
Percutaneous Two-Dimensional Shear Wave Elastography for Diagnosis of Pancreatic Tumor

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study and Patient Enrollment
- in-/out-patients with pancreatic tumor lesions and those scheduled for surgical procedure or fine needle biopsy (FNA) for histological examination or out-patients with focal pancreatic lesions that have already been confirmed histologically as benign by a past EUS-guided FNA (EUS-FNA); and
- patients without any abdominal surgical history. The final diagnosis was based on the histological analysis of surgically resected specimens or EUS-FNA results. The control group comprised participants lacking a history of pancreatic disease or abdominal symptoms. However, patients who were pregnant at the time of screening were excluded.
2.2. ERCP, EUS, and EUS-FNA
2.3. SWE
2.4. SWE Data Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
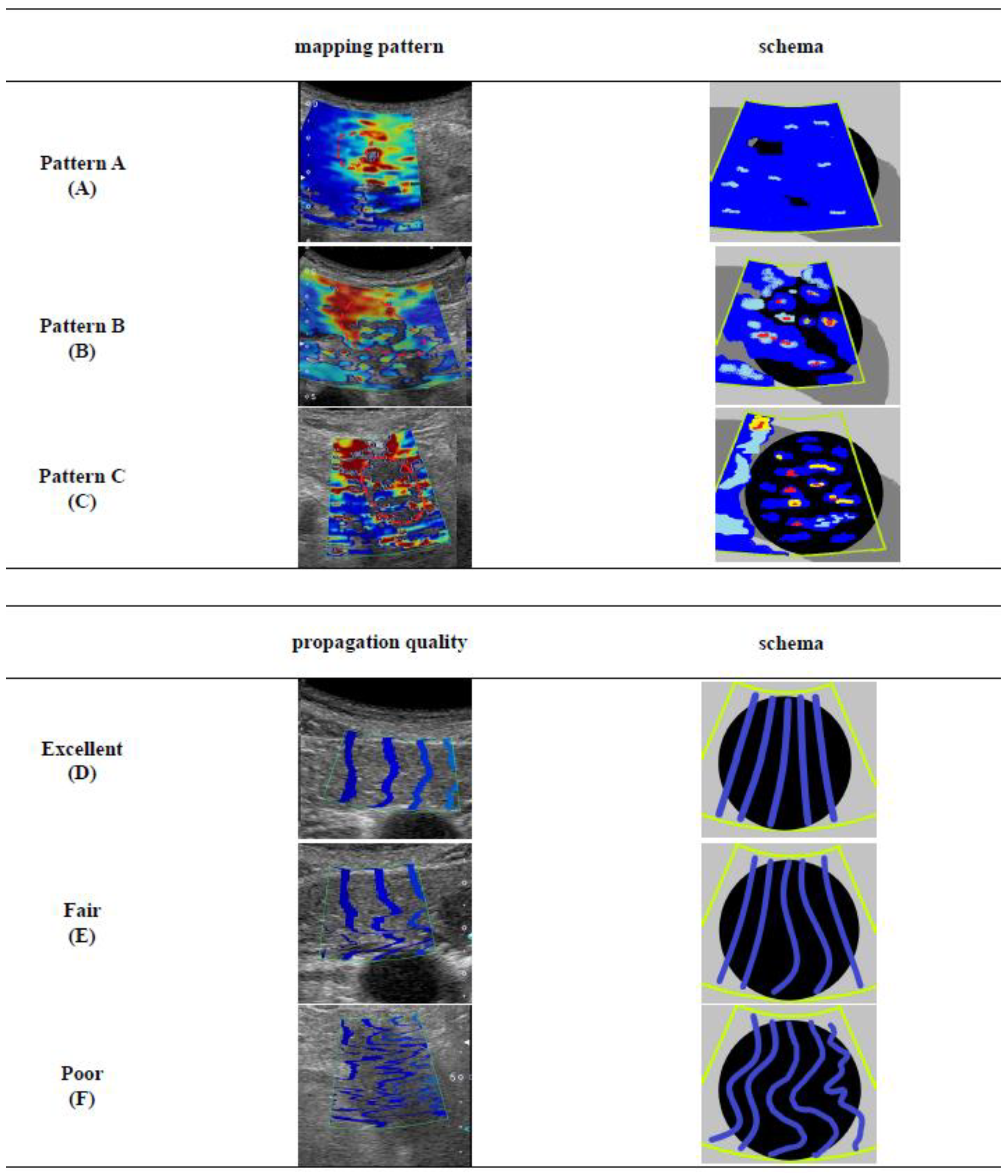
3.2. SWE-Mapping Patterns and Propagation Quality
3.3. Diagnostic Performance of SWE Findings for Pancreatic Tumors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tasu, J.P. Imaging: The cornerstone of pancreatic tumor management. Diagn. Interv. Imaging 2016, 97, 1205–1206. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Cepelli, P.; Scarpa, A. Pancreatic Ductal Adenocarcinoma and Its Variants. Surg. Pathol. Clin. 2016, 9, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Toft, J.; Hadden, W.J.; Laurence, J.M.; Lam, V.; Yuen, L.; Janssen, A.; Pleass, H. Imaging modalities in the diagnosis of pancreatic adenocarcinoma: A systematic review and meta-analysis of sensitivity, specificity and diagnostic accuracy. Eur. J. Radiol. 2017, 92, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, M.J.; McPhail, M.J.; Possamai, L.; Dhar, A.; Vlavianos, P.; Monahan, K.J. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: A meta-analysis. Gastrointest. Endosc. 2012, 75, 319–331. [Google Scholar] [CrossRef]
- Erickson, R.A. ERCP and Pancreatic Cancer. Ann. Surg. Oncol. 2004, 11, 555–557. [Google Scholar] [CrossRef]
- Herrmann, E.; De Lédinghen, V.; Cassinotto, C.; Chu, W.C.W.; Leung, V.Y.-F.; Ferraioli, G.; Filice, C.; Castera, L.; Vilgrain, V.; Ronot, M.; et al. Assessment of biopsy-proven liver fibrosis by two-dimensional shear wave elastography: An individual patient data-based meta-analysis. Hepatology 2018, 67, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Elkrief, L.; Ronot, M.; Andrade, F.; Burgio, M.D.; Issoufaly, T.; Zappa, M.; Roux, O.; Bissonnette, J.; Payancé, A.; Lebrec, D.; et al. Non-invasive evaluation of portal hypertension using shear-wave elastography: Analysis of two algorithms combining liver and spleen stiffness in 191 patients with cirrhosis. Aliment. Pharmacol. Ther. 2018, 47, 621–630. [Google Scholar] [CrossRef]
