Aortic Root Dilatation in Taiwanese Patients with Mucopolysaccharidoses and the Long-Term Effects of Enzyme Replacement Therapy

 ,
,  ,
, 
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Data Analysis and Statistics
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Neufeld, E.F.; Muenzer, J. The Mucopolysaccharidoses. In The Online Metabolic and Molecular Bases of Inherited Disease (OMMBID); Valle, D., Beaudet, A.L., Vogelstein, B., Kinzler, K.W., Antonarakis, S.E., Ballabio, A., Gibson, K., Mitchell, G., Eds.; McGraw-Hill: New York, NY, USA, 2015; Chapter 136. [Google Scholar]
- Lin, S.-P.; Lee, C.-L.; Lo, Y.-T.; Wang, T.-J.; Huang, S.-F.; Chen, T.-L.; Wang, Y.-S.; Niu, D.-M.; Chuang, C.-K.; Lin, S.-P. The relationships between urinary glycosaminoglycan levels and phenotypes of mucopolysaccharidoses. Mol. Genet. Genom. Med. 2018, 6, 982–992. [Google Scholar] [CrossRef]
- Jones, S.A.; on behalf of the HOS Investigators; Almassy, Z.; Beck, M.; Burt, K.B.; Clarke, J.T.; Giugliani, R.; Hendriksz, C.J.; Kroepfl, T.; Lavery, L.L.; et al. Mortality and cause of death in mucopolysaccharidosis type II—A historical review based on data from the Hunter Outcome Survey (HOS). J. Inherit. Metab. Dis. 2009, 32, 534–543. [Google Scholar] [CrossRef]
- Lin, H.-Y.; Lin, S.-P.; Chuang, C.-K.; Chen, M.-R.; Chen, B.-F.; Wraith, J.E. Mucopolysaccharidosis I under enzyme replacement therapy with laronidase—A mortality case with autopsy report. J. Inherit. Metab. Dis. 2005, 28, 1146–1148. [Google Scholar] [CrossRef]
- Lin, H.-Y.; Chuang, C.-K.; Huang, Y.-H.; Tu, R.-Y.; Lin, F.-J.; Lin, S.J.; Chiu, P.C.; Niu, D.-M.; Tsai, F.-J.; Hwu, W.-L.; et al. Causes of death and clinical characteristics of 34 patients with Mucopolysaccharidosis II in Taiwan from 1995-2012. Orphanet J. Rare Dis. 2016, 11, 85. [Google Scholar] [CrossRef]
