
Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases

 ,
, 
 ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. Autopsy Room (A.R.)
- Filter MULTICEL mod. 3mc14 305 × 610 × 292
- Type—HEPA 20 R01
- Integral efficiency (%)—99.995 at MPPS
- Local efficiency (%)—99.975 AT MPPS
- Class to en 1822—H 14
- Size (mm)—305 × 610 × 292
- Airflow (m3/h)—1700
- Resistance to airflow (Pa)—250
- Reference number—20 13
- Serial number—600777.
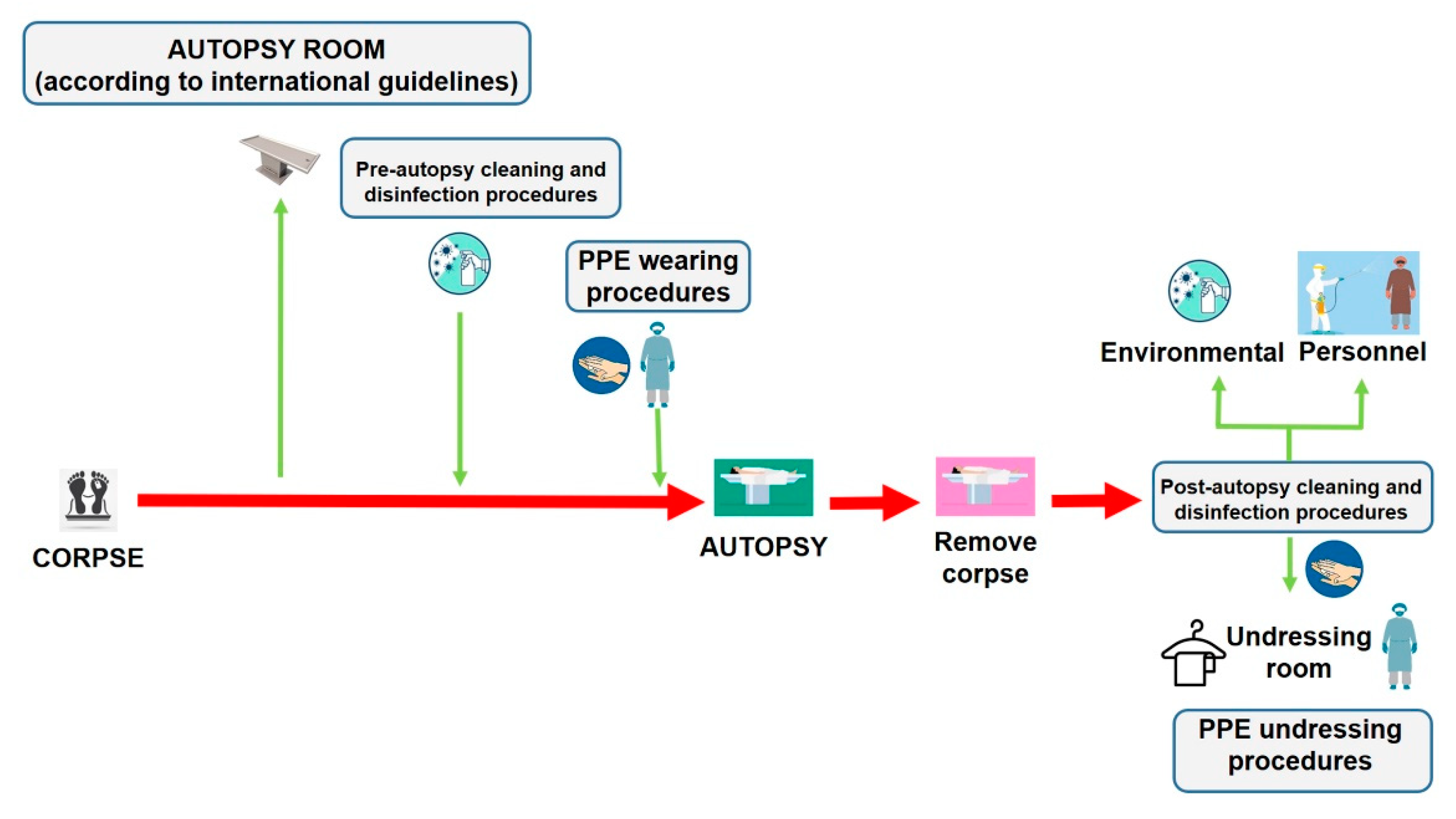
2.3. Autopsy Protocol
- T0—before the autopsy;
- T1—at the end of autopsy (without removing the corpse);
- T2—after the autopsy (after cleaning and disinfection of the AR).
