Grip Strength: A Useful Marker for Composite Hepatic Events in Patients with Chronic Liver Diseases

Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. GS and Skeletal Muscle Mass Index
2.3. Primary Outcome Measure of This Study
2.4. Physical Component Summary Score and Mental Component Summary Score on the SF36
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
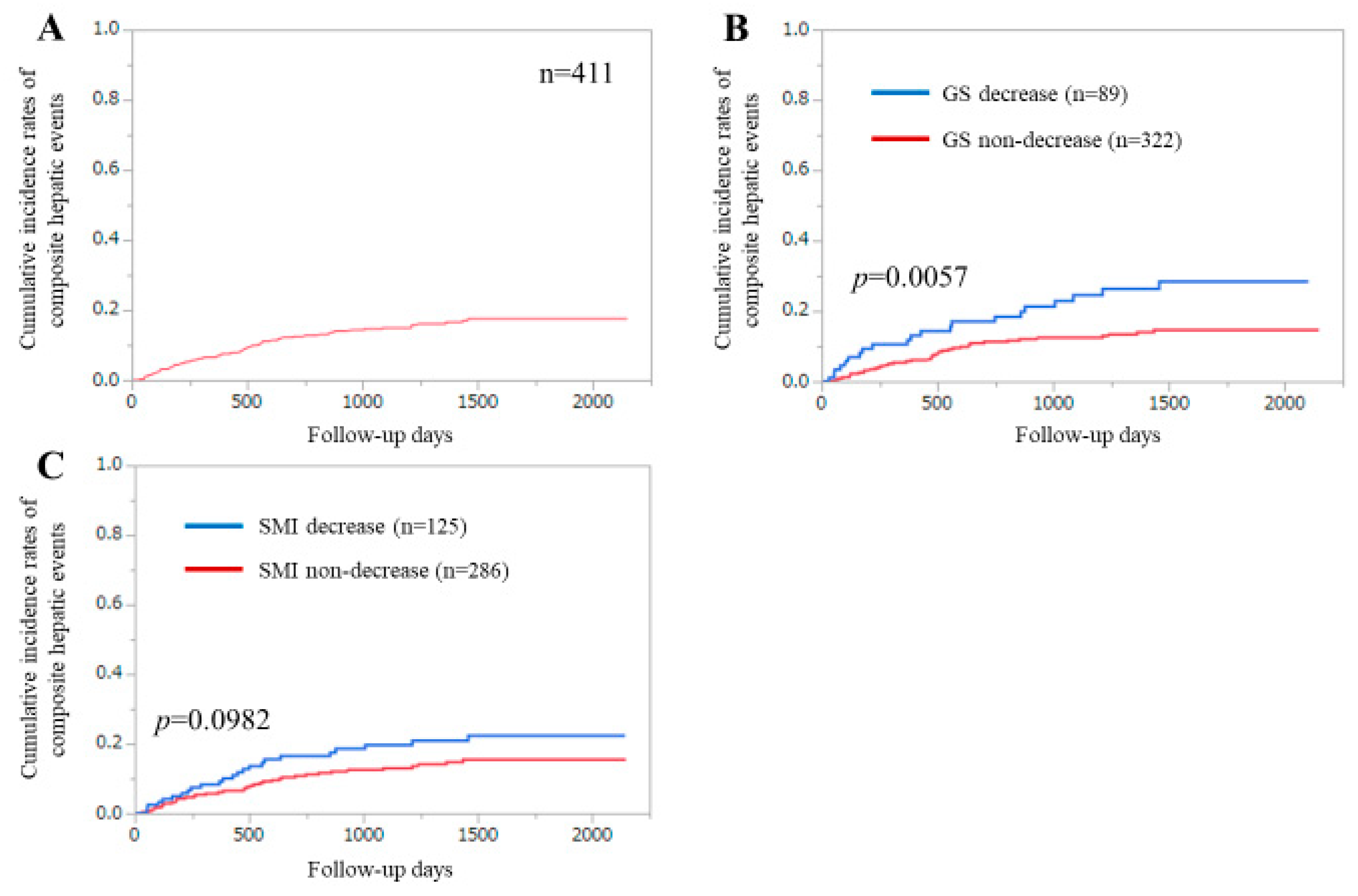
3.2. Cumulative Incidences of CHEs for All Cases
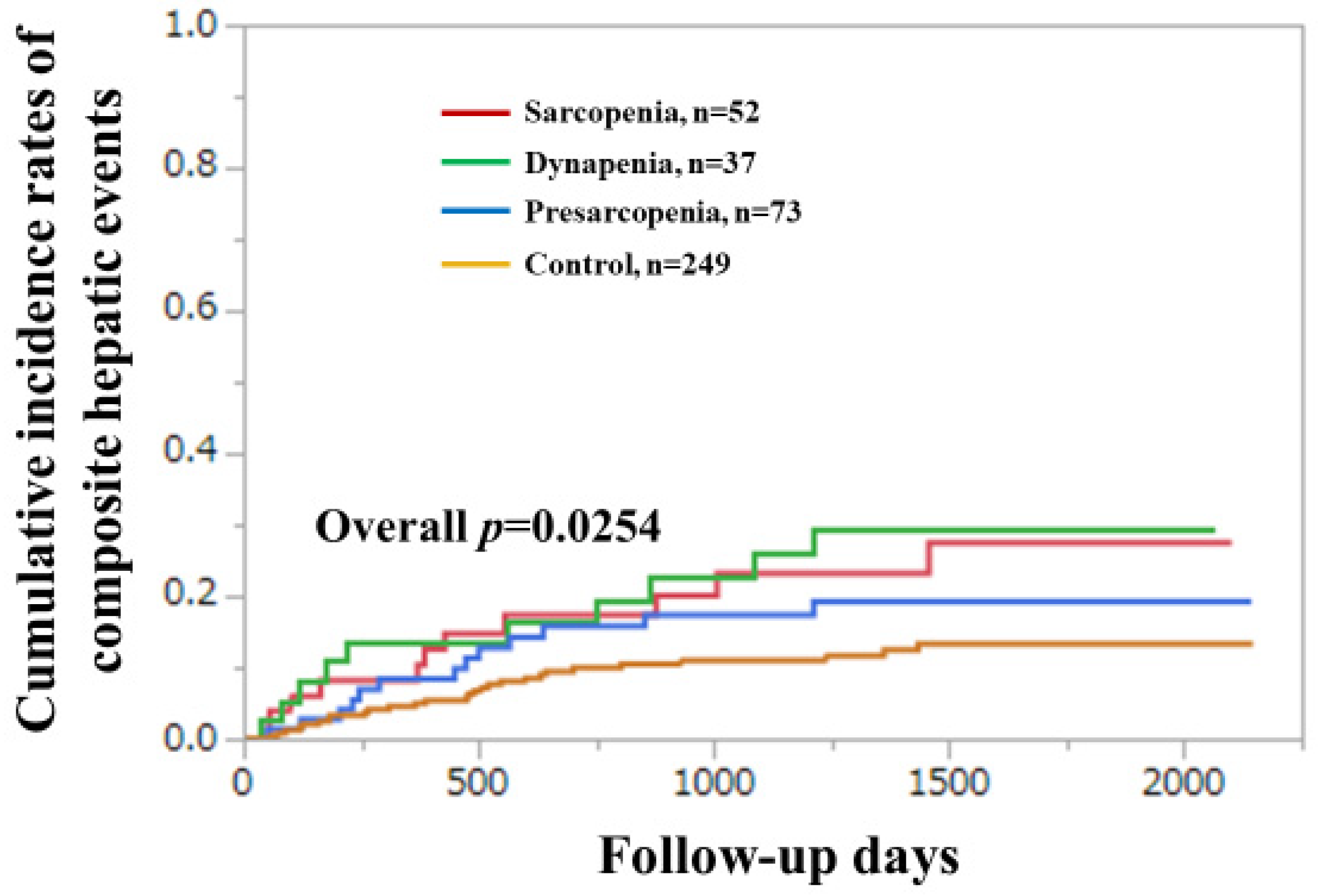
3.3. Cumulative Incidences of CHEs for All Cases Stratified by GS or SMI
3.4. Uni- and Multivariate Analyses of Factors Linked to the Incidence of CHEs
3.5. Subgroup Analysis 1. Cumulative Incidences of CHEs for LC Cases and Non-LC Cases Stratified by GS and SMI
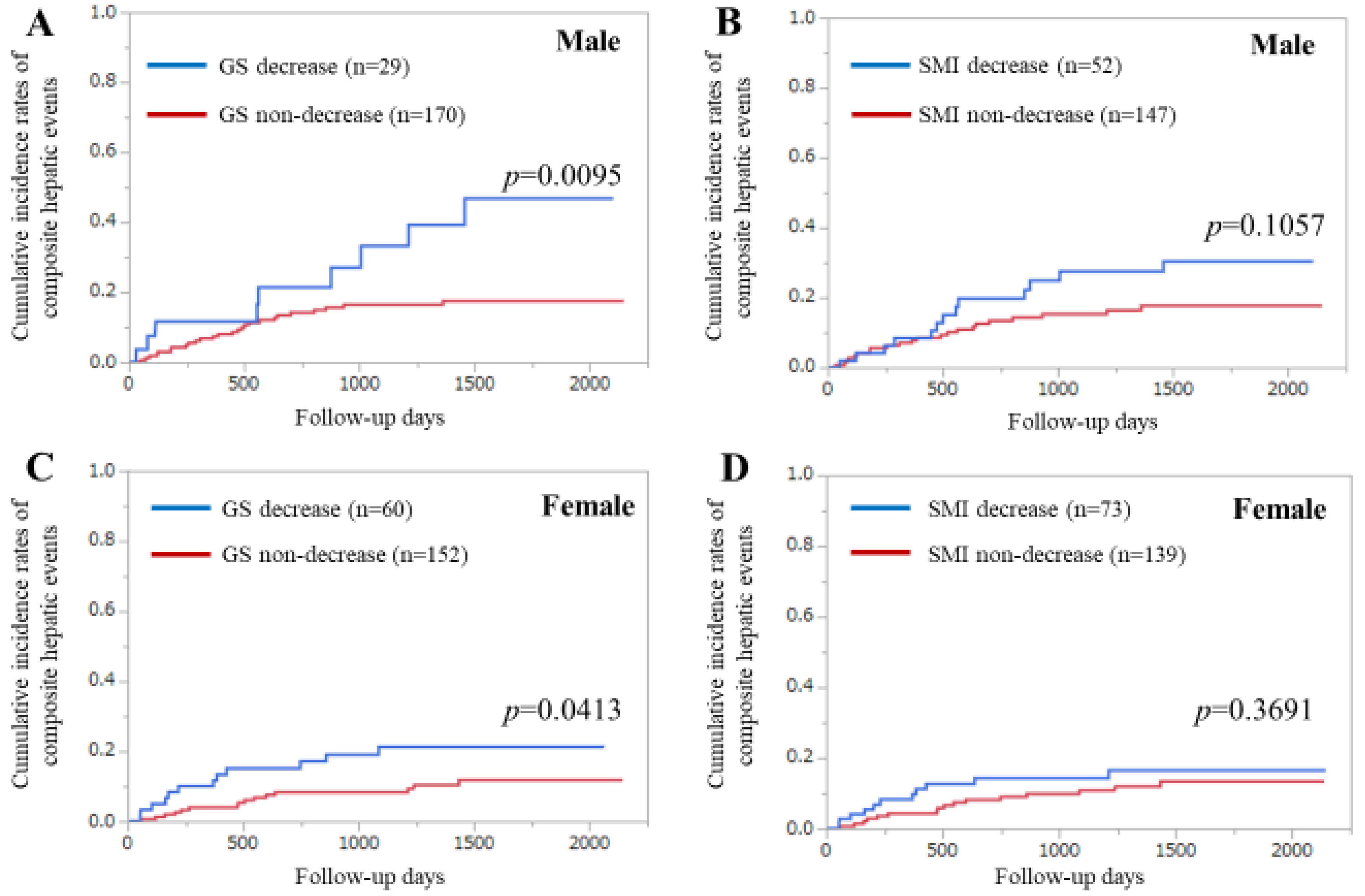
3.6. Subgroup Analysis 2. Cumulative Incidence Rates of CHEs for Male and Female Cases Stratified by GS and SMI
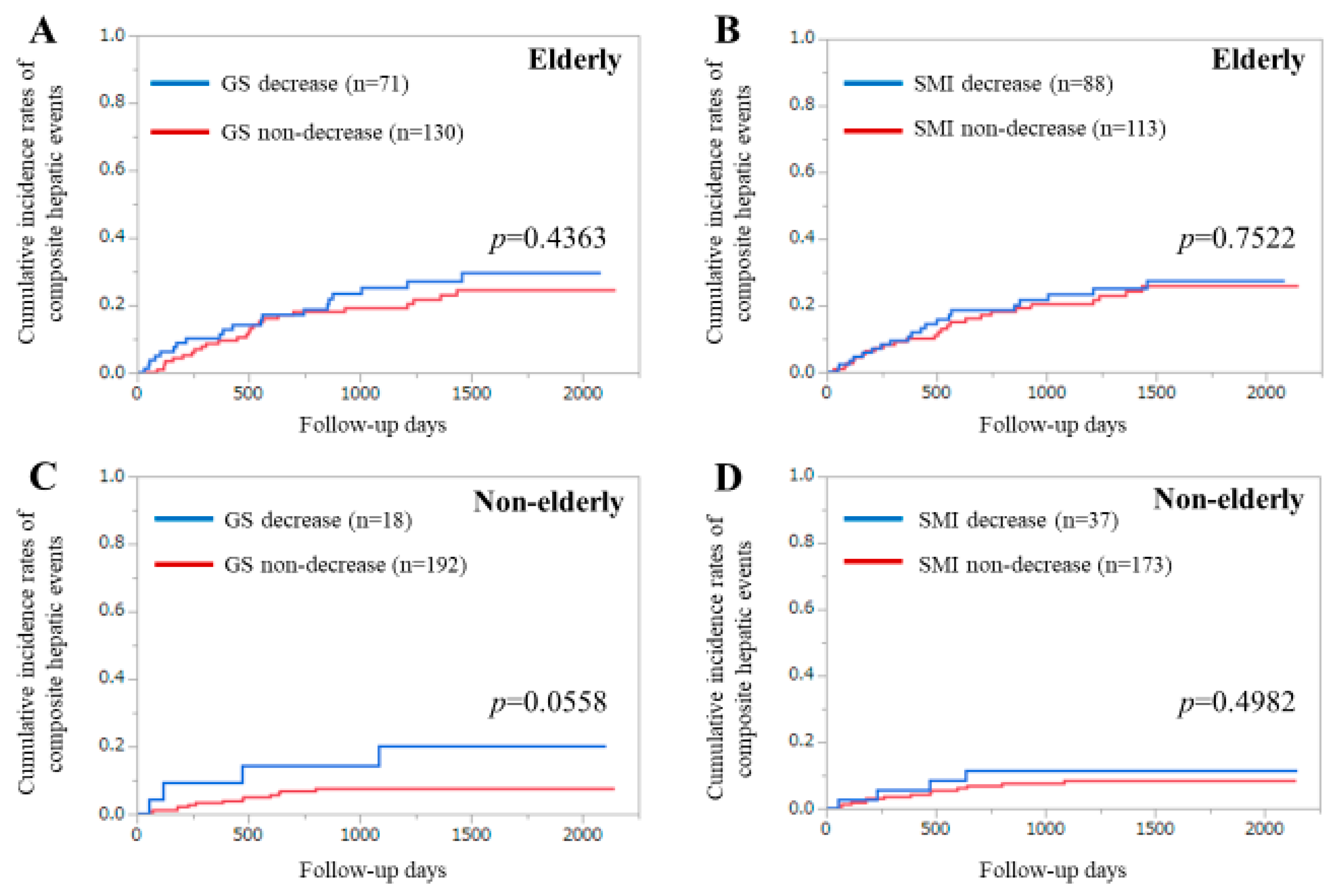
3.7. Subgroup Analysis 3. Cumulative Incidence Rates of CHEs for Elderly Cases and Younger Cases Stratified by GS and SMI
3.8. Additional Analyses Using Different Cutoff Point of GS in Men (<28 kg)
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | alanine aminotransferase |
| AWGS | Asian Working Group for Sarcopenia |
| BIA | bioimpedance analysis |
| BP | bodily pain |
| CHEs | composite hepatic events |
| CI | confidence interval |
| CLDs | chronic liver diseases |
| GH | general health perception |
| GS | grip strength |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| HE | hepatic encephalopathy |
