
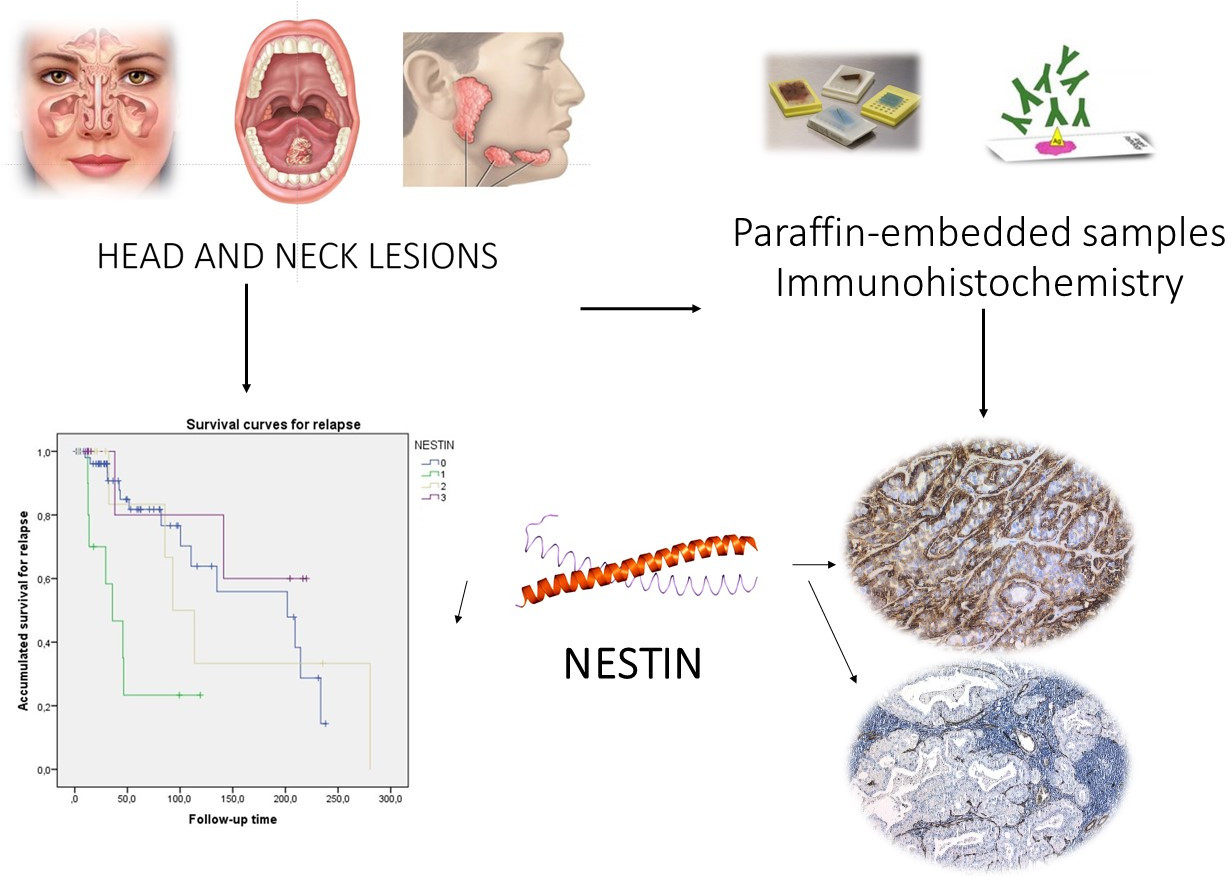
Nestin Expression Is Associated with Relapses in Head and Neck Lesions

 ,
,  , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical and Histopathological Data
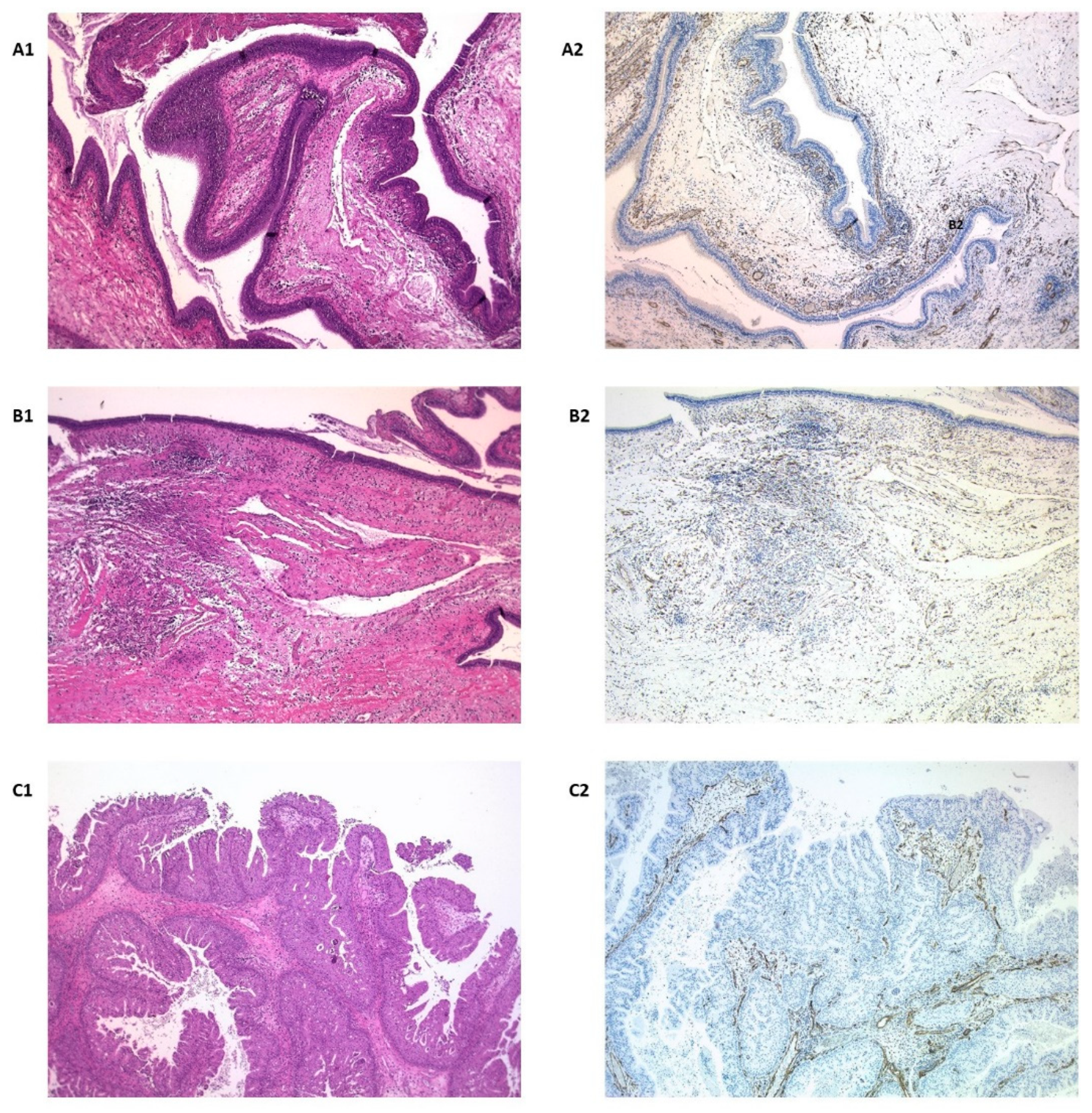
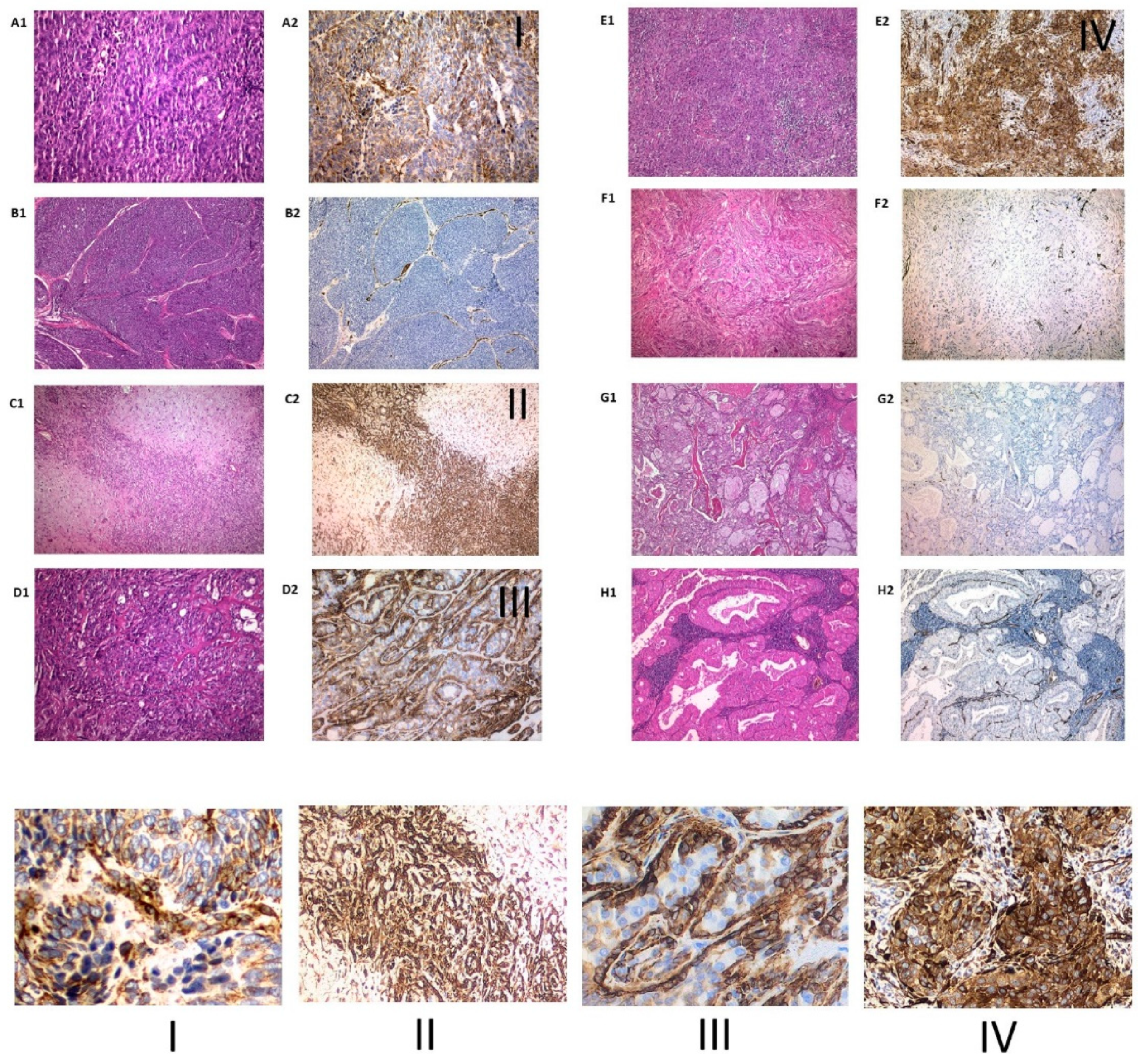
3.2. Immunohistochemical Expression of Nestin
3.3. Follow-Up: Mortality and Recurrence
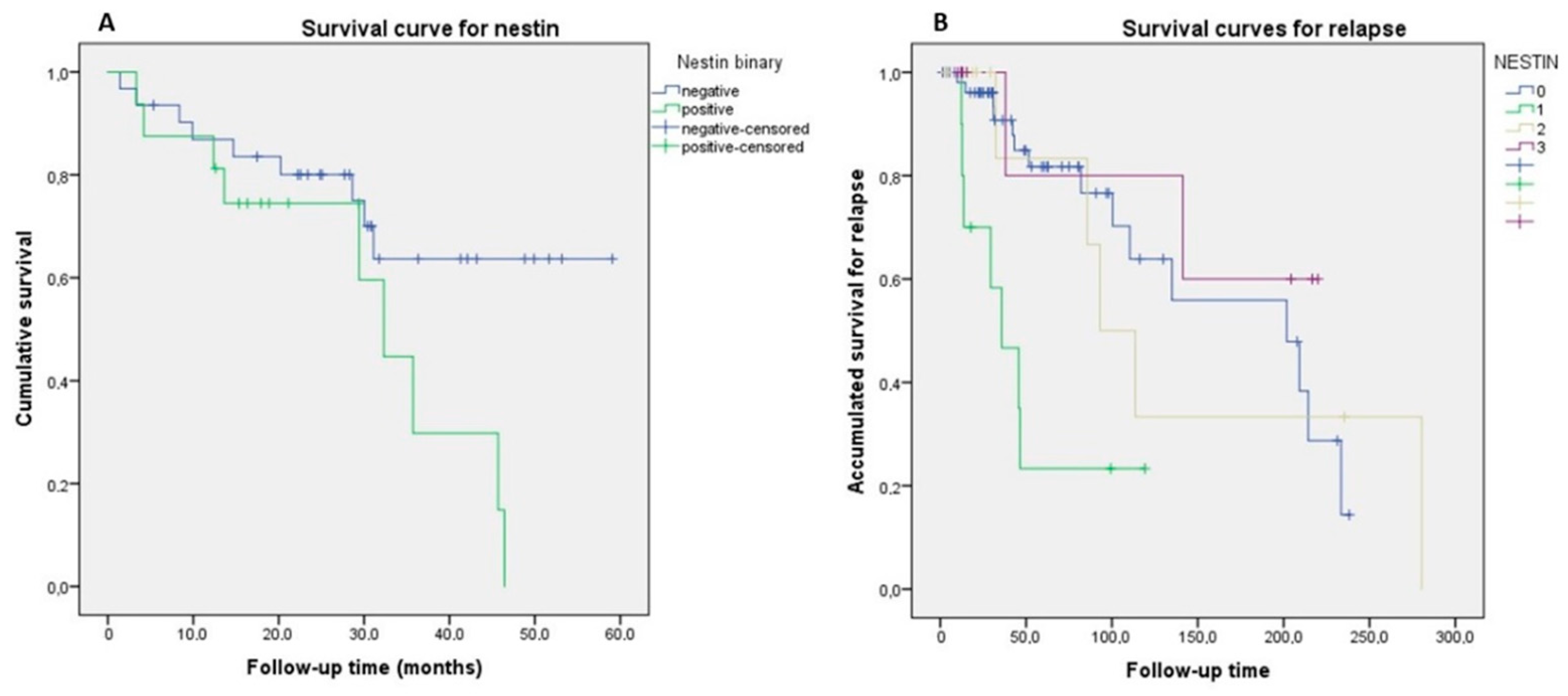
3.4. Survival Analysis
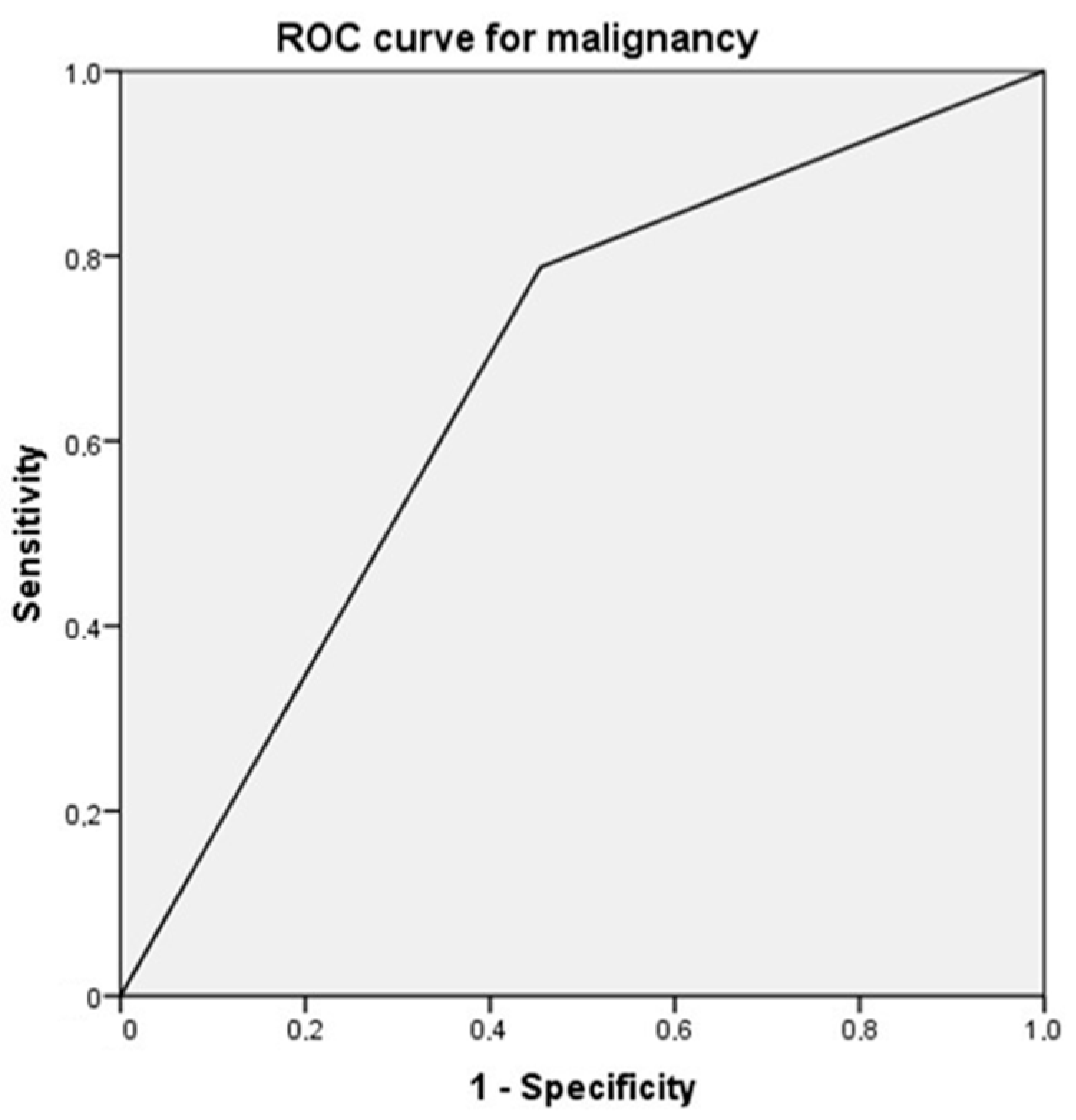
3.5. Diagnostic Yield
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mignone, J.L.; Kukekov, V.; Chiang, A.; Steindler, D.; Enikolopov, G. Neural stem and progenitor cells in nestin-GFP transgenic mice. J. Comp. Neurol. 2004, 3, 311–324. [Google Scholar] [CrossRef]
- Vasuri, F.; Fittipaldi, S.; Buzzi, M.; Degiovanni, A.; Stella, A.; D’Errico-Grigioni, A.; Pasquinelli, G. Nestin and WT1 expression in small-sized vasa vasorum from human normal arteries. Histol. Histopathol. 2012, 27, 1195–1202. [Google Scholar] [PubMed]
- Gleiberman, A.S.; Encinas, J.M.; Mignone, J.L.; Michurina, T.; Rosenfeld, M.G.; Enikolopov, G. Expression of nestin-green fluorescent protein transgene marks oval cells in the adult liver. Dev. Dyn. 2005, 2, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.; Nissen, N.; Mailänder, P.; Stang, F.; Siemers, F.; Kruse, C.; Danner, S. Mammary gland-derived nestin-positive cell populations can be isolated from human male and female donors. Stem Cell Res. Ther. 2013, 4, 78. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, D.; Bakopoulou, A.; Leyhausen, G.; Epivatianos, A.; Volk, J.; Markopoulos, A.; Geurtsen, W. Minor salivary glands of the lips: A novel, easily accessible source of potential stem/progenitor cells. Clin. Oral. Investig. 2014, 3, 847–856. [Google Scholar] [CrossRef]
