Abstract
The first step leading to metastasis, or for the acquisition of local invasiveness, involves changes in the phenotype of neoplastic cells in the primary tumor. The epithelial–mesenchymal transition (EMT) is a process that determines the acquisition of a form and a transcriptional program that are characteristic of mesenchymal cells, in epithelial cells. The factors involved in this process are E-cadherin and N-cadherin adhesion proteins and some transcription factors such as Slug and Twist. EMT is a site-specific mechanism that is also active in embryogenesis—embryonic cells are affected if invested in certain points, probably due to the signals emanating from the cells or groups of surrounding cells. It is known that neuroendocrine neoplasms have a biological behavior that differs in grading, staging, and site. The aim of our study was to investigate the immunohistochemical expression of EMT factors (Twist, Slug, and E-cadherin) in the neuroendocrine neoplasms of the gastrointestinal tract, the pancreas, and lungs, in 65 cases retrieved from the archives of the Department of Pathology, of three hospitals. The immunoscores were compared in each site and correlated with the clinico-pathological parameters. Statistical evaluation revealed an association between the higher Twist immunoscore and higher grading (p value < 0.0001) and staging (p value = 0.0055). Slug was detected only in pancreatic cases where its reduced expression was associated with a higher grading (p value = 0.0033). This data could be of diagnostic utility in the case of metastases from neuroendocrine neoplasm, to define the site of the primitive tumor when the traditional immunohistochemical panel is not sufficient. In summary, our results indicated, first that the EMT is also an active process in neuroendocrine neoplasms. To the best of our knowledge, this was the first study that evaluated the expression of EMT factors in neuroendocrine neoplasms of different districts.
1. Introduction
Neuroendocrine neoplasms (NEN) are rare (around 1–5 cases/100,000/year) and have a low incidence and high prevalence [1]. They arise from neuroendocrine cells that are disseminated all over the body and whose role is essential for the development of organs and the complex functional regulation of tissue. Their biology is strongly related to site, grading, and staging. The most common forms arise from the gastro–entero–pancreatic tract, specifically in the small intestine (19%), appendix (4%), and large intestine (20%), and their pathological classification relies on the morphological and proliferative markers (Table 1). In the gastroenteropancreatic tract [2], these neoplasms are categorized into well differentiated (neuroendocrine tumors, NET) and poorly differentiated forms (neuroendocrine carcinomas, NEC).

Table 1.
Classification of neuroendocrine neoplasms.
While NEC are high grade by definition, NET can be distinguished into low (G1), intermediate (G2), and high (G3) grade forms, on the basis of Ki67 [3] proliferative index/mitotic activity (Table 1).
More and more evidences [4] show that the G3 NET are distinct from G3 NEC, because the former are resistant to cisplatinum/etoposide therapy and show a higher overall survival than NEC. Mixed neuroendocrine/non-neuroendocrine neoplasms are labelled as MiNEN (Mixed Neuroendocrine Neoplasms), when each component constitutes ≥30% of the lesion.
In general, when compared to adenocarcinomatous lesions of the same site, neuroendocrine neoplasms show a better overall survival. However, among them, there are important site-specific differences [1,5] in terms of biology and overall survival, which could be explained by the extreme functional diversity of normal neuroendocrine cells, besides microenvironmental factors.
The current 2015 WHO Classification [6] of neuroendocrine neoplasms of the lungs and thorax catalogues four categories, on the basis of purely morphological parameters (cellular pleomorphism, absence/presence of necrosis, and mitotic activity) (Table 1). Although a grading system is not recommended in lung NEN, typical carcinoid, atypical carcinoid, and neuroendocrine carcinoma (large cell and small cell) are considered synonymous 6, respectively, with the G1, G2, and G3 forms.
Overall, differences among the districts are reflected into differences in the classification systems applied to each site. Despite this, however, a proposal to unify the nomenclature used for neuroendocrine neoplasms deriving from any district of the body is underway [7].