| HR | hazard ratio |
| LC | liver cirrhosis |
| MELD | Model for End-Stage Liver Disease |
| IQR | interquartile range |
| MCS | mental component summary score |
| MH | mental health |
| PCS | physical component summary score |
| PF | physical functioning |
| PT | prothrombin time |
| QOL | quality of life |
| RE | role emotion |
| RP | role physical |
| SF | social functioning |
| SF36 | 36-Item Short-Form Health Survey |
| SMI | skeletal muscle mass index |
| VT | vitality |
References
- Tandon, P.; Raman, M.; Mourtzakis, M.; Merli, M. A practical approach to nutritional screening and assessment in cirrhosis. Hepatology 2017, 65, 1044–1057. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Elevated serum myostatin level is associated with worse survival in patients with liver cirrhosis. J. Cachexia Sarcopenia Muscle 2017, 8, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [PubMed]
- Meyer, F.; Valentini, L. Disease-Related Malnutrition and Sarcopenia as Determinants of Clinical Outcome. Visc. Med. 2019, 35, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Bunchorntavakul, C.; Reddy, K.R. Review article: Malnutrition/sarcopenia and frailty in patients with cirrhosis. Aliment. Pharmacol. Ther. 2020, 51, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Aby, E.S.; Saab, S. Frailty, sarcopenia, and malnutrition in cirrhotic patients. Clin. Liver Dis. 2019, 23, 589–605. [Google Scholar] [CrossRef]