- Lin, S.-P.; Chuang, C.-K.; Lee, C.-L.; Tu, R.; Lo, Y.; Chiu, P.C.; Niu, D.; Fang, Y.; Chen, T.; Tsai, F.; et al. Mucopolysaccharidosis III in Taiwan: Natural history, clinical and molecular characteristics of 28 patients diagnosed during a 21-year period. Am. J. Med. Genet. Part A 2018, 176, 1799–1809. [Google Scholar] [CrossRef]
- Lin, S.-P.; Chuang, C.-K.; Chen, M.-R.; Chiu, P.C.; Ke, Y.-Y.; Niu, D.-M.; Tsai, F.-J.; Hwu, W.-L.; Lin, J.-L.; Lin, S.-P. Natural history and clinical assessment of Taiwanese patients with mucopolysaccharidosis IVA. Orphanet J. Rare Dis. 2014, 9, 21. [Google Scholar] [CrossRef]
- Braunlin, E.; Harmatz, P.R.; Scarpa, M.; Furlanetto, B.; Kampmann, C.; Loehr, J.P.; Ponder, K.P.; Roberts, W.C.; Rosenfeld, H.M.; Giugliani, R. Cardiac disease in patients with mucopolysaccharidosis: Presentation, diagnosis and management. J. Inherit. Metab. Dis. 2011, 34, 1183–1197. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.Y.; Rudser, K.D.; Dengel, D.R.; Evanoff, N.; Steinberger, J.; Movsesyan, N.; Garrett, R.; Christensen, K.; Boylan, D.; Braddock, S.R.; et al. Abnormally increased carotid intima media-thickness and elasticity in patients with Morquio A disease. Orphanet J. Rare Dis. 2020, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-M.; Lin, S.-P.; Chuang, C.-K.; Lin, S.-P.; Chen, M.-R. Cardiovascular abnormalities in Taiwanese patients with mucopolysaccharidosis. Mol. Genet. Metab. 2014, 111, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Lavery, C.; Hendriksz, C. Mortality in Patients with Morquio Syndrome A. JIMD Rep. 2015, 15, 59–66. [Google Scholar] [CrossRef]
- Schroeder, L.; Orchard, P.; Whitley, C.B.; Berry, J.M.; Tolar, J.; Miller, W.; Braunlin, E. Cardiac Ultrasound Findings in Infants with Severe (Hurler Phenotype) Untreated Mucopolysaccharidosis (MPS) Type I. JIMD Rep. 2013, 10, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Kampmann, C.; Abu-Tair, T.; Gökce, S.; Lampe, C.; Reinke, J.; Mengel, E.; Hennermann, J.B.; Wiethoff, C.M. Heart and Cardiovascular Involvement in Patients with Mucopolysaccharidosis Type IVA (Morquio-A Syndrome). PLoS ONE 2016, 11, e0162612. [Google Scholar] [CrossRef] [PubMed]
