Predictive Biomarkers and Patient Outcome in Platinum-Resistant (PLD-Treated) Ovarian Cancer

 , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Tissue Samples
2.3. Evaluation of the Immunohistochemical Expression of E-cadherin, Vimentin, and Osteopontin
2.4. Survival Endpoints
2.5. Clinical and Radiological Assessments
2.6. Statistical Analysis
3. Results
3.1. Patient Sample Features
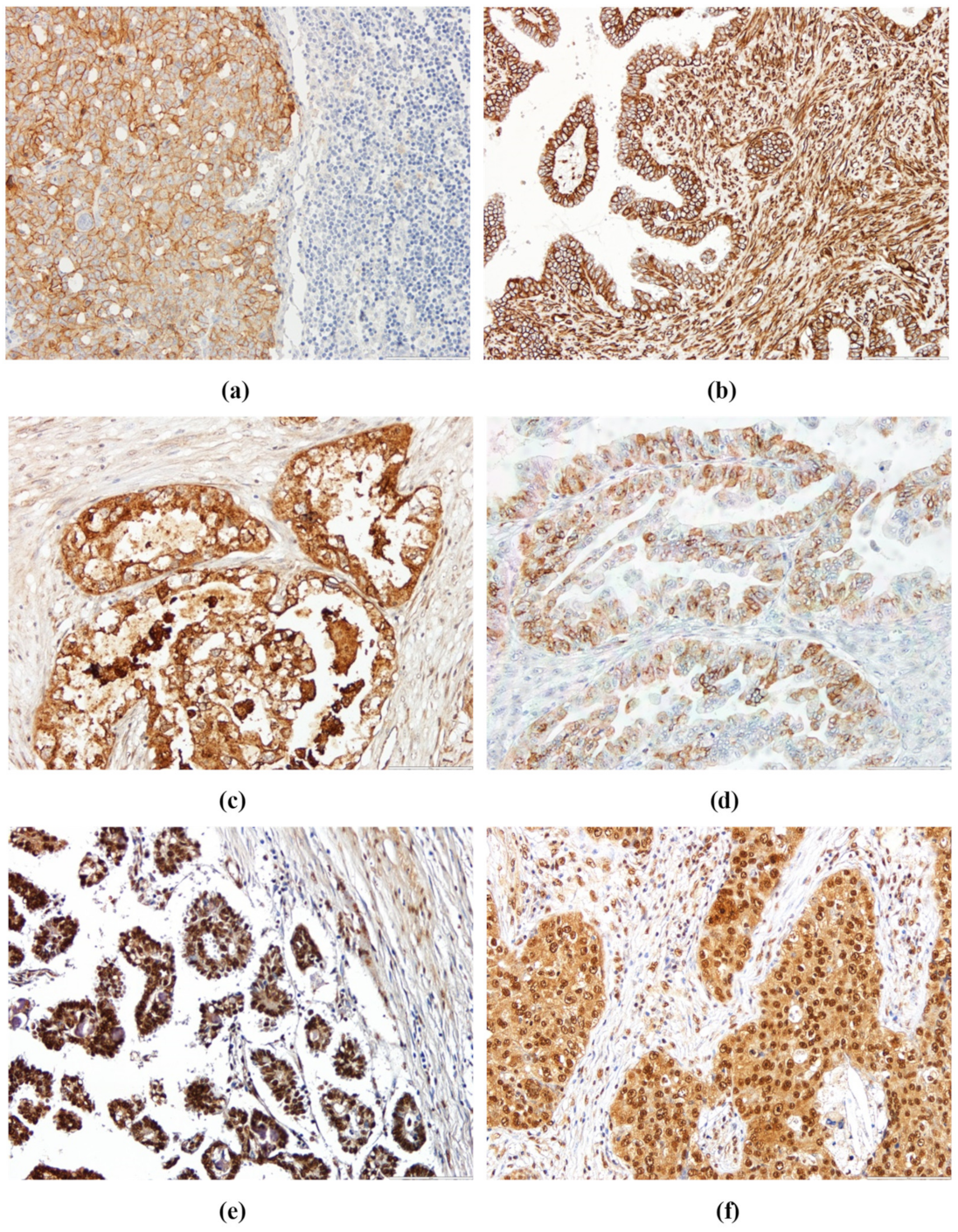
3.2. Immunohistochemistry Analysis
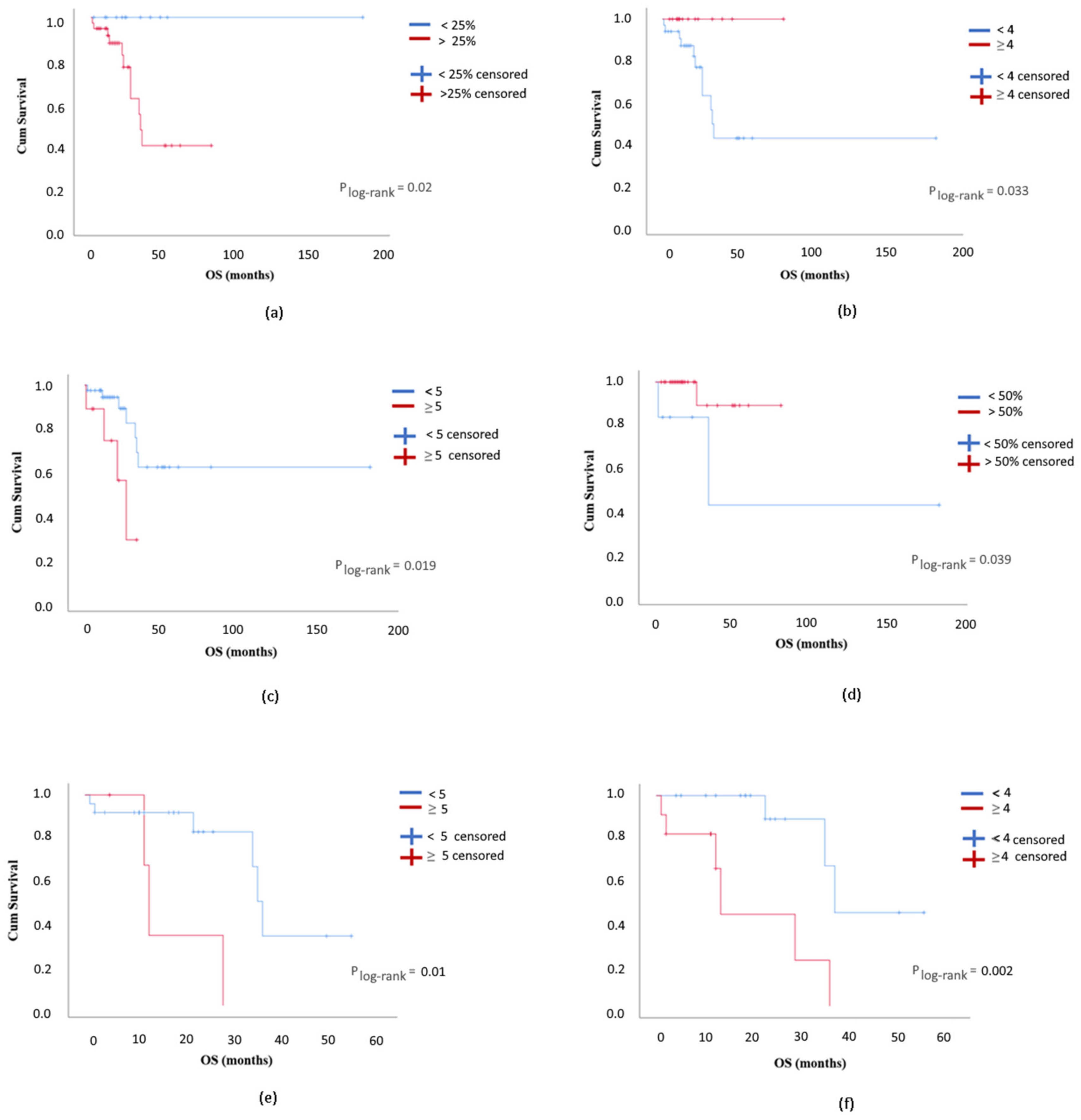
3.3. E-cadherin, Vimentin, OPN, and OPN-c Staining Patterns in OC Cases and Survival Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Armstrong, D.K.; Alvarez, R.D.; Bakkum-Gamez, J.N.; Barroilhet, L.; Behbakht, K.; Berchuck, A.; Berek, J.S.; Chen, L.M.; Cristea, M.; DeRosa, M.; et al. Nccn guidelines insights: Ovarian cancer, version 1.2019. J. Natl. Compr. Canc. Netw. 2019, 17, 896–909. [Google Scholar] [CrossRef]
- Colombo, N.; Sessa, C.; Du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. Esmo-esgo consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent diseasedagger. Ann. Oncol. 2019, 30, 672–705. [Google Scholar] [CrossRef] [PubMed]
- Duska, L.R.; Kohn, E.C. The new classifications of ovarian, fallopian tube, and primary peritoneal cancer and their clinical implications. Ann. Oncol. 2017, 28, viii8–viii12. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Kehoe, S.T.; Kumar, L.; Friedlander, M. Cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynaecol. Obs. 2018, 143 (Suppl. 2), 59–78. [Google Scholar] [CrossRef]
- Sjoquist, K.M.; Friedlander, M.L.; O’Connell, R.L.; Voysey, M.; King, M.T.; Stockler, M.R.; Oza, A.M.; Gillies, K.; Martyn, J.K.; Butow, P.N. Hope, quality of life, and benefit from treatment in women having chemotherapy for platinum-resistant/refractory recurrent ovarian cancer: The gynecologic cancer intergroup symptom benefit study. Oncologist 2013, 18, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Staropoli, N.; Ciliberto, D.; Botta, C.; Fiorillo, L.; Gualtieri, S.; Salvino, A.; Tassone, P.; Tagliaferri, P. A retrospective analysis of pegylated liposomal doxorubicin in ovarian cancer: Do we still need it? J. Ovarian Res. 2013, 6, 10. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Kristeleit, R.S. Optimal treatment for relapsing ovarian cancer. Ann. Oncol. 2010, 21 (Suppl. 7), vii218–vii222. [Google Scholar] [CrossRef]