- Sebag, F.; Vaillant-Lombard, J.; Berbis, J.; Griset, V.; Henry, J.F.; Petit, P.; Oliver, C. Shear wave elastography: A new ultrasound imaging mode for the differential diagnosis of benign and malignant thyroid nodules. J. Clin. Endocrinol. Metab. 2010, 95, 5281–5288. [Google Scholar] [CrossRef]
- Tan, R.; Xiao, Y.; He, Q. Ultrasound Elastography. Its Potential Role in Assessment of Cervical Lymphadenopathy. Acad. Radiol. 2010, 17, 849–855. [Google Scholar] [CrossRef]
- Ferraioli, G.; Filice, C.; Castera, L.; Choi, B.I.; Sporea, I.; Wilson, S.R.; Cosgrove, D.; Dietrich, C.F.; Amy, D.; Bamber, J.C.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 3: Liver. Ultrasound Med. Biol. 2015, 41, 1161–1179. [Google Scholar] [CrossRef]
- Barr, R.G. Shear wave liver elastography. Abdom. Radiol. 2018, 43, 800–807. [Google Scholar] [CrossRef]
- Yashima, Y.; Sasahira, N.; Isayama, H.; Kogure, H.; Ikeda, H.; Hirano, K.; Mizuno, S.; Yagioka, H.; Kawakubo, K.; Sasaki, T.; et al. Acoustic radiation force impulse elastography for noninvasive assessment of chronic pancreatitis. J. Gastroenterol. 2012, 47, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, K.; Hirooka, Y.; Kawashima, H.; Ohno, E.; Ishikawa, T.; Kawai, M.; Suhara, H.; Takeyama, T.; Koya, T.; Tanaka, H.; et al. The propagation display method improves the reproducibility of pancreatic shear wave elastography. Ultrasound Med. Biol. 2019, 45, 2242–2247. [Google Scholar] [CrossRef] [PubMed]
- Onoyama, T.; Koda, M.; Fujise, Y.; Takata, T.; Kawata, S.; Okamoto, T.; Miyoshi, K.; Matono, T.; Sugihara, T.; Matsumoto, K.; et al. Utility of virtual touch quantification in the diagnosis of pancreatic ductal adenocarcinoma. Clin. Imaging 2017, 42, 64–67. [Google Scholar] [CrossRef]
- Park, M.K.; Jo, J.; Kwon, H.; Cho, J.H.; Oh, J.Y.; Noh, M.H.; Nam, K.J. Usefulness of acoustic radiation force impulse elastography in the differential diagnosis of benign and malignant solid pancreatic lesions. Ultrasonography 2014, 33, 26–33. [Google Scholar] [CrossRef]
- Goertz, R.S.; Schuderer, J.; Strobel, D.; Pfeifer, L.; Neurath, M.F.; Wildner, D. Acoustic radiation force impulse shear wave elastography (ARFI) of acute and chronic pancreatitis and pancreatic tumor. Eur. J. Radiol. 2016, 85, 2211–2216. [Google Scholar] [CrossRef]
- Adsay, N.V.; Basturk, O.; Cheng, J.D.; A Andea, A. Ductal neoplasia of the pancreas: Nosologic, clinicopathologic, and biologic aspects. Semin. Radiat. Oncol. 2005, 15, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Shimosegawa, T.; Chari, S.T.; Frulloni, L.; Kamisawa, T.; Kawa, S.; Mino-Kenudson, M.; Kim, M.H.; Klöppel, G.; Lerch, M.M.; Löhr, M.; et al. International consensus diagnostic criteria for autoimmune pancreatitis: Guidelines of the international association of pancreatology. Pancreas 2011, 40, 352–358. [Google Scholar] [CrossRef]
