1. Introduction
Regarding spine surgery, evaluating spinal alignment before surgery is routinely performed because there are reports of a significant relationship between sagittal alignment and postoperative patient-reported outcome scores [
1,
2,
3]. The current first choice for assessing sagittal alignment is a whole-spine standing lateral radiograph, which is simple, easy to access, cost-effective, and involve a single brief exposure [
4]. In the last few years, antero-posterior and latero-lateral projections (EOS imaging system) have been made available for orthopedic applications. The EOS
® slot scanner (EOS imaging, Paris, France) is a proprietary imaging technique based on ultrasensitive X-ray detection technology, which was launched in 2007. This imaging modality depicts the patient’s natural, weight-bearing posture by taking frontal and lateral images of the patient’s body with a very low radiation dose (50–80% less than conventional X-rays) and high image quality [
5]. Unlike conventional radiography systems, EOS images do not cause distortions between the center and edges of the radiograph, because linear X-ray sources and detector arrays move together [
6]. This full-body EOS enables evaluation of the global alignment of the spine, pelvis, and lower limbs, which is important in diagnosing spinal deformity and surgical outcomes [
7,
8,
9,
10,
11]. Hence, EOS images are increasingly becoming routine before spine surgery [
12].
For preoperative image analysis, reliability and reproducibility should be high. A recent study of whole-body alignment in adolescent idiopathic scoliosis (AIS) reported that most parameters measured by serial EOS images in this group are generally reproducible [
13,
14]. A study of EOS-based measurement of the sagittal alignment of the spine and pelvis in patients without congenital anomaly, deformity, or previous history of spine and pelvis surgery showed excellent intra-rater and inter-rater reliability [
15]. In adult patients with lower extremity mechanical axis malalignment, EOS-based measurements were reproducible and showed excellent statistical reliability, comparable to the gold standard of conventional radiographs [
16].
However, another study comparing serial whole-body sagittal alignment images in adult patients with mild low back pain showed that the sagittal vertical axis (SVA) has the largest variation between individuals of low pelvic tilt (PT) due to reflections of dynamism in spinal balancing [
17]. There are limited data on the interval difference of sagittal parameters for preoperative assessments in adult patients with severe pain requiring surgery. If the reproducibility of images performed serially for the preoperative analysis is low, this will cast doubt on the reliability of EOS-based measurements for accurate surgical planning.
There is a need to analyze the possible changes in measurement parameters when EOS is taken at regular intervals in patients with sufficient pain who undergo surgery. Moreover, if statistically significant interval changes between two measurements can occur over a certain period, it may be necessary to retake the EOS images shortly before surgery. Therefore, this study assessed the variations in sagittal spinal alignment on serial EOS imaging in adult patients before spine surgery.
4. Discussion
In the evaluation and treatment of spinal disease, the sagittal balance of the spine and pelvis is the most important [
19]. Conventionally, for sagittal curvature evaluation, whole-spine standing lateral radiography is widely performed based on its easy usability and simplicity, showing good intra-observer reliability and a good-to-excellent inter-rater reproducibility [
20]. However, whole-spine standing lateral radiography has several limitations. The distortion between the center and edges of the radiograph results in measurement errors due to the enlargement of structures located far from the central region [
21]. To assess the whole lateral view, it is necessary to combine split images, with the possibility of distortion. The patient’s movements during radiography induced by relatively long sagittal image acquisition times cause a change in sagittal alignment. After developing EOS, these limitations were overcome by allowing a single-shot image and a shorter acquisition time (8 to 15 s), presenting the possibility of low-dose radiation exposure. According to recently published clinical reports, the EOS average skin dose was reduced from six to nine times in the thoracoabdominal region compared with that of computed radiography [
21]. The dose-area product of EOS is as low as 38% of that of standard digital radiography systems [
22]. With the aid of paired X-ray sources and detectors that move in tandem, EOS has no geometric magnification. Moreover, EOS does not need to stitch multiple images together to produce complete spinal lateral images due to its ability to scan a full-body image. Regarding Cobb’s angle measurements, EOS provides comparable accuracy and reproducibility in both pre- and post-operative adolescent idiopathic scoliosis patients compared with CT [
23,
24]. Furthermore, EOS gives lower labor costs per examination due to the shorter examination time (248 s to complete EOS vs. 449 s for standard digital radiography) and greater patient comfort regarding noise, compared with standard digital radiographs [
22]. For these reasons, EOS imaging is an attractive alternative to conventional radiography for spine or whole-body alignment evaluation [
25].