- Fung-Kee-Fung, M.; Oliver, T.; Elit, L.; Oza, A.; Hirte, H.W.; Bryson, P. Optimal chemotherapy treatment for women with recurrent ovarian cancer. Curr. Oncol. 2007, 14, 195–208. [Google Scholar] [CrossRef]
- Curtis, M.; Mukherjee, A.; Lengyel, E. The tumor microenvironment takes center stage in ovarian cancer metastasis. Trends Cancer 2018, 4, 517–519. [Google Scholar] [CrossRef]
- Rosso, M.; Majem, B.; Devis, L.; Lapyckyj, L.; Besso, M.J.; Llaurado, M.; Abascal, M.F.; Matos, M.L.; Lanau, L.; Castellvi, J.; et al. E-cadherin: A determinant molecule associated with ovarian cancer progression, dissemination and aggressiveness. PLoS ONE 2017, 12, e0184439. [Google Scholar] [CrossRef]
- Angst, B.D.; Marcozzi, C.; Magee, A.I. The cadherin superfamily: Diversity in form and function. J. Cell Sci 2001, 114, 629–641. [Google Scholar] [PubMed]
- Van Roy, F.; Berx, G. The cell-cell adhesion molecule e-cadherin. Cell Mol. Life Sci 2008, 65, 3756–3788. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.S. The morphogenetic role of cadherin cell adhesion molecules in human cancer: A thematic review. Cancer Investig. 1998, 16, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Hirohashi, S. Inactivation of the e-cadherin-mediated cell adhesion system in human cancers. Am. J. Pathol. 1998, 153, 333–339. [Google Scholar] [CrossRef]
- Bacic, B.; Haller, H.; Mrklic, I.; Kosta, V.; Caric, A.; Tomic, S. Prognostic role of e-cadherin in patients with advanced serous ovarian cancer. Arch. Gynecol. Obs. 2013, 287, 1219–1224. [Google Scholar] [CrossRef]
- Huo, Y.; Zheng, Z.; Chen, Y.; Wang, Q.; Zhang, Z.; Deng, H. Downregulation of vimentin expression increased drug resistance in ovarian cancer cells. Oncotarget 2016, 7, 45876–45888. [Google Scholar] [CrossRef]
- Thiery, J.P. Epithelial-mesenchymal transitions in tumour progression. Nat. Rev. Cancer 2002, 2, 442–454. [Google Scholar] [CrossRef]
- Ko, S.H.; Suh, S.H.; Kim, B.J.; Ahn, Y.B.; Song, K.H.; Yoo, S.J.; Son, H.S.; Cha, B.Y.; Lee, K.W.; Son, H.Y.; et al. Expression of the intermediate filament vimentin in proliferating duct cells as a marker of pancreatic precursor cells. Pancreas 2004, 28, 121–128. [Google Scholar] [CrossRef]