- Bolourchi, M.; Renella, P.; Wang, R.Y. Aortic Root Dilatation in Mucopolysaccharidosis I–VII. Int. J. Mol. Sci. 2016, 17, 2004. [Google Scholar] [CrossRef] [PubMed]
- Poswar, F.D.O.; De Souza, C.F.M.; Giugliani, R.; Baldo, G. Aortic root dilatation in patients with mucopolysaccharidoses and the impact of enzyme replacement therapy. Heart Vessels 2019, 34, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-Y.; Chen, M.-R.; Lin, S.-M.; Hung, C.-L.; Niu, D.-M.; Chuang, C.-K.; Lin, S.-P. Cardiac features and effects of enzyme replacement therapy in Taiwanese patients with Mucopolysaccharidosis IVA. Orphanet J. Rare Dis. 2018, 13, 148. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-Y.; Chen, M.-R.; Lin, S.-M.; Hung, C.-L.; Niu, D.-M.; Chang, T.-M.; Chuang, C.-K.; Lin, S.-P. Cardiac characteristics and natural progression in Taiwanese patients with mucopolysaccharidosis III. Orphanet J. Rare Dis. 2019, 14, 140. [Google Scholar] [CrossRef]
- Lin, S.-P.; Chuang, C.-K.; Lee, C.-L.; Chen, M.-R.; Sung, K.-T.; Lin, S.-M.; Hou, C.J.-Y.; Niu, D.-M.; Chang, T.-M.; Hung, C.-L.; et al. Cardiac Evaluation Using Two-Dimensional Speckle-Tracking Echocardiography and Conventional Echocardiography in Taiwanese Patients with Mucopolysaccharidoses. Diagnostics 2020, 10, 62. [Google Scholar] [CrossRef]
- Sawamoto, K.; Stapleton, M.; Alméciga-Díaz, C.J.; Espejo-Mojica, A.J.; Losada, J.C.; Suarez, D.A.; Tomatsu, S. Therapeutic Options for Mucopolysaccharidoses: Current and Emerging Treatments. Drugs 2019, 79, 1103–1134. [Google Scholar] [CrossRef]
- Metcalf, J.A.; Linders, B.; Wu, S.; Bigg, P.; O’Donnell, P.; Sleeper, M.M.; Whyte, M.P.; Haskins, M.; Ponder, K.P. Upregulation of elastase activity in aorta in mucopolysaccharidosis I and VII dogs may be due to increased cytokine expression. Mol. Genet. Metab. 2010, 99, 396–407. [Google Scholar] [CrossRef]