However, before using this new low-radiation-dose X-ray device, the accuracy and reliability should be checked. In a study by Kim et al., the EOS system showed excellent intra-rater (intraclass correlation coefficients (ICCs) ranging from 0.898 to 0.982) and interrater reliability (ICC ranging from 0.794 to 0.837) in the assessment of the sagittal alignment of the spine and pelvis [
15]. A recent study measuring all sagittal radiographic parameters in patients with first-episode mild low back pain to describe normal variation showed small mean variations (<1°), except for in pelvic tilt (PT) (1.2°), C2–T1 alignment (1.2°), and SVA (2.9 cm) [
17]. This result guarantees the reliability of EOS imaging in normal adult patients and raises the possibility of inconsistency in some parameters due to the dynamic nature of body balance [
26]. However, no previous studies have been conducted on patients who require surgical treatment, and clinically, EOS is often part of a preoperative analysis, which necessitates research on patients who underwent surgery. In our study, most sagittal alignment parameters on serial EOS imaging did not show statistically significant interval changes even in patients requiring surgical treatment, which can be interpreted in the same context as the results of a previous study [
17].
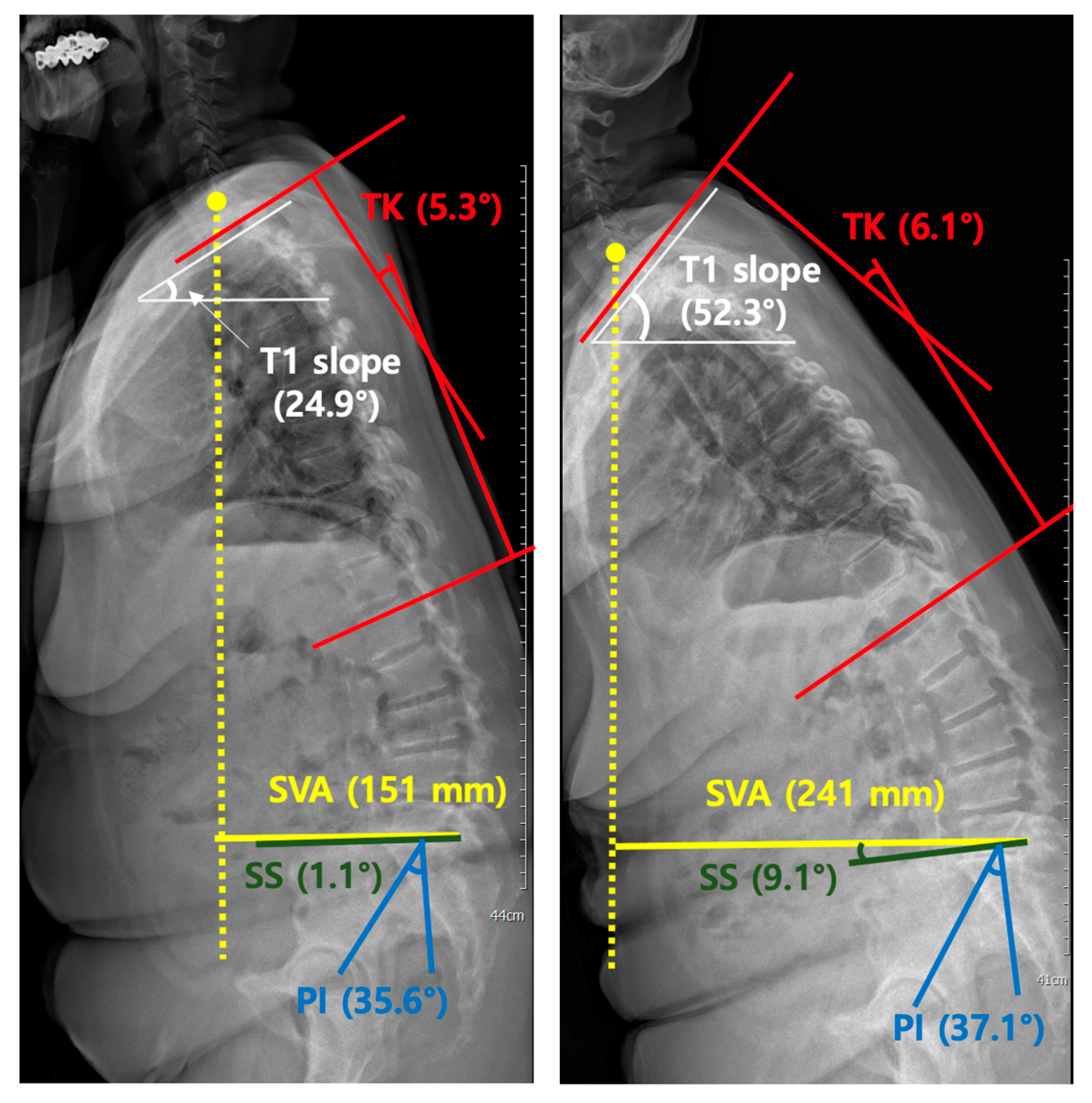
The difference in existing results in our work is that SVA showed statistically significant interval variations (p = 0.023). This variation in SVA was shown in subgroup analyses when the EOS retake interval was >3 months and based on age; borderline significance was shown at an advanced age of 65 years. Interestingly, variations were not apparent in patients with short time intervals or relatively young patients with serial EOS images. In the first group (≤65 years), the mean value of SVA in the second radiograph showed a difference from that of the first (66.6 vs. 96.4), which