Arterial Function in Healthy Pregnant Women vs. Non-Pregnant Women—A 10-Year Study

 ,
, 

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Paraclinical Evaluation
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Khalil, A.; Akolekar, R.; Syngelaki, A.; Elkhouli, M.; Nicolaides, K.H. Maternal Hemodynamics at 11-13 Weeks’ Gestation and Risk of Pre-Eclampsia. Ultrasound Obs. Gynecol. 2012, 40, 28–34. [Google Scholar] [CrossRef]
- Kim, H.-L.; Kim, S.-H. Pulse Wave Velocity in Atherosclerosis. Front. Cardiovasc. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Wong, N.D. Metabolic Syndrome, Cardiovascular Risk and Screening for Subclinical Atherosclerosis. Expert Rev. Cardiovasc. Ther. 2009, 7, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-N.; Gao, H.-Q.; Li, B.-Y.; Cheng, M.; Ma, Y.-B.; Zhang, Z.-M.; Gao, X.-M.; Liu, Y.-P.; Wang, M. Pulse Wave Velocity as a marker of Artheriosclerosis and Its Comorbidities in Chinese Patients. Hypertens. Res. 2007, 30, 237–242. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Allali, J.; Chauve, C.; Denise, A.; Drevet, C.; Ferraro, P.; Gautheret, D.; Herrbach, C.; Leclerc, F.; Ouangraoua, A.; Sagot, M.-F.; et al. BRASERO: A Resource for Benchmarking RNA Secondary Structure Comparison Algorithms. Adv. Bioinform. 2012, 2012, 5. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, J.; Gharib, A.M.; Garcia, A.; Heroux, J.; Yazdani, S.K.; Malvè, M.; Tracqui, P.; Martinez, M.A.; Doblare, M.; Finet, G.; et al. Is Arterial Wall-Strain Stiffening an Additional Process Responsible for Atherosclerosis in Coronary Bifurcations?: An in Vivo Study Based on Dynamic CT and MRI. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H1097–H1106. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.S.; Protogerou, A.D.; et al. Expert Consensus Document on the Measurement of Aortic Stiffness in Daily Practice Using Carotid-Femoral Pulse Wave Velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef]
- Inoue, N.; Maeda, R.; Kawakami, H.; Shokawa, T.; Yamamoto, H.; Ito, C.; Sasaki, H. Aortic Pulse Wave Velocity Predicts Cardiovascular Mortality in Middle-Aged and Elderly Japanese Men. Circ. J. 2009, 73, 549–553. [Google Scholar] [CrossRef]
- Stephanie, R.A.; Curtis, L. Heart Disease and Pregnancy. Cardiol. Ther. 2017, 6, 157–173. [Google Scholar]
- Meah, V.L.; Cockcroft, J.R.; Backx, K.; Shave, R.; Stöhr, E.J. Cardiac Output and Related Haemodynamics during Pregnancy: A Series of Meta-Analyses. Heart 2016, 102, 518–526. [Google Scholar] [CrossRef]
- Lopes van Balen, V.A.; van Gansewinkel, T.A.G.; de Haas, S.; van Kuijk, S.M.J.; van Drongelen, J.; Ghossein-Doha, C.; Spaanderman, M.E.A. Physiological Adaptation of Endothelial Function to Pregnancy: Systematic Review and Meta-Analysis. Ultrasound Obs. Gynecol. 2017, 50, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.B.; Abraham, W.T.; Zamudio, S.; Coffin, C.; Merouani, A.; Young, D.; Johnson, A.; Osorio, F.; Goldberg, C.; Moore, L.G.; et al. Temporal Relationships between Hormonal and Hemodynamic Changes in Early Human Pregnancy. Kidney Int. 1998, 54, 2056–2063. [Google Scholar] [CrossRef] [PubMed]
- Elvan-Taşpinar, A.; Franx, A.; Bots, M.L.; Koomans, H.A.; Bruinse, H.W. Arterial Stiffness and Fetal Growth in Normotensive Pregnancy. Am. J. Hypertens. 2005, 18, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Lof, M.; Olausson, H.; Bostrom, K.; Janerot-Sjöberg, B.; Sohlstrom, A.; Forsum, E. Changes in Basal Metabolic Rate during Pregnancy in Relation to Changes in Body Weight and Composition, Cardiac Output, Insulin-like Growth Factor I, and Thyroid Hormones and in Relation to Fetal Growth. Am. J. Clin. Nutr. 2005, 81, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Selzer, A. Risks of Pregnancy in Women With Cardiac Disease. JAMA J. Am. Med. Assoc. 1977, 238, 892–893. [Google Scholar] [CrossRef]