- Baldo, G.; Wu, S.; Howe, R.A.; Ramamoothy, M.; Knutsen, R.H.; Fang, J.; Mecham, R.P.; Liu, Y.; Wu, X.; Atkinson, J.P.; et al. Pathogenesis of aortic dilatation in mucopolysaccharidosis VII mice may involve complement activation. Mol. Genet. Metab. 2011, 104, 608–619. [Google Scholar] [CrossRef]
- Chuang, C.-K.; Lin, S.-P.; Wang, T.-J.; Tsai, C.-C.; Liu, H.-L.; Lin, S.-P. A modified liquid chromatography/tandem mass spectrometry method for predominant disaccharide units of urinary glycosaminoglycans in patients with mucopolysaccharidoses. Orphanet J. Rare Dis. 2014, 9, 135. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Colan, S.D.; McElhinney, D.B.; Crawford, E.C.; Keane, J.F.; Lock, J.E. Validation and re-evaluation of a discriminant model predicting anatomic suitability for biventricular repair in neonates with aortic stenosis. J. Am. Coll. Cardiol. 2006, 47, 1858–1865. [Google Scholar] [CrossRef] [PubMed]
- Dallaire, F.; Bigras, J.-L.; Prsa, M.; Dahdah, N. Bias Related to Body Mass Index in Pediatric Echocardiographic Z Scores. Pediatr. Cardiol. 2015, 36, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Haycock, G.B.; Schwartz, G.J.; Wisotsky, D.H. Geometric method for measuring body surface area: A height–weight formula validated in infants, children, and adults. J. Pediatr. 1978, 93, 62–66. [Google Scholar] [CrossRef]
- Collins, J.A.; Munoz, J.-V.; Patel, T.R.; Loukas, M.; Tubbs, R.S. The anatomy of the aging aorta. Clin. Anat. 2014, 27, 463–466. [Google Scholar] [CrossRef]
- Ma, X.; Tittiger, M.; Knutsen, R.H.; Kovacs, A.; Schaller, L.; Mecham, R.P.; Ponder, K.P. Upregulation of elastase proteins results in aortic dilatation in mucopolysaccharidosis I mice. Mol. Genet. Metab. 2008, 94, 298–304. [Google Scholar] [CrossRef]
- Nemes, A.; Timmermans, R.G.M.; Wilson, J.H.P.; Soliman, O.; Krenning, B.J.; Cate, F.J.T.; Geleijnse, M.L. The mild form of mucopolysaccharidosis type I (Scheie syndrome) is associated with increased ascending aortic stiffness. Heart Vessels 2008, 23, 108–111. [Google Scholar] [CrossRef]