- Rösch, T.; Lorenz, R.; Braig, C.; Feuerbach, S.; Siewert, J.R.; Classen, M. Endosonographic diagnosis of pancreatic tumors. Dtsch. Med. Wochenschr. 1990, 115, 1339–1347. [Google Scholar] [CrossRef]
- Senoo, J.; Mikata, R.; Kishimoto, T.; Hayashi, M.; Kusakabe, Y.; Yasui, S.; Yamato, M.; Ohyama, H.; Sugiyama, H.; Tsuyuguchi, T.; et al. Immunohistochemical analysis of IMP3 and p53 expression in endoscopic ultrasound-guided fine needle aspiration and resected specimens of pancreatic diseases. Pancreatology 2018, 18, 176–183. [Google Scholar] [CrossRef]
- Maruyama, H.; Kobayashi, K.; Kiyono, S.; Sekimoto, T.; Kanda, T.; Yokosuka, O. Two-dimensional shear wave elastography with propagation-based reliability assessment for grading hepatic fibrosis and portal hypertension. J. Hepatobiliary Pancreat. Sci. 2016, 23, 595–602. [Google Scholar] [CrossRef]
- Nagpal, S.J.S.; Sharma, A.; Chari, S.T. Autoimmune Pancreatitis. Am. J. Gastroenterol. 2018, 62, 1301–1309. [Google Scholar] [CrossRef]
- Reid, M.D.; Balci, S.; Saka, B.; Adsay, N.V. Neuroendocrine tumors of the pancreas: Current concepts and controversies. Endocr. Pathol. 2014, 25, 65–79. [Google Scholar] [CrossRef]
- Kawada, N.; Tanaka, S.; Uehara, H.; Ohkawa, K.; Yamai, T.; Takada, R.; Shiroeda, H.; Arisawa, T.; Tomita, Y. Potential use of point shear wave elastography for the pancreas: A single center prospective study. Eur. J. Radiol. 2014, 83, 620–624. [Google Scholar] [CrossRef]
- Okasha, H.; Elkholy, S.; El-Sayed, R.; Wifi, M.-N.; El-Nady, M.; El-Nabawi, W.; A El-Dayem, W.; I Radwan, M.; Farag, A.; El-Sherif, Y.; et al. Real time endoscopic ultrasound elastography and strain ratio in the diagnosis of solid pancreatic lesions. World J. Gastroenterol. 2017, 23, 5962–5968. [Google Scholar] [CrossRef] [PubMed]
- Itokawa, F.; Itoi, T.; Sofuni, A.; Kurihara, T.; Tsuchiya, T.; Ishii, K.; Tsuji, S.; Ikeuchi, N.; Umeda, J.; Tanaka, R.; et al. EUS elastography combined with the strain ratio of tissue elasticity for diagnosis of solid pancreatic masses. J. Gastroenterol. 2011, 46, 843–853. [Google Scholar] [CrossRef]
- Săftoiu, A.; Vilmann, P.; Gorunescu, F.; Janssen, J.; Hocke, M.; Larsen, M.; Iglesias-Garcia, J.; Arcidiacono, P.; Will, U.; Giovannini, M.; et al. Accuracy of endoscopic ultrasound elastography used for differential diagnosis of focal pancreatic masses: A multicenter study. Endoscopy 2011, 43, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Garcia, J.; Larino-Noia, J.; Abdulkader, I.; Forteza, J.; Dominguez-Munoz, J.E. EUS elastography for the characterization of solid pancreatic masses. Gastrointest. Endosc. 2009, 70, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Botelberge, T.; Bories, E.; Pesenti, C.; Caillol, F.; Esterni, B.; Monges, G.; Arcidiacono, P.; Deprez, P.; Yeung, R.; et al. Endoscopic ultrasound elastography for evaluation of lymph nodes and pancreatic masses: A multicenter study. World J. Gastroenterol. 2009, 15, 1587–1593. [Google Scholar] [CrossRef]