- Hayashi, F.; Matsumoto, Y.; Momoki, C.; Yuikawa, M.; Okada, G.; Hamakawa, E.; Kawamura, E.; Hagihara, A.; Toyama, M.; Fujii, H.; et al. Physical inactivity and insufficient dietary intake are associated with the frequency of sarcopenia in patients with compensated viral liver cirrhosis. Hepatol. Res. 2013, 43, 1264–1275. [Google Scholar] [CrossRef]
- Ohashi, K.; Ishikawa, T.; Hoshi, A.; Suzuki, M.; Mitobe, Y.; Yamada, E.; Abeywickrama, H.M.; Seki, N.; Koyama, C.; Aoki, H.; et al. Relationship between sarcopenia and both physical activity and lifestyle in patients with chronic liver disease. J. Clin. Med. Res. 2018, 10, 920–927. [Google Scholar] [CrossRef]
- Stenholm, S.; Tiainen, K.; Rantanen, T.; Sainio, P.; Heliövaara, M.; Impivaara, O.; Koskinen, S. Long-term determinants of muscle strength decline: Prospective evidence from the 22-year mini-Finland follow-up survey. J. Am. Geriatr. Soc. 2012, 60, 77–85. [Google Scholar] [CrossRef]
- Younossi, Z.M. Patient-reported outcomes and the economic effects of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: The value proposition. Hepatology 2018, 68, 2405–2412. [Google Scholar] [CrossRef]
- Golfieri, L.; Gitto, S.; Morelli, M.C.; Pinna, A.D.; Grandi, S.; Andreone, P. Impact of hepatitis C virus infection on health-related quality of life before and after liver transplantation: A multidisciplinary point of view. Expert Rev. Anti. Infect. Ther. 2017, 15, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Stepanova, M.; Younossi, I.; Pan, C.Q.; Janssen, H.L.A.; Papatheodoridis, G.; Nader, F. Long-term effects of treatment for chronic HBV infection on patient-reported outcomes. Clin. Gastroenterol Hepatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Schramm, C.; Wahl, I.; Weiler-Normann, C.; Voigt, K.; Wiegard, C.; Glaubke, C.; Brähler, E.; Löwe, B.; Lohse, A.W.; Rose, M. Health-related quality of life, depression, and anxiety in patients with autoimmune hepatitis. J. Hepatol. 2014, 60, 618–624. [Google Scholar] [CrossRef]
- Dyson, J.K.; Wilkinson, N.; Jopson, L.; Mells, G.; Bathgate, A.; Heneghan, M.A.; Neuberger, J.; Hirschfield, G.M.; Ducker, S.J.; UK-PBC Consortium; et al. The inter-relationship of symptom severity and quality of life in 2055 patients with primary biliary cholangitis. Aliment. Pharmacol. Ther. 2016, 44, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Health-related quality of life in chronic liver diseases: A strong impact of hand grip strength. J. Clin. Med. 2018, 7, 553. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Duarte-Rojo, A.; Meza-Junco, J.; Baracos, V.E.; Sawyer, M.B.; Pang, J.X.; Beaumont, C.; Esfandiari, N.; Myers, R.P. Inclusion of sarcopenia within MELD (MELD-Sarcopenia) and the prediction of mortality in patients with cirrhosis. Clin. Transl. Gastroenterol. 2015, 6, e102. [Google Scholar] [CrossRef] [PubMed]
- Marty, E.; Liu, Y.; Samuel, A.; Or, O.; Lane, J. A review of sarcopenia: Enhancing awareness of an increasingly prevalent disease. Bone 2017, 105, 276–286. [Google Scholar] [CrossRef]
