Unstimulated Parotid Saliva Sampling in Juvenile Idiopathic Arthritis and Healthy Controls: A Proof-of-Concept Study on Biomarkers

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Ethical Approval
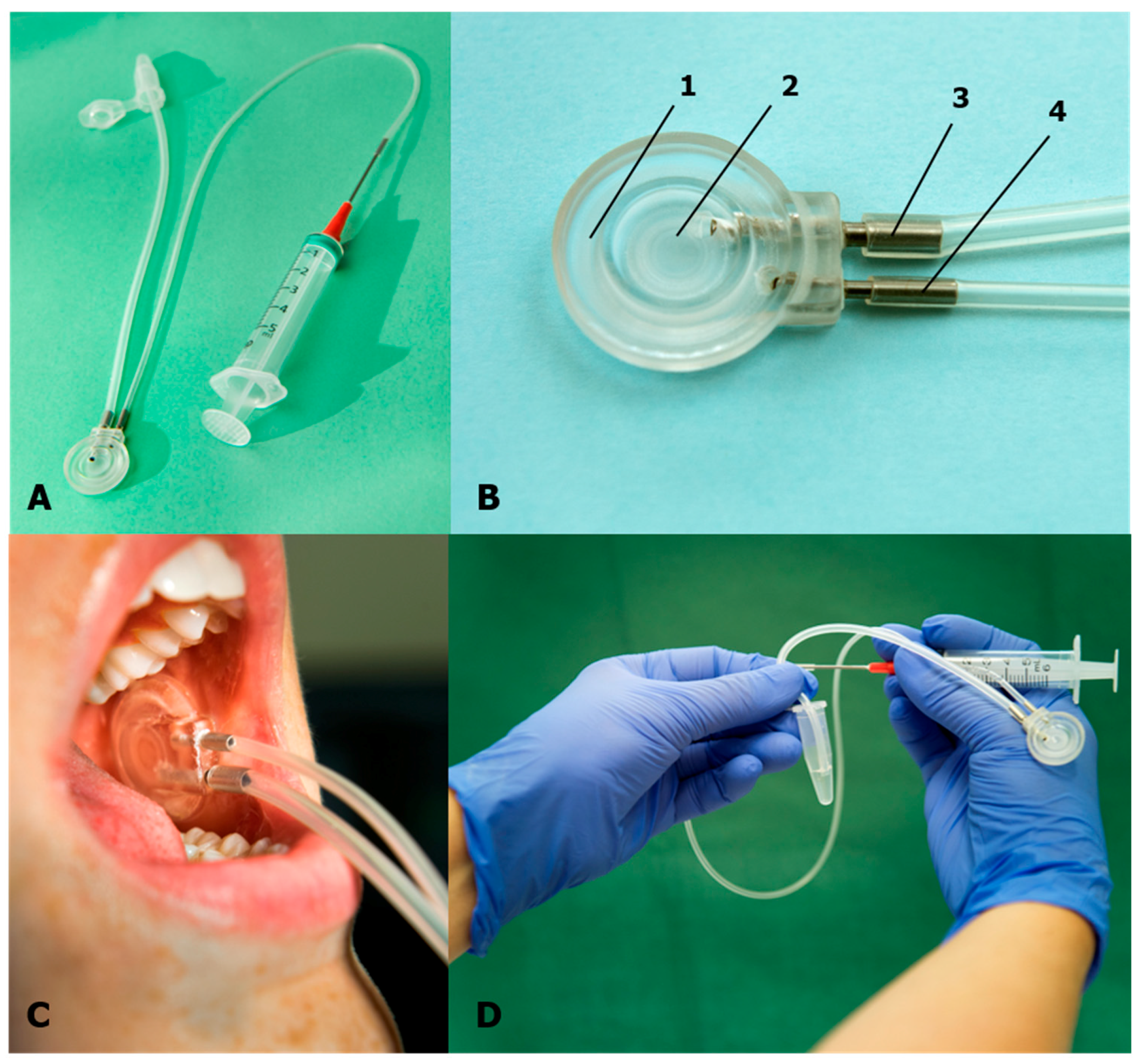
2.3. Parotid Saliva Collection Method
2.4. Biochemical Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
Methodological Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.M.; et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar]
- Ravelli, A.; Martini, A. Juvenile idiopathic arthritis. Lancet 2007, 369, 767–778. [Google Scholar] [CrossRef]
- Prakken, B.; Albani, S.; Martini, A. Juvenile idiopathic arthritis. Lancet 2011, 377, 2138–2149. [Google Scholar] [CrossRef]
- Stoll, M.L.; Kau, C.H.; Waite, P.D.; Cron, R.Q. Temporomandibular joint arthritis in juvenile idiopathic arthritis, now what? Pediatr. Rheumatol. Online J. 2018, 16, 32. [Google Scholar] [CrossRef]
- Svensson, B.; Adell, R.; Kopp, S. Temporomandibular disorders in juvenile chronic arthritis patients. A clinical study. Swed. Dent. J. 2000, 24, 83–92. [Google Scholar]
- Kjellberg, H. Craniofacial growth in juvenile chronic arthritis. Acta Odontol. Scand. 1998, 56, 360–365. [Google Scholar] [CrossRef]
- Lomonaco, T.; Ghimenti, S.; Piga, I.; Biagini, D.; Onor, M.; Fuoco, R.; Di Francesco, F. Influence of sampling on the determination of warfarin and warfarin alcohols in oral fluid. PLoS ONE 2014, 9, e114430. [Google Scholar] [CrossRef]
- Lomonaco, T.; Ghimenti, S.; Piga, I.; Biagini, D.; Onor, M.; Fuoco, R.; Paolicchi, A.; Ruocco, L.; Pellegrini, G.; Trivella, M.G.; et al. Monitoring of warfarin therapy: Preliminary results from a longitudinal pilot study. Microchem. J. 2017, 136, 170–176. [Google Scholar] [CrossRef]
- Segal, A.; Wong, D.T. Salivary diagnostics: Enhancing disease detection and making medicine better. Eur. J. Dent. Educ. Off. J. Assoc. Dent. Educ. Eur. 2008, 12 (Suppl. 1), 22–29. [Google Scholar] [CrossRef]
- Hassaneen, M.; Maron, J.L. Salivary Diagnostics in Pediatrics: Applicability, Translatability, and Limitations. Front. Public Health 2017, 5, 83. [Google Scholar] [CrossRef]
- Ghafouri, B.; Tagesson, C.; Lindahl, M. Mapping of proteins in human saliva using two-dimensional gel electrophoresis and peptide mass fingerprinting. Proteomics 2003, 3, 1003–1015. [Google Scholar] [CrossRef]
- Rathnayake, N.; Akerman, S.; Klinge, B.; Lundegren, N.; Jansson, H.; Tryselius, Y.; Sorsa, T.; Gustafsson, A. Salivary biomarkers for detection of systemic diseases. PLoS ONE 2013, 8, e61356. [Google Scholar] [CrossRef]
- Goodson, J.M.; Kantarci, A.; Hartman, M.L.; Denis, G.V.; Stephens, D.; Hasturk, H.; Yaskell, T.; Vargas, J.; Wang, X.; Cugini, M.; et al. Metabolic disease risk in children by salivary biomarker analysis. PLoS ONE 2014, 9, e98799. [Google Scholar] [CrossRef]
