
Evidence of TB Services at Primary Healthcare Level during COVID-19: A Scoping Review

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
- Studies reporting on TB services during COVID-19;
- Studies reporting on TB services at PHC;
- All of the publications reporting evidence on TB services during COVID-19 at PHC, regardless of study design;
- Studies from all countries around the world.
- Studies reporting on TB services outside the PHC level;
- Studies reporting evidence on TB services and viral diseases other than COVID-19;
- Studies reporting evidence on health services other than TB during COVID-19;
- Publications from before 2020.
2.2. Quality Appraisal
2.3. Collating, Summarizing, and Reporting Results
3. Results
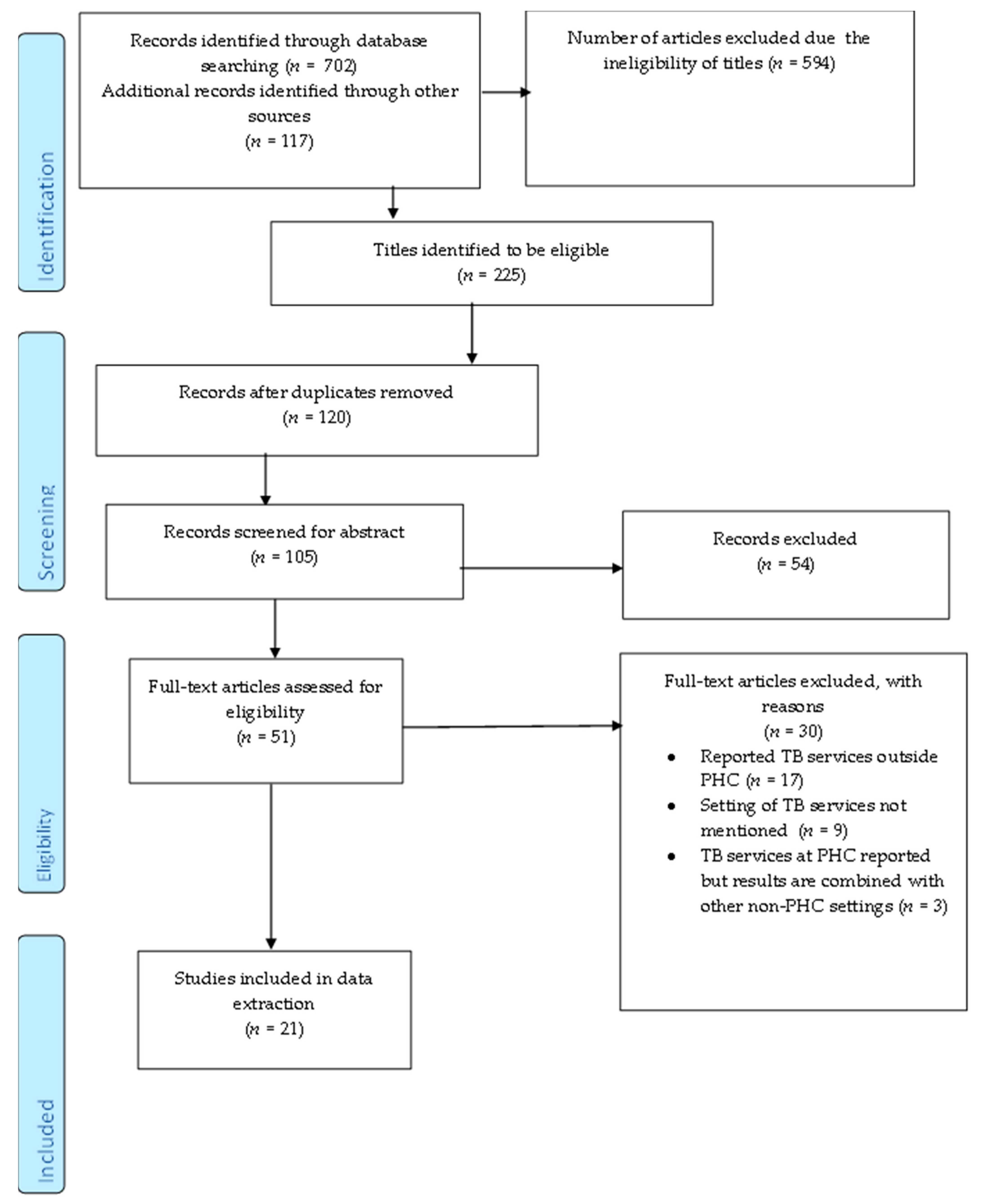
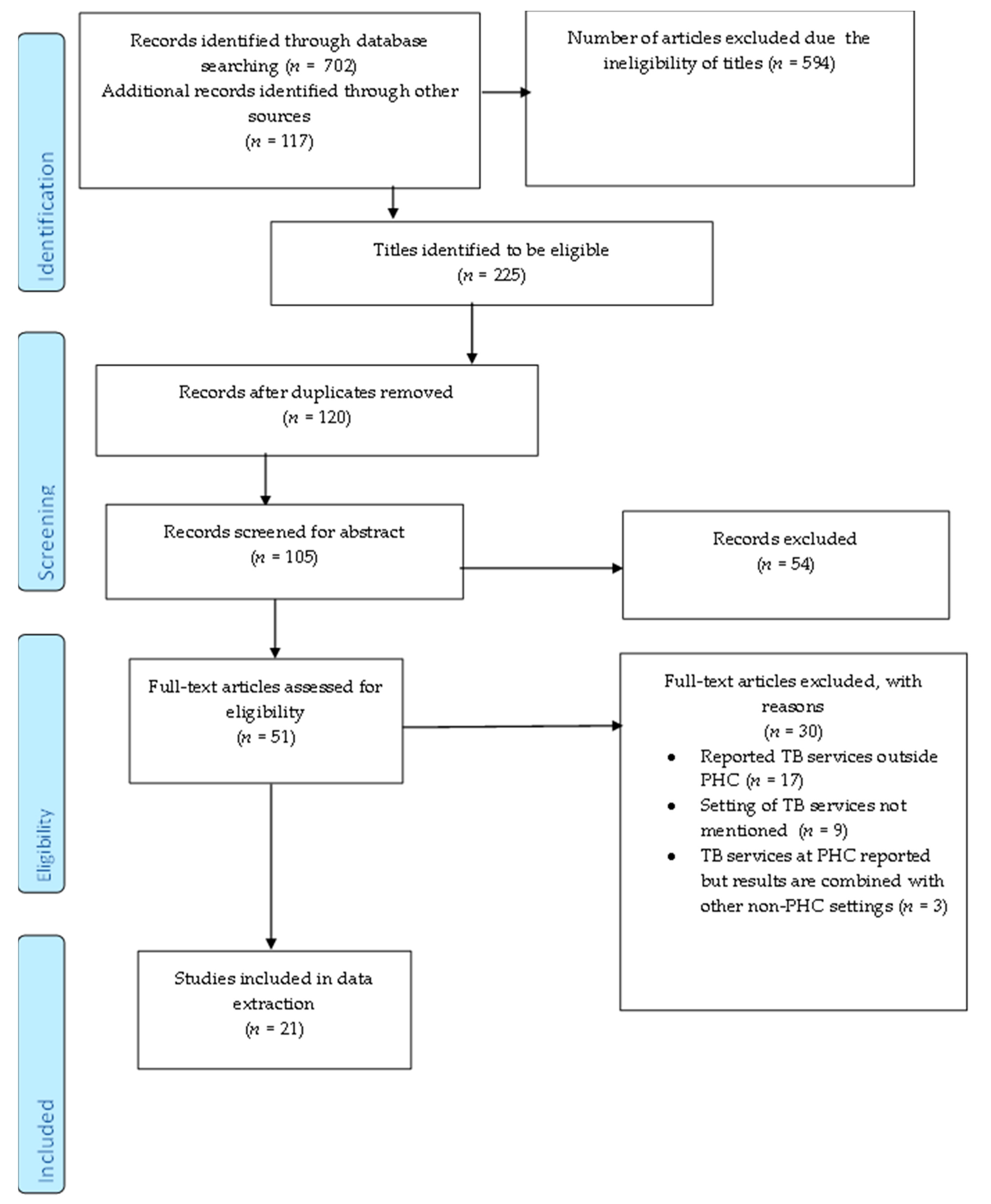
3.1. Screening Results
3.2. Characteristics of the Included Studies
3.3. Quality Appraisal
3.4. Summary of the Evidence
3.4.1. Consequences of the COVID-19 Pandemic on TB Services
3.4.2. Patient and Provider Experiences
3.4.3. Recommendations and Adaptations of TB Services
3.4.4. Implementing the Recommendations for TB Services
4. Discussion
4.1. Implication for Research
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Section and Topic | Item No. | Checklist Item | Reported on Page |
|---|---|---|---|
| ADMINISTRATIVE INFORMATION | |||
| Title: | |||
| Identification | 1 | Evidence of TB services at the primary healthcare level during COVID-19: A scoping review. | 1 |
| Registration | 2 | Open Science Framework: https://osf.io/pq3ba (accessed on 16 September 2021) | |
| INTRODUCTION | |||
| Rationale | 3 | Despite the availability of vaccinations and chemotherapy for prevention and treatment [1], 10 million new cases of tuberculosis (TB) were recorded in 2019 [2]. A third of these cases were missed by health systems [3], and considerably more were not started on an appropriate treatment [1]. These missed cases contribute to the ongoing transmission [4], while prolonged diagnosis and treatment initiation exacerbate disease severity and continued spread [5]. Interrupting transmission through early and accurate detection, rapid treatment initiation, and completion, preferably at the primary healthcare level (PHC), aids efforts in ending the TB epidemic [3,6]. In 2020, COVID-19 emerged, hindering global TB control efforts [7], many routine TB services were sidelined in response to the COVID-19 pandemic [8,9]. These services suffered a sharp decline due to lockdowns limiting access to healthcare and a rise in fear and stigma since the advent of COVID-19 [8,10,11]. Studies that predict the potential impact of COVID-19 on TB services suggest that temporary disruptions in response to COVID-19 will likely affect all aspects of the TB care cascade [12,13,14]. Even small disruptions to these services could have long-term consequences on TB control [12]. These will especially be felt by high burden countries where TB incidence and mortality have been predicted to increase by 6.3 and 1.4 million between 2020–2025, respectively [12]. Delays in patients seeking timely diagnosis and treatment