Bile Acids Quantification by Liquid Chromatography–Tandem Mass Spectrometry: Method Validation, Reference Range, and Interference Study

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Analytical Standards and Solvents
2.2. Calibrators, Quality Control Samples, and Internal Standard Solution
2.3. Sample Collection
2.4. Sample Preparation
2.5. LC–MS/MS Settings
2.6. Validation Procedures
2.7. Reference Ranges
2.8. Interference Study
2.8.1. In Vitro Study
2.8.2. In Vivo Study
3. Results
3.1. LC–MS/MS Optimization
3.2. Method Validation
3.3. Reference Ranges
3.4. Interference Study
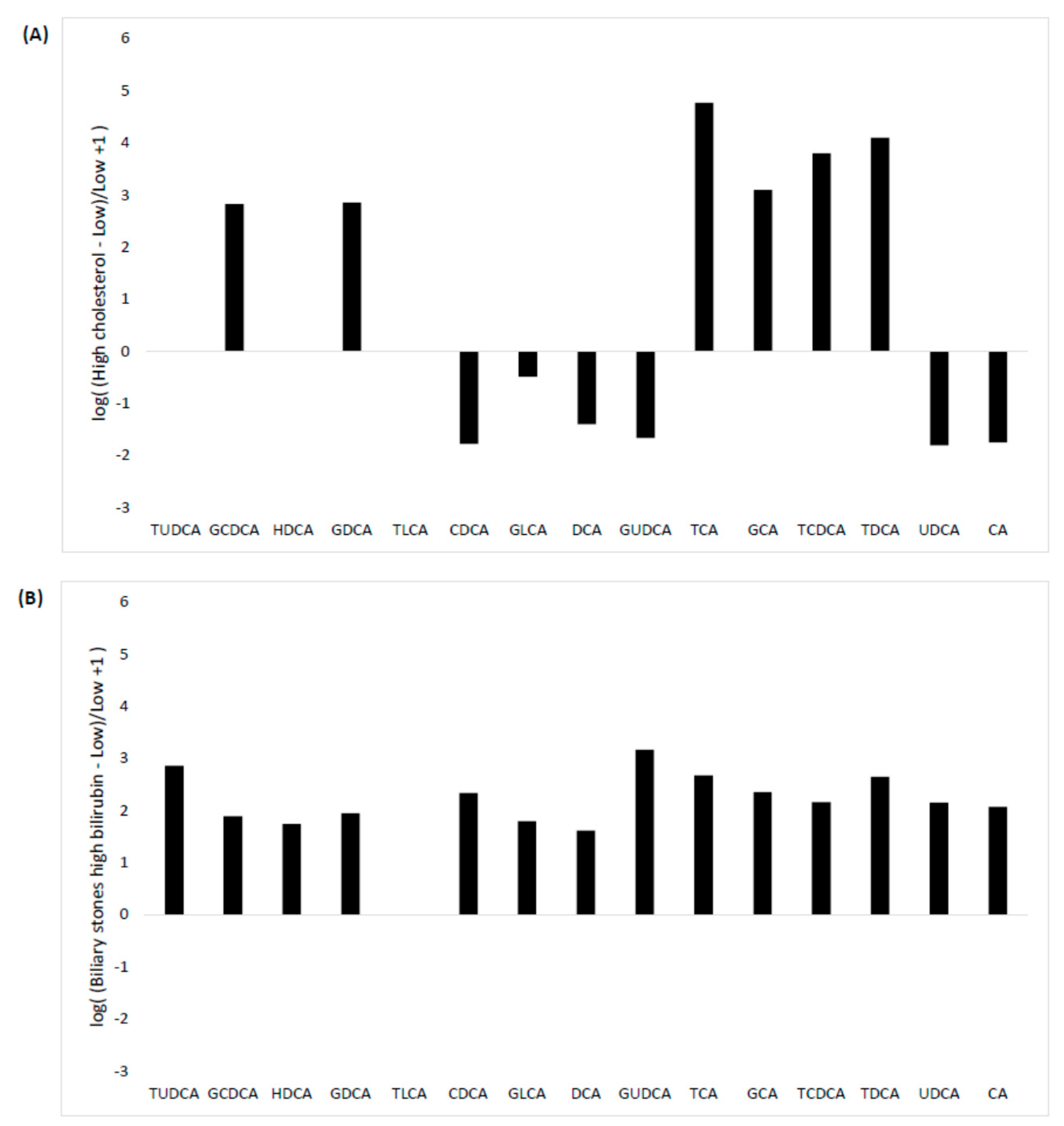
3.4.1. In Vitro Study
3.4.2. In Vivo Study
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chiang, J.Y.L. Bile acid metabolism and signaling. Compr. Physiol. 2013, 3, 1191–1212. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.Y.L. Bile acids: Regulation of synthesis. J. Lipid Res. 2009, 50, 1955–1966. [Google Scholar] [CrossRef] [PubMed]
- Staley, C.; Weingarden, A.R.; Khoruts, A.; Sadowsky, M.J. Interaction of gut microbiota with bile acid metabolism and its influence on disease states. Appl. Microbiol. Biotechnol. 2017, 101, 47–64. [Google Scholar] [CrossRef]
- de Aguiar Vallim, T.Q.; Tarling, E.J.; Edwards, P.A. Pleiotropic Roles of Bile Acids in Metabolism. Cell Metab. 2013, 17, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Kühn, T.; Stepien, M.; López-Nogueroles, M.; Damms-Machado, A.; Sookthai, D.; Johnson, T.; Roca, M.; Hüsing, A.; Maldonado, S.G.; Cross, A.J.; et al. Prediagnostic Plasma Bile Acid Levels and Colon Cancer Risk: A Prospective Study. J. Natl. Cancer Inst. 2019, 112, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.L.; Tomaro-Duchesneau, C.; Prakash, S. The gut microbiome, probiotics, bile acids axis, and human health. Trends Microbiol. 2014, 22, 306–308. [Google Scholar] [CrossRef]
- Stenman, L.K.; Holma, R.; Eggert, A.; Korpela, R. A novel mechanism for gut barrier dysfunction by dietary fat: Epithelial disruption by hydrophobic bile acids. Am. J. Physiol. Gastrointest. Liver Physiol. 2013, 304, G227–G234. [Google Scholar] [CrossRef]
- Duboc, H.; Rajca, S.; Rainteau, D.; Benarous, D.; Maubert, M.-A.; Quervain, E.; Thomas, G.; Barbu, V.; Humbert, L.; Despras, G.; et al. Connecting dysbiosis, bile-acid dysmetabolism and gut inflammation in inflammatory bowel diseases. Gut 2013, 62, 531–539. [Google Scholar] [CrossRef]