Tumorigenesis is a complex and dynamic process consisting of three steps—initiation, progression, and metastasis [8]. The first step for metastatic evolution is the acquisition of local invasiveness through major changes of cancer cell phenotype. Epithelial–mesenchymal transition (EMT) implies, in epithelial cells, the acquisition of a form and a transcriptional program that are characteristic of mesenchymal cells. This process is normally activated in embryogenesis and at the edge of a wound but also at the border of tumor infiltration. Every type of cancer can follow EMT process, before acquiring motility and invasiveness. Normal and pathological EMT [9] lead to alterations in the expression profiles of some genes—actually, the expression of epithelial markers (E-cadherin and cytokeratin) is repressed while there is an induction of vimentin and this phenotypic switch is turned on by the transcription factor (e.g., Slug, Snail, and Twist).
The clinical implications of EMT programs in cancer were extensively investigated through studies of immunohistochemical expression in several histotypes. For instance, in colo-rectal cancer [10], it was observed that a higher expression of Smad4, a linker of the TGFβ pathway, was related to higher levels of Snail, Slug, and Twist factors, as well as to a reduction of E-cadherin. In breast cancer, Slug is a negative prognostic factor [11] and, in a relevant study of metanalysis (including 2671 patients) [12], it was observed that a higher tissue expression of Twist was correlated with a greater tumor size, lymph nodes metastases, higher grading, and HER2 positivity.
A few studies were conducted to evaluate the expression of EMT factors implicated in gastro-intestinal and pancreatic neuroendocrine tumors [13,14,15]. No statistically significant correlation was detected between E-cadherin loss or Snail/Twist expression and overall survival, but an inverse correlation between E-cadherin and Snail/Twist was present. Recently, it was shown that in pancreatic NETs Slug-mediated EMT was driven by cancer stem cells [16] and that, in this context, immunohistochemical evaluation of Snail and E-cadherin was useful for predicting the risk of vessel invasion and metastasis [17]. Among pulmonary neuroendocrine neoplasms, most of the studies concerned small cell lung carcinoma and showed that EMT triggering can confer resistance to EGFR tyrosine kinase inhibitors [18].
The aim of our study was to assess the expression of EMT proteins in a collection of specimens of gastrointestinal, pancreatic, and pulmonary NEN, and to correlate it with clinico-pathological parameters.
2. Methods
2.1. Collective
The present study was multicentric and included 65 patients affected by neuroendocrine neoplasms, that underwent surgical resection at the Federico II University Hospital (38 cases), at the Monaldi Hospital (15 cases) and at the Cardarelli Hospital (12 cases) of Naples. The specimens were retrieved from the archives of the Department of Pathology of each hospital. The neoplasms were diagnosed in the period between 2001 and 2019, they were re-classified and graded according to the current World Health Organization (WHO) Classification system for neuroendocrine neoplasms of the gastroenteropancreatic tract (2019 WHO), and lung and thorax (2015 WHO). Staging was made in accordance with the American Joint Committee on Cancer (AJCC VIII edition) system [19].
2.2. Immunohistochemistry
Four micrometer sections were used for the immunohistochemistry. Sections were dewaxed in xylene, hydrated in a graded series of alcohol, and subjected to heat-induced antigen retrieval (10 mM Sodium Citrate, 0.05% Tween 20, pH 6.0). After blocking the endogenous peroxidase activity, the tissue was incubated with monoclonal antibody against Slug (sc.166476 clone, mouse, SantaCruz, Santa Cruz, CA, USA- 1:100 dilution) or against E-cadherin (EP700Y clone, rabbit, Ventana, Oro Valley, AZ, USA- 1:100 dilution), or with the polyclonal antibody Twist (49254, rabbit, Abcam, Cambridge, United Kingdom- 1:500 dilution). For all antibodies, the incubation time was of 90 min. Subsequently, the slices were rinsed and incubated with the biotinylated secondary antibody, at room temperature, for 30 min. The bound antibody complexes were stained for 3–5 min, or until appropriate, for microscopic examination with diaminobenzidine, and they were then counterstained with hematoxylin (30 s) and mounted. Appropriate positive controls were chosen—normal breast tissue for Slug, glioblastoma for Twist, and breast cancer for E-cadherin. Negative control was obtained by omitting the primary antibody.