are listed as the potential drivers for these grim outcomes [12,14]. The World Health Organization’s (WHO) End TB strategy and the sustainable development goal (SDGs) 3.3 aim to end TB through timely diagnosis and treatment, treatment adherence, and preventative therapy [15,16]. The WHO aims to eliminate the TB epidemic by 2035 and has also set short-term milestones to reduce TB deaths and incidence rates by 2020 and 2025 [3,15]. Findings from the TB global health report showed that 2020 milestones were not achieved [3]. Similarly, interim targets were set by the United Nations (UN) to diagnose and treat 40 million additional people by 2022 [7]. Although progress towards these goals has been made, it is below the threshold that would make TB elimination attainable [3,18]. It is also possible that the small gains made towards controlling TB were disrupted by the COVID-19 pandemic, pushing the global TB targets further into the future [7,19]. As the first point of contact with health services, PHC can reach large proportions of the population. It also promotes equitable access to health services and continuity of care and is thereby recognized as a powerful way that health SDGs can be achieved [16,20]. The WHO has also emphasized that progress towards containing the TB epidemic can accelerate when TB control has been integrated with PHC [21]. Furthermore, high-quality PHC services are an important predictor for whether TB control strategies will realize their promise [22]. Despite the emergence of other public health priorities, such as the COVID-19 pandemic, uninterrupted TB services at PHC are crucial for TB targets to be reached. Given the novelty of the COVID-19 pandemic, its effects on TB services at the PHC level remain unclear and require further exploration. Therefore, this review aimed to systematically map evidence on TB services at the PHC level during the COVID-19 pandemic. The evidence obtained from the study will be used to develop primary research that is aimed at addressing and improving TB services at the PHC level during the COVID-19 pandemic to accelerate global efforts to end TB. | 3–4 |
| Objectives | 4 | This review aimed to systematically map evidence on TB services at the PHC level during the COVID-19 pandemic. | 4 |
| METHODS | |||
| Eligibility criteria | 5 | Inclusion criteria Publications that adhere to the following criteria were included:
This review excluded studies based on the following:
| 6 |
| Information sources | 6 | We conducted an advanced search using the following five academic databases: PubMed, Web of Science, Medline OVID, Medline EBSCO, and Scopus. | 5 |
| Search strategy | 7 | Studies were identified using the following keywords and medical subject heading (MeSH) terms: “TB diagnostics”, “Health Service” “TB testing” “COVID-19”, “SARS-CoV-2”, “COVID-19 Pandemic”, “COVID-19 era” and “Primary healthcare”. A combination of medical subject headings (MeSH) and free word texts of the keywords were used when conducting the searches. WHO and Stop TB partnership websites were accessed for reports and the reference lists of all the included studies were consulted for additional literature. | 5–6 |