- Insua, A.; Monje, A.; Urban, I.; Kruger, L.G.; Garaicoa-Pazmiño, C.; Sugai, J.V.; Wang, H.L. The Sinus Membrane-Maxillary Lateral Wall Complex: Histologic Description and Clinical Implications for Maxillary Sinus Floor Elevation. Int. J. Periodontics Restor. Dent. 2017, 6, e328–e336. [Google Scholar] [CrossRef][Green Version]
- Abe, S.; Yamaguchi, S.; Sato, Y.; Harada, K. Sphere-Derived Multipotent Progenitor Cells Obtained from Human Oral Mucosa Are Enriched in Neural Crest Cells. Stem Cells Transl. Med. 2016, 1, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.; Liu, X.; Fan, M.; Yang, L.; Peng, L.; Zhang, L. Isolation and differentiation of nestin positive cells from rat oral mucosal lamina propria. Differentiation 2010, 1, 9–14. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, S.; Ma, J.; Deng, G.; Qu, Y.; Guo, C.; Shen, H. Nestin overexpression in hepatocellular carcinoma associates with epithelial-mesenchymal transition and chemoresistance. J. Exp. Clin. Cancer Res. 2016, 35, 111. [Google Scholar] [CrossRef] [PubMed]
- Malvi, D.; de Biase, D.; Fittipaldi, S.; Grillini, M.; Visani, M.; Pession, A.; D’Errico, A.; Vasuri, F. Immunomorphology and molecular biology of mixed primary liver cancers: Is Nestin a marker of intermediate-cell carcinoma? Histopathology 2020, 2, 265–274. [Google Scholar] [CrossRef]
- Sharma, P.; Alsharif, S.; Fallatah, A.; Chung, B.M. Intermediate Filaments as Effectors of Cancer Development and Metastasis: A Focus on Keratins, Vimentin, and Nestin. Cells 2019, 8, 497. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 1, 57–70. [Google Scholar] [CrossRef]
- Wiese, C.; Rolletschek, A.; Kania, G.; Blyszczuk, P.; Tarasov, K.V.; Tarasova, Y.; Wersto, R.P.; Boheler, K.R.; Wobus, A.M. Nestin expression—A property of multi-lineage progenitor cells? Cell Mol. Life Sci. 2004, 61, 2510–2522. [Google Scholar] [CrossRef] [PubMed]