For all cases, Ki67 immunostaining was performed according to the automated procedure (Benchmark XT, Roche-Ventana, Oro Valley, AZ, USA).
2.3. Immunostaining Scoring System
The immunostaining of EMT proteins (Slug and Twist) was evaluated in tumor cells, in the stroma and in normal epithelium. The assessment of their immunostaining was based on the percentage of positive cells—no signal was set as “0”, ≤15% as “1”, >15% and <50% as “2”, and ≥50% as “3”.
For the E-cadherin staining, three categories were identified according to the percentage of cancer cells that preserved membranous staining: <5% positively stained cells were considered as ‘negative’ (score 1), 5–50% were classified as ‘reduced’ (score 2), and >50% stained cells as ‘preserved’ (score 3). All slices were reviewed by four experienced pathologists (M.D., E.G., S.C., and N.D.R.), using light microscopy. In discordant cases, the slides were re-evaluated on a multi-headed microscope to achieve consensus.
For the evaluation of the Ki67 Labeling Index, “hot spot” areas were chosen at a low magnification and an average of the values obtained on 5 adjacent fields (at least 500 neoplastic cells) was calculated [20]. When the score was discordant, it was assessed again, collegially, by manually counting the unlabeled and labeled nuclei on a camera-captured, printed image.
2.4. Statistical Evaluation
The study of association between the scoring group of each marker and clinico-pathological features (age, sex, site, grading and staging) was carried out by Fisher’s exact test. Spearman’s correlation test was used to examine the correlation between Twist and Ki67.
A p value ≤ 0.05 was considered statistically significant. All tests were two sided and carried out with the GraphPad Prism 5 software (GraphPad Software, La Jolla, CA, USA).
2.5. Ethical Approval
This was a retrospective study on tissue samples retrieved from the archives of three hospitals. The project was included in the POR CAMPANIA FESR 2014/2020 RARE.PLAT.NET project (CUP B63D18000380007) that was approved by the Ethics Committee of the Federico II University of Naples (2019/233, 16 July 2019).
For each patient, a written informed consent to use part of the specimen for scientific or the research scopes was provided.
2.6. Declarations
All procedures performed in the study, involving human participants, were in accordance with the ethical standards of the institutional board and with the 1964 Helsinki declaration, including signed informed consent for study participation.
3. Results
3.1. Clinico-Pathological Features
The collective (Table 2 and Table 3) consisted of 31 males and 34 females, aged between 27 and 79 years, with a mean age of 59.57 years and a median age of 61 years. They were all affected by the neuroendocrine neoplasms originating from the gastrointestinal tract, the pancreas, and the lung, respectively, in 28, 19, and 18 cases. The diagnosis was of NET G1 in 17 cases, NET G2 in 14 cases, TC in 10 cases, AC in 5 cases, NET G3 in 2 cases, and NEC in 17 cases. In two cases, NEC co-existed with adenocarcinoma, thereby, the final diagnosis was a high-grade Mixed Neuroendocrine Neoplasm (MiNEN). Ki67 L.I. ranged from 2% in NET G1 to 90% in NEC. We identified two staging groups—in 29 cases the disease was metastatic while in 36 it was non-metastatic (any pT and N0, M0).
Table 2.
Clinico-pathological features of 64 study cases.
Table 3.
Grouping of cases based on the clinico-pathological features.
Tissue was taken from the primary tumor in 60 cases and from a metastatic site in 5 cases (Table 2).
3.2. Differential Expression of Twist in Single Sites
Twist protein showed a nuclear or cytoplasmic signal (Figure 1) and it was expressed in the neoplastic cells in 51 cases, with a score that was variable, being 1, 2, and 3 in 12, 19, and 20 cases, respectively. The cases were subsequently divided into two different scoring groups (independently from cytoplasmic or nuclear staining)—26 with absent/low signal (score 0–1) and 39 with moderate/high signal (score 2–3). Variable expression was also detected in normal tissue.