- Hinek, A.; Wilson, S.E. Impaired elastogenesis in Hurler disease: Dermatan sulfate accumulation linked to deficiency in elastin-binding protein and elastic fiber assembly. Am. J. Pathol. 2000, 156, 925–938. [Google Scholar] [CrossRef]
- Lin, S.-P.; Chuang, C.-K.; Chen, M.-R.; Lin, S.-J.; Chiu, P.C.; Niu, D.-M.; Tsai, F.-J.; Hwu, W.-L.; Chien, Y.-H.; Lin, J.-L.; et al. Clinical characteristics and surgical history of Taiwanese patients with mucopolysaccharidosis type II: Data from the hunter outcome survey (HOS). Orphanet J. Rare Dis. 2018, 13, 89. [Google Scholar] [CrossRef]
- Carlson, M.; Silberbach, M. Dissection of the aorta in Turner syndrome: Two cases and review of 85 cases in the literature. BMJ Case Rep. 2009, 2009, bcr0620091998. [Google Scholar] [CrossRef]
- Jain, D.; Dietz, H.C.; Oswald, G.L.; Maleszewski, J.J.; Halushka, M.K. Causes and histopathology of ascending aortic disease in children and young adults. Cardiovasc. Pathol. 2011, 20, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, J.D. Possible mechanical roles of glycosaminoglycans in thoracic aortic dissection and associations with dysregulated transforming growth factor-β. J. Vasc. Res. 2013, 50, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Weinsaft, J.W.; Devereux, R.B.; Preiss, L.R.; Feher, A.; Roman, M.J.; Basson, C.T.; Geevarghese, A.; Ravekes, W.; Dietz, H.C.; Holmes, K.; et al. Aortic Dissection in Patients with Genetically Mediated Aneurysms: Incidence and Predictors in the GenTAC Registry. J. Am. Coll. Cardiol. 2016, 67, 2744–2754. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, E.A.; Tavares, A.M.V.; Poletto, E.; Giugliani, R.; Matte, U.; Baldo, G. Losartan improves aortic dilatation and cardiovascular disease in mucopolysaccharidosis I. J. Inherit. Metab. Dis. 2017, 40, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Osborn, M.J.; Webber, B.R.; McElmurry, R.T.; Rudser, K.D.; Defeo, A.P.; Muradian, M.; Petryk, A.; Hallgrimsson, B.; Blazar, B.R.; Tolar, J.; et al. Angiotensin receptor blockade mediated amelioration of mucopolysaccharidosis type I cardiac and craniofacial pathology. J. Inherit. Metab. Dis. 2017, 40, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-P.; Lee, C.