| Study records: | |||
| Data management | 8a | Describe the mechanism(s) that will be used to manage records and data throughout the review. | |
| Selection process | 8b | The studies were selected in three phases. First, the principal investigator screened the titles of each article using the eligibility criteria as a guide. Eligible articles were exported to an EndNote20 library where duplicates were identified and removed. In the second phase, two independent reviewers screened the abstracts of the included articles using a screening tool developed through the use of the inclusion and exclusion criteria. The screening tool was piloted and adjusted using 10 articles before the screening process was conducted. The reviewers discussed any discrepancies that arose until they reached a consensus on the articles to select. In the third phase, the two reviewers screened the full texts of the relevant articles using a screening tool guided by eligibility criteria. Before use, the screening tool was piloted by both screeners, and changes were made accordingly. Discrepancies during full-text screening were resolved by a third reviewer. The level of agreement between the two reviewers was calculated using McNemar’s Chi-square statistic. | 6 |
| Data collection process | 8c | An electronic data charting form containing variables relevant to the research question was developed. Two independent reviewers then piloted the data extraction tool using 10 of the included studies. The necessary changes were applied according to the feedback given by the reviewers. | 7 |
| Data items | 9 | Data were extracted from the included studies based on the following categories: Author, aim, type of publication, country, type of TB service, and primary healthcare provider. | 7 |
| Data synthesis | 10 | We employed thematic analysis to extract relevant evidence to answer our research questions and presented a narrative summary that centered around the emerging themes. The themes that arose most from the included studies were as follows: The unintended consequences of COVID-19 on TB services; comparison of TB services before and after COVID-19; patient experiences of TB services during COVID-19; and recommendations for TB services at PHC during COVID-19. | 7 |
| Confidence in cumulative evidence | 11 | To assess the risk of bias we determined the quality of the included studies using the mixed methods appraisal tool (MMAT) V.2018 software [27]. The tool assessed the methodological quality of the included primary studies. The particular study design guided how the article was appraised, following stipulations by the MMAT guidelines. Once the scores for each study were calculated as a percentage, they were given a specific rank. Studies equal to or below 50% were ranked as low quality, those between 51–75% were deemed average quality, and those ranging from 76–100% were given a high-quality score. | 7 |
References
- Bloom, B.R.; Atun, R.; Cohen, T.; Dye, C.; Fraser, H.; Gomez, G.B.; Knight, G.; Murray, M.; Nardell, E.; Rubin, E.; et al. Tuberculosis; The World Bank: Washington, DC, USA, 2017; pp. 233–313. [Google Scholar]
