcazar, J.L. Does sphere volume affect the performance of three-dimensional power Doppler virtual vascular sampling for predicting malignancy in vascularized solid or cystic-solid adnexal masses? Ultrasound Obstet. Gynecol. 2010, 35, 602–608. [Google Scholar] [CrossRef]
- Martins, W.P.; Raine-Fenning, N.J.; Ferriani, R.A.; Nastri, C.O. Quantitative three-dimensional power Doppler angiography: A flow-free phantom experiment to evaluate the relationship between color gain, depth and signal artifact. Ultrasound Obstet. Gynecol. 2010, 35, 361–368. [Google Scholar] [CrossRef]
- Hildreth, K.L.; Ozemek, C.; Kohrt, W.M.; Blatchford, P.J.; Moreau, K.L. Vascular dysfunction across the stages of the menopausal transition is associated with menopausal symptoms and quality of life. Menopause 2018, 25, 1011–1019. [Google Scholar] [CrossRef]
- Moreau, K.L.; Hildreth, K.L.; Meditz, A.L.; Deane, K.D.; Kohrt, W.M. Endothelial function is impaired across the stages of the menopause transition in healthy women. J. Clin. Endocrinol. Metab. 2012, 97, 4692–4700. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
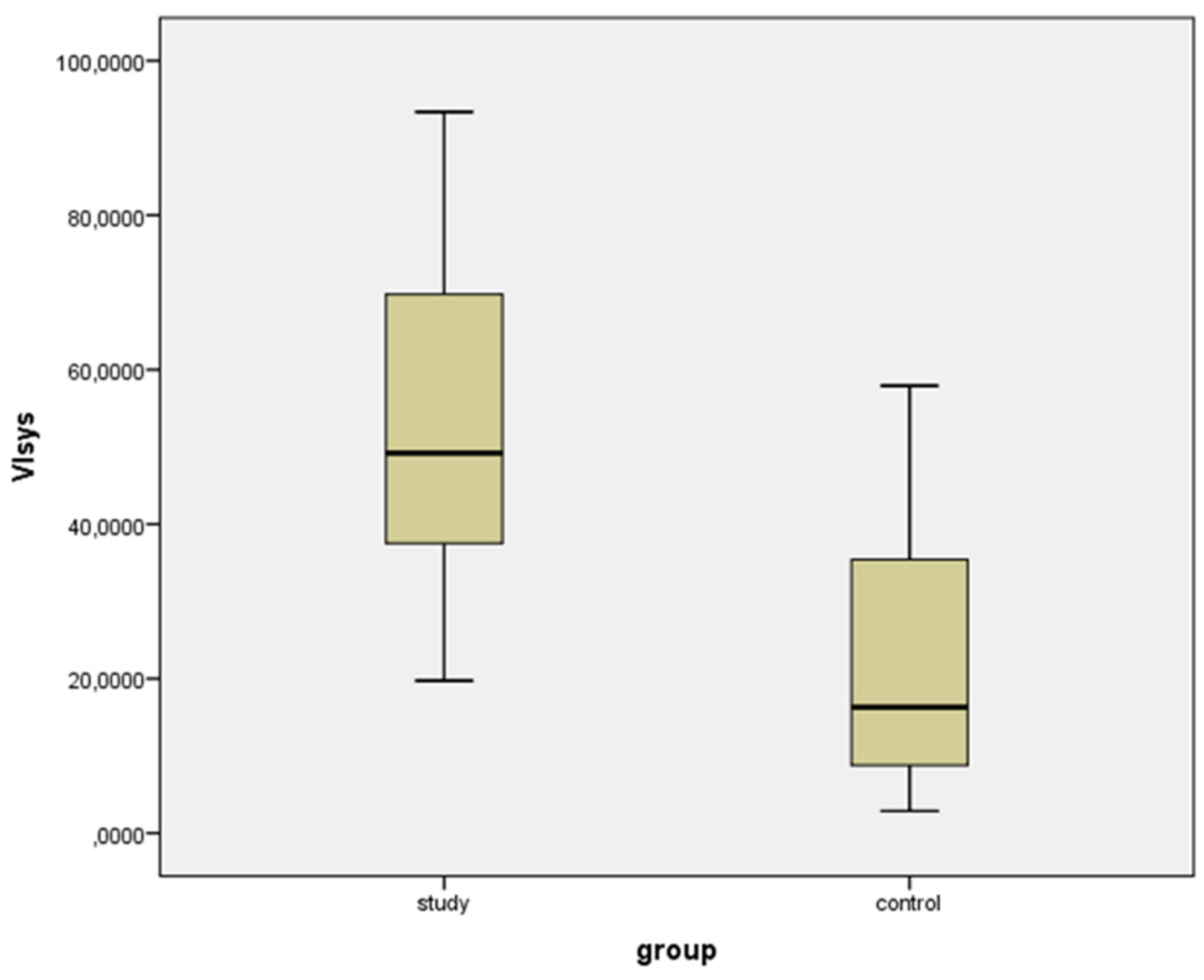
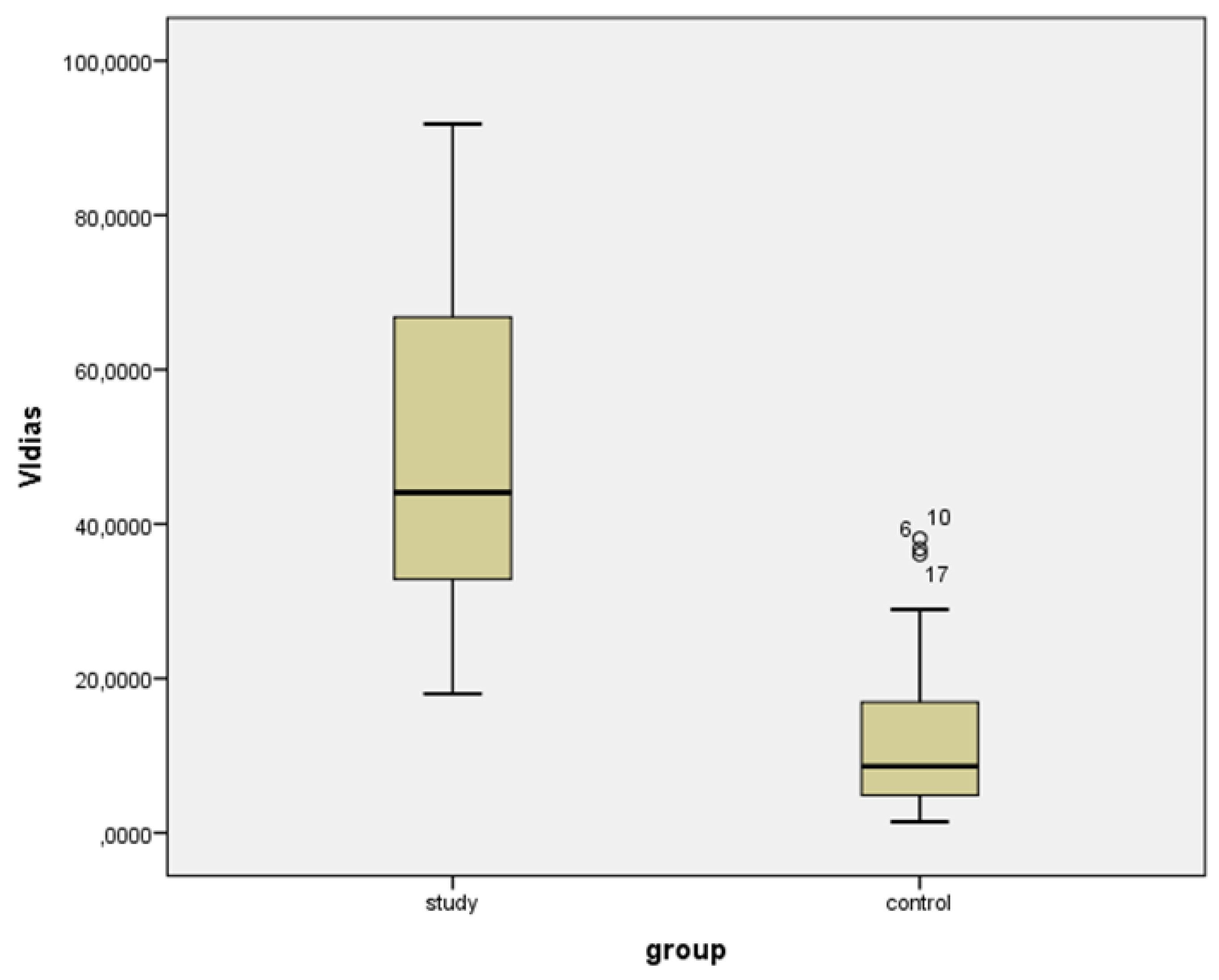
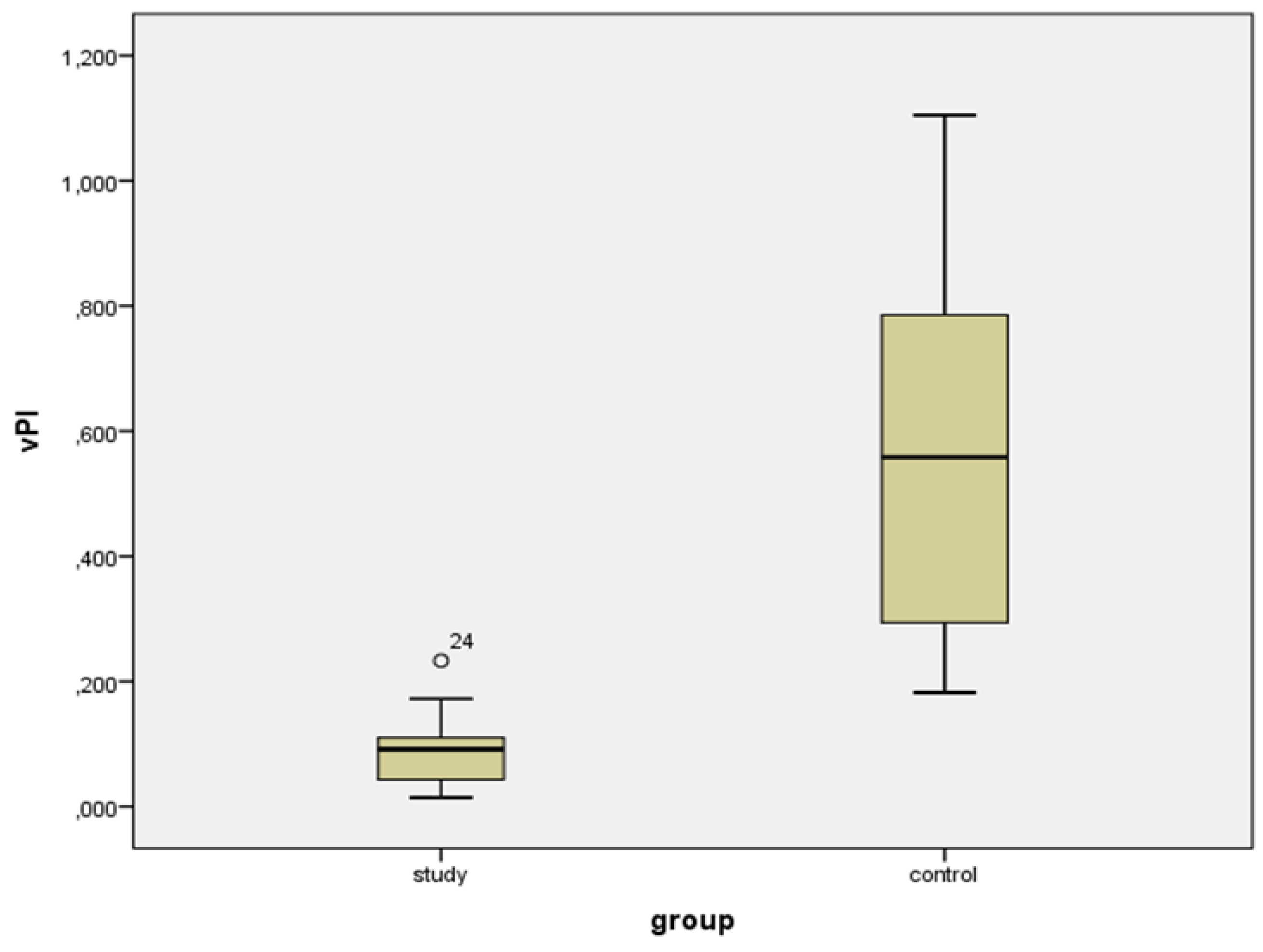
| VIsys * | VIdias * | vS/D + | vPI + | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (%) (SD) | Range | Mean (%) (SD) | Range | Median (IQR) | Range | Median (IQR) | Range | |
| Study group | 53.729 (22.104) | 19.737 to 93.359 | 49.169 (21.827) | 18.508 to 91.800 | 1.096 (0.770) | 1.015 to 1.204 | 0.092 (0.071) | 0.015 to 0.233 |
| Controls | 22.201 (15.989) | 2.876 to 57.912 | 13.447 (11.835) | 1.440 to 38.116 | 1.794 (0.994) | 1.243 to 3.469 | 0.558 (0.581) | 0.182 to 1.105 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kudla, M.J.; Zikan, M.; Fischerova, D.; Stolecki, M.; Alcazar, J.L. 4D Doppler Ultrasound in High Grade Serous Ovarian Cancer Vascularity Evaluation—Preliminary Study. Diagnostics 2021, 11, 582. https://doi.org/10.3390/diagnostics11040582
Kudla MJ, Zikan M, Fischerova D, Stolecki M, Alcazar JL. 4D Doppler Ultrasound in High Grade Serous Ovarian Cancer Vascularity Evaluation—Preliminary Study. Diagnostics. 2021; 11(4):582. https://doi.org/10.3390/diagnostics11040582
Chicago/Turabian StyleKudla, Marek Jerzy, Michal Zikan, Daniela Fischerova, Mateusz Stolecki, and Juan Luis Alcazar. 2021. "4D Doppler Ultrasound in High Grade Serous Ovarian Cancer Vascularity Evaluation—Preliminary Study" Diagnostics 11, no. 4: 582. https://doi.org/10.3390/diagnostics11040582
APA StyleKudla, M. J., Zikan, M., Fischerova, D., Stolecki, M., & Alcazar, J. L. (2021). 4D Doppler Ultrasound in High Grade Serous Ovarian Cancer Vascularity Evaluation—Preliminary Study. Diagnostics, 11(4), 582. https://doi.org/10.3390/diagnostics11040582