- Narita, K.; Matsuda, Y.; Seike, M.; Naito, Z.; Gemma, A.; Ishiwata, T. Nestin regulates proliferation, migration, invasion and stemness of lung adenocarcinoma. Int. J. Oncol. 2014, 4, 1118–1130. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, A.; Susaki, M.; Takano, Y.; Mizusawa, M.; Mishima, M.; Iijima, M.; Kuroda, S.I.; Okada, T.; Nakamura, C. The Structural Function of Nestin in Cell Body Softening is Correlated with Cancer Cell Metastasis. Int. J. Biol. Sci. 2019, 7, 1546–1556. [Google Scholar] [CrossRef]
- Li, J.; Wang, R.; Yang, L.; Wu, Q.; Wang, Q.; Nie, Z.; Yu, Y.; Ma, J.; Pan, Q. Knockdown of Nestin inhibits proliferation and migration of colorectal cancer cells. Int. J. Clin. Exp. Pathol. 2015, 6, 6377–6386. [Google Scholar]
- Gao, N.; Xu, H.; Liu, C.; Xu, H.; Chen, G.; Wang, X.; Li, Y.; Wang, Y. Nestin: Predicting specific survival factors for breast cancer. Tumour Biol. 2014, 3, 1751–1755. [Google Scholar] [CrossRef] [PubMed]
- Curtarelli, R.B.; Gonçalves, J.M.; Dos, S.; Luciane, G.P.; Savi, M.G.; Nör, J.E.; Mezzomo, L.A.M.; Cordeiro, M.M.R. Expression of Cancer Stem Cell Biomarkers in Human Head and Neck Carcinomas: A Systematic Review. Stem Cell Rev. Rep. 2018, 6, 769–784. [Google Scholar] [CrossRef]
- Luo, W.; Li, S.; Peng, B.; Ye, Y.; Deng, X.; Yao, K. Embryonic stem cells markers SOX2, OCT4 and Nanog expression and their correlations with epithelial-mesenchymal transition in nasopharyngeal carcinoma. PLoS ONE 2013, 2, e56324. [Google Scholar]
- Mascolo, M.; Ilardi, G.; Romano, M.F.; Celetti, A.; Siano, M.; Romano, S.; Luise, C.; Merolla, F.; Rocco, A.; Vecchione, M.L.; et al. Overexpression of chromatin assembly factor-1 p60, poly(ADP-ribose) polymerase 1 and nestin predicts metastasizing behaviour of oral cancer. Histopathology 2012, 6, 1089–1105. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Chen, W.; Li, J.; Lind, A.C.; Lu, D. Diagnostic utility of neural stem and progenitor cell markers nestin and SOX2 in distinguishing nodal melanocytic nevi from metastatic melanomas. Mod. Pathol. 2013, 1, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, J.; Kolár, Z.; Mokry, J. Nestin as a diagnostic and prognostic marker: Immunohistochemical analysis of its expression in different tumours. J. Clin. Pathol. 2005, 2, 222–223. [Google Scholar] [CrossRef]
- Han, S.; Huang, T.; Wu, X.; Wang, X.; Li, W.; Liu, S.; Yang, W.; Shi, Q.; Li, H.; Shi, K.; et al. Prognostic value of ALDH1 and Nestin in advanced cancer: A systematic meta-analysis with trial sequential analysis. Ther. Adv. Med. Oncol. 2019, 11, 1758835919830831. [Google Scholar] [CrossRef]
- Smane-Filipova, L.; Pilmane, M.; Akota, I. Immunohistochemical analysis of nestin, CD34 and TGFβ3 in facial tissue of children with complete unilateral and bilateral cleft lip and palate. Stomatologija 2016, 3, 98–104. [Google Scholar]
- Derjac-Aramă, A.I.; Sarafoleanu, C.; Manea, C.M.; Nicolescu, M.I.; Vrapciu, A.D.; Rusu, M.C. Regenerative potential of human schneiderian membrane: Progenitor cells and epithelial-mesenchymal transition. Anat. Rec. 2015, 12, 2132–2140. [Google Scholar] [CrossRef]
- Kuk, S.K.; Won, C.H.; Lee, W.J.; Shin, W.J.; Yoon, H.J.; Hong, S.D.; Hong, S.P.; Lee, J. Prognostic significance of nestin in primary malignant melanoma of the oral cavity. Melanoma Res. 2016, 5, 457–463. [Google Scholar] [CrossRef]
- Ravindran, G.; Devaraj, H. Prognostic significance of neural stem cell markers, Nestin and Musashi-1, in oral squamous cell carcinoma: Expression pattern of Nestin in the precancerous stages of oral squamous epithelium. Clin. Oral Investig. 2015, 6, 1251–1260. [Google Scholar] [CrossRef]
- Yanai, H.; Sato, Y.; Nagatsuka, H.; Yoshino, T. Nestin is a wide-spectrum abluminal cell marker of salivary gland tumors. Pathol. Int. 2013, 10, 496–501. [Google Scholar] [CrossRef]