- Tuberculosis. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 8 March 2021).
- Chakaya, J.; Khan, M.; Ntoumi, F.; Aklillu, E.; Fatima, R.; Mwaba, P.; Kapata, N.; Mfinanga, S.; Hasnain, S.E.; Katoto, P.D.M.C.; et al. Global Tuberculosis Report 2020—Reflections on the Global TB burden, treatment and prevention efforts. Int. J. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pai, M.; Nicol, M.P.; Boehme, C.C. Tuberculosis Diagnostics: State of the Art and Future Directions. Microbiol. Spectr. 2016, 4, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Nathavitharana, R.R. Stamping out tuberculosis: The importance of diagnostic innovation and effective implementation. Ann. Am. Thorac. Soc. 2019, 16, 1112–1113. [Google Scholar] [CrossRef]
- Dheda, K.; Ruhwald, M.; Theron, G.; Peter, J.; Yam, W.C. Point-of-care diagnosis of tuberculosis: Past, present and future. Respirology 2013, 18, 217–232. [Google Scholar] [CrossRef] [PubMed]
- Sahu, S.; Ditiu, L.; Sachdeva, K.S.; Zumla, A. Recovering from the Impact of the Covid-19 Pandemic and Accelerating to Achieving the United Nations General Assembly Tuberculosis Targets. Int. J. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Alene, K.A.; Wangdi, K.; Clements, A.C.A. Impact of the COVID-19 Pandemic on Tuberculosis Control: An Overview. Trop. Med. Infect. Dis. 2020, 5, 123. [Google Scholar] [CrossRef] [PubMed]
- Fei, H.; Yinyin, X.; Hui, C.; Ni, W.; Xin, D.; Wei, C.; Tao, L.; Shitong, H.; Miaomiao, S.; Mingting, C.; et al. The impact of the COVID-19 epidemic on tuberculosis control in China. Lancet Reg. Health West. Pac. 2020, 3, 100032. [Google Scholar] [CrossRef]
- Karim, Q.A.; Karim, S.S.A. COVID-19 affects HIV and tuberculosis care. Science 2020, 369, 366–368. [Google Scholar] [CrossRef]
- Jain, V.K.; Iyengar, K.P.; Samy, D.A.; Vaishya, R. Tuberculosis in the era of COVID-19 in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1439–1443. [Google Scholar] [CrossRef]
- Cilloni, L.; Fu, H.; Vesga, J.F.; Dowdy, D.; Pretorius, C.; Ahmedov, S.; Nair, S.A.; Mosneaga, A.; Masini, E.; Sahu, S.; et al. The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis. EClinicalMedicine 2020, 28, 100603. [Google Scholar] [CrossRef]
- McQuaid, C.F.; McCreesh, N.; Read, J.M.; Sumner, T.; Houben, R.; White, R.G.; Harris, R.C. The potential impact of COVID-19-related disruption on tuberculosis burden. Eur. Respir. J. 2020, 56, 2001718. [Google Scholar] [CrossRef]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- Uplekar, M.; Weil, D.; Lonnroth, K.; Jaramillo, E.; Lienhardt, C.; Dias, H.M.; Falzon, D.; Floyd, K.; Gargioni, G.; Getahun, H.; et al. WHO′s new end TB strategy. Lancet 2015, 385, 1799–1801. [Google Scholar] [CrossRef]
- Hone, T.; Macinko, J.; Millett, C. Revisiting Alma-Ata: What is the role of primary health care in achieving the Sustainable Development Goals? Lancet 2018, 392, 1461–1472. [Google Scholar] [CrossRef]
- World Health Organization. Global tuberculosis report 2020. Available online: https://www.who.int/publications/i/item/9789240013131 (accessed on 11 July 2021).