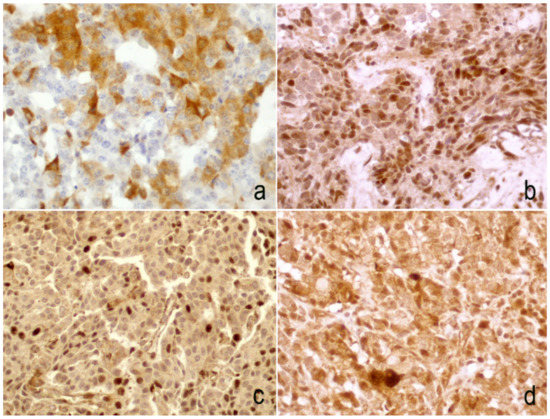
Figure 1.
Examples of the Twist immunoscore—cytoplasmic signal was evident in 15–50% (a) and in >50% (d) of neoplastic cells; in some cases an exclusive nuclear signal was observed in >50% (b) and in 15–50% (c) of neoplastic cells. (b–d. 20× magnification; a. 40× magnification).
In most cases, especially in well-differentiated tumors, the signal was stronger at the periphery of neoplastic nests (Figure 2), where the epithelial cells were in contact with the surrounding stroma.
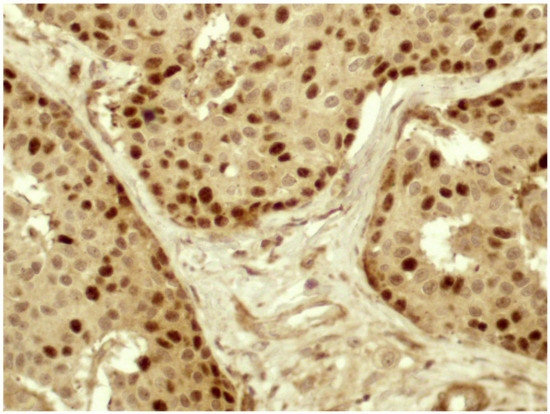
Figure 2.
In most cases, Twist reactivity was located mainly at the periphery of the neoplastic nests, at strict contact with the stroma (40× magnification).
Fisher’s exact test did not reveal any statistically significant correlation with age and sex (Figure 3). However, a higher Twist expression was associated with a higher grading (p value < 0.0001), with metastatic staging (p value = 0.0055), and with gastro-intestinal tract localization (p value = 0.0045).
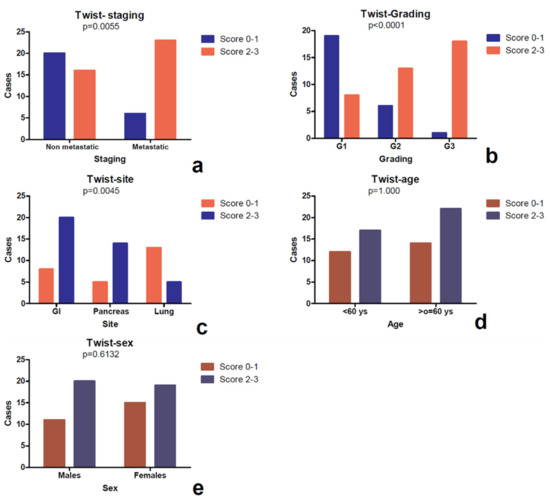
Figure 3.
Study of association between the Twist score and the clinico-pathological parameters assessed by the Fisher’s exact test. It was observed that a higher signal (score 2–3) was more frequent in metastastic cases instead of non metastatic forms (a), in cases with higher grading (b) and in NEN located in the gastrointestinal tract, compared to pancreatic and pulmonary forms (c). No correlation was evident between Twist score and clinical parameters (sex and age) (d,e).
A separate statistical analysis for the cytoplasmic and nuclear stainings did not highlight relevant associations between immunoscoring and the clinico-pathological parameters.
In the subgroup of gastrointestinal and pulmonary neoplasms (Table 4), Twist was confirmed to be a factor related to higher grading (p value = 0.0034 and p value = 0.0129), but not with a higher staging.
Table 4.
Statistical analyses using the Fisher’s exact test.
A slight tendency, although not statistically significant, was observed between a higher Twist score and the metastatic stage (p value = 0.0638) in the gastrointestinal NEN subgroup.
No relevant association was observed between the Twist immunoscoring and the clinico-pathological parameters, among pancreatic lesions.