- Liguori, I.; Russo, G.; Aran, L.; Bulli, G.; Curcio, F.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Sarcopenia: Assessment of disease burden and strategies to improve outcomes. Clin. Interv. Aging 2018, 13, 913–927. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Tse, Y.K.; Yip, T.C.; Lam, K.L.; Lui, G.C.; Wong, V.W. Normal on-treatment ALT during antiviral treatment is associated with a lower risk of hepatic events in patients with chronic hepatitis B. J. Hepatol. 2018, 69, 793–802. [Google Scholar] [CrossRef]
- Bihari, C.; Rastogi, A.; Sen, B.; Bhadoria, A.S.; Maiwall, R.; Sarin, S.K. Quantitative fibrosis estimation by image analysis predicts development of decompensation, composite events and defines event-free survival in chronic hepatitis B patients. Hum. Pathol. 2016, 55, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Bichoupan, K.; Ku, L.; Yalamanchili, R.; Harty, A.; Gardenier, D.; Ng, M.; Motamed, D.; Khaitova, V.; Bach, N.; et al. Hepatic decompensation/serious adverse events in post-liver transplantation recipients on sofosbuvir for recurrent hepatitis C virus. World J. Gastroenterol. 2016, 22, 2844–2854. [Google Scholar] [CrossRef] [PubMed]
- Muto, Y.; Sato, S.; Watanabe, A.; Moriwaki, H.; Suzuki, K.; Kato, A.; Kato, M.; Nakamura, T.; Higuchi, K.; Nishiguchi, S.; et al. Long-Term Survival Study Group. Effects of oral branched-chain amino acid granules on event-free survival in patients with liver cirrhosis. Clin. Gastroenterol. Hepatol. 2005, 3, 705–713. [Google Scholar] [CrossRef]