- McFaul, P.B.; Dornan, J.C.; Lamki, H.; Boyle, D. Pregnancy Complicated by Maternal Heart Disease. A Review of 519 Women. Bjog Int. J. Obs. Gynaecol. 1988, 95, 861–867. [Google Scholar] [CrossRef]
- Soma-Pillay, P.; Nelson-Piercy, C.; Tolppanen, H.; Mebazaa, A. Physiological Changes in Pregnancy. Cardiovasc. J. Afr. 2016, 27, 89–94. [Google Scholar] [CrossRef]
- Ngene, N.C.; Moodley, J. Physiology of Blood Pressure Relevant to Managing Hypertension in Pregnancy. J. Matern. Fetal Neonatal Med. 2019, 32, 1368–1377. [Google Scholar] [CrossRef]
- Foo, F.L.; McEniery, C.M.; Lees, C.; Khalil, A. Assessment of Arterial Function in Pregnancy: Recommendations of the International Working Group on Maternal Hemodynamics. Ultrasound Obs. Gynecol. 2017, 50, 324–331. [Google Scholar] [CrossRef]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic Stiffness Is an Independent Predictor of All-Cause and Cardiovascular Mortality in Hypertensive Patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Katsahian, S.; Fassot, C.; Tropeano, A.I.; Gautier, I.; Laloux, B.; Boutouyrie, P. Aortic Stiffness Is an Independent Predictor of Fatal Stroke in Essential Hypertension. Stroke 2003, 34, 1203–1206. [Google Scholar] [CrossRef] [PubMed]
- Boutouyrie, P.; Tropeano, A.I.; Asmar, R.; Gautier, I.; Benetos, A.; Lacolley, P.; Laurent, S. Aortic Stiffness Is an Independent Predictor of Primary Coronary Events in Hypertensive Patients: A Longitudinal Study. Hypertension 2002, 39, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Hwang, S.J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Casiglia, E.; Gasowski, J.; Głuszek, J.; Jankowski, P.; Narkiewicz, K.; Saladini, F.; Stolarz-Skrzypek, K.; Tikhonoff, V.; Van Bortel, L.; et al. Arterial Stiffness, Central Hemodynamics, and Cardiovascular Risk in Hypertension. Vasc. Health Risk Manag. 2011, 2011, 725–739. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-G.; Joo, S.-J. Arterial Stiffness and Cardiovascular Risk. Korean J. Intern. Med. 2019, 34, 504–506. [Google Scholar] [CrossRef]
- Ogola, B.O.; Zimmerman, M.A.; Clark, G.L.; Abshire, C.M.; Gentry, K.M.; Miller, K.S.; Lindsey, S.H. Sex Differences in Cardiovascular and Cerebrovascular Physiology, Disease, and Signaling Mechanisms: New Insights into Arterial Stiffening: Does Sex Matter? Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1073–H1087. [Google Scholar] [CrossRef]
- Mattace-Raso, F.U.S.; Van Der Cammen, T.J.M.; Hofman, A.; Van Popele, N.M.; Bos, M.L.; Schalekamp, M.A.D.H.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.G.; Breteler, M.M.B.; et al. Arterial Stiffness and Risk of Coronary Heart Disease and Stroke: The Rotterdam Study. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef]
- Mzayek, F.; Sherwin, R.; Hughes, J.; Hassig, S.; Srinivasan, S.; Chen, W.; Berenson, G.S. The Association of Birth Weight with Arterial Stiffness at Mid-Adulthood: The Bogalusa Heart Study. J. Epidemiol. Community Health 2009, 63, 729–733. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Recommendations Guiding Physicians in Biomedical Research Involving Human Subjects. JAMA J. Am. Med. Assoc. 1997, 277, 925–926. [Google Scholar] [CrossRef]
- Devices—TensioMed & Arterial Stiffness. Available online: https://www.tensiomed.eu/devices/ (accessed on 1 June 2020).