The comparison between markers highlighted a direct correlation between Twist and Ki67 L.I. (p value = 0.0112, r = 0.3128) (Figure 4).
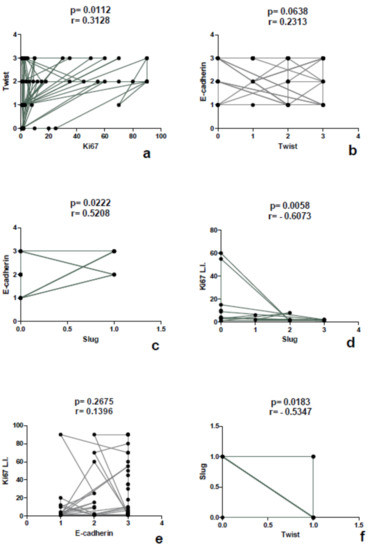
Figure 4.
Correlation study between the markers performed by the Spearman’s exact test. Each dot represents a case.
3.3. Expression of Slug
Slug protein was expressed only in pancreatic neoplasms and was found to be homogeneously negative in all other locations. It showed cytoplasmic signal in 9 cases and the score was 1 in 2 cases, 2 in 3 cases, and 3 in 4 cases. Immunoreactivity was also observed in perilesional pancreatic tissue, but only in endocrine cells (Figure 5a–c). No association was detected between the immunoscore and the clinico-pathological parameters such as age, sex, site (head vs. corpus/tail), and stage. The most evident finding was a direct association between Slug lost/reduced expression and a higher grading (p value = 0.0033) (Figure 6), as well as an inverse correlation between Slug immunoscore and Ki67 L.I. (p value= 0.0058, r= −0.6073) and Twist (p value = 0.0030, r = −0.6428), using a Spearman’s exact test (Figure 4).
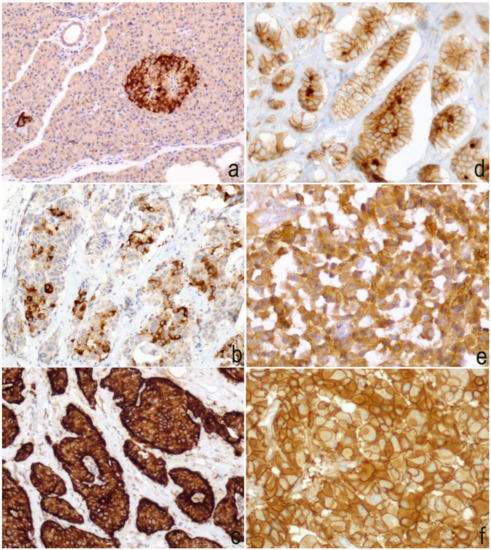
Figure 5.
Slug immunoscore—(a) an intense cytoplasmic immunoreaction was evident in the normal pancreatic tissue that was located exclusively in the neuroendocrine compartment. Negative scores were exocrine pancreas (20× magnification); (b) cytoplasmic signal was observed in 15–50% of neoplastic cells (20× magnification); (c) in this field, strong and diffuse (>50%) immunoreaction was detected in neoplastic cells (40× magnification); (d) 20× magnification, and (e) 40× magnification. E-cadherin expression was reduced compared to cases where the expression was preserved (f) 40× magnification.
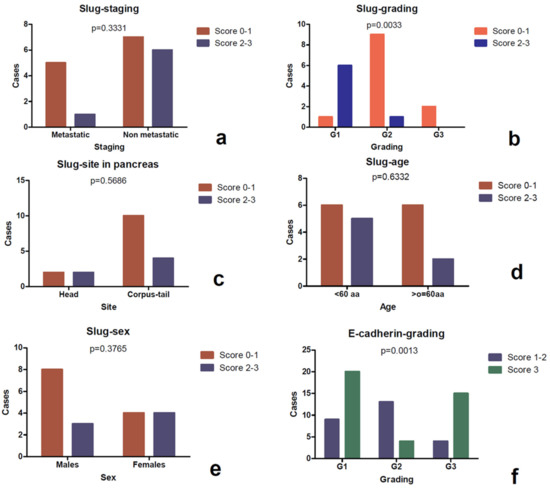
Figure 6.