- Levin, R.J.; Bradley, M.K. Neuroectodermal antigens persist in benign and malignant salivary gland tumor cultures. Arch. Otolaryngol. Head Neck Surg. 1996, 5, 551–558. [Google Scholar] [CrossRef]
- Sedassari, B.T.; Rodrigues, M.F.S.D.; Mariano, F.V.; Altemani, A.; Nunes, F.D.; Sousa, S. The Stem Cell Marker Bmi-1 Is Sensitive in Identifying Early Lesions of Carcinoma ex Pleomorphic Adenoma. Medicine (Baltimore) 2015, 27, e1035. [Google Scholar] [CrossRef]
- Debiec-Rychter, M.; Van Valckenborgh, I.; Van den Broeck, C.; Hagemeijer, A.; Van de Ven, W.J.; Kas, K.; Van Damme, B.; Voz, M.L. Histologic localization of PLAG1 (pleomorphic adenoma gene 1) in pleomorphic adenoma of the salivary gland: Cytogenetic evidence of common origin of phenotypically diverse cells. Lab. Investig. 2001, 9, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Aigner, T.; Neureiter, D.; Völker, U.; Belke, J.; Kirchner, T. Epithelial-mesenchymal transdifferentiation and extracellular matrix gene expression in pleomorphic adenomas of the parotid salivary gland. J. Pathol. 1998, 2, 178–185. [Google Scholar] [CrossRef]
- Carrière, C.; Seeley, E.S.; Goetze, T.; Longnecker, D.S.; Korc, M. The Nestin progenitor lineage is the compartment of origin for pancreatic intraepithelial neoplasia. Proc. Natl. Acad. Sci. USA 2007, 11, 4437–4442. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Filho, M.S.; Nör, J.E. The biology of head and neck cancer stem cells. Oral Oncol. 2012, 48, 1–9. [Google Scholar] [CrossRef]
- Scotti, F.M.; Mitt, V.C.; Vieira, D.S.; Biz, M.T.; Castro, R.G.; Modolo, F. Expression of stem cell markers Nanog and Nestin in lip squamous cell carcinoma and actinic cheilitis. Oral Dis. 2018, 24, 1209–1216. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Nestin Expression | Total | p-Value | ||||