- World Health Organization. End TB Strategy. Available online: https://www.who.int/tb/End_TB_brochure.pdf?ua=1 (accessed on 25 April 2021).
- Zumla, A.; Chakaya, J.; Khan, M.; Fatima, R.; Wejse, C.; Al-Abri, S.; Fox, G.J.; Nachega, J.; Kapata, N.; Knipper, M.; et al. World Tuberculosis Day 2021 Theme-‘THE CLOCK IS TICKING’- and the world is running out of time to deliver the United Nations General Assembly commitments to End TB due to the COVID-19 pandemic. Int. J. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Binagwaho, A.; Adhanom Ghebreyesus, T. Primary healthcare is cornerstone of universal health coverage. BMJ 2019, 365, 12391. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Brief Guide on Tuberculosis Control for Primary Health Care Providers for Countries in the WHO European Region with a High and Intermediate Burden of Tuberculosis. Available online: https://www.euro.who.int/__data/assets/pdf_file/0015/123162/E82858.pdf (accessed on 20 July 2021).
- Davis, J.; Katamba, A.; Vasquez, J.; Crawford, E.; Sserwanga, A.; Kakeeto, S.; Kizito, F.; Dorsey, G.; Den Boon, S.; Vittinghoff, E.; et al. Evaluating Tuberculosis Case Detection via Real-Time Monitoring of Tuberculosis Diagnostic Services. Am. J. Respir. Crit. Care Med. 2011, 184, 362–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O′Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O′Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O′Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Apprais. Tool (MMAT), Version 2018; Registration of Copyright (#1148552); Canadian Intellectual Property Office: Ottawa, ON, Canada, 2018. [Google Scholar]
- Aguiar, A.; Furtado, I.; Sousa, M.; Pinto, M.; Duarte, R. Changes to TB care in an outpatient centre during the COVID-19 pandemic. Int. J. Tuberc. Lung Dis. 2021, 25, 163b–166. [Google Scholar] [CrossRef] [PubMed]
- Beyene, N.W.; Sitotaw, A.L.; Tegegn, B.; Bobosha, K. The impact of COVID-19 on the tuberculosis control activities in Addis Ababa. Pan Afr. Med. J. 2021, 38, 243. [Google Scholar] [CrossRef]
- Senoo, Y.; Suzuki, Y.; Takahashi, K.; Tsuda, K.; Tanimoto, T. Prioritizing infants in a time of Bacille Calmette–Guérin vaccine shortage caused by premature expectations against COVID-19. QJM Int. J. Med. 2020, 113, 773–774. [Google Scholar] [CrossRef]
- Soko, R.N.; Burke, R.M.; Feasey, H.R.A.; Sibande, W.; Nliwasa, M.; Henrion, M.Y.R.; Khundi, M.; Dodd, P.J.; Ku, C.C.; Kawalazira, G.; et al. Effects of Coronavirus Disease Pandemic on Tuberculosis Notifications, Malawi. Emerg. Infect. Dis. 2021, 27, 1831–1839. [Google Scholar] [CrossRef] [PubMed]
- Burzynski, J.J.; Macaraig, M.; Nilsen, D.; Schluger, N.W. Transforming essential services for tuberculosis during the COVID-19 pandemic: Lessons from New York City. Int. J. Tuberc. Lung Disease 2020, 24, 735–736. [Google Scholar] [CrossRef]
- Jamal, W.Z.; Habib, S.; Khowaja, S.; Safdar, N.; Zaidi, S.M.A. COVID-19: Ensuring continuity of TB services in the private sector. Int. J. Tuberc. Lung Dis. 2020, 24, 870–872. [Google Scholar] [CrossRef]
- Fatima, R.; Akhtar, N.; Yaqoob, A.; Harries, A.D.; Khan, M.S. Building better tuberculosis control systems in a post-COVID world: Learning from Pakistan during the COVID-19 pandemic. Int. J. Infect. Dis. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Adewole, O.O. Impact of COVID-19 on TB care: Experiences of a treatment centre in Nigeria. Int. J. Tuberc. Lung Dis. 2020, 24, 981–982. [Google Scholar] [CrossRef]
- Debriche Health Development Centre. Webinar on the Impact of COVID-19 on TB and PHC Services in Nigeria. Available online: https://stoptb-strategicinitiative.org/index.php/2020/07/12/webinar-on-the-impact-of-covid-19-on-tb-and-phc-services-in-nigeria/ (accessed on 18 August 2021).