- Mahrle, G.; Bolling, R.; Osborn, M.; Weber, K. Intermediate filaments of the vimentin and prekeratin type in human epidermis. J. Investig. Derm. 1983, 81, 46–48. [Google Scholar] [CrossRef]
- Evans, R.M. Vimentin: The conundrum of the intermediate filament gene family. Bioessays 1998, 20, 79–86. [Google Scholar] [CrossRef]
- Cochard, P.; Paulin, D. Initial expression of neurofilaments and vimentin in the central and peripheral nervous system of the mouse embryo in vivo. J. Neurosci. 1984, 4, 2080–2094. [Google Scholar] [CrossRef] [PubMed]
- Kanakkanthara, A.; Rawson, P.; Northcote, P.T.; Miller, J.H. Acquired resistance to peloruside a and laulimalide is associated with downregulation of vimentin in human ovarian carcinoma cells. Pharm. Res. 2012, 29, 3022–3032. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Behera, R.; Chakraborty, G.; Jain, S.; Kumar, V.; Sharma, P.; Bulbule, A.; Kale, S.; Kumar, S.; Mishra, R.; et al. Osteopontin: A potentially important therapeutic target in cancer. Expert Opin. Targets 2011, 15, 1113–1126. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.D.; Liu, X.F.; Liu, X.C.; Ding, C.M.; Hu, C.J. Diagnostic accuracy of osteopontin for malignant pleural mesothelioma: A systematic review and meta-analysis. Clin. Chim. Acta 2014, 433, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Wang, W.; Sun, C.; Li, M.; Wang, B.; Lv, Y. Meta-analysis of the prognostic and diagnostic significance of serum/plasma osteopontin in hepatocellular carcinoma. J. Clin. Gastroenterol. 2014, 48, 806–814. [Google Scholar] [CrossRef]
- Bramwell, V.H.; Doig, G.S.; Tuck, A.B.; Wilson, S.M.; Tonkin, K.S.; Tomiak, A.; Perera, F.; Vandenberg, T.A.; Chambers, A.F. Serial plasma osteopontin levels have prognostic value in metastatic breast cancer. Clin. Cancer Res. 2006, 12, 3337–3343. [Google Scholar] [CrossRef]
- Gimba, E.R.; Tilli, T.M. Human osteopontin splicing isoforms: Known roles, potential clinical applications and activated signaling pathways. Cancer Lett. 2013, 331, 11–17. [Google Scholar] [CrossRef]
- Marques, D.S.; Grativol, J.; Alves da Silva Peres, R.; da Rocha Matos, A.; Gimba, E.R.P. Osteopontin-c isoform levels are associated with sr and hnrnp differential expression in ovarian cancer cell lines. Tumour Biol. 2017, 39, 1010428317725442. [Google Scholar] [CrossRef]