|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | ||||
| Gender | Female | 24 (60) | 4 (10) | 5 (12.5) | 7 (17.5) | 40 (45.5) | 0.635 |
| Male | 31 (64.6) | 6 (12.5) | 7 (14.6) | 4 (8.3) | 48 (54.5) | ||
| Origin | Nasosinus | 33 (84.6) | 2 (5.1) | 4 (10.3) | 0 | 39 (44.3) | 0.001 |
| Salivary glands | 18 (48.6) | 6 (16.2) | 3 (8.1) | 10 (27) | 37 (42) | ||
| Oral | 4 (33.3) | 2 (16.7) | 5 (41.7) | 1 (8.3) | 12 (13.6) | ||
| Localization | Nasosinus | 33 (84.6) | 2 (5.1) | 4 (10.3) | 0 | 39 (44.3) | 0.001 |
| Parotid gland | 16 (51.6) | 6 (19.4) | 1 (3.2) | 3 (25.8) | 31 (35.2) | ||
| Submandibular gland | 2 (33.3) | 0 | 2 (33.3) | 2 (33.3) | 6 (6.8) | ||
| Alveolar mucosa | 3 (60) | 0 | 2 (40) | 0 | 5 (5.7) | ||
| Buccal mucosa | 1 (50) | 1 (50) | 0 | 0 | 2 (2.3) | ||
| Floor of the mouth | 0 | 0 | 1 (50) | 1 (50) | 2 (2.3) | ||
| Lip | 0 | 0 | 1 | 0 | 1 (1.1) | ||
| Tongue | 0 | 0 | 1 | 0 | 1 (1.1) | ||
| Retromolar trigone | 0 | 1 | 0 | 0 | 1 (1.1) | ||
| Histological type | Adenocarcinoma | 4 (50) | 2 (25) | 1 (12.5) | 1 (12.5) | 8 (9.1) | <0.001 |
| Carcinoma | 16 (44.4) | 6 (16.7) | 11 (30.6) | 3 (8.3) | 36 (40.9) | ||
| Lymphoma | 1 (33.3) | 2 (66.7) | 0 | 0 | 3 (3.4) | ||
| Inverted papilloma | 14 (100) | 0 | 0 | 0 | 14 (15.9) | ||
| Polyp | 13 (100) | 0 | 0 | 0 | 13 (14.8) | ||
| Pleomorphic adenoma | 0 | 0 | 0 | 7 (100) | 7 (8) | ||
| Warthin tumor | 4 (100) | 0 | 0 | 0 | 4 (4.5) | ||
| Mucoepidermoid carcinoma | 3 (100) | 0 | 0 | 0 | 3 (3.4) | ||
| Malignancy | No | 30 (81.1) | 0 | 0 | 7 (18.9) | 37 (42) | <0.001 |
| Yes | 25 (49) | 10 (19.6) | 12 (23.5) | 4 (7.8) | 51 (58) | ||
| Death | No | 42 (66.7) | 2 (3.2) | 8 (12.7) | 11 (17.5) | 63 (71.6) | <0.001 |
| Yes | 13 (52) | 8 (32) | 4 (16) | 0 | 25 (28.4) | ||
| Death by lesion | No exitus | 42 (66.7) | 2 (3.2) | 8 (12.7) | 11 (17.5) | 63 (71.6) | <0.001 |