is thought to have occurred due to large differences in SVA in 3 out of 15 patients. The SVA differences in the three patients were 239.0, 111.9, and 89.9 mm, respectively. In the rest of the patients in group 1, the changes in SVA between the first and second radiographs were not significant, which resulted in no statistically significant differences overall.
SVA has several clinically important significances and must be strictly evaluated before surgery. Generally, sagittal spine alignment is affected by age. There are two points of importance: increasing “positive spinal balance” due to a loss of lumbar lordosis with a more forward sagittal vertical axis [
27] and increasing thoracic kyphosis with advancing age [
28]. In a retrospective study correlating radiographic measurements with clinical symptoms in adult scoliosis, a positive sagittal balance was the most important and significant predictor of clinical symptoms, regardless of previous surgery [
29]. Therefore, the surgeon should plan for a more normal sagittal balance of the spine as an important goal of reconstructive spine surgery. According to a recent study assessing the effect of sagittal spino-pelvic alignment on the clinical symptoms of thoracic, lumbar kyphosis (TLK) in osteoporotic patients, sagittal imbalance (SVA > 5 cm) was more closely related to clinical symptoms than other radiological parameters [
30]. The main purpose of surgery for kyphosis is reducing deformity, pain, and neurological symptoms, and preventing the curve from worsening. Therefore, the sagittal imbalance should be considered in the management of TLK in osteoporotic patients. SVA is the most important parameter not only before surgery, but also after surgery, influencing the clinical outcome of patients surgically treated for degenerative lumbar spondylolisthesis [
31]. Overall postoperative sagittal balance, as defined by SVA, determines the postoperative patient-rated outcome.