- Wang, Y.D.; Chen, H.; Liu, H.Q.; Hao, M. Correlation between ovarian neoplasm and serum levels of osteopontin: A meta-analysis. Tumour Biol. 2014, 35, 11799–11808. [Google Scholar] [CrossRef]
- Weber, G.F.; Lett, G.S.; Haubein, N.C. Categorical meta-analysis of osteopontin as a clinical cancer marker. Oncol. Rep. 2011, 25, 433–441. [Google Scholar] [CrossRef]
- Moszynski, R.; Szubert, S.; Szpurek, D.; Michalak, S.; Sajdak, S. Role of osteopontin in differential diagnosis of ovarian tumors. J. Obs. Gynaecol Res. 2013, 39, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.D.; Wei, T.T.; Yang, M.; Ma, N.; Tang, Q.Q.; Qin, B.D.; Fu, H.T.; Zhong, R.Q. Diagnostic value of osteopontin in ovarian cancer: A meta-analysis and systematic review. PLoS ONE 2015, 10, e0126444. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Skates, S.J.; Uede, T.; Wong, K.K.; Schorge, J.O.; Feltmate, C.M.; Berkowitz, R.S.; Cramer, D.W.; Mok, S.C. Osteopontin as a potential diagnostic biomarker for ovarian cancer. JAMA 2002, 287, 1671–1679. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Samant, R.S.; Shevde, L.A. Nonclassical activation of hedgehog signaling enhances multidrug resistance and makes cancer cells refractory to smoothened-targeting hedgehog inhibition. J. Biol. Chem. 2013, 288, 11824–11833. [Google Scholar] [CrossRef] [PubMed]
- Shevde, L.A.; Samant, R.S. Role of osteopontin in the pathophysiology of cancer. Matrix Biol. 2014, 37, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.B.; Tavares, C.; Pestana, A.; Pereira, C.L.; Eloy, C.; Pinto, M.T.; Castro, P.; Batista, R.; Rios, E.; Sobrinho-Simoes, M.; et al. Osteopontin-A splice variant is overexpressed in papillary thyroid carcinoma and modulates invasive behavior. Oncotarget 2016, 7, 52003–52016. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the eastern cooperative oncology group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Rustin, G.J.; Vergote, I.; Eisenhauer, E.; Pujade-Lauraine, E.; Quinn, M.; Thigpen, T.; Du Bois, A.; Kristensen, G.; Jakobsen, A.; Sagae, S.; et al. Definitions for response and progression in ovarian cancer clinical trials incorporating recist 1.1 and ca 125 agreed by the gynecological cancer intergroup (gcig). Int. J. Gynecol. Cancer 2011, 21, 419–423. [Google Scholar] [CrossRef]
- Kraft, J.C.; Freeling, J.P.; Wang, Z.; Ho, R.J. Emerging research and clinical development trends of liposome and lipid nanoparticle drug delivery systems. J. Pharm. Sci. 2014, 103, 29–52. [Google Scholar] [CrossRef]