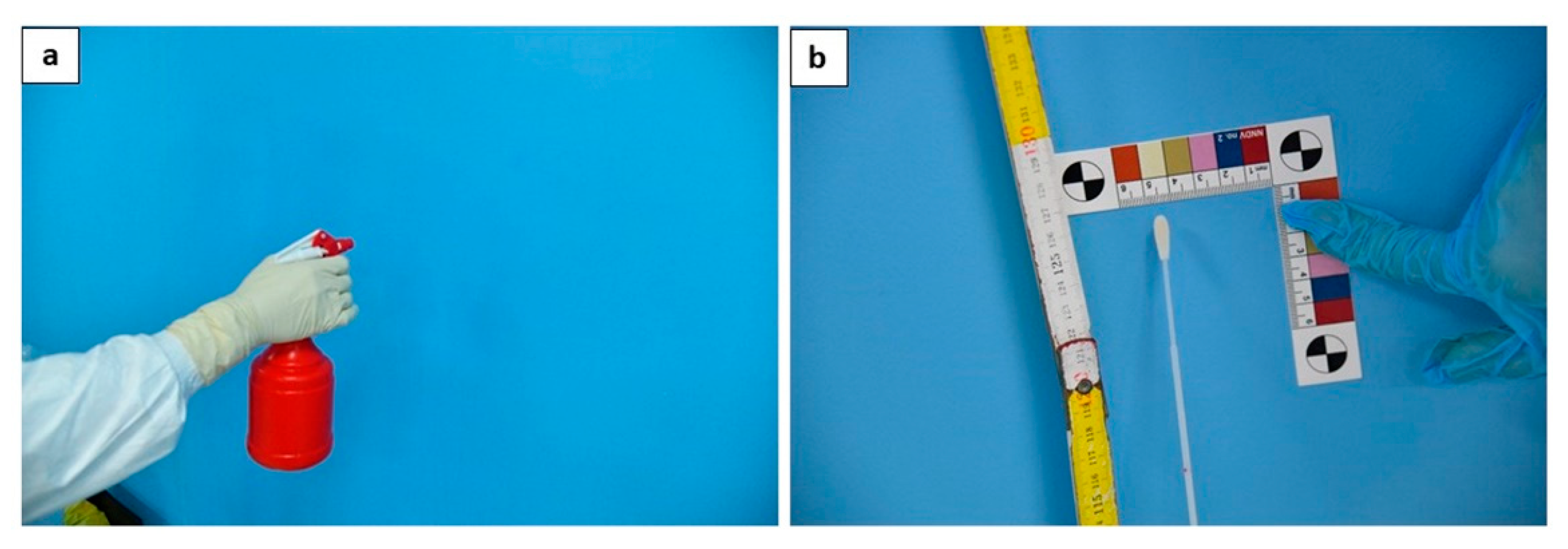
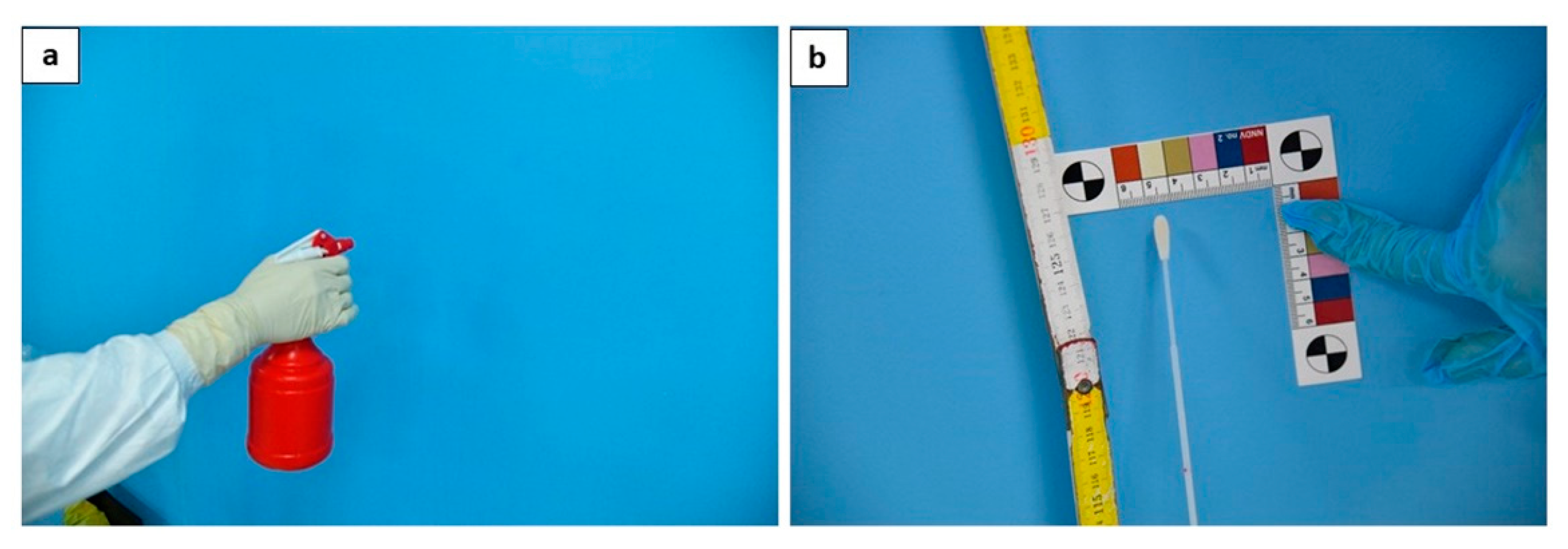
2.3.1. T0—Before the Autopsy
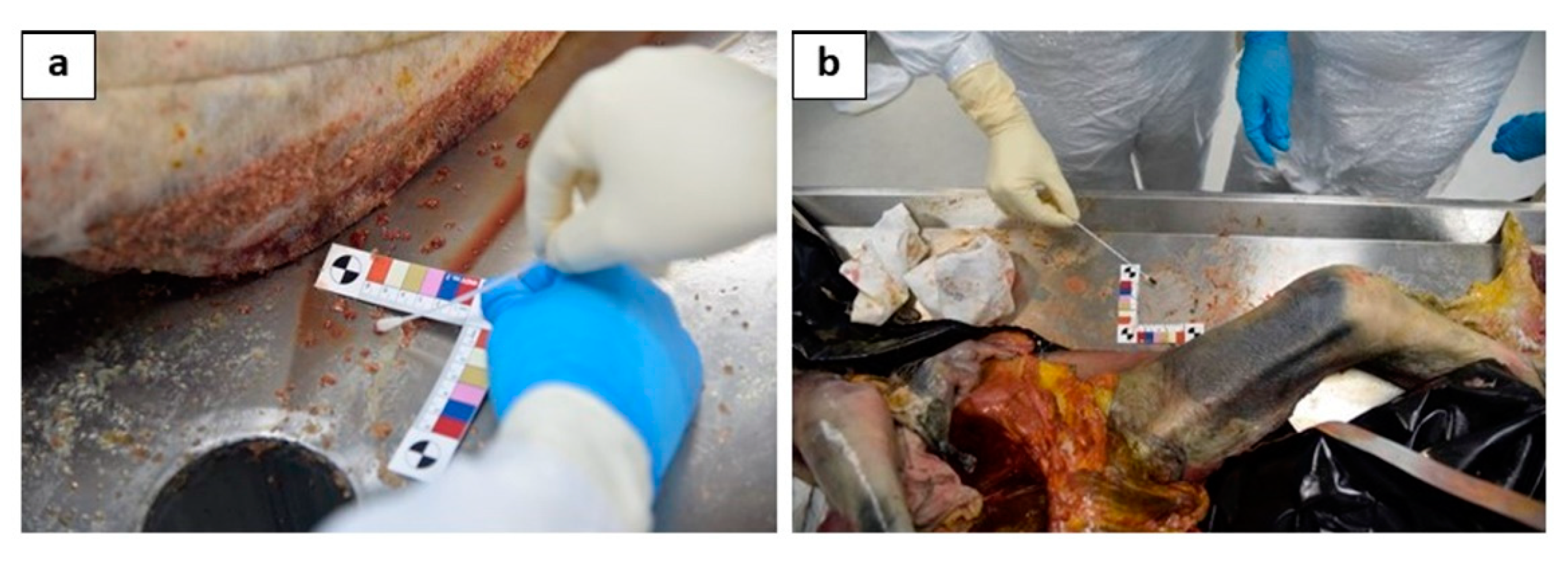
2.3.2. T1—At the End of Autopsy
2.3.3. T2—Disinfection Procedures after the Autopsy
2.4. Swab Analysis
2.5. Statistical Analysis
3. Results
3.1. Result of Low Respiratory Swabs
3.2. Result of Environmental Swab
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Fernandes, F.; Castillo, P.; Bassat, Q.; Quintó, L.; Hurtado, J.C.; Martínez, M.J.; Lovane, L.; Jordao, D.; Bene, R.; Nhampossa, T.; et al. Contribution of the clinical information to the accuracy of the minimally invasive and the complete diagnostic autopsy. Hum. Pathol. 2019, 13, e1002171. [Google Scholar] [CrossRef]
- De Cock, K.M.; Zielinski-Gutiérrez, E.; Lucas, S.B. Learning from the Dead. N. Engl. J. Med. 2019, 381, 1889–1891. [Google Scholar] [CrossRef]
- Pomara, C.; Volti, G.L.; Cappello, F. COVID-19 Deaths: Are We Sure It Is Pneumonia? Please, Autopsy, Autopsy, Autopsy! J. Clin. Med. 2020, 9, 1259. [Google Scholar] [CrossRef]