- Adepoju, P. Tuberculosis and HIV responses threatened by COVID-19. Lancet HIV 2020, 7, e319–e320. [Google Scholar] [CrossRef]
- Rai, D.K.; Kumar, R. Problems faced by tuberculosis patients during COVID-19 pandemic: Urgent need to intervene. Indian J. Tuberc. 2020, 67, S173–S174. [Google Scholar] [CrossRef] [PubMed]
- Datta, B.; Jaiswal, A.; Goyal, J.; Prakash, A.; Tripathy, J.; Trehan, N. The untimely demise of the TB Free block model in the wake of coronavirus disease 2019 in India. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 789–791. [Google Scholar] [CrossRef] [PubMed]
- Meneguim, A.C.; Rebello, L.; Das, M.; Ravi, S.; Mathur, T.; Mankar, S.; Kharate, S.; Tipre, P.; Oswal, V.; Iyer, A.; et al. Adapting TB services during the COVID-19 pandemic in Mumbai, India. Int. J. Tuberc. Lung Dis. Off. J. Int. Union Against Tuberc. Lung Dis. 2020, 24, 1119–1121. [Google Scholar] [CrossRef]
- Pilane, P. Covid-19 disrupts HIV and TB services. Mail Guardian 2020. Available online: https://mg.co.za/coronavirus-essentials/2020-09-04-covid-19-sets-hiv-treatment-and-testing-back/ (accessed on 21 September 2021).
- Keene, C.; Mohr-Holland, E.; Cassidy, T.; Scott, V.; Nelson, A.; Furin, J.; Triviño-Duran, L. How COVID-19 could benefit tuberculosis and HIV services in South Africa. Lancet Respir. Med. 2020, 8, 844–846. [Google Scholar] [CrossRef]
- Ongole, J.J.; Rossouw, T.M.; Fourie, P.B.; Stoltz, A.C.; Hugo, J.; Marcus, T.S. Sustaining essential healthcare in Africa during the COVID-19 pandemic. Int. J. Tuberc. Lung Dis. 2020, 24, 643–645. [Google Scholar] [CrossRef] [PubMed]
- Cox, V.V.; Wilkinson, L.; Grimsrud, A.; Hughes, J.; Reuter, A.; Conradie, F.; Nel, J.; Boyles, T. Critical changes to services for TB patients during the COVID-19 pandemic. Int. J. Tuberc. Lung Dis. 2020, 24, 542–544. [Google Scholar] [CrossRef]
- Comella-Del-Barrio, P.; De Souza-Galvão, M.L.; Prat-Aymerich, C.; Domínguez, J. Impact of COVID-19 on Tuberculosis Control. Arch. Bronconeumol. 2021, 57 (Suppl. 2), 5–6. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization (WHO) Information Note: Tuberculosis and COVID-19. Available online: https://www.who.int/docs/default-source/documents/tuberculosis/infonote-tb-covid-19.pdf (accessed on 15 August 2021).
- Stop TB Partnership. The Impact of COVID-19 on the TB Epidemic: A Community Perspective. Available online: http://www.stoptb.org/assets/documents/resources/publications/acsm/Civil%20Society%20Report%20on%20TB%20and%20COVID.pdf (accessed on 15 August 2021).
- Ansumana, R.; Keitell, S.; Roberts, G.M.T.; Ntoumi, F.; Petersen, E.; Ippolito, G.; Zumla, A. Impact of infectious disease epidemics on tuberculosis diagnostic, management, and prevention services: Experiences and lessons from the 2014–2015 Ebola virus disease outbreak in West Africa. Int. J. Infect. Dis. 2017, 56, 101–104. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, S.J.; Silverberg, S.L. Delays in Global Disease Outbreak Responses: Lessons from H1N1, Ebola, and Zika. Am. J. Public Health 2018, 108, 329–333. [Google Scholar] [CrossRef]
- Zumla, A.; Hui, D.S.C. Emerging and Reemerging Infectious Diseases: Global Overview. Infect. Dis. Clin. North Am. 2019, 33, xiii–xix. [Google Scholar] [CrossRef]
- Alfaraj, S.H.; Al-Tawfiq, J.A.; Altuwaijri, T.A.; Memish, Z.A. Middle East Respiratory Syndrome Coronavirus and Pulmonary Tuberculosis Coinfection: Implications for Infection Control. Intervirology 2017, 60, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Alvarez, M.; Jarde, A.; Usuf, E.; Brotherton, H.; Bittaye, M.; Samateh, A.L.; Antonio, M.; Vives-Tomas, J.; D′Alessandro, U.; Roca, A. COVID-19 pandemic in west Africa. Lancet Glob. Health 2020, 8, e631–e632. [Google Scholar] [CrossRef]
- Stop TB Partnership. The potential impact of the COVID-19 response on tuberculosis in high-burden countries: A modelling analysis. Available online: http://www.stoptb.org/assets/documents/news/Modeling%20Report_1%20May%202020_FINAL.pdf (accessed on 5 July 2021).