- Gordon, A.N.; Fleagle, J.T.; Guthrie, D.; Parkin, D.E.; Gore, M.E.; Lacave, A.J. Recurrent epithelial ovarian carcinoma: A randomized phase iii study of pegylated liposomal doxorubicin versus topotecan. J. Clin. Oncol. 2001, 19, 3312–3322. [Google Scholar] [CrossRef]
- Davidson, B.; Berner, A.; Nesland, J.M.; Risberg, B.; Berner, H.S.; Trope, C.G.; Kristensen, G.B.; Bryne, M.; Ann Florenes, V. E-cadherin and alpha-, beta-, and gamma-catenin protein expression is up-regulated in ovarian carcinoma cells in serous effusions. J. Pathol. 2000, 192, 460–469. [Google Scholar] [CrossRef]
- Szubert, S.; Koper, K.; Dutsch-Wicherek, M.M.; Jozwicki, W. High tumor cell vimentin expression indicates prolonged survival in patients with ovarian malignant tumors. Ginekol. Pol. 2019, 90, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Li, B.; Shi, J.; Peng, L.; Zhang, D.; Qian, W.; Hou, S.; Zhao, L.; Gao, J.; Cao, Z.; et al. A humanized anti-osteopontin antibody inhibits breast cancer growth and metastasis in vivo. Cancer Immunol. Immunother. 2010, 59, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, W.; Al-Ahwal, M.; Hamour, O.; Al-Maghrabi, J. Osteopontin cytoplasmic immunoexpression is a predictor of poor disease-free survival in thyroid cancer. J. Microsc. Ultrastruct. 2013, 1, 8–16. [Google Scholar] [CrossRef]
- Tilli, T.M.; Bellahcene, A.; Castronovo, V.; Gimba, E.R. Changes in the transcriptional profile in response to overexpression of the osteopontin-c splice isoform in ovarian (ovcar-3) and prostate (pc-3) cancer cell lines. BMC Cancer 2014, 14, 433. [Google Scholar] [CrossRef]
- Tilli, T.M.; Franco, V.F.; Robbs, B.K.; Wanderley, J.L.; da Silva, F.R.; de Mello, K.D.; Viola, J.P.; Weber, G.F.; Gimba, E.R. Osteopontin-c splicing isoform contributes to ovarian cancer progression. Mol. Cancer Res. 2011, 9, 280–293. [Google Scholar] [CrossRef]
- Hao, C.; Wang, Z.; Gu, Y.; Jiang, W.G.; Cheng, S. Prognostic value of osteopontin splice variant-c expression in breast cancers: A meta-analysis. Biomed. Res. Int. 2016, 2016, 7310694. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antigen Retrieval | Primary Antibody | Secondary Antibody |
|---|---|---|
| Not performed | Chicken Anti-OPNc IgY; | Goat Anti-Chicken IgY (H + L) Biotin Conjugated |