- Jia, X.; Lu, S.; Zeng, Z.; Liu, Q.; Dong, Z.; Chen, Y.; Zhu, Z.; Hong, Z.; Zhang, T.; Du, G.; et al. Characterization of Gut Microbiota, Bile Acid Metabolism, and Cytokines in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 71, 893–906. [Google Scholar] [CrossRef]
- Sugita, T.; Amano, K.; Nakano, M.; Masubuchi, N.; Sugihara, M.; Matsuura, T. Analysis of the Serum Bile Acid Composition for Differential Diagnosis in Patients with Liver Disease. Gastroenterol. Res. Pract. 2015, 2015, 1–10. [Google Scholar] [CrossRef]
- Luo, L.; Aubrecht, J.; Li, D.; Warner, R.L.; Johnson, K.J.; Kenny, J.; Colangelo, J.L. Assessment of serum bile acid profiles as biomarkers of liver injury and liver disease in humans. PLoS ONE 2018, 13, e0193824. [Google Scholar] [CrossRef] [PubMed]
- Danese, E.; Ruzzenente, A.; Montagnana, M.; Lievens, P.M.-J. Current and future roles of mucins in cholangiocarcinoma—recent evidences for a possible interplay with bile acids. Ann. Transl. Med. 2018, 6, 333. [Google Scholar] [CrossRef] [PubMed]
- Danese, E.; Salvagno, G.L.; Negrini, D.; Brocco, G.; Montagnana, M.; Lippi, G. Analytical evaluation of three enzymatic assays for measuring total bile acids in plasma using a fully-automated clinical chemistry platform. PLoS ONE 2017, 12, e0179200. [Google Scholar] [CrossRef] [PubMed]
- Rejchrt, S.; Hroch, M.; Repak, R.; Fejfar, T.; Douda, T.; Kohoutova, D.; Peterova, E.; Bures, J. Investigation of 23 Bile Acids in Liver Bile in Benign and Malignant Biliary Stenosis: A Pilot Study. Gastroenterol. Res. Pract. 2019, 2019, 1–7. [Google Scholar] [CrossRef]
- Lynch, K.L. CLSI C62-A: A New Standard for Clinical Mass Spectrometry. Clin. Chem. 2016, 62, 24–29. [Google Scholar] [CrossRef]
- Lippi, G.; Cadamuro, J.; Danese, E.; Gelati, M.; Montagnana, M.; von Meyer, A.; Salvagno, G.L.; Simundic, A.-M. Internal quality assurance of HIL indices on Roche Cobas c702. PLoS ONE 2018, 13, e0200088. [Google Scholar] [CrossRef]
- Lippi, G. Interference studies: Focus on blood cell lysates preparation and testing. Clin. Lab. 2012, 58, 351–355. [Google Scholar]
- Salvagno, G.L.; Favaloro, E.J.; Demonte, D.; Gelati, M.; Poli, G.; Targher, G.; Lippi, G. Influence of hypertriglyceridemia, hyperbilirubinemia and hemolysis on thrombin generation in human plasma. Clin. Chem. Lab. Med. 2019, 57, 1784–1789. [Google Scholar] [CrossRef]
- Fu, X.; Xiao, Y.; Golden, J.; Niu, S.; Gayer, C.P. Serum bile acids profiling by liquid chromatography-tandem mass spectrometry (LC-MS/MS) and its application on pediatric liver and intestinal diseases. Clin. Chem. Lab. Med. 2020, 58, 787–797. [Google Scholar] [CrossRef]