- Sriwijitalai, W.; Wiwanitkit, V. COVID-19 in forensic medicine unit personnel: Observation from Thailand. J. Forensic Leg. Med. 2020, 72, 101964. [Google Scholar] [CrossRef] [PubMed]
- Salerno, M.; Sessa, F.; Piscopo, A.; Montana, A.; Torrisi, M.; Patanè, F.; Murabito, P.; Li Volti, G.; Pomara, C. No Autopsies on COVID-19 Deaths: A Missed Opportunity and the Lockdown of Science. J. Clin. Med. 2020, 9, 1472. [Google Scholar] [CrossRef] [PubMed]
- College of American Pathologists Amended COVID-19 Autopsy Guideline Statement from the CAP Autopsy Committee. Coll. Am. Pathol. 2020. Available online: https://www.cap.org/member-resources/councils-committees/cancer-topic-center/autopsy-topic-center (accessed on 31 January 2021).
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Fineschi, V.; Aprile, A.; Aquila, I.; Arcangeli, M.; Asmundo, A.; Bacci, M.; Cingolani, M.; Cipolloni, L.; D’Errico, S.; De Casamassimi, I.; et al. Management of the corpse with suspect, probable or confirmed COVID-19 respiratory infection – Italian interim recommendations for personnel potentially exposed to material from corpses, including body fluids, in morgue structures, during autopsy practice. Pathol.—J. Ital. Soc. Anat. Pathol. Diagn. Cytopathol. 2020, 112, 64–77. [Google Scholar]
- Sessa, F.; Bertozzi, G.; Cipolloni, L.; Baldari, B.; Cantatore, S.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; Salerno, M.; et al. Clinical-Forensic Autopsy Findings to Defeat COVID-19 Disease: A Literature Review. J. Clin. Med. 2020, 9, 2026. [Google Scholar] [CrossRef]
- WHO Interm Guidance Infection Prevention and Control for the safe management of a dead body in the context of COVID-19. J. Hosp. Infect. 2020, 104, 246–251.
- CDC Collection and Submission of Postmortem Specimens from Deceased Persons with Confirmed or Suspected COVID-19. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html (accessed on 11 December 2020).