| Ref # AhOPN-c NA, Gallus Immunoyech INc; | REF #A16058, NOVEX–LIFE TECHNOLOGIES®, | |
| Diluted 1:900 in antibody diluent Solution (Thermo Scientific Quanto, | Diluted 1:3000 in antibody diluent Solution (Thermo Scientific Quanto, | |
| Ref #TA-125-ADQ) for 30 min at RT | REF.# TA-125-ADQ) for 16 min | |
| Antibody retrieval solution (Novocastra™-Leica Biosystems, Ref # RE 7119) 40 min at the steamer cooker, followed by 30 min at RT | Goat anti- E-cadherin | Biotinylated Goat Polyvalent |
| Ref#3195 Cell Signaling) | (Ref # TP 125-BNE, Thermo Scientific, | |
| Diluted 1:100 Dilution1:900 in antibody diluent Solution (Thermo Scientific Quanto, Ref # TA-125-ADQ) | Solution ready to use, 10 min, RT | |
| for 1 h at RT | ||
| Antibody retrieval solution (Novocastra™-Leica Biosystems, Ref # RE 7119) 40 min at the steamer cooker, followed by 30 min at RT | Monoclonal mouse anti-Vimentin | Biotinylated Goat Polyvalent |
| Ref # V6389, SIGMA-ALDRICH® | Ref # TP 125-BNE, Thermo Scientific | |
| Diluted 1:400 in antibody diluent Solution (Thermo Scientific Quanto, | ||
| REF.# TA-125-ADQ) for 1h at RT | Solution ready to use, 10 min at RT | |
| Citrate Buffer pH = 6 at microwave oven for 10 min, then 30 min at RT | Goat anti-total OPN; | Rabbit anti-goat |
| Ref # AF1433, R&D Systems; | Ref # E0466, Dako | |
| Diluted 1:450 in antibody diluent Solution Thermo Scientific Quanto, REF. TA-125-ADQ) for 16–18 h at 4 °C | Diluted 1:200 in antibody diluent Solution (Thermo Scientific Quanto, REF. TA-125-ADQ) for 16 min |
| OC Series (n = 68) | PLD Arm (n = 37) | |
|---|---|---|
| Median age at diagnosis (years) | 57.0 (39–79) | 56.5 (39–73) |
| ECOG PS * at diagnosis | ||
| 0 | 29 (42.6%) | 13 (35.1%) |
| 1 | 39 (57.4%) | 24 (64.9%) |
| Stage at diagnosis | ||
| II | 14 (20.6%) | 5 (13.5%) |
| III | 48 (70.6%) | 28 (75.7%) |
| IV | 6 (8.8%) | 4 (10.8%) |
| Lymph node positive | 13 (19.1%) | 10 (27.0%) |
| Laterality | ||
| Unilateral | 41 (60.3%) | 20 (54.1%) |
| Bilateral | 27 (39.7%) | 17 (45.9%) |
| Histologic subtype | ||
| High-grade serous carcinoma | 37 (54.4%) | 22 (59.5%) |
| Low-grade serous carcinoma | 18 (26.5%) | 8 (21.6%) |
| Mucinous | 5 (7.4%) | 3 (8.1%) |
| Clear cells | 4 (5.9%) | 2 (5.4%) |
| Endometrioid | 4 (5.9%) | 2 (5.4%) |
| Initial surgery | 62 (91.2%) | 33 (89.2%) |