-L.; Lo, Y.-T.; Tu, R.-Y.; Chang, C.-Y.; Chiu, P.C.; Tsai, W.-H.; Niu, D.-M.; Chuang, C.-K. An At-Risk Population Screening Program for Mucopolysaccharidoses by Measuring Urinary Glycosaminoglycans in Taiwan. Diagnostics 2019, 9, 140. [Google Scholar] [CrossRef]
- Chuang, C.-K.; Lin, S.-P.; Wang, T.-J.; Huang, Y.-H.; Chan, M.-J.; Liao, H.-C.; Lo, Y.-T.; Wang, L.-Y.; Tu, R.-Y.; Fang, Y.-Y.; et al. Status of newborn screening and follow up investigations for Mucopolysaccharidoses I and II in Taiwan. Orphanet J. Rare Dis. 2018, 13, 1–14. [Google Scholar] [CrossRef]
- Chan, M.-J.; Liao, H.-C.; Gelb, M.H.; Chuang, C.-K.; Liu, M.-Y.; Chen, H.-J.; Kao, S.-M.; Lin, S.-P.; Huang, Y.-H.; Kumar, A.B.; et al. Taiwan National Newborn Screening Program by Tandem Mass Spectrometry for Mucopolysaccharidoses Types I, II, and VI. J. Pediatr. 2019, 205, 176–182. [Google Scholar] [CrossRef]
- Chien, Y.-H.; Lee, N.-C.; Chen, P.-W.; Yeh, H.-Y.; Gelb, M.H.; Chiu, P.-C.; Chu, S.-Y.; Lee, C.-H.; Lee, A.-R.; Hwu, W.-L. Newborn screening for Morquio disease and other lysosomal storage diseases: Results from the 8-plex assay for 70,000 newborns. Orphanet J. Rare Dis. 2020, 15, 38. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MPS I | MPS II | MPS III | MPS IV | MPS VI | All | |
|---|---|---|---|---|---|---|
| n | 11 | 49 | 25 | 29 | 11 | 125 |
| Gender (M/F) | 5/6 | 49/0 | 13/12 | 13/16 | 5/6 | 85/40 |
| Age (years) | 7.0 (8.1) | 7.2 (5.0) | 8.1 (4.4) | 9.8 (5.1) | 8.9 (5.0) | 8.1 (5.3) |
| Age range (years) | 0.1–18.9 | 0.1–19.1 | 1.8–18.5 | 1.1–18.4 | 2.2–17.1 | 0.1–19.1 |
| Height z score | −2.59 (3.96) | −1.81 (2.77) | −0.73 (1.75) | −6.16 (3.43) | −5.13 (3.15) | −2.96 (3.56) |
| Weight z score | −0.92 (1.14) | 0.04 (1.94) | −0.13 (1.51) | −2.09 (1.13) | −1.78 (1.10) | −0.73 (1.80) |
| BSA (m2) | 0.65 (0.41) | 0.78 (0.25) | 0.92 (0.24) | 0.69 (0.20) | 0.69 (0.10) | 0.77 (0.26) |