- Coroners Society of Ireland. Statement of Coroners Service from the Coroners Society of Ireland; Coroners Society of Ireland: Dublin, Ireland, 2020; Available online: http://www.coroners.ie/ (accessed on 11 December 2020).
- Pomara, C.; Fineschi, V. Forensic and Clinical Forensic Autopsy. An Atlas and Handbook, 2nd ed.; Pomara, C., Fineschi, V., Eds.; CRC Press: Baca Rotan, FL, USA, 2020; ISBN 9780367330712. [Google Scholar]
- Lu, X.; Wang, L.; Sakthivel, S.K.; Whitaker, B.; Murray, J.; Kamili, S.; Lynch, B.; Malapati, L.; Burke, S.A.; Harcourt, J.; et al. US CDC real-time reverse transcription PCR panel for detection of severe acute respiratory syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1654. [Google Scholar] [CrossRef]
- Stevens, B.; Hogan, C.A.; Sahoo, M.K.; Huang, C.; Garamani, N.; Zehnder, J.; Kurzer, J.; Pinsky, B.A. Comparison of a Point-of-Care Assay and a High-Complexity Assay for Detection of SARS-CoV-2 RNA. J. Appl. Lab. Med. 2020, 5, 1307–1312. [Google Scholar] [CrossRef]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, P246–P251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Yaacoub, S.; Schünemann, H.J.; Khabsa, J.; El-Harakeh, A.; Khamis, A.M.; Chamseddine, F.; El Khoury, R.; Saad, Z.; Hneiny, L.; Cuello Garcia, C.; et al. Safe management of bodies of deceased persons with suspected or confirmed COVID-19: A rapid systematic review. BMJ Glob. Health 2020, 5, e002650. [Google Scholar] [CrossRef] [PubMed]
- Edler, C.; Schröder, A.S.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 infection—An autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int. J. Leg. Med. 2020, 134, 1275–1284. [Google Scholar] [CrossRef]
- Dijkhuizen, L.G.M.; Gelderman, H.T.; Duijst, W.L.J.M. Review: The safe handling of a corpse (suspected) with COVID-19. J. Forensic Leg. Med. 2020, 73, 101999. [Google Scholar] [CrossRef] [PubMed]
- Martines, R.B.; Ritter, J.M.; Matkovic, E.; Gary, J.; Bollweg, B.C.; Bullock, H.; Goldsmith, C.S.; Silva-Flannery, L.; Seixas, J.N.; Reagan-Steiner, S.; et al. Pathology and Pathogenesis of SARS-CoV-2 Associated with Fatal Coronavirus Disease, United States. Emerg. Infect. Dis. 2020, 26, 2005–2015. [Google Scholar] [CrossRef] [PubMed]
- WHO Rational Use of Personal Protective Equipment for Coronavirus Disease 2019 (COVID-19); World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/rational-use-of-personal-protective-equipment-for-coronavirus-disease-(covid-19)-and-considerations-during-severe-shortages (accessed on 13 December 2020).
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in suspected COVID-19 cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Finegan, O.; Fonseca, S.; Guyomarc’h, P.; Morcillo Mendez, M.D.; Rodriguez Gonzalez, J.; Tidball-Binz, M.; Winter, K.A. International Committee of the Red Cross (ICRC): General guidance for the management of the dead related to COVID-19. Forensic Sci. Int. Synerg. 2020, 2, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Osborn, M.; Lucas, S.B.; Stewart, R.; Swift, B.; Youd, E. Autopsy Practice Relating to Possible Cases of COVID-19 (2019-nCov, Novel Coronavirus from China 2019/2020). Available online: https://www.rcpath.org/uploads/assets/d5e28baf-5789-4b0f-acecfe370eee6223/447e37d0-29dd-4994-a11fe27b93de0905/Briefing-on-COVID-19-autopsy-Feb-2020.pdf (accessed on 18 August 2020).