- Selvaraju, V.; Babu, J.R.; Geetha, T. Association of salivary C-reactive protein with the obesity measures and markers in children. Diabet. Metab. Syndr. Obes. Targets Ther. 2019, 12, 1239–1247. [Google Scholar] [CrossRef]
- Ribeiro, C.C.C.; Pacheco, C.J.B.; Costa, E.L.; Ladeira, L.L.C.; Costa, J.F.; da Silva, R.A.; Carmo, C.D.S. Proinflammatory cytokines in early childhood caries: Salivary analysis in the mother/children pair. Cytokine 2018, 107, 113–117. [Google Scholar] [CrossRef]
- Lomonaco, T.; Ghimenti, S.; Biagini, D.; Bramanti, E.; Onor, M.; Bellagambi, F.G.; Fuoco, R.; Di Francesco, F. The effect of sampling procedures on the urate and lactate concentration in oral fluid. Microchem. J. 2017, 136, 255–262. [Google Scholar] [CrossRef]
- Bellagambi, F.G.; Lomonaco, T.; Salvo, P.; Vivaldi, F.; Hangouët, M.; Ghimenti, S.; Biagini, D.; Di Francesc, F.; Fuoco, R. Abdelhamid Errachid Saliva sampling: Methods and devices. An overview. Trends Anal. Chem. 2019, 124. [Google Scholar] [CrossRef]
- Edgar, W.M. Saliva: Its secretion, composition and functions. Br. Dent. J. 1992, 172, 305. [Google Scholar] [CrossRef]
- Nakamura, M.; Slots, J. Salivary enzymes. Origin and relationship to periodontal disease. J. Periodont. Res. 1983, 18, 559–569. [Google Scholar] [CrossRef]
- Al Kawas, S.; Rahim, Z.H.; Ferguson, D.B. Potential uses of human salivary protein and peptide analysis in the diagnosis of disease. Arch. Oral Biol. 2012, 57, 1–9. [Google Scholar] [CrossRef]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Shannon, I.L.; Prigmore, J.R.; Chauncey, H.H. Modified Carlson-Crittenden device for the collection of parotid fluid. J. Dent. Res. 1962, 41, 778–783. [Google Scholar] [CrossRef]
- Chiappin, S.; Antonelli, G.; Gatti, R.; De Palo, E.F. Saliva specimen: A new laboratory tool for diagnostic and basic investigation. Clin. Chim. Acta Int. J. Clin. Chem. 2007, 383, 30–40. [Google Scholar] [CrossRef]
- Dabitao, D.; Margolick, J.B.; Lopez, J.; Bream, J.H. Multiplex measurement of proinflammatory cytokines in human serum: Comparison of the Meso Scale Discovery electrochemiluminescence assay and the Cytometric Bead Array. J. Immunol. Methods 2011, 372, 71–77. [Google Scholar] [CrossRef]
- Gerdle, B.; Bäckryd, E.; Falkenberg, T.; Lundström, E.; Ghafouri, B. Changes in inflammatory plasma proteins from patients with chronic pain associated with treatment in an interdisciplinary multimodal rehabilitation program—An explorative multivariate pilot study. Scand. J. Pain 2019, 20, 125–138. [Google Scholar] [CrossRef]
- Moret, S.; Coudert, J.L.; Bejat, C.; Robin, O.; Lissac, M. The influence of basal anxiety on unstimulated parotid and submandibular saliva. Arch. Oral Biol. 1993, 38, 751–754. [Google Scholar] [CrossRef]
- Villa, A.; Connell, C.L.; Abati, S. Diagnosis and management of xerostomia and hyposalivation. Ther. Clin. Risk Manag. 2015, 11, 45–51. [Google Scholar] [CrossRef]
- Crossner, C.G. Salivary flow rate in children and adolescents. Swed. Dent. J. 1984, 8, 271–276. [Google Scholar]