- Obied, D.A.; Alhamlan, F.S.; Al-Qahtani, A.A.; Al-Ahdal, M.N. Containment of COVID-19: The unprecedented response of Saudi Arabia. J. Infect. Dev. Ctries. 2020, 14, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Algaissi, A.A.; Alharbi, N.K.; Hassanain, M.; Hashem, A.M. Preparedness and response to COVID-19 in Saudi Arabia: Building on MERS experience. J. Infect. Public Health 2020, 13, 834–838. [Google Scholar] [CrossRef] [PubMed]
| Determinants | Description |
|---|---|
| Population | Primary healthcare providers—healthcare practitioners providing TB services, which are the first point of contact between people in a community and the healthcare system. |
| Concept | TB services—the processes involved in finding, diagnosing, treating, and preventing TB, which leads to cases being notified to national health systems. |
| Context | COVID-19 era—the time since COVID-19 emerged, from January 2020 to date. |
| Date | Database | Keywords | Number of Results Retrieved |
|---|---|---|---|
| 7 June 2021 | PubMed | ((“Health Services” [Mesh] OR “primary health care” [MeSH Terms] OR “Primary health care” [Text Word] OR “health care” [Text Word] OR “health service*” [Text Word] OR “Primary healthcare” [Text Word]) AND (“sars-cov-2” [MeSH Terms] OR “covid-19” [MeSH Terms] OR covid [Text Word] OR coronavirus OR “corona virus”)) AND (“tuberculosis” [MeSH Terms] OR tuberculosis [Text Word]) | 191 |
| 7 June 2021 | PubMed | ((“primary health care” [MeSH Terms] OR “Primary health care” [Text Word] OR “Primary healthcare” [Text Word]) AND (“sars-cov-2” [MeSH Terms] OR “covid-19” [MeSH Terms] OR covid [Text Word] OR coronavirus OR “corona virus”)) AND (“tuberculosis” [MeSH Terms] OR tuberculosis [Text Word]) | 13 |
| 11 June 2021 | Web of Science | (TITLE-ABS-KEY (tuberculosis OR tb) AND TITLE-ABS-KEY (sars-cov-2 OR covid-19 OR covid OR coronavirus OR“corona AND virus”) AND TITLE-ABS-KEY (“primary health care” OR “primary AND healthcare” OR “primary AND care” OR “Health Services”)) | 5 |
| 7 June 2021 | Medline OVID | (((MH “COVID-19”)) OR “covid-19” OR ((MH “SARS-CoV-2”)) OR “sars-cov-2”) AND (((MH “Tuberculosis+”)) OR “tuberculosis”) AND (((MH “Primary Health Care”)) OR (“primary health care”) OR ((MH “Health Services+”)) OR (“health services”) OR (“primary health”)) | 223 |
| 7 June 2021 | Medline EBSCO | (((MH “COVID-19”)) OR “covid-19” OR ((MH “SARS-CoV-2”)) OR “sars-cov-2”) AND (((MH “Tuberculosis+”)) OR “tuberculosis”) AND (((MH “Primary Health Care”)) OR (“primary health care”) OR ((MH “Health Services+”)) OR (“health services”) OR (“primary health”)) | 189 |
| 7 June 2021 | Scopus | (TITLE-ABS-KEY (tuberculosis OR tb) AND TITLE-ABS-KEY (sars-cov-2 OR covid-19 OR covid OR coronavirus OR “corona AND virus”) AND TITLE-ABS-KEY (“primary health care” OR “primary AND healthcare” OR “primary AND care” OR “Health Services”)) | 81 |
| Author and Date | Aim of Study | Publication Type | Country | Primary Healthcare Provider | Type of TB Service(s) Reported |
|---|---|---|---|---|---|
| Fatima et al. 2021 [34] | To demonstrate how TB services were strengthened during COVID-19 | Research article | Pakistan | PHC centers, private healthcare providers (PHCP) | General TB services and case notifications |
| Aguiar 2021 [28] | To show the changes made at a TB outpatient center as a result of COVID-19 | Letter | Portugal | Outpatient center | TB case finding and treatment |
| Beyene et al. 2021 [29] | To assess the impact of COVID-19 on TB control programs at various clinics in Addis Ababa | Research article | Ethiopia | Public health clinics | TB screening and testing |
| Comella-del-Barrio et al. 2021 [45] | To give an overview of the effects of COVID-19 on TB control | Editorial | Low to middle-income countries (LMIC) | Primary healthcare in general | TB testing |
| Fei et al. 2020 [9] | To show how COVID-19 has affected TB control in China | Research article | China | Primary healthcare workers and clinics | General TB services |