- Skok, K.; Stelzl, E.; Trauner, M.; Kessler, H.H.; Lax, S.F. Post-mortem viral dynamics and tropism in COVID-19 patients in correlation with organ damage. Virchows Arch. 2020, 1–11. [Google Scholar] [CrossRef]
- Cipolloni, L.; Sessa, F.; Bertozzi, G.; Baldari, B.; Cantatore, S.; Testi, R.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; et al. Preliminary Post-Mortem COVID-19 Evidence of Endothelial Injury and Factor VIII Hyperexpression. Diagnostics 2020, 10, 575. [Google Scholar] [CrossRef]
- Dell’Aquila, M.; Cattani, P.; Fantoni, M.; Marchetti, S.; Aquila, I.; Stigliano, E.; Carbone, A.; Oliva, A.; Arena, V. Postmortem Swabs in the Severe Acute Respiratory Syndrome Coronavirus 2 Pandemic: Report on 12 Complete Clinical Autopsy Cases. Arch. Pathol. Lab. Med. 2020, 144, 1298–1302. [Google Scholar] [CrossRef]
- Sapino, A.; Facchetti, F.; Bonoldi, E.; Gianatti, A.; Barbareschi, M. The autopsy debate during the COVID-19 emergency: The Italian experience. Virchows Arch. 2020, 476, 821–823. [Google Scholar] [CrossRef]
- Pomara, C.; Li Volti, G.; Cappello, F. The post-lockdown era: What is next in Italy? Front. Pharmacol. 2020, 11, 1074. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, P. COVID-19 as a Vascular Disease: Lesson Learned from Imaging and Blood Biomarkers. Diagnostics 2020, 10, 440. [Google Scholar] [CrossRef] [PubMed]
- Keresztesi, A.-A.; Perde, F.; Ghita-Nanu, A.; Radu, C.-C.; Negrea, M.; Keresztesi, G. Post-Mortem Diagnosis and Autopsy Findings in SARS-CoV-2 Infection: Forensic Case Series. Diagnostics 2020, 10, 1070. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SARS-CoV-2 RNA Test Results from Corpses | ||||||
|---|---|---|---|---|---|---|
| Cadaver ID | Age | Sex | COVID-19 rRT-PCR Assay Diagnostic Test Performed on Post-Mortem Swab (Days) | PMI (Days) | Molecular Test for SARS-CoV-2 Using Quantitative RT-PCR (Right Bronchus) | Molecular Test for SARS-CoV-2 Using Quantitative RT-PCR (Left Bronchus) |
| 1 | 50 | F | 58 | 54 | Pos | Pos |
| 2 | 91 | F | NA | 58 | Pos | Pos |
| 3 | 92 | M | 54 | 54 | Pos | Pos |
| 4 | 83 | M | NA | 61 | Pos | Pos |
| 5 | 89 | M | NA | 64 | Pos | Pos |
| 6 | 88 | F | 54 | 50 | Pos | Pos |
| 7 | 93 | F | NA | 78 | Pos | Pos |
| 8 | 79 | F | 19 | 1 | Pos | Pos |
| 9 | 72 | F | 5 | 5 | Pos | Pos |
| 10 | 86 | F | 9 | 1 | Pos | Pos |
| 11 | 64 | M | 30 | 1 | Pos | Pos |
| 12 | 74 | F | 18 | 1 | Pos | Pos |
| 13 | 59 | M | 9 | 1 | Pos | Pos |
| 14 | 59 | M | 7 | 1 | Pos | Pos |
| 15 | 51 | M | 17 | 1 | Pos | Pos |
| 16 | 72 | M | 5 | 1 | Pos | Pos |
| Comparison of Positive Rates between Short PMI and Long PMI | |||||
|---|---|---|---|---|---|
| Short PMI | Long PMI | ||||
| Cadaver ID | Positive Swabs/Total Swabs (Percentage) | Rate (Positive Environmental Swabs/Total Swabs) | Cadaver ID | Positive Swabs/Total Swabs (Percentage) | Rate (Positive Environmental Swabs/Total Swabs) |
| 1 | 7/11 (63.6%) | 0.63 | 8 | 1/11 (9%) | 0.09 |
| 2 | 6/11 (54.5%) | 0.54 | 9 | 5/11 (45.4%) | 0.45 |