- EUR-Lex-32016R0679-EN-EUR-Lex. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 1 June 2020).
- Vermeersch, S.J.; Dynamics, B.; Society, L. Determinants of Pulse Wave Velocity in Healthy People and in the Presence of Cardiovascular Risk Factors: ‘Establishing Normal and Reference Values. Eur. Heart J. 2010, 31, 2338–2350. [Google Scholar]
- La Rocca, H.-P.B. Towards applicability of measures of arterial stiffness in clinical routine. Eur. Heart J. 2010, 31, 2320–2322. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Song, T.J.; Song, D.; Lee, K.J.; Kim, E.H.; Lee, H.S.; Nam, C.M.; Nam, H.S.; Kim, Y.D.; Heo, J.H. Brachial-Ankle Pulse Wave Velocity Is a Strong Predictor for Mortality in Patients with Acute Stroke. Hypertension 2014, 64, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Ki, Y.J.; Choi, D.H.; Lee, Y.M.; Lim, L.; Song, H.; Koh, Y.Y. Predictive Value of Brachial-Ankle Pulse Wave Velocity for Long-Term Clinical Outcomes after Percutaneous Coronary Intervention in a Korean Cohort. Int. J. Cardiol. 2014, 175, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Cruickshank, K.; Riste, L.; Anderson, S.G.; Wright, J.S.; Dunn, G.; Gosling, R.G. Aortic Pulse-Wave Velocity and Its Relationship to Mortality in Diabetes and Glucose Intolerance: An Integrated Index of Vascular Function? Circulation 2002, 106, 2085–2090. [Google Scholar] [CrossRef] [PubMed]
- Blacher, J.; Guerin, A.P.; Pannier, B.; Marchais, S.J.; Safar, M.E.; London, G.M. Impact of Aortic Stiffness on Survival in End-Stage Renal Disease. Circulation 1999, 99, 2434–2439. [Google Scholar] [CrossRef] [PubMed]
- Lynch, M.M.; Amoozegar, J.B.; McClure, E.M.; Squiers, L.B.; Broussard, C.S.; Lind, J.N.; Polen, K.N.; Frey, M.T.; Gilboa, S.M.; Biermann, J. Improving Safe Use of Medications During Pregnancy: The Roles of Patients, Physicians, and Pharmacists. Qual. Health Res. 2017, 27, 2071–2080. [Google Scholar] [CrossRef]
- Babiker, A.; El Husseini, M.; Al Nemri, A.; Al Frayh, A.; Al Juryyan, N.; Faki, M.O.; Assiri, A.; Al Saadi, M.; Shaikh, F.; Al Zamil, F. Health Care Professional Development: Working as a Team to Improve Patient Care. Sudan. J. Paediatr. 2014, 14, 9–16. [Google Scholar]
- Yannoutsos, A.; Bahous, S.A.; Safar, M.E.; Blacher, J. Clinical Relevance of Aortic Stiffness in End-Stage Renal Disease and Diabetes: Implication for Hypertension Management. J. Hypertens. 2018, 36, 1237–1246. [Google Scholar] [CrossRef]