- Shannon, I.L.; Feller, R.P. Parotid saliva flow rate, calcium, phosphorus, and magnesium concentrations in relation to dental caries experience in children. Pediatr. Dent. 1979, 1, 16–20. [Google Scholar]
- Bretz, W.A.; do Valle, E.V.; Jacobson, J.J.; Marchi, F.; Mendes, S.; Nor, J.E.; Cancado, M.F.; Schneider, L.G. Unstimulated salivary flow rates of young children. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 541–545. [Google Scholar] [CrossRef]
- Helenius, L.M.; Meurman, J.H.; Helenius, I.; Kari, K.; Hietanen, J.; Suuronen, R.; Hallikainen, D.; Kautiainen, H.; Leirisalo-Repo, M.; Lindqvist, C. Oral and salivary parameters in patients with rheumatic diseases. Acta Odontol. Scand. 2005, 63, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Moen, K.; Bertelsen, L.T.; Hellem, S.; Jonsson, R.; Brun, J.G. Salivary gland and temporomandibular joint involvement in rheumatoid arthritis: Relation to disease activity. Oral Dis. 2005, 11, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Hammenfors, D.S.; Valim, V.; Bica, B.; Pasoto, S.G.; Lilleby, V.; Nieto-González, J.C.; Silva, C.A.; Mossel, E.; Pereira, R.M.R.; Coelho, A.; et al. Juvenile Sjögren’s Syndrome: Clinical Characteristics With Focus on Salivary Gland Ultrasonography. Arth. Care Res. 2020, 72, 78–87. [Google Scholar] [CrossRef]


{kind=link}
| Patients | Healthy Individuals | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Percentiles | Percentiles | ||||||||
| Median | 25th | 75th | n | Median | 25th | 75th | n | ||
| Individuals | |||||||||
| Age | years | 12 | 10 | 15 | 45 | 13 | 10 | 13 | 16 |
| Sex | boys/girls | 12/33 | 5/11 | ||||||
| Age at diagnosis | years | 9 | 5 | 12 | 45 | n.a | |||
| Disease duration | years | 4 | 3 | 7 | 45 | n.a | |||
| Patients | Healthy Individuals | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Percentiles | Percentiles | |||||||||
| Median | 25th | 75th | n | Median | 25th | 75th | n | p | ||
| Time | min | 15 | 12 | 30 | 45 | 14 | 10 | 19 | 16 | 0.162 |
| Flow | mL/min | 0.016 | 0.007 | 0.020 | 45 | 0.020 | 0.014 | 0.036 | 16 | 0.039 |
| First 10 | Last 10 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Percentiles | Percentiles | |||||||||
| Saliva | Median | 25th | 75th | n | Median | 25th | 75th | n | p | |
| Time | min | 14 | 11 | 15 | 10 | 16 | 13 | 22 | 10 | 0.218 |
| Flow | ml/min | 0.025 | 0.020 | 0.030 | 10 | 0.020 | 0.010 | 0.020 | 10 | 0.165 |
| Abbreviations | Proteins | Detected in Proportion of Assayed Samples | Detection Limit (pg/mL) |
|---|---|---|---|
| bFGF | Basic fibroblast growth factor | 6/6 | 0.14 |
| CRP | C-Reactive Protein | 5/6 | 2.9 |
| Eotaxin | Eosinophil chemotactic protein | 5/5 | 0.88 |
| Eotaxin-3 | Eosinophil chemotactic protein 3 | 5/5 | 1.7 |
| Flt-1 | Vascular endothelial growth factor receptor 1 | 6/6 | 1.2 |
| GM-CSF | Granulocyte-macrophage colony-stimulating factor | 5/5 | 0.11 |