Study of association between the Slug score and the clinico-pathological parameters assessed by the Fisher’s exact test. It was observed that a higher Slug score (score 2–3) was correlated with a lower grading (b), as well as E-cadherin loss resulted was to be statistically correlated to higher grading (f). Slug was not associated with stageing (a), pancreatic regions (c), age (d) and sex (e).
3.4. Expression of E-Cadherin
E-cadherin was observed at the intercellular junctions and with a partly reduced expression in the cytoplasm of some tumor cells (Figure 5d–f). The expression was preserved (score 3) in 39 cases, reduced (score 2) in 13 cases, and lost (score 1) in 13 cases. In the collective of 65 cases, a significant association was observed between E-cadherin reduced/lost expression and a higher grading (p value = 0.0013) (Figure 6f), and it was confirmed in the pancreatic (p value = 0.0116) and pulmonary (p value = 0.0017) subgroups (Table 4). Not confirmed in the subgroups was the statistically significant association observed in the whole cohort between the metastatic stage and E-cadherin reduction or loss of expression (p value = 0.001). No association was evident with the other clinico-pathological parameters. However, Spearman’s test highlighted a direct correlation (Figure 4) between the Slug and E-cadherin (p value = 0.0222, r = 0.5208) immunoscore.
4. Discussion
The aim of our study was to investigate the potential role of the Epithelial–Mesenchymal Transition process in neuroendocrine neoplasms, through an immunohistochemical study of Twist, Slug, and E-cadherin proteins. These factors were extensively studied in the oncological field [10,11,12], showing possible relevant prognostic factors.
As observed in the literature, both Slug and Twist showed heterogeneous expression in different tumor sites, as well as a variable association with clinico-pathological parameters [8]. Furthermore, within the same tumor, Twist expression appeared to be heterogeneous with a predilection, mainly in well-differentiated forms, at the periphery of epithelial nests, at strict contact with mesenchymal stroma.
In our collective, a higher expression of the Twist factor was observed in the cases with a higher grading. This finding could configure, for this marker, a prognostic role, as a discriminating factor in the post-operative follow-up among the cases that need more or less strict controls. Furthermore, Twist analysis could be a predictive factor for therapeutic options, representing both a useful criterion to choose more aggressive therapeutic regimens, and a therapy resistance factor, as demonstrated in gastric cancer, compared to regimens based on chemotherapy with Paclitaxel [21].
Tumors located in the gastrointestinal tract were characterized by a higher expression of Twist, compared to other sites.
EMT transcription factors are various and are normally expressed in different combinations in different cancer types, demonstrating that EMT programs differ cell by cell and neoplasm by neoplasm [8]. The acquisition of a mesenchymal phenotype can occur also without losing the pre-existent epithelial phenotype. Furthermore, each factor, alone, was not able to determine EMT changes. In our collective, Twist was more expressed in the gastro-intestinal tract, where, however, Slug was not expressed at all. This finding was in contrast with what was observed in other forms of cancer [10,11,12], as well as in neuroendocrine neoplasms of the pancreas where Slug was expressed.
Slug appeared to be a tissue-specific protein within neuroendocrine neoplasms and its loss of expression was associated with an increase in the histological grade of malignancy. This evidence could be of diagnostic utility in the case of metastases from neuroendocrine neoplasms, to define the site of the primitive tumor when the traditional immunohistochemical panel was not sufficient. Moreover, the evidence of Slug in the endocrine component of normal pancreatic tissue is suggestive of its possible role in embryogenesis.
A diagnostic utility of EMT factors could also be hypothesized in lung neoplasms. Indeed, it is well-known that the diagnosis of atypical carcinoid is based on the evaluation of morphological parameters (presence/absence of necrosis and mitotic activity), which are not very objective and have poor reproducibility [22]. The current classification system, in fact, is not very feasible and often does not reflect the actual biological behavior of the examined tumor. The finding of a greater Twist expression in the atypical carcinoid forms, with respect to the typical forms could, therefore, constitute a useful differential diagnostic factor, above all, in cases of limited and not representative biopsies of the whole tumor.