- Iglesias–Garcia, J.; Larino–Noia, J.; Abdulkader, I.; Forteza, J.; Dominguez–Munoz, J.E. Quantitative endoscopic ultrasound elastography: An accurate method for the differentiation of solid pancreatic masses. Gastroenterology 2010, 139, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Dawwas, M.F.; Taha, H.; Leeds, J.S.; Nayar, M.K.; Oppong, K.W. Diagnostic accuracy of quantitative EUS elastography for discriminating malignant from benign solid pancreatic masses: A prospective, single-center study. Gastrointest. Endosc. 2012, 76, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Hu, Z.; Chen, J.; Guo, X. Comparison of ERCP, EUS, and ERCP combined with EUS in diagnosing pancreatic neoplasms: A systematic review and meta-analysis. Tumour Biol. 2014, 35, 8867–8874. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-L.; Sherman, S.; Watkins, J.L.; Barnett, J.; Freeman, M.; Geenen, J.; Ryan, M.; Parker, H.; Frakes, J.T.; Fogel, E.L.; et al. Risk factors for post-ERCP pancreatitis; a prospective multicenter study. Am. J. Gastroenterol. 2006, 101, 139–147. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PDAC (n = 36) | Non-PDAC (n = 16) | Control | |
|---|---|---|---|---|
| TFP (n = 15) | NET (n = 1) | (n = 33) | ||
| Sex (Male/Female) | 22/14 | 10/5 | 1/0 | 12/21 |
| Age (year) | 68.3 ± 12.2 | 64.0 ± 10.4 | 64 | 68.0 ± 12.4 |
| (35–87) | (48–84) | - | (35-94) | |
| BMI (kg/m2) | 21.4 ± 3.19 | 22.3 ± 3.95 | 24.6 | 22.4 ± 2.46 |
| (15.5–28.5) | (17.0–31.2) | - | (18.3-28.3 | |
| Smoking, n (%) | 18 (50) | 6 (40) | 0 (0) | 12(36.4) |
| Alcohol, n (%) | 4 (11.1) | 3 (20) | 0 (0) | 3(9.1) |
| Diabetes mellitus, n (%) | 8 (22.2) | 5 (33.3) | 0 (0) | 4(12.1) |
| Pancreatic lesion | ||||
| Location (Head/Body or Tail) | 13/23 | 8/7 | 1/0 | |
| Size (mm) | 28.0 ± 12.3 | 28.6 ± 8.86 | 22.0 | |
| (13.0–69.6) | (14.0–40.0) | - | ||
| Histological assessment | ||||
| (FNA/Resection) | 23/13 | 15/0 | 0/1 | |
| Characteristics | Mapping Pattern | ||
|---|---|---|---|
| A | B | C | |
| Number (case) | 3 | 24 | 25 |
| PDAC/TFP/ NET | 0/3/0 | 11/12/1 | 25/0/0 |
| Age (year) | 64.7 ± 10.7 | 65.0 ± 11.3 | 69.2 ± 12.1 |
| (53–74) | (44–87) | (35–85) | |
| BMI (kg/m2) | 21.9 ± 5.59 | 22.9 ± 3.65 | 20.8 ± 3.04 |
| (17.0–28.0) | (17.0–31.1) | (15.5–28.5) | |
| Smoking, n (%) | 1 (33.3) | 9 (37.5) | 14 (56.0) |
| Alcohol, n (%) | 0 | 4 (16.7) | 3 (12.0) |
| Pancreatic lesion | |||
| Size (mm) | 20.4 ± 7.88 | 26.2 ± 6.95 | 32.5 ± 14.0 |
| (14.0–29.9) | (15.0–40.0) | (13.0–69.0) | |