| ICAM-1 | Intercellular adhesion molecule 1 | 6/6 | 2.55 |
| IFN-γ | Interferon gamma | 6/6 | 0.40 |
| IL-10 | Interleukin 10 | 6/6 | 0.03 |
| IL-12/23p40 | 23p40 Interleukin 12/23 disulfide-linked p40 | 5/5 | 0.24 |
| IL-12p70 | Interleukin 12, p70 | 2/6 | 0.04 |
| IL-13 | Interleukin 13 | 6/6 | 0.73 |
| IL-15 | Interleukin 15 | 5/5 | 0.17 |
| IL-16 | Interleukin 16 | 5/5 | 0.80 |
| IL-17A | Interleukin-17A | 5/5 | 0.22 |
| IL-1α | Interleukin 1α | 5/5 | 0.04 |
| IL-1β | Interleukin 1β | 6/6 | 0.02 |
| IL-2 | Interleukin 2 | 6/6 | 0.05 |
| IL-4 | Interleukin 4 | 4/6 | 0.01 |
| IL-6 | Interleukin 6 | 6/6 | 0.04 |
| IL-7 | Interleukin 7 | 5/5 | 0.08 |
| IL-8 | Interleukin 8 | 6/6 | 0.03 |
| IL-8(HA) | Interleukin anti-hu-8 | 2/5 | 186 |
| IP-10 | kDa interferon gamma-induced protein | 5/5 | 0.09 |
| MCP-1 | Monocyte chemoattractant protein | 5/5 | 0.07 |
| MCP-4 | Monocyte chemoattractant protein 4 | 5/5 | 1.40 |
| MDC | Macrophage-derived chemokine | 5/5 | 1.77 |
| MIP-1α | Macrophage inflammatory protein 1-alpha | 5/5 | 2.10 |
| MIP-1β | Macrophage inflammatory protein 1-beta | 5/5 | 0.04 |
| PlGF | Placental growth factor | 6/6 | 0.14 |
| SAA | Serum amyloid A-1 protein | 6/6 | 18 |
| TARC | Thymus and activation-regulated chemokine | 5/5 | 0.05 |
| Tie-2 | Angiopoietin-1 receptor/Endothelial tyrosine kinase | 2/6 | 43 |
| TNF | Tumor necrosis factor | 6/6 | 0.06 |
| VCAM-1 | Vascular cell adhesion protein 1 | 5/6 | 7.8 |
| VEGF | Vascular Endothelial Growth Factor | 5/5 | 0.70 |
| VEGF | Vascular endothelial growth factor | 5/6 | 0.42 |
| VEGF-C | Vascular endothelial growth factor C | 6/6 | 18 |
| VEGF-D | Vascular endothelial growth factor D | 5/6 | 4.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimitrijevic Carlsson, A.; Ghafouri, B.; Starkhammar Johansson, C.; Alstergren, P. Unstimulated Parotid Saliva Sampling in Juvenile Idiopathic Arthritis and Healthy Controls: A Proof-of-Concept Study on Biomarkers. Diagnostics 2020, 10, 251. https://doi.org/10.3390/diagnostics10040251
Dimitrijevic Carlsson A, Ghafouri B, Starkhammar Johansson C, Alstergren P. Unstimulated Parotid Saliva Sampling in Juvenile Idiopathic Arthritis and Healthy Controls: A Proof-of-Concept Study on Biomarkers. Diagnostics. 2020; 10(4):251. https://doi.org/10.3390/diagnostics10040251
Chicago/Turabian StyleDimitrijevic Carlsson, Alexandra, Bijar Ghafouri, Carin Starkhammar Johansson, and Per Alstergren. 2020. "Unstimulated Parotid Saliva Sampling in Juvenile Idiopathic Arthritis and Healthy Controls: A Proof-of-Concept Study on Biomarkers" Diagnostics 10, no. 4: 251. https://doi.org/10.3390/diagnostics10040251
APA StyleDimitrijevic Carlsson, A., Ghafouri, B., Starkhammar Johansson, C., & Alstergren, P. (2020). Unstimulated Parotid Saliva Sampling in Juvenile Idiopathic Arthritis and Healthy Controls: A Proof-of-Concept Study on Biomarkers. Diagnostics, 10(4), 251. https://doi.org/10.3390/diagnostics10040251