| 3 | 5/11 (45.4%) | 0.45 | 10 | 3/11 (27.2%) | 0.27 |
| 4 | 5/11 (45.4%) | 0.45 | 11 | 1/11 (9%) | 0.09 |
| 5 | 4/11 (36.3%) | 0.36 | 12 | 6/11 (54.5%) | 0.54 |
| 6 | 3/11 (27.2%) | 0.27 | 13 | 7/11 (63.6%) | 0.63 |
| 7 | 1/11 (9%) | 0.09 | 14 | 0 (0%) | 0 |
| 15 | 2/11 (18.1%) | 0.18 | |||
| 16 | 4/11 (36.3%) | 0.36 | |||
| Comparison of Positive Rates between “Near Swabs” and “Far Swabs” by Long PMI and Short PMI | |||||
|---|---|---|---|---|---|
| Long PMI | Short PMI | ||||
| Cadaver ID | NEAR SWABS (Autopsy Table + Face Shield) | FAR SWABS (Wall + Floor) | Cadaver ID | NEAR SWABS (Autopsy Table + Face Shield) | FAR SWABS (Wall + Floor) |
| Rate (Positive Environmental Swabs/Total Swabs) | Rate (Positive Environmental Swabs/Total Swabs) | Rate (Positive Environmental Swabs/Total Swabs) | Rate (Positive Environmental Swabs/Total Swabs) | ||
| 1 | 0.83 | 0.4 | 8 | 0.16 | 0 |
| 2 | 0.83 | 0.2 | 9 | 0.66 | 0.2 |
| 3 | 0.66 | 0.2 | 10 | 0.5 | 0 |
| 4 | 0.83 | 0 | 11 | 0.16 | 0 |
| 5 | 0.66 | 0 | 12 | 0.83 | 0.2 |
| 6 | 0.5 | 0 | 13 | 0.83 | 0.4 |
| 7 | 0.16 | 0 | 14 | 0 | 0 |
| 15 | 0.33 | 0 | |||
| 16 | 0.33 | 0.4 | |||
| Mean values | 0.64 ± 0.24 | 0.11 ± 0.15 | Mean values | 0.42 ± 0.3 | 0.13 ± 0.17 |
| Results of t-Test for Each Statistical Analysis Performed | |||||
|---|---|---|---|---|---|
| Positive Rate of Total near Swabs vs. Positive Rate of Total Far Swabs | Positive Rate of near Swabs Long PMI vs. Positive Rate of Far Swabs Long PMI | Positive Rate of near Swabs Short PMI vs. Positive Rate of Far Swabs Short PMI | Positive Rate of near Swabs Long PMI vs. Positive Rate of near Swabs Short PMI | Positive Rate of Far Swabs Long PMI vs. Positive Rate of Far Swabs Short PMI | |
| t-test values | p < 0.05 | p < 0.05 | p < 0.05 | n.s. | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomara, C.; Salerno, M.; Sessa, F.; Esposito, M.; Barchitta, M.; Ledda, C.; Grassi, P.; Liberto, A.; Mattaliano, A.R.; Rapisarda, V.; et al. Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases. Diagnostics 2021, 11, 457. https://doi.org/10.3390/diagnostics11030457
Pomara C, Salerno M, Sessa F, Esposito M, Barchitta M, Ledda C, Grassi P, Liberto A, Mattaliano AR, Rapisarda V, et al. Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases. Diagnostics. 2021; 11(3):457. https://doi.org/10.3390/diagnostics11030457
Chicago/Turabian StylePomara, Cristoforo, Monica Salerno, Francesco Sessa, Massimiliano Esposito, Martina Barchitta, Caterina Ledda, Patrizia Grassi, Aldo Liberto, Anna Rita Mattaliano, Venerando Rapisarda, and et al. 2021. "Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases" Diagnostics 11, no. 3: 457. https://doi.org/10.3390/diagnostics11030457
APA StylePomara, C., Salerno, M., Sessa, F., Esposito, M., Barchitta, M., Ledda, C., Grassi, P., Liberto, A., Mattaliano, A. R., Rapisarda, V., Ferrante, M., & Agodi, A. (2021). Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases. Diagnostics, 11(3), 457. https://doi.org/10.3390/diagnostics11030457