- Succop, P.A.; Clark, S.; Chen, M.; Galke, W. Imputation of data values that are less than a detection limit. J. Occup. Environ. Hyg. 2004, 1, 436–441. [Google Scholar] [CrossRef]
- García-Cañaveras, J.C.; Donato, M.T.; Castell, J.V.; Lahoz, A. Targeted profiling of circulating and hepatic bile acids in human, mouse, and rat using a UPLC-MRM-MS-validated method. J. Lipid Res. 2012, 53, 2231–2241. [Google Scholar] [CrossRef] [PubMed]
- Wegner, K.; Just, S.; Gau, L.; Mueller, H.; Gérard, P.; Lepage, P.; Clavel, T.; Rohn, S. Rapid analysis of bile acids in different biological matrices using LC-ESI-MS/MS for the investigation of bile acid transformation by mammalian gut bacteria. Anal. Bioanal. Chem. 2017, 409, 1231–1245. [Google Scholar] [CrossRef] [PubMed]
- Humbert, L.; Maubert, M.A.; Wolf, C.; Duboc, H.; Mahé, M.; Farabos, D.; Seksik, P.; Mallet, J.M.; Trugnan, G.; Masliah, J.; et al. Bile acid profiling in human biological samples: Comparison of extraction procedures and application to normal and cholestatic patients. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2012, 899, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Burkard, I.; von Eckardstein, A.; Rentsch, K.M. Differentiated quantification of human bile acids in serum by high-performance liquid chromatography–tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2005, 826, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Steiner, C.; von Eckardstein, A.; Rentsch, K.M. Quantification of the 15 major human bile acids and their precursor 7α-hydroxy-4-cholesten-3-one in serum by liquid chromatography–tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2010, 878, 2870–2880. [Google Scholar] [CrossRef]
- Sarafian, M.H.; Lewis, M.R.; Pechlivanis, A.; Ralphs, S.; McPhail, M.J.W.; Patel, V.C.; Dumas, M.-E.; Holmes, E.; Nicholson, J.K. Bile Acid Profiling and Quantification in Biofluids Using Ultra-Performance Liquid Chromatography Tandem Mass Spectrometry. Anal. Chem. 2015, 87, 9662–9670. [Google Scholar] [CrossRef]
- Scherer, M.; Gnewuch, C.; Schmitz, G.; Liebisch, G. Rapid quantification of bile acids and their conjugates in serum by liquid chromatography-tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2009, 877, 3920–3925. [Google Scholar] [CrossRef]