| Yes by the lesion | 8 (61.5) | 2 (15.4) | 3 (23.1) | 0 | 13 (14.8) | ||
| Yes other reasons | 5 (41.7) | 6 (50) | 1 (8.3) | 0 | 12 (13.6) | ||
| Relapse | No | 40 (67.8) | 3 (5.1) | 7 (11.9) | 9 (15.3) | 59 (67) | 0.038 |
| Yes | 15 (51.7) | 7 (24.1) | 5 (17.2) | 2 (6.9) | 29 (33) | ||
| Total | 55 (62.5) | 10 (11.4) | 12 (13.6) | 11 (12.5) | 88 (100) | ||
| Nestin 0 Average ± SD (CI95%) | Nestin 1 Average ± SD (CI95%) | Nestin 2 Average ± SD (CI95%) | Nestin 3 Average ± SD (CI95%) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 51.7 ± 1.5 | 76.3 ± 9.4 | 49.5 ± 17.4 | 55.2 ± 22.3 | 0.001 * |
| (47–56.5) | (69.5–83) | (38.4–60.6) | (40.2–70.2) | ||
| Overall survival | 40.7 ± 39.9 | 51 ± 38.4 | 38.3 ± 51.9 | – | 0.827 |
| (16.6–64.9) | (18.9–83.1) | (18.8–83.1) | |||
| Maximum follow-up time Disease Free Survival | 71.73 ± 65.53 54.02–89.45 31.1 ± 39.9 (9–53.2) | 43.24 ± 37.41 16.48–70 15.6 ± 9 (7.2–24) | 77.80 ± 92.1 19.28–126.32 96 ± 85.5 (–10.1–202.2) | 81.47 ± 92.98 19.01–143.94 48.7 ± 37 (–283.8–381.3) | 0.600 0.037 ** |
| Disease specific survival | 37.6 ± 43.3 | 21.9 ± 13.5 | 50 ± 56.8 | – | 0.791 |
| (1.4–73.8) | (–100–143.9) | (–91.1–191.1) | |||
| Number of relapses | 0.5 ± 1.3 | 1.3 ± 1.5 | 0.75 ± 1 | 0.27 ± 0.6 | 0.289 |
| (0.17–0.92) | (0.18–2.4) | (0.8–1.4) | (–0.16–0.7) | ||
| Time until last relapse | 84.5–59.3 | 30.8 ± 6.1 | 117.9 ± 126 | 129.4 | 0.637 |
| (22.2–146.9) | (–24.5–86.1) | (–195–431) | |||
| Period of relapses | 53.4 ± 45 | 13.8 ± 1.37 | 20.9 ± 16.9 | 54.52 | 0.470 |
| (6.1–100.6) | (1.5–26.1) | (–21–62.9) |
| Cox Regression Covariate | Relapse | |||
|---|---|---|---|---|
| Univariate HR (95% CI) | p Value | Adjusted HR (95 % CI) | p Value | |
| Nestin | ||||
| Negative Vs 1 | 4.577 (1.802–11.626) | 0.001 | 8.918 (2.71–305.62) | <0.001 |
| Negative Vs 2 Negative Vs 3 | 1.023 (0.332–3.158) | 0.968 | 1.347 (0.354–5.118) | 0.662 |