| Adewole 2020 [35] | How COVID-19 has impacted TB care in Nigeria | Letter | Nigeria | TB clinic | TB case notification and detection |
| Burzynsky et al. 2020 [32] | To show how TB services have been adapted for COVID-19 during the closure of non-essential services in New York | Letter | United States of America | TB clinics | TB detection, testing, and treatment |
| Cox et al. 2021 [44] | To provide recommendations for TB care during COVID-19 in high burden settings | Letter | Countries with a high TB burden | Clinics | TB treatment |
| Keene et al. 2020 [42] | How TB and HIV services can leverage the COVID-19 pandemic | Expert Opinion | South Africa | Clinics | TB screening, testing, treatment, and detection |
| Rai and Kumar 2020 [38] | How TB patients were affected by the lockdown in India | Letter | India | Pharmacists, outpatient department, and general practitioners (GP) | TB treatment |
| World Health Organization 2020 [46] | To give guidance on how TB care should be conducted during COVID-19 | Report | All countries | Outpatient centers and primary healthcare workers | TB treatment |
| Stop TB partnership 2020 [47] | To show how COVID-19 has impacted different TB stakeholders around the world | Report Survey | Global fund implementing countries | Clinics | General TB services |
| Soko et al. 2021 [31] | To estimate the impact of COVID-19 on TB case notifications | Research Article | Malawi | Primary healthcare centers | TB case notifications |
| Meneguim et al. 2020 [40] | How a TB center adapted its service for COVID-19 in India | Letter | India | Outpatient hospital department | TB diagnostics, treatment, follow-up, and adherence support |
| Pilane et al. 2020 [41] | Reporting disruption of TB and HIV services due to COVID-19 | News Article | South Africa | PHC facilities | General TB services |
| Datta et al. 2020 [40] | To show how COVID-19 disrupted a TB free block model pilot study | Report | India | Mobile diagnostic services | Active case-finding and TB diagnostics |
| Debriche Health and Development Center 2020 [36] | To discuss how TB and PHC services have been impacted by COVID-19 and propose solutions | Webinar | Nigeria | PHC centers | General TB services |
| Adepoju 2020 [37] | To demonstrate how COVID-19 has affected TB care | Feature | Nigeria | PHC centers and clinics | TB screening and treatment |
| Jamal et al. 2020 [33] | To detail how TB services were maintained in the private sector during COVID-19 | Letter | Pakistan | GPs | TB treatment and diagnostics |
| Ongole et al. 2020 [43] | To give insight into how TB care can be conducted during COVID-19 through strengthened PHC | Letter | South Africa | PHC centers | General TB services at PHC |
| Senoo et al. 2020 [30] | To report on the shortages of the BCG vaccine | Letter | Japan | Clinics | TB vaccinations |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dlangalala, T.; Musekiwa, A.; Brits, A.; Maluleke, K.; Jaya, Z.N.; Kgarosi, K.; Mashamba-Thompson, T. Evidence of TB Services at Primary Healthcare Level during COVID-19: A Scoping Review. Diagnostics 2021, 11, 2221. https://doi.org/10.3390/diagnostics11122221
Dlangalala T, Musekiwa A, Brits A, Maluleke K, Jaya ZN, Kgarosi K, Mashamba-Thompson T. Evidence of TB Services at Primary Healthcare Level during COVID-19: A Scoping Review. Diagnostics. 2021; 11(12):2221. https://doi.org/10.3390/diagnostics11122221
Chicago/Turabian StyleDlangalala, Thobeka, Alfred Musekiwa, Alecia Brits, Kuhlula Maluleke, Ziningi Nobuhle Jaya, Kabelo Kgarosi, and Tivani Mashamba-Thompson. 2021. "Evidence of TB Services at Primary Healthcare Level during COVID-19: A Scoping Review" Diagnostics 11, no. 12: 2221. https://doi.org/10.3390/diagnostics11122221
APA StyleDlangalala, T., Musekiwa, A., Brits, A., Maluleke, K., Jaya, Z. N., Kgarosi, K., & Mashamba-Thompson, T. (2021). Evidence of TB Services at Primary Healthcare Level during COVID-19: A Scoping Review. Diagnostics, 11(12), 2221. https://doi.org/10.3390/diagnostics11122221