- Inagaki, T.; Moschetta, A.; Lee, Y.-K.; Peng, L.; Zhao, G.; Downes, M.; Yu, R.T.; Shelton, J.M.; Richardson, J.A.; Repa, J.J.; et al. Regulation of antibacterial defense in the small intestine by the nuclear bile acid receptor. Proc. Natl. Acad. Sci. USA 2006, 103, 3920–3925. [Google Scholar] [CrossRef]
- McCauley-Myers, D.L.; Eichhold, T.H.; Bailey, R.E.; Dobrozsi, D.J.; Best, K.J.; Hayes, J.W.; Hoke, S.H. Rapid bioanalytical determination of dextromethorphan in canine plasma by dilute-and-shoot preparation combined with one minute per sample LC-MS/MS analysis to optimize formulations for drug delivery. J. Pharm. Biomed. Anal. 2000, 23, 825–835. [Google Scholar] [CrossRef]
- Salihović, S.; Dickens, A.M.; Schoultz, I.; Fart, F.; Sinisalu, L.; Lindeman, T.; Halfvarson, J.; Orešič, M.; Hyötyläinen, T. Simultaneous determination of perfluoroalkyl substances and bile acids in human serum using ultra-high-performance liquid chromatography-tandem mass spectrometry. Anal. Bioanal. Chem. 2020, 412, 2251–2259. [Google Scholar] [CrossRef]
- Fisher, D.S.; Partridge, S.J.; Handley, S.A.; Couchman, L.; Morgan, P.E.; Flanagan, R.J. LC–MS/MS of some atypical antipsychotics in human plasma, serum, oral fluid and haemolysed whole blood. Forensic Sci. Int. 2013, 229, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Salen, G.; Shefer, S.; Tint, G.S.; Nguyen, L.B.; Parker, T.T.; Chen, T.S.; Roberts, J.; Kong, X.; Greenblatt, D. Regulation of classic and alternative bile acid synthesis in hypercholesterolemic rabbits: Effects of cholesterol feeding and bile acid depletion. J. Lipid Res. 1998, 39, 1608–1615. [Google Scholar] [PubMed]
- Granado-Serrano, A.B.; Martín-Garí, M.; Sánchez, V.; Riart Solans, M.; Berdún, R.; Ludwig, I.A.; Rubió, L.; Vilaprinyó, E.; Portero-Otín, M.; Serrano, J.C.E. Faecal bacterial and short-chain fatty acids signature in hypercholesterolemia. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Charach, G.; Karniel, E.; Novikov, I.; Galin, L.; Vons, S.; Grosskopf, I.; Charach, L. Reduced bile acid excretion is an independent risk factor for stroke and mortality: A prospective follow-up study. Atherosclerosis 2020, 293, 79–85. [Google Scholar] [CrossRef]
- Xie, G.; Wang, Y.; Wang, X.; Zhao, A.; Chen, T.; Ni, Y.; Wong, L.; Zhang, H.; Zhang, J.; Liu, C.; et al. Profiling of Serum Bile Acids in a Healthy Chinese Population Using UPLC–MS/MS. J. Proteome Res. 2015, 14, 850–859. [Google Scholar] [CrossRef]
- Li, Y.; Faden, H.S.; Zhu, L. The Response of the Gut Microbiota to Dietary Changes in the First Two Years of Life. Front. Pharmacol. 2020, 11, 334. [Google Scholar] [CrossRef]