- Burton, G.J.; Yung, H.W.; Cindrova-Davies, T.; Charnock-Jones, D.S. Placental Endoplasmic Reticulum Stress and Oxidative Stress in the Pathophysiology of Unexplained Intrauterine Growth Restriction and Early Onset Preeclampsia. Placenta 2009, 30, 43–48. [Google Scholar] [CrossRef]
- Chaiworapongsa, T.; Chaemsaithong, P.; Yeo, L.; Romero, R. Pre-Eclampsia Part 1: Current Understanding of Its Pathophysiology. Nat. Rev. Nephrol. 2014, 10, 466–480. [Google Scholar] [CrossRef]
- Savvidou, M.D.; Hingorani, A.D.; Tsikas, D.; Frölich, J.C.; Vallance, P.; Nicolaides, K.H. Endothelial Dysfunction and Raised Plasma Concentrations of Asymmetric Dimethylarginine in Pregnant Women Who Subsequently Develop Pre-Eclampsia. Lancet 2003, 361, 1511–1517. [Google Scholar] [CrossRef]
- Beck, D.T.; Martin, J.S.; Casey, D.P.; Braith, R.W. Exercise Training Reduces Peripheral Arterial Stiffness and Myocardial Oxygen Demand in Young Prehypertensive Subjects. Am. J. Hypertens. 2013, 26, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Iurciuc, S.; Avram, C.; Turi, V.; Militaru, A.; Avram, A.; Cimpean, A.M.; Iurciuc, M. Physical Training, Hemodynamic Parameters and Arterial Stiffness: Friends or Foes of the Hypertensive Patient? In Vivo 2016, 30, 521–528. [Google Scholar]
- Crişan, S.; Petrescu, L.; Lazăr, M.A.; Văcărescu, C.; Nicola, A.R.; Cozma, D.; Mornoş, C.; Luca, C.T. Reduced Ejection Fraction Heart Failure—New Data from Multicenter Studies and National Registries Regarding General and Elderly Populations: Hopes and Disappointments. Clin. Interv. Aging 2018, 13, 651–656. [Google Scholar] [CrossRef]
- Beetham, K.S.; Giles, C.; Noetel, M.; Clifton, V.; Jones, J.C.; Naughton, G. The Effects of Vigorous Intensity Exercise in the Third Trimester of Pregnancy: A Systematic Review and Meta-Analysis. BMC Pregnancy Childbirth 2019, 19, 281. [Google Scholar] [CrossRef]
- Cavalcante, J.L.; Lima, J.A.C.; Redheuil, A.; Al-Mallah, M.H. Aortic Stiffness: Current Understanding and Future Directions. J. Am. Coll. Cardiol. 2011, 57, 1511–1522. [Google Scholar] [CrossRef]
- Dragan, S.; Buleu, F.; Christodorescu, R.; Cobzariu, F.; Iurciuc, S.; Velimirovici, D.; Xiao, J.; Luca, C.T. Benefits of Multiple Micronutrient Supplementation in Heart Failure: A Comprehensive Review. Crit. Rev. Food Sci. Nutr. 2019, 59, 965–981. [Google Scholar] [CrossRef]