| 0.546 (0.122–2.433) | 0.427 | 0.899 (0.151–5.356) | 0.907 | |
| Location | ||||
| Nasal/Sinus Vs trigone | 0.034 (0.03–0.389) | 0.006 | 0.210 (0.070–0.627) | 0.005 |
| Parotid Vs trigone | 0.013 (0.001–0.160) | 0.001 | 0.246 (0.020–2.966) | 0.270 |
| Submaxilla Vs trigone | 0.010 (0–0.236) | 0.004 | 2.497 (0.413–15.087) | 0.319 |
| Alveolar ridge Vs trigone | 0.086 (0.006—1.270) | 0.074 | 0 | 0.992 |
| Buccal mucosa Vs trigone | 0 | 0.991 | 0 | 0.994 |
| Floor of mouth Vs trigone | 0 | 0.991 | 0 | 0.963 |
| Lip Vs trigone | 0 | 0.956 | 0 | 0.995 |
| Tongue Vs trigone | 0 | 0.994 | 4.405 (0.344–56.384) | 0.254 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Sayáns, M.; Chamorro-Petronacci, C.M.; Baltazar, F.; Pires, F.R.; Ínsua, Á.; Suárez-Quintanilla, J.A.; Suárez-Peñaranda, J.M. Nestin Expression Is Associated with Relapses in Head and Neck Lesions. Diagnostics 2021, 11, 583. https://doi.org/10.3390/diagnostics11040583
Pérez-Sayáns M, Chamorro-Petronacci CM, Baltazar F, Pires FR, Ínsua Á, Suárez-Quintanilla JA, Suárez-Peñaranda JM. Nestin Expression Is Associated with Relapses in Head and Neck Lesions. Diagnostics. 2021; 11(4):583. https://doi.org/10.3390/diagnostics11040583
Chicago/Turabian StylePérez-Sayáns, Mario, Cintia M Chamorro-Petronacci, Fátima Baltazar, Fabio Ramoa Pires, Ángel Ínsua, Juan A Suárez-Quintanilla, and José M Suárez-Peñaranda. 2021. "Nestin Expression Is Associated with Relapses in Head and Neck Lesions" Diagnostics 11, no. 4: 583. https://doi.org/10.3390/diagnostics11040583
APA StylePérez-Sayáns, M., Chamorro-Petronacci, C. M., Baltazar, F., Pires, F. R., Ínsua, Á., Suárez-Quintanilla, J. A., & Suárez-Peñaranda, J. M. (2021). Nestin Expression Is Associated with Relapses in Head and Neck Lesions. Diagnostics, 11(4), 583. https://doi.org/10.3390/diagnostics11040583