- Jusakul, A.; Khuntikeo, N.; Haigh, W.G.; Kuver, R.; Ioannou, G.N.; Loilome, W.; Namwat, N.; Bhudhisawasdi, V.; Pugkhem, A.; Pairojkul, C.; et al. Identification of biliary bile acids in patients with benign biliary diseases, hepatocellular carcinoma and cholangiocarcinoma. Asian Pac. J. Cancer Prev. 2012, 13 Suppl., 77–82. [Google Scholar]
- Rees, D.O.; Crick, P.J.; Jenkins, G.J.; Wang, Y.; Griffiths, W.J.; Brown, T.H.; Al-Sarireh, B. Comparison of the composition of bile acids in bile of patients with adenocarcinoma of the pancreas and benign disease. J. Steroid Biochem. Mol. Biol. 2017, 174, 290–295. [Google Scholar] [CrossRef]
- Griffiths, W.J.; Sjövall, J. Bile acids: Analysis in biological fluids and tissues. J. Lipid Res. 2010, 51, 23–41. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Bile Acid | Internal Standard | Precursor Ion m/z | Retention Time (min) | Product Ion m/z | Collision Voltage (V) | Calibration Linearity in Methanol (r2) | Calibration Linearity in Steroid-Free Serum (r2) |
|---|---|---|---|---|---|---|---|---|
| STD | Tauroursodeoxycholic acid (TUDCA) | d4-GCA | 498.28 | 2.58 | 80.00 | 60 | 0.998387 | 0.999016 |
| STD | Taurocholic acid (TCA) | d4-TCA | 514.28 | 2.7 | 80.00 | 64 | 0.999312 | 0.999820 |
| STD | Glycoursodeoxycholic acid (GUDCA) | d4-GCA | 448.28 | 2.92 | 74.00 | 35 | 0.997775 | 0.999103 |
| STD | Glycocholic acid (GCA) | d4-GCA | 464.28 | 3.06 | 74.00 | 34 | 0.998718 | 0.999051 |
| STD | Taurochenodeoxycholic acid (TCDCA) | d4-GCA | 498.28 | 3.3 | 80.00 | 60 | 0.997292 | 0.998966 |
| STD | Taurodeoxycholic acid (TDCA) | d4-GCA | 498.28 | 3.46 | 80.00 | 60 | 0.998165 | 0.998822 |
| STD | Cholic acid (CA) | d4-CA | 407.28 | 3.64 | 343.28 | 34 | 0.999410 | 0.999722 |
| STD | Ursodeoxycholic acid (UDCA) | d4-UDCA | 391.28 | 3.65 | 391.28 | 16 | 0.999290 | 0.999731 |
| STD | Glycochenodeoxycholic acid (GCDCA) | d4-CA | 448.28 | 3.67 | 74.00 | 35 | 0.998938 | 0.999806 |
| STD | Hyodeoxycholic acid (HDCA) | d4-CA | 391.28 | 3.77 | 391.28 | 16 | 0.999384 | 0.999745 |
| STD | Glycodeoxycholic acid (GDCA) | d4-CA | 448.28 | 3.87 | 74.00 | 35 | 0.998329 | 0.999870 |
| STD | Taurolithocholic acid (TLCA) | d4-CDCA | 482.28 | 4.02 | 80.00 | 60 | 0.997170 | 0.999418 |
| STD | Chenodeoxycholic acid (CDCA) | d4-CDCA | 391.28 | 4.41 | 391.28 | 16 | 0.999702 | 0.999748 |
| STD | Glycolithocholic acid (GLCA) | d4-DCA | 432.28 | 4.49 | 74.00 | 35 | 0.999886 | 0.998580 |