- Vamvakis, A.; Gkaliagkousi, E.; Triantafyllou, A.; Gavriilaki, E.; Douma, S. Beneficial Effects of Nonpharmacological Interventions in the Management of Essential Hypertension. Jrsm Cardiovasc. Dis. 2017, 6, 204800401668389. [Google Scholar] [CrossRef]
- Stoicescu, M.; Csepento, C.; Muţiu, G.; Bungǎu, S. The Role of Increased Plasmatic Renin Level in the Pathogenesis of Arterial Hypertension in Young Adults. Rom. J. Morphol. Embryol. 2011, 52, 419–423. [Google Scholar]
- Vesa, C.M.; Popa, L.; Popa, A.R.; Rus, M.; Zaha, A.A.; Bungau, S.; Tit, D.M.; Corb Aron, R.A.; Zaha, D.C. Current Data Regarding the Relationship between Type 2 Diabetes Mellitus and Cardiovascular Risk Factors. Diagnostics 2020, 10, 314. [Google Scholar] [CrossRef]
- Fujime, M.; Tomimatsu, T.; Okaue, Y.; Koyama, S.; Kanagawa, T.; Taniguchi, T.; Kimura, T. Central Aortic Blood Pressure and Augmentation Index during Normal Pregnancy. Hypertens. Res. 2012, 35, 633–638. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Age Category (Years) | Mean (+2 SD) * | Median (10–90 pc) ** |
|---|---|---|
| <30 years | 6.2 (4.7–7.6) | 6.1 (5.3–7.1) |
| 30–39 years | 6.5 (3.8–9.2) | 6.4 (5.2–8.0) |
| 40–49 | 7.2 (4.6–9.8) | 6.9 (5.9–8.6) |
| 50–59 | 8.3 (4.5–12.1) | 8.1 (6.3–10.0) |
| 60–69 | 10.3 (5.5–15.0) | 9.7 (7.9–13.1) |
| ≥70 | 10.9 (5.5–16.3) | 10.6 (8.0–14.6) |
| Statistics | Age | BMI (Kg/m2) | SBP (mmHg) | DBP (mmHg) | PP (mmHg) | SBPao (mmHg) | HR (1/min) | Brachial AIx (%) | PWVao (m/s) |
|---|---|---|---|---|---|---|---|---|---|
| Mean | 30.15 | 21.43 | 122.30 | 72.62 | 49.68 | 115.21 | 72.28 | −47.41 | 6.78 |
| 29.61 | 21.43 | 122.59 | 74.72 | 47.87 | 109.16 | 71.57 | −49.50 | 7.43 | |
| Standard error | 0.24 | 0.10 | 0.49 | 0.28 | 0.30 | 0.14 | 0.16 | 0.20 | 0.01 |
| 0.22 | 0.09 | 0.42 | 0.30 | 0.28 | 0.55 | 0.48 | 0.79 | 0.02 | |
| Median | 27 | 20.76 | 130 | 75 | 54 | 116 | 73 | −47.47 | 6.81 |
| 31 | 21.36 | 122 | 75 | 48 | 110 | 71 | −50.7 | 7.4 | |
| Mode | 27 | 19.96 | 130 | 75 | 55 | 116 | 73 | −52.6 | 6.78 |
| 32 | 22.58 | 130 | 80 | 40 | 119 | 68 | −34.5 | 7.4 | |
| Standard deviation | 5.22 | 2.27 | 10.72 | 6.06 | 6.51 | 3.11 | 3.49 | 4.36 | 0.16 |
| 4.39 | 1.86 | 8.64 | 6.09 | 5.69 | 11.22 | 9.75 | 16.20 | 0.49 | |
| Sample variance | 27.24 | 5.14 | 114.98 | 36.70 | 42.35 | 9.66 | 12.17 | 19.02 | 0.02 |
| 19.26 | 3.47 | 74.60 | 37.12 | 32.33 | 125.80 | 95.14 | 262.60 | 0.24 | |
| Kurtosis | −0.79 | −0.87 | 0.19 | −0.06 | −0.20 | 0.81 | 0.11 | −1.25 | 6.17 |