| AoD (cm) | 1.67 (0.39) | 2.10 (0.47) | 2.19 (0.44) | 2.11 (0.31) | 1.99 (0.16) | 2.07 (0.42) |
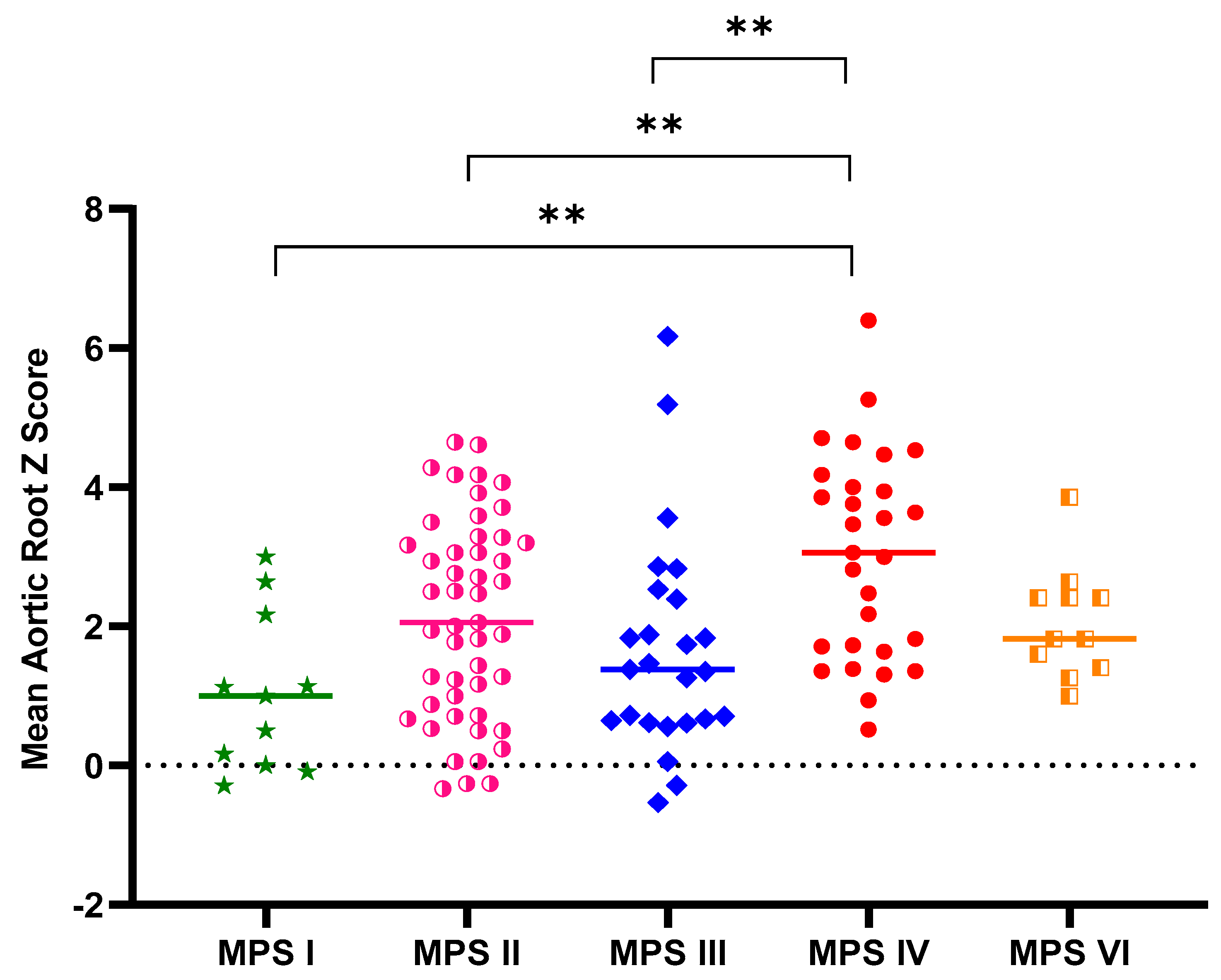
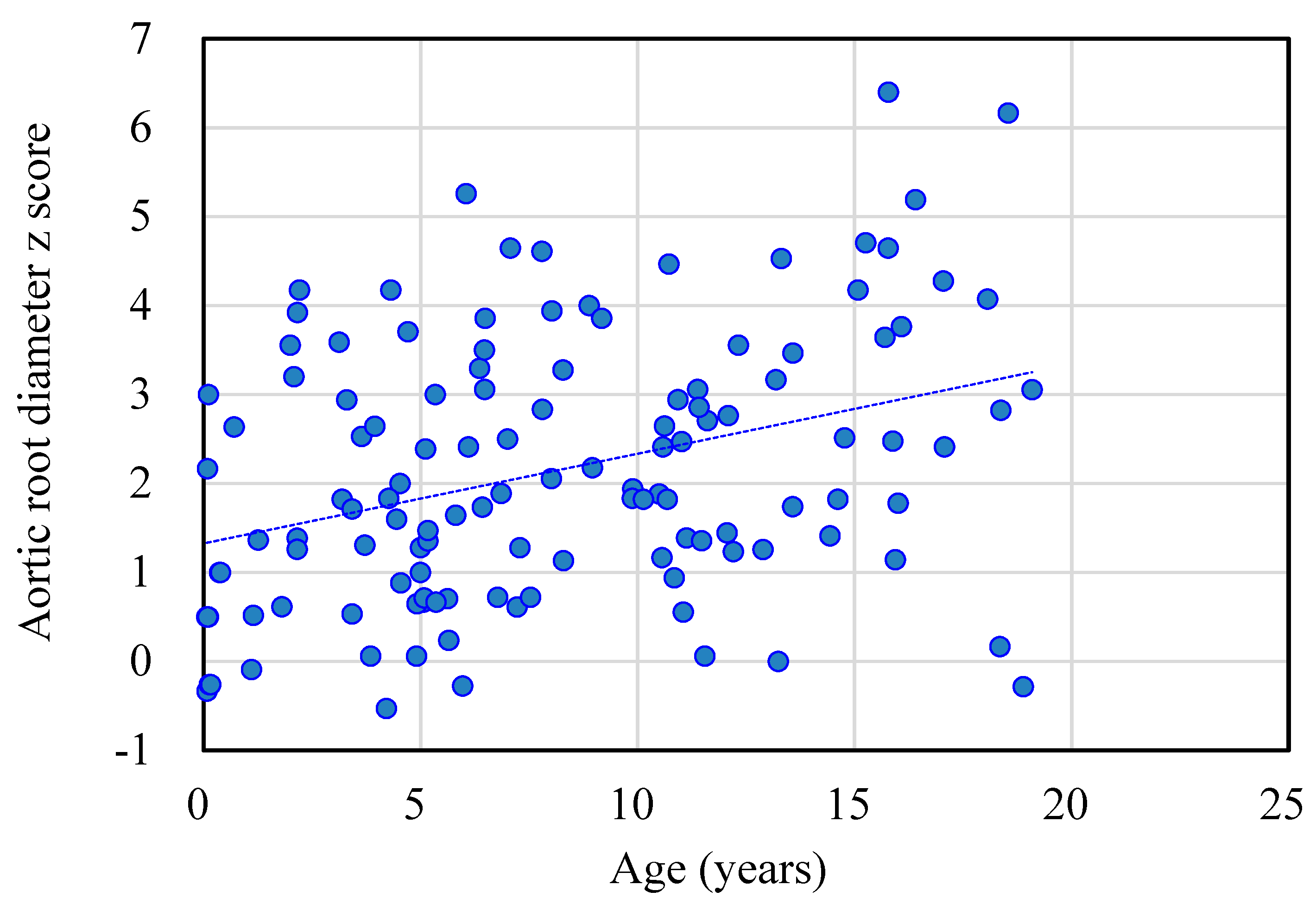
| AoD z score | 1.03 (1.13) | 2.12 (1.43) | 1.68 (1.57) | 3.03 (1.48) | 2.06 (0.80) | 2.14 (1.50) |
| AoD z score > 2, n (%) | 3 (27%) | 25 (51%) | 7 (28%) | 19 (66%) | 5 (45%) | 59 (47%) |
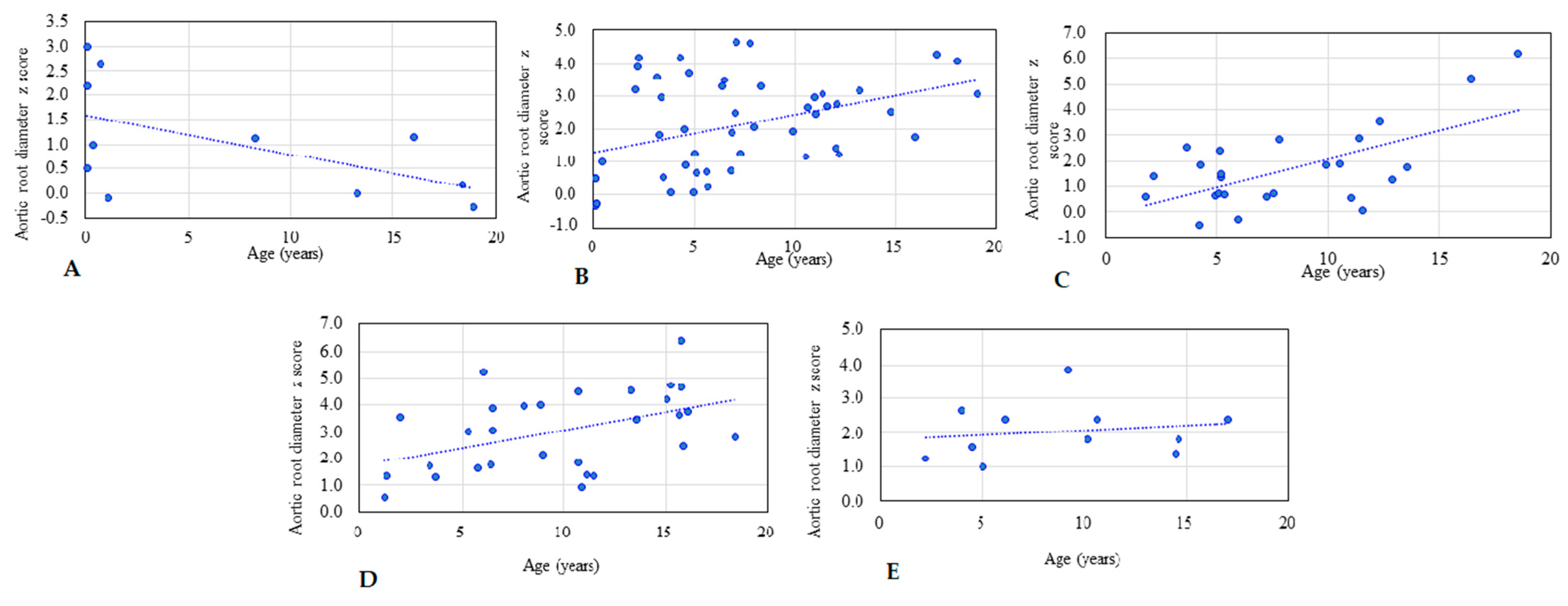
| r value (AoD z score versus age) | −0.566 | 0.394 | 0.624 | 0.457 | 0.161 | 0.353 |
| p-value | p < 0.05 | p < 0.01 | p < 0.01 | p < 0.01 | p > 0.05 | p < 0.01 |
| Covariate | MPS II (Mild) | MPS II (Severe) |
|---|---|---|
| n | 22 | 27 |
| Gender (M/F) | 22/0 | 27/0 |
| Age (years) | 7.7 (5.9) | 6.7 (4.2) |
| Age range (years) | 0.1–19.1 | 0.1–13.2 |
| Height z score | −2.03 (3.23) | −1.63 (2.38) |
| Weight z score | 0.06 (1.62) | 0.03 (2.19) |
| BSA (m2) | 0.82 (0.29) | 0.75 (0.21) |
| AoD (cm) | 2.10 (0.54) | 2.10 (0.42) |
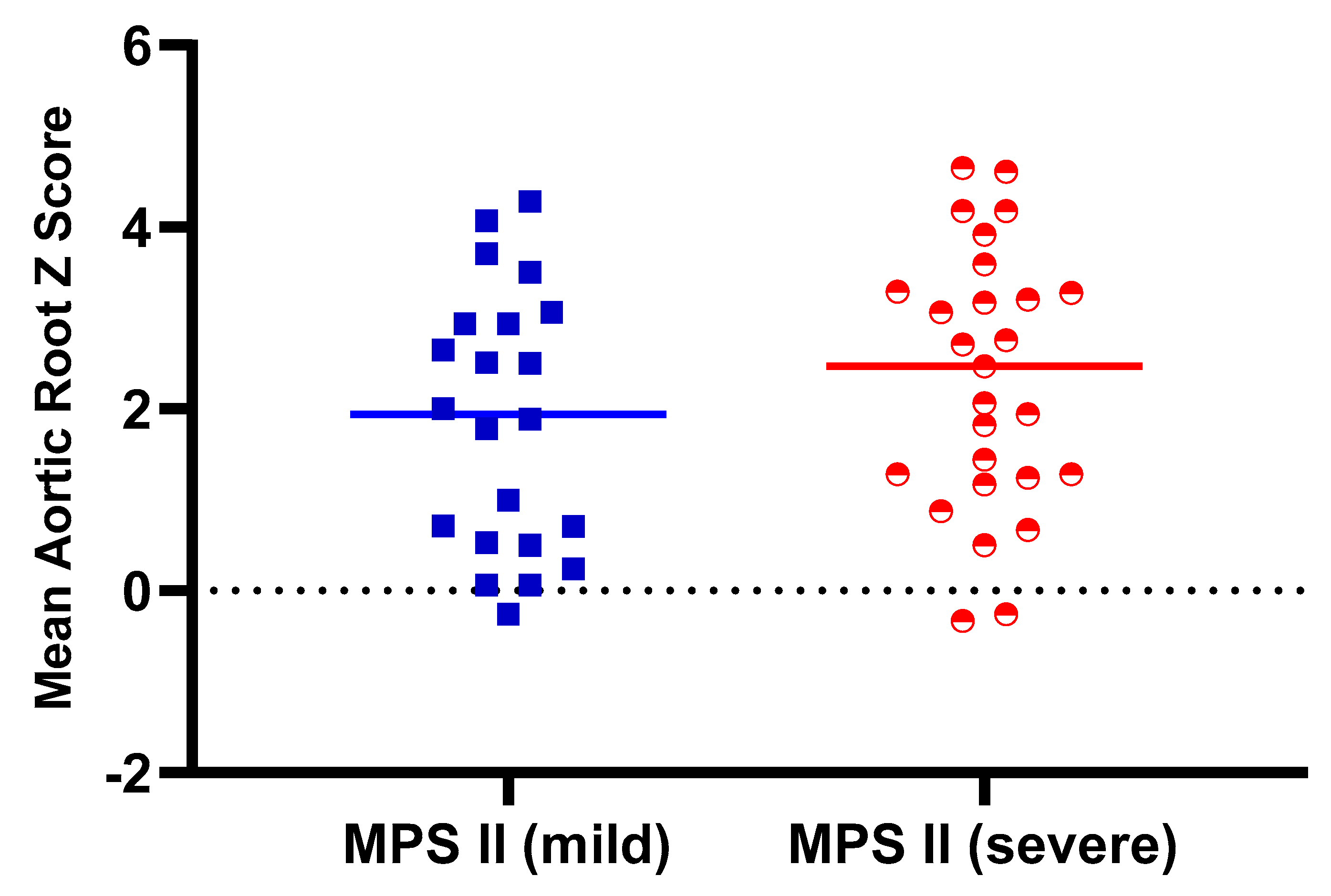
| AoD z score | 1.88 (1.43) | 2.32 (1.44) |
| AoD z score > 2, n (%) | 10 (45%) | 15 (56%) |
| r value (AoD z score versus age) | 0.642 | 0.180 |
| p-value | p < 0.01 | p > 0.05 |
| No. | MPS Type | Gender | Age at Baseline (Years) | Age at Follow-Up (Years) | ERT Duration (Years) | AoD (cm) | AoD (z Score) | Change (z Score) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | |||||||
| 1 | I (H/S) | F | 0.7 | 7.7 | 7.0 | 1.70 | 1.90 | 2.60 | 0.60 | −2.00 |
| 2 | I (H/S) | F | 1.1 | 6.9 | 5.8 | 1.40 | 2.00 | −0.10 | 1.20 | 1.30 |
| 3 | I (H/S) | M | 18.2 | 20.2 | 2.0 | 1.63 | 1.88 | −2.00 | −0.61 | 1.39 |
| 4 | II (M) | M | 13.2 | 25.7 | 12.4 | 2.28 | 2.50 | 1.12 | 0.52 | −0.60 |
| 5 | II (M) | M | 14.8 | 23.3 | 8.5 | 2.54 | 3.10 | 2.51 | 2.74 | 0.23 |
| 6 | II (M) | M | 15.4 | 17.7 | 2.2 | 2.85 | 2.14 | 4.47 | 0.29 | −4.18 |
| 7 | II (M) | M | 17.5 | 29.8 | 12.3 | 2.80 | 2.90 | 3.00 | 2.00 | −1.00 |
| 8 | II (M) | M | 18.1 | 26.6 | 8.6 | 3.46 | 3.70 | 4.07 | 4.06 | −0.01 |