| STD | Deoxycholic acid (DCA) | d4-DCA | 391.28 | 4.51 | 391.28 | 16 | 0.999446 | 0.999799 |
| IS | Taurocholic acid-d4 (d4-TCA) | 518.28 | 2.7 | 80.00 | 64 | |||
| IS | Glycocholic acid-d4 (d4-GCA) | 468.28 | 3.06 | 74.00 | 34 | |||
| IS | Cholic acid-d4 (d4-CA) | 411.28 | 3.64 | 347.28 | 34 | |||
| IS | Ursodeoxycholic acid-d4 (d4-UDCA) | 395.28 | 3.65 | 395.28 | 16 | |||
| IS | Chenodeoxycholic acid-d4 (d4-CDCA) | 395.28 | 4.41 | 395.28 | 16 | |||
| IS | Deoxycholic acid-d4 (d4-DCA) | 395.28 | 4.51 | 395.28 | 16 |
| BA Species | Mean (ng/mL) | 2.5 Percentile (ng/mL) | 97.5 Percentile (ng/mL) |
|---|---|---|---|
| Total BA | 795.4 | 143.2 | 2152.4 |
| TUDCA | <5 | <5 | 5.2 |
| GCDCA | 203.5 | 24.8 | 706.5 |
| HDCA | 6.9 | <5 | 14.1 |
| GDCA | 75.3 | 7.2 | 273.9 |
| TLCA | <5 | <5 | <5 |
| CDCA | 97.4 | 5.1 | 521.3 |
| GLCA | 5.8 | <5 | 21.7 |
| DCA | 161.4 | 9.6 | 542.8 |
| GUDCA | 40.1 | 3.9 | 145.8 |
| TCA | 11.3 | <5 | 65.9 |
| GCA | 77.4 | 8.6 | 415.1 |
| TCDCA | 24.1 | <5 | 92.8 |
| TDCA | 11.7 | <5 | 45.1 |
| UDCA | 17.9 | <5 | 77.7 |
| CA | 71.3 | <5 | 495.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danese, E.; Negrini, D.; Pucci, M.; De Nitto, S.; Ambrogi, D.; Donzelli, S.; Lievens, P.M.-J.; Salvagno, G.L.; Lippi, G. Bile Acids Quantification by Liquid Chromatography–Tandem Mass Spectrometry: Method Validation, Reference Range, and Interference Study. Diagnostics 2020, 10, 462. https://doi.org/10.3390/diagnostics10070462
Danese E, Negrini D, Pucci M, De Nitto S, Ambrogi D, Donzelli S, Lievens PM-J, Salvagno GL, Lippi G. Bile Acids Quantification by Liquid Chromatography–Tandem Mass Spectrometry: Method Validation, Reference Range, and Interference Study. Diagnostics. 2020; 10(7):462. https://doi.org/10.3390/diagnostics10070462
Chicago/Turabian StyleDanese, Elisa, Davide Negrini, Mairi Pucci, Simone De Nitto, Davide Ambrogi, Simone Donzelli, Patricia M.-J. Lievens, Gian Luca Salvagno, and Giuseppe Lippi. 2020. "Bile Acids Quantification by Liquid Chromatography–Tandem Mass Spectrometry: Method Validation, Reference Range, and Interference Study" Diagnostics 10, no. 7: 462. https://doi.org/10.3390/diagnostics10070462
APA StyleDanese, E., Negrini, D., Pucci, M., De Nitto, S., Ambrogi, D., Donzelli, S., Lievens, P. M.-J., Salvagno, G. L., & Lippi, G. (2020). Bile Acids Quantification by Liquid Chromatography–Tandem Mass Spectrometry: Method Validation, Reference Range, and Interference Study. Diagnostics, 10(7), 462. https://doi.org/10.3390/diagnostics10070462