| Adjuvant chemotherapy | 62 (91.2%) | 33 (89.2%) |
| Therapy response | 48 (70.6%) | 21 (56.8%) |
| Cases Analyzed (n = 49) | E-cadherin | Vimentin | Cytoplasm OPN | Membrane OPN | Nuclear OPN-c | Cytoplasm OPN-c |
|---|---|---|---|---|---|---|
| Proportion of positive stained cells | ||||||
| <5% | 7 (14.3%) | 30 (61.2%) | 28 (57.1%) | 37 (75.5%) | 2 (4.1%) | 23 (47.0%) |
| 5–25% | 5 (10.2%) | 11 (22.4%) | 6 (12.2%) | 3 (6.1%) | 5 (10.2%) | 4 (8.2%) |
| 25–50% | 5 (10.2%) | 2 (4.1%) | 6 (12.2%) | 4 (8.2%) | 3 (6.1%) | 5 (10.2%) |
| 50–75% | 7 (14.3%) | 1 (2.0%) | 5 (10.2%) | 4 (8.2%) | 7 (14.3%) | 8 (16.3%) |
| >75% | 25 (51.0%) | 5 (10.2%) | 4 (8.2%) | 1 (2.0%) | 32 (65.3%) | 9 (18.4%) |
| Staining intensity | ||||||
| Absent | 5 (10.2%) | 21 (42.9%) | 17 (34.7%) | 29 (59.2%) | 2 (4.1%) | 21 (42.9%) |
| Faint | 8 (16.3%) | 1 (2.0%) | 13 (26.5%) | 2 (4.1%) | 17 (34.7%) | 16 (32.7%) |
| Moderate | 16 (32.7%) | 8 (16.3%) | 14 (28.6%) | 5 (10.2%) | 15 (30.6%) | 9 (18.4%) |
| Strong | 20 (40.9%) | 19 (38.8%) | 5 (10.2%) | 13 (26.4%) | 15 (30.6%) | 3 (6.1%) |
| Staining Score | ||||||
| 0 | 5 (10.2%) | 21 (42.9%) | 17 (34.7%) | 29 (59.2%) | 2 (4.1%) | 21 (42.9%) |
| 1 | 1 (2.0%) | 0 (0.0%) | 8 (16.3%) | 2 (4.1%) | 0 (0.0%) | 2 (4.1%) |
| 2 | 3 (6.1%) | 5 (10.2%) | 3 (6.1%) | 2 (4.1%) | 5 (10.2%) | 3 (6.1%) |
| 3 | 3 (6.1%) | 7 (14.3%) | 8 (16.3%) | 5 (10.2%) | 0 (0.0%) | 4 (8.2%) |
| 4 | 7 (14.3%) | 9 (18.4%) | 4 (8.2%) | 3 (6.1%) | 6 (12.2%) | 6 (12.2%) |
| 5 | 5 (10.2%) | 1 (2.0%) | 4 (8.2%) | 4 (8.2%) | 9 (18.4%) | 8 (16.3%) |
| 6 | 8 (16.3%) | 2 (4.1%) | 4 (8.2%) | 3 (6.1%) | 12 (24.5%) | 2 (4.1%) |
| 7 | 17 (34.7%) | 4 (8.2%) | 1 (2.0%) | 1 (2.0%) | 15 (30.6%) | 3 (6.1%) |
| Cases of the PLD Arm Analyzed (n = 28) | E-cadherin | Vimentin | Cytoplasm OPN | Membrane OPN | Nuclear OPN-c | Cytoplasm OPN-c |
|---|---|---|---|---|---|---|
| Proportion of positive stained cells | ||||||
| <5% | 4 (14.3%) | 17 (60.7%) | 15 (53.6%) | 22 (78.6%) | 1 (3.6%) | 14 (50.0%) |
| 5–25% | 4 (14.3%) | 6 (21.4%) | 3 (10.7%) | 2 (7.1%) | 3 (10.7%) | 1 (3.6%) |
| 25–50% | 0 (0.0%) | 1 (3.6%) | 4 (14.3%) | 2 (7.1%) | 3 (10.7%) | 4 (14.3%) |
| 50–75% | 5 (17.9%) | 0 (0.0%) | 3 (10.7%) | 2 (7.1%) | 2 (7.1%) | 6 (21.4%) |
| >75% | 15 (53.6%) | 4 (14.3%) | 3 (10.7%) | 0 (0.0%) | 19 (67.9% | 3 (10.7%) |
| Staining intensity | ||||||