The variations in SVA can be attributed to multiple factors, the first of which is that SVA itself has a large interval variation. A previous study [
17] reporting the normal variation in sagittal spinal alignment parameters concluded that SVA has the largest variation in individuals with low pelvic tilt, suggesting a wide range of normality. In our patients, SVA exhibited a wide range and large SDs, which is consistent with these results. In our study, the mean SVA was measured at 67.7 mm, which is significantly higher than that in the normal population. This may be attributed to the difficulty in sagittal balancing due to stooping postures or severe pain in patients requiring surgical treatment, which may have caused statistical differences. According to a study by Steven et al. [
32], in patients with spinal deformity, positive SVA correlates with the severity of symptoms in a linear fashion.
Furthermore, compared to a similar study performed by Hey et al. [
4] in patients with adolescent idiopathic scoliosis (AIS) and a previously mentioned report [
17], our study showed predictable differences in SVA between the first and second EOS recorded serially. The analysis was based on three months’ records because the patient’s regular follow-up period in our institution is usually three months, and the average serial EOS interval in this study is approximately over three months. These results can also be attributed to the wide variations in the SVA or to the increasing degree of pain as the timing of surgery approaches. The borderline significance seen in older patients can be interpreted as reflecting complex and various sagittal balancing in advanced ages. Consequently, these results suggest that the interpretation of SVA results in patients who are about to undergo surgery should be considered; the measurement values may show statistically significant differences, which requires attention to conclude with a single image.
Excluding the differences related to SVA, the T1 slope in patients with X-rays recorded <3 months apart (
p = 0.048) and the C4–T1 in patients underwent multilevel fusion surgery remained the only borderline significant difference. We believe that the difference could be due to the following reason: radiographically, some parameters related to C7 and T1 are difficult to measure because there are overlapping points. Due to overlapping with surrounding chest wall structures, the T1 slope was the most difficult parameter to measure [
15]. In cervical spondylotic myelopathy, cervical sagittal imbalance, as defined by a C2–C7 SVA (the distance from a plumb line drawn at the midpoint at the base of C2 to that drawn at the midpoint of the base of C7) of >40 mm, is associated with worse postoperative clinical outcomes after surgery, resulting in <50% of patients clinically improving after cervical spine surgery [
33]. According to a study performed by Chong et al., T1 slope is the only parameter that demonstrated a significant correlation with both Cobb’s angles of C2–C7 and C2–C7 SVA in symptomatic patients [
34]. In our study, T1 slope and C4–T1 showed borderline differences in variation, but in patients subject to cervical surgery where cervical sagittal balance is essential, it may be necessary to attend to the interpretation of T1 slope measurements, similar to SVA. However, because the subjects of this study were patients who underwent surgery due to symptoms in the thoracolumbar region, additional consideration of the variation of the T1 slope or the lower cervical alignment C4–T1 will be needed in patients who undergo surgery due to degenerative cervical diseases.
The limitations of this study can be grouped into four aspects. First, measurement errors were caused. EOS is photographed with low-dose radiation; therefore, the resolution may be poor, and measurement errors may have occurred depending on the investigator. Secondly, although the patients were requested to assume a proper position during X-ray exposure, it might have been difficult for elderly patients. As such, only patients with no significant posture difference between two serial images were involved in this study. We excluded 14 inappropriate EOS images out of 80 images due to inconsistent posture, causing a not-completely covered whole spine (n = 9), severe artifacts (n = 3), and usage of support devices (n = 2). Especially, in the case of inconsistent posture, most of the patients who underwent deformity correction operations presented with severe stooping. As a result, at least one of the two EOS images did not cover a portion of the cervical spine. This may raise the possibility of a selection bias. Thirdly, selection bias could have occurred because, unlike plain radiography performed as a routine process, the EOS was conducted in selective patients. In our country, where the study was conducted, EOS imaging is not yet covered by medical insurance. Therefore, it is not implemented routinely, and EOS does not reflect the entire cohort. The final limitation of the study pertains to the relatively small sample size. Although there were no statistical errors, this possibly resulted in no significant differences between the first and second images. The small number of patients also entails limitations because they were not classified according to the etiology of the pain. Subsequently, an increase in the number of patients and subgroup analysis is required according to each etiology.





{kind=link}
{kind=link}