| Location (head), n (%) | 1 (33.3) | 13 (54.2) | 8 (32.0) |
| SWE (kPa) | 10.6 | 22.1 | 27.1 |
| IQR | (7.3–11.3) | (13.0–56.2) | (13.0–148.3) |
| SD (kPa) | 4.94 | 17.6 | 27.1 |
| IQR | (3.6–5.7) | (9.5–27.7) | (13.0–48.3) |
| SWE tumor/non-tumor ratio | 1.21 | 1.97 | 3.37 |
| IQR | (1.07–1.60) | (1.43–4.07) | (2.47–5.46) |
| Characteristics | PDAC | Non-PDAC | p-Value |
|---|---|---|---|
| Number | 11 | 13 | |
| Age (year) | 66.3 ± 12.8 | 65 ± 10.4 | p = 0.5236 |
| (44–87) | (48–84) | ||
| BMI (kg/m2) | 22.7 ± 3.29 | 23.1 ± 4.14 | p = 0.8696 |
| (17.0–27.8) | (18.9–31.2) | ||
| Diabetes mellitus, n (%) | 2 (18.2) | 5 (38.5) | p = 0.6576 |
| Smoking, n (%) | 4 (36.4) | 4 (30.8) | p = 0.8190 |
| Alcohol, n (%) | 1 (9.1) | 3 (23.1) | p = 0.5207 |
| Lesion | |||
| SWE value (kPa) | 34.7 | 26.2 | p = 0.0987 |
| IQR | (23.1–69.1) | (12.8–44.6) | |
| SD (kPa) | 25.6 | 17.0 | p = 0.2466 |
| IQR | (12.2–29.9) | (6.93–25.3) | |
| kPa/SD | 1.58 | 1.28 | p = 0.7721 |
| IQR | (1.17–1.97) | (1.12–2.28) | |
| Parenchyma | |||
| SWE value (kPa) | 10.2 | 9.86 | p = 0.6021 |
| IQR | (9.8–12.9) | (9.22–15.1) | |
| SD (kPa) | 3.38 | 5.83 | p = 0.1320 |
| IQR | (2.49–5.48) | (4.10–6.90) | |
| kPa/SD | 3.57 | 1.80 | p = 0.2024 |
| IQR | (1.82–5.86) | (1.12–2.28) | |
| SWE tumor/non-tumor ratio | |||
| SWE value (kPa) | 3.89 | 1.53 | p = 0.0045 |
| IQR | (2.37–5.17) | (1.12–1.78) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iino, Y.; Maruyama, H.; Mikata, R.; Yasui, S.; Koroki, K.; Nagashima, H.; Awatsu, M.; Shingyoji, A.; Kusakabe, Y.; Kobayashi, K.; et al. Percutaneous Two-Dimensional Shear Wave Elastography for Diagnosis of Pancreatic Tumor. Diagnostics 2021, 11, 498. https://doi.org/10.3390/diagnostics11030498
Iino Y, Maruyama H, Mikata R, Yasui S, Koroki K, Nagashima H, Awatsu M, Shingyoji A, Kusakabe Y, Kobayashi K, et al. Percutaneous Two-Dimensional Shear Wave Elastography for Diagnosis of Pancreatic Tumor. Diagnostics. 2021; 11(3):498. https://doi.org/10.3390/diagnostics11030498
Chicago/Turabian StyleIino, Yotaro, Hitoshi Maruyama, Rintaro Mikata, Shin Yasui, Keisuke Koroki, Hiroki Nagashima, Masami Awatsu, Ayako Shingyoji, Yuko Kusakabe, Kazufumi Kobayashi, and et al. 2021. "Percutaneous Two-Dimensional Shear Wave Elastography for Diagnosis of Pancreatic Tumor" Diagnostics 11, no. 3: 498. https://doi.org/10.3390/diagnostics11030498
APA StyleIino, Y., Maruyama, H., Mikata, R., Yasui, S., Koroki, K., Nagashima, H., Awatsu, M., Shingyoji, A., Kusakabe, Y., Kobayashi, K., Kiyono, S., Nakamura, M., Ohyama, H., Sugiyama, H., Sakai, Y., Chiba, T., Kato, J., Tsuyuguchi, T., & Kato, N. (2021). Percutaneous Two-Dimensional Shear Wave Elastography for Diagnosis of Pancreatic Tumor. Diagnostics, 11(3), 498. https://doi.org/10.3390/diagnostics11030498