| Absent | 2 (7.1%) | 13 (46.4%) | 10 (35.7%) | 15 (53.6%) | 1 (3.6%) | 12 (42.9%) |
| Faint | 6 (21.4%) | 0 (0.0%) | 8 (28.6%) | 2 (7.1%) | 10 (35.7%) | 8 (28.6%) |
| Moderate | 6 (21.4%) | 4 (14.3%) | 7 (25.0%) | 2 (7.1%) | 9 (32.1%) | 7 (25.0%) |
| Strong | 14 (50.0%) | 11 (39.3%) | 3 (10.7%) | 9 (32.1%) | 8 (28.6%) | 1 (3.6%) |
| Staining Score | ||||||
| 0 | 2 (7.1%) | 13 (46.4%) | 10 (35.7%) | 15 (53.6%) | 1 (3.6%) | 12 (42.9%) |
| 1 | 1 (3.6%) | 0 (0.0%) | 5 (17.9%) | 2 (7.1%) | 0 (0.0%) | 2 (7.1%) |
| 2 | 2 (7.1%) | 1 (3.6%) | 0 (0.0%) | 1 (3.6%) | 3 (10.7%) | 1 (3.6%) |
| 3 | 2 (7.1%) | 5 (17.9%) | 5 (17.9%) | 5 (17.9%) | 0 (0.0%) | 2 (7.1%) |
| 4 | 3 (10.7%) | 4 (14.3%) | 1 (3.6%) | 1 (3.6%) | 3 (10.7%) | 4 (14.3%) |
| 5 | 3 (10.7%) | 1 (3.6%) | 3 (10.7%) | 2 (7.1%) | 7 (25.0%) | 5 (17.9%) |
| 6 | 4 (14.3%) | 1 (3.6%) | 4 (14.3%) | 2 (7.1%) | 6 (21.4%) | 1 (3.6%) |
| 7 | 11 (39.3%) | 3 (10.7%) | 0 (0.0%) | 0 (0.0%) | 8 (28.6%) | 1 (3.6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dionísio de Sousa, I.J.; Marques, D.S.; Príncipe, C.; Portugal, R.V.; Canberk, S.; Prazeres, H.; Lopes, J.M.; Gimba, E.R.P.; Lima, R.T.; Soares, P. Predictive Biomarkers and Patient Outcome in Platinum-Resistant (PLD-Treated) Ovarian Cancer. Diagnostics 2020, 10, 525. https://doi.org/10.3390/diagnostics10080525
Dionísio de Sousa IJ, Marques DS, Príncipe C, Portugal RV, Canberk S, Prazeres H, Lopes JM, Gimba ERP, Lima RT, Soares P. Predictive Biomarkers and Patient Outcome in Platinum-Resistant (PLD-Treated) Ovarian Cancer. Diagnostics. 2020; 10(8):525. https://doi.org/10.3390/diagnostics10080525
Chicago/Turabian StyleDionísio de Sousa, Isabel J., Durval S. Marques, Catarina Príncipe, Raquel V. Portugal, Sule Canberk, Hugo Prazeres, José M. Lopes, Etel R. P. Gimba, Raquel T. Lima, and Paula Soares. 2020. "Predictive Biomarkers and Patient Outcome in Platinum-Resistant (PLD-Treated) Ovarian Cancer" Diagnostics 10, no. 8: 525. https://doi.org/10.3390/diagnostics10080525
APA StyleDionísio de Sousa, I. J., Marques, D. S., Príncipe, C., Portugal, R. V., Canberk, S., Prazeres, H., Lopes, J. M., Gimba, E. R. P., Lima, R. T., & Soares, P. (2020). Predictive Biomarkers and Patient Outcome in Platinum-Resistant (PLD-Treated) Ovarian Cancer. Diagnostics, 10(8), 525. https://doi.org/10.3390/diagnostics10080525