Surprising results were those obtained from the study of the E-cadherin expression. In accordance with what is known in the literature [10,11,23], the loss of expression of the adhesion protein was shown to be greater in cases showing a greater histological grade, therefore was more aggressive, even if no correlation with the tumor stage was observed. Opposite to what was observed in other tumors [10,11,12] was the direct correlation described between the E-cadherin and Slug expression. Generally [8], transcription factors act as an EMT inducer, hence they provoke the transformation from the epithelial cell phenotype into mesenchymal calls, starting from the loss of adhesion proteins (like E-cadherin) and the acquisition of new proteins (e.g., N-cadherin).
In summary, our results are the first to indicate that EMT is also an active process in neuroendocrine neoplasms. To the best of our knowledge, this is the first study that evaluate the expression of EMT factors in neuroendocrine neoplasms of different districts. The finding that Twist is more expressed in the gastro-enteric tract, together with the data, according to which Slug is expressed only in pancreatic NETs, is indicative of the real, possibly different nature and biology of these neuroendocrine neoplasms, according to the different onset site.
Author Contributions
E.G. design of the work, interpretation of data, and drafting the paper; S.C. acquisition of data and drafting the work; S.P. and G.B. methodology; G.D.D. and N.D.R. critical revision of the work; M.D.B.D.C. conception of the work, project administration, and final approval of the version to be published. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by AINET (Associazione Italiana Tumori Neuroendocrini) association and it was part of the POR CAMPANIA FESR 2014/2020 RARE.PLAT.NET project (CUP B63D18000380007).
Conflicts of Interest
The authors declare no competing interests.
References
- Fraenkel, M.; Faggiano, A.; Valk, G.D. Epidemiology of neuroendocrine tumors. Front. Horm. Res. 2015, 44, 1–23. [Google Scholar] [PubMed]
- Klimstra, D.S.; Kloppel, G.; La Rosa, S.; Rindi, G. Classification of Neuroendocrine Neoplasms of the Digestive System. In WHO Classification of Tumors of the Digestive System, 5th ed.; IARC Press: Lyon, France, 2019; pp. 16–19. [Google Scholar]
- Rindi, G.; D’Adda, T.; Froio, E.; Fellegara, G.; Bordi, C. Prognostic factors in gastrointestinal endocrine tumors. Endocr. Pathol. 2007, 18, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Zatelli, M.C.; Guadagno, E.; Messina, E.; Lo Calzo, F.; Faggiano, A.; Colao, A. Open issues on G3 neuroendocrine neoplasms: Back to the future. Endocr. Relat. Cancer 2018, 25, R375–R384. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G.; Rindi, G.; Anlauf, M.; Perren, A.; Komminoth, P. Site-specificbiology and pathology of gastroenteropancreatic neuroendocrine tumors. Virchows Arch. 2007, 451 (Suppl. 1), S9–S27. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, E.; Beasley, M.B.; Austin, J.H.M.; Capelozzi, V.L.; Chirieac, L.R.; Devesa, S.S.; Frank, G.A.; Gazdar, A.; Ishikawa, Y.; Jen, J.; et al. Neuroendocrine tumours. In WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; IARC Press: Lyon, France, 2015; pp. 63–78. [Google Scholar]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Fernandez-Cuesta, L. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, R.A. The biology of cancer. In Garland Science, 2nd ed.; Garland Science, Taylor and Francis Group: New York, NY, USA, 2013; Chapter 14. [Google Scholar]