| 0.30 | −0.81 | −0.94 | −0.58 | −0.86 | 0.04 | 0.03 | 0.45 | 7.95 | |
| Skewness | 0.77 | 0.50 | −1.15 | −0.05 | −0.94 | −0.95 | −0.68 | −0.04 | −2.18 |
| 0.11 | 0.19 | 0.04 | −0.05 | 0.28 | 0.04 | 0.45 | 0.41 | 2.26 | |
| Range | 25 | 9.65 | 36 | 25 | 26 | 13 | 16 | 17 | 0.92 |
| 25 | 7.52 | 34 | 30 | 20 | 56 | 53 | 101.6 | 3 | |
| Minimum | 20 | 17.30 | 94 | 60 | 29 | 107 | 63 | −57 | 6.09 |
| 20 | 18.20 | 108 | 62 | 40 | 82 | 52 | −85.9 | 6.7 | |
| Maximum | 45 | 26.95 | 130 | 85 | 55 | 120 | 79 | −40 | 7.01 |
| 45 | 25.71 | 142 | 92 | 60 | 138 | 105 | 15.7 | 9.7 |
| Statistics → Variables ↓ | Group | Mean | Standard Deviation | Std. Error Mean | p Value t-Test | p Value Mann–Whitney | |
|---|---|---|---|---|---|---|---|
| Age | Years | 1 | 30.15 | 5.2 | 0.241 | 0.096 | 0.607 |
| 2 | 29.61 | 4.39 | 0.22 | ||||
| BMI | Kg/m2 | 1 | 21.42 | 2.2 | 0.1045 | <0.001 * | 0.034 * |
| 2 | 21.43 | 1.86 | 0.09 | ||||
| Brachial AIx | % | 1 | −47.41 | 4.36 | 0.20 | 0.011* | 0.012 * |
| 2 | −49.50 | 16.20 | 0.79 | ||||
| PWVao | m/s | 1 | 6.77 | 0.157 | 0.007 | <0.001 * | <0.001 * |
| 2 | 7.43 | 0.49 | 0.023 | ||||
| SBP | (mm Hg) | 1 | 122.30 | 10.723 | 0.494 | <0.001 * | <0.001 * |
| 2 | 122.59 | 8.64 | 0.42 | ||||
| DBP | 1 | 72.62 | 6.058 | 0.279 | <0.001 * | <0.001 * | |
| 2 | 74.72 | 6.09 | 0.3 | ||||
| PP | 1 | 49.68 | 6.507 | 0.300 | <0.001 * | <0.001 * | |
| 2 | 47.87 | 5.69 | 0.28 | ||||
| SBPao | 1 | 115.21 | 3.108 | 0.143 | <0.001 * | <0.001 * | |
| 2 | 109.16 | 11.22 | 0.55 | ||||
| HR | 1/min | 1 | 72.28 | 3.488 | 0.161 | <0.001 * | <0.001 * |
| 2 | 71.57 | 9.75 | 0.48 | ||||
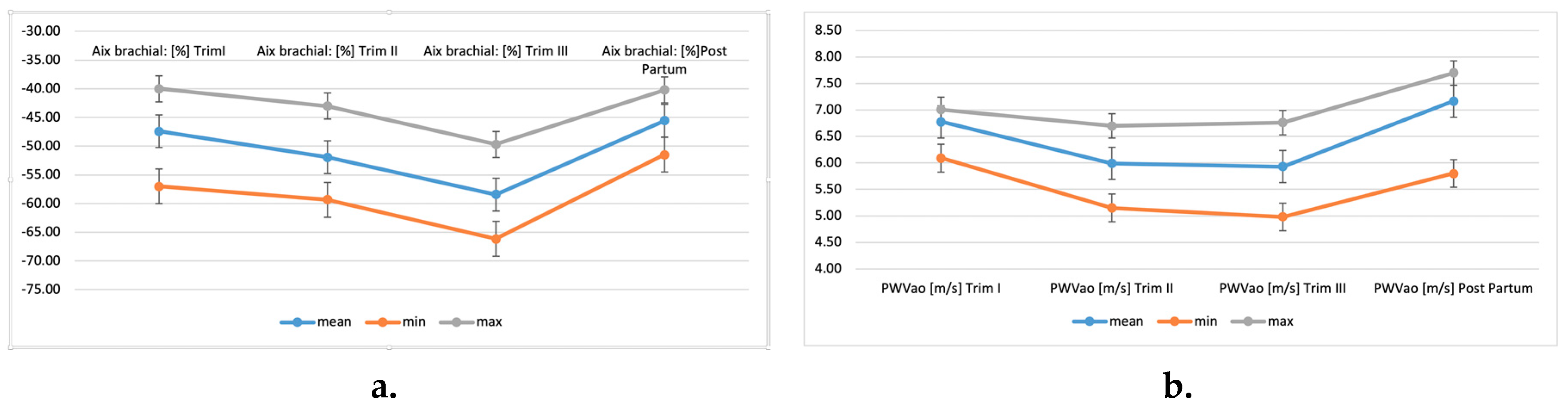
| Statistics | Brachial AIx (%) | PWVao (m/s) | Brachial AIx (%) | PWVao (m/s) | Brachial AIx (%) | PWVao (m/s) | Brachial AIx (%) | PWVao (m/s) |
|---|---|---|---|---|---|---|---|---|
| 1st trimester | 2nd trimester | 3rd trimester | Post-partum | |||||
| Mean | −47.41 | 6.78 | −51.93 | 5.99 | −58.40 | 5.93 | −45.57 | 7.17 |
| Standard error | 0.20 | 0.01 | 0.11 | 0.02 | 0.22 | 0.02 | 0.16 | 0.02 |
| Median | −47.47 | 6.81 | −52.18 | 6.1 | −58.45 | 6.07 | −45.16 | 7.35 |
| Mode | −52.6 | 6.78 | −52.6 | 6.1 | −52.6 | 6.14 | −45.16 | 7.39 |
| Standard deviation | 4.36 | 0.16 | 2.43 | 0.51 | 4.73 | 0.53 | 3.54 | 0.43 |
| Sample variance | 19.02 | 0.02 | 5.89 | 0.26 | 22.37 | 0.28 | 12.51 | 0.18 |
| Kurtosis | −1.25 | 6.17 | 1.86 | −1.65 | −1.41 | −1.18 | −1.38 | 4.64 |