| 9 | IVA | M | 1.1 | 7.4 | 6.3 | 1.56 | 2.40 | 0.52 | 4.18 | 3.66 |
| 10 | IVA | M | 2.3 | 6.6 | 4.3 | 1.64 | 1.80 | 0.92 | 1.20 | 0.28 |
| 11 | IVA | M | 7.2 | 10.5 | 3.3 | 2.08 | 2.30 | 2.29 | 2.39 | 0.10 |
| 12 | IVA | F | 14.8 | 19.0 | 4.2 | 2.42 | 2.40 | 4.29 | 3.59 | −0.70 |
| 13 | IVA | F | 16.8 | 23.2 | 6.4 | 2.80 | 2.60 | 5.94 | 3.39 | −2.55 |
| 14 | VI | M | 7.6 | 21.6 | 14.0 | 2.06 | 2.20 | 3.57 | 1.83 | −1.74 |
| 15 | VI | M | 8.3 | 22.4 | 14.1 | 2.38 | 2.80 | 5.07 | 4.18 | −0.89 |
| 16 | VI | M | 11.7 | 27.9 | 16.2 | 2.67 | 2.70 | 4.44 | 3.94 | −0.50 |
| Mean | 10.6 | 18.5 | 8.0 | 2.27 | 2.46 | 2.67 | 2.22 | −0.45 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-Y.; Chen, M.-R.; Lee, C.-L.; Lin, S.-M.; Hung, C.-L.; Niu, D.-M.; Chang, T.-M.; Chuang, C.-K.; Lin, S.-P. Aortic Root Dilatation in Taiwanese Patients with Mucopolysaccharidoses and the Long-Term Effects of Enzyme Replacement Therapy. Diagnostics 2021, 11, 16. https://doi.org/10.3390/diagnostics11010016
Lin H-Y, Chen M-R, Lee C-L, Lin S-M, Hung C-L, Niu D-M, Chang T-M, Chuang C-K, Lin S-P. Aortic Root Dilatation in Taiwanese Patients with Mucopolysaccharidoses and the Long-Term Effects of Enzyme Replacement Therapy. Diagnostics. 2021; 11(1):16. https://doi.org/10.3390/diagnostics11010016
Chicago/Turabian StyleLin, Hsiang-Yu, Ming-Ren Chen, Chung-Lin Lee, Shan-Miao Lin, Chung-Lieh Hung, Dau-Ming Niu, Tung-Ming Chang, Chih-Kuang Chuang, and Shuan-Pei Lin. 2021. "Aortic Root Dilatation in Taiwanese Patients with Mucopolysaccharidoses and the Long-Term Effects of Enzyme Replacement Therapy" Diagnostics 11, no. 1: 16. https://doi.org/10.3390/diagnostics11010016
APA StyleLin, H.-Y., Chen, M.-R., Lee, C.-L., Lin, S.-M., Hung, C.-L., Niu, D.-M., Chang, T.-M., Chuang, C.-K., & Lin, S.-P. (2021). Aortic Root Dilatation in Taiwanese Patients with Mucopolysaccharidoses and the Long-Term Effects of Enzyme Replacement Therapy. Diagnostics, 11(1), 16. https://doi.org/10.3390/diagnostics11010016