- Wang, M.; Zhao, J.; Zhang, L.; Wei, F.; Lian, Y.; Wu, Y.; Gong, Z.; Zhang, S.; Zhou, J.; Cao, K.; et al. Role of tumor microenvironment in tumorigenesis. J. Cancer 2017, 8, 761–773. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, M.; Kouvaras, E.; Papamichali, R.; Samara, M.; Chiotoglou, I.; Koukoulis, G. Smad4 and epithelial-mesenchymal transition proteins in colorectal carcinoma: An immunohistochemical study. J. Mol. Histol. 2018, 49, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Sun, X.; Yu, L.; Zhou, R.; Li, A.; Li, M.; Yang, W. Differential expression and clinical significance of epithelial-mesenchymal transition markers among different histological types of triple-negative breast cancer. J. Cancer 2018, 9, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Qiao, W.; Jia, Z.; Liu, H.; Liu, Q.; Zhang, T.; Guo, W.; Li, P.; Deng, M.; Li, S. Prognostic and clinicopathologicalvalue of Twist expression in breastcancer: A meta-analysis. PLoS ONE 2017, 12, e018619. [Google Scholar]
- Fendrich, V.; Maschuw, K.; Waldmann, J.; Buchholz, M.; Rehm, J.; Gress, T.M.; Bartsch, D.K.; König, A. Epithelial-mesenchymaltransitionis a critical step in tumorgenesis of pancreatic neuroendocrine tumors. Cancers 2012, 4, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Galván, J.A.; Astudillo, A.; Vallina, A.; Fonseca, P.J.; Gómez-Izquierdo, L.; García-Carbonero, R.; González, M.V. Epithelial-mesenchymaltransition markers in the differentialdiagnosis of gastroenteropancreatic neuroendocrine tumors. Am. J. Clin. Pathol. 2013, 140, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Cives, M.; Rizzo, F.; Simone, V.; Bisceglia, F.; Stucci, S.; Seeber, A.; Spizzo, G.; Montrone, T.; Resta, L.; Silvestris, F. Reviewing the osteotropism in neuroendocrine tumors: The role of epithelial-mesenchymal transition. Neuroendocrinology 2016, 103, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Ikezono, Y.; Koga, H.; Akiba, J.; Abe, M.; Yoshida, T.; Wada, F.; Nakamura, T.; Iwamoto, H.; Masuda, A.; Sakaue, T.; et al. Pancreatic neuroendocrine tumors and EMT behavior are driven by the CSC marker DCLK1. Mol. Cancer Res. 2017, 15, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Yonemori, K.; Kurahara, H.; Maemura, K.; Mataki, Y.; Sakoda, M.; Iino, S.; Ueno, S.; Shinchi, H.; Natsugoe, S. Impact of snail and E-cadherinexpression in pancreatic neuroendocrine tumors. Oncol. Lett. 2017, 14, 1697–1702. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.; Chiu, Y.F.; Kuo, M.H.; Lee, K.L.; Lee, A.C.; Yu, C.C.; Chang, J.L.; Huang, W.C.; Hsiao, S.H.; Lin, S.E.; et al. Expression of neuroendocrine factor VGF in lung cancer cells confers resistance to EGFR kinase inhibitors and triggers epithelial-to-mesenchymal transition. Cancer Res. 2017, 77, 3013–3026. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Schilsky, R.L.; Laurie, E.G.; Washington, M.K.; Sullivan, D.C.; Brookland, R.K.; Brierley, J.D.; Balch, C.M.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Reid, M.D.; Bagci, P.; Ohike, N.; Saka, B.; Erbarut, S.I.; Dursun, N.; Balci, S.; Gucer, H.; Jang, K.-T.; Tajiri, T.; et al. Calculation of the Ki67 index in pancreatic neuroendocrine tumors: A comparative analysis of four counting methodologies. Mod. Pathol. 2016, 29, 93. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.H.; Park, H.J.; Choi, Y.; Won, Y.J.; Lee, S.J.; Park, D.Y. TWIST mediates resistance to paclitaxel by regulating Akt and Bcl-2 expression in gastric cancer cells. Tumor Biol. 2017, 39. [Google Scholar] [CrossRef] [PubMed]
- Righi, L.; Gatti, G.; Volante, M.; Papotti, M. Lung neuroendocrine tumors: Pathological characteristics. J. Thorac. Dis. 2017, 9 (Suppl. 15), S1442–S1447. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Mandhani, A.; Agrawal, V.; Garg, M. Positive correlation between matrix metalloproteinases and epithelial-to-mesenchymal transition and its association with clinical outcome in bladder cancer patients. Cancer Microenviron. 2018, 11, 23–39. [Google Scholar] [CrossRef] [PubMed]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).