| Skewness | −0.04 | −2.18 | 0.10 | −0.04 | 0.13 | −0.31 | −0.21 | −2.43 |
| Range | 17 | 0.92 | 16.3 | 1.55 | 16.46 | 1.78 | 11.28 | 1.9 |
| Minimum | −57 | 6.09 | −59.3 | 5.15 | −66.15 | 4.98 | −51.5 | 5.8 |
| Maximum | −40 | 7.01 | −43 | 6.7 | −49.69 | 6.76 | −40.22 | 7.7 |
| Statistics | Gestational Period (Weeks) | APGAR Score at 1 min | Foetus Weight (g) |
|---|---|---|---|
| Mean | 39.34 | 9.22 | 3468.97 |
| Standard error | 0.05 | 0.04 | 6.86 |
| Median | 39 | 9 | 3500 |
| Mode | 40 | 10 | 3500 |
| Standard deviation | 1.05 | 0.95 | 148.84 |
| Sample variance | 1.09 | 0.90 | 22,154.52 |
| Kurtosis | 0.97 | 11.92 | −0.09 |
| Skewness | −0.30 | −2.17 | 0.18 |
| Range | 7 | 9 | 820 |
| Minimum | 35 | 1 | 3100 |
| Maximum | 42 | 10 | 3920 |
| Variables | Yes/Yes/Girl/Natural | No/No/Boy/C-Section | ||
|---|---|---|---|---|
| Number | % | Number | % | |
| Group 1 (N1 = 471) | ||||
| Exercise | 160 | 33.97 | 311 | 66.03 |
| Smoker | 194 | 41.19 | 277 | 58.81 |
| Baby gender | 204 | 43.31 | 267 | 56.69 |
| Delivery type | 233 | 49.47 | 238 | 50.53 |
| Group 2 (Control Group, N2 = 416) | ||||
| Exercise | 191 | 45.91 | 225 | 54.09 |
| Smoker | 160 | 38.46 | 256 | 61.54 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turi, V.; Dragan, S.; Iurciuc, M.; Moleriu, L.; Bungau, S.; Tit, D.M.; Toader, D.-O.; Diaconu, C.C.; Behl, T.; Petre, I. Arterial Function in Healthy Pregnant Women vs. Non-Pregnant Women—A 10-Year Study. Diagnostics 2020, 10, 374. https://doi.org/10.3390/diagnostics10060374
Turi V, Dragan S, Iurciuc M, Moleriu L, Bungau S, Tit DM, Toader D-O, Diaconu CC, Behl T, Petre I. Arterial Function in Healthy Pregnant Women vs. Non-Pregnant Women—A 10-Year Study. Diagnostics. 2020; 10(6):374. https://doi.org/10.3390/diagnostics10060374
Chicago/Turabian StyleTuri, Vladiana, Simona Dragan, Mircea Iurciuc, Lavinia Moleriu, Simona Bungau, Delia Mirela Tit, Daniela-Oana Toader, Camelia Cristina Diaconu, Tapan Behl, and Izabella Petre. 2020. "Arterial Function in Healthy Pregnant Women vs. Non-Pregnant Women—A 10-Year Study" Diagnostics 10, no. 6: 374. https://doi.org/10.3390/diagnostics10060374
APA StyleTuri, V., Dragan, S., Iurciuc, M., Moleriu, L., Bungau, S., Tit, D. M., Toader, D.-O., Diaconu, C. C., Behl, T., & Petre, I. (2020). Arterial Function in Healthy Pregnant Women vs. Non-Pregnant Women—A 10-Year Study. Diagnostics, 10(6), 374. https://doi.org/10.3390/diagnostics10060374