- Olsson, R.; Boberg, K.M.; de Muckadell, O.S.; Lindgren, S.; Hultcrantz, R.; Folvik, G.; Bell, H.; Gangsøy-Kristiansen, M.; Matre, J.; Rydning, A.; et al. High-dose ursodeoxycholic acid in primary sclerosing cholangitis: A 5-year multicenter, randomized, controlled study. Gastroenterology 2005, 129, 1464–1472. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical practice guidelines for hepatocellular carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef]
- Lanz, J.; Kim, W.K.; Walther, T.; Burgdorf, C.; Möllmann, H.; Linke, A.; Redwood, S.; Thilo, C.; Hilker, M.; Joner, M.; et al. Safety and efficacy of a self-expanding versus a balloon-expandable bioprosthesis for transcatheter aortic valve replacement in patients with symptomatic severe aortic stenosis: A randomised non-inferiority trial. Lancet 2019, 394, 1619–1628. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Iglesias, J.F.; Muller, O.; Heg, D.; Roffi, M.; Kurz, D.J.; Moarof, I.; Weilenmann, D.; Kaiser, C.; Tapponnier, M.; Stortecky, S.; et al. Biodegradable polymer sirolimus-eluting stents versus durable polymer everolimus-eluting stents in patients with ST-segment elevation myocardial infarction (BIOSTEMI): A single-blind, prospective, randomised superiority trial. Lancet 2019, 394, 1243–1253. [Google Scholar] [CrossRef]
- Kudo, M.; Zheng, R.Q.; Kim, S.R.; Okabe, Y.; Osaki, Y.; Iijima, H.; Itani, T.; Kasugai, H.; Kanematsu, M.; Ito, K.; et al. Diagnostic accuracy of imaging for liver cirrhosis compared to histologically proven liver cirrhosis. A multicenter collaborative study. Intervirology 2008, 51, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Zarski, J.P.; Sturm, N.; Guechot, J.; Paris, A.; Zafrani, E.S.; Asselah, T.; Boisson, R.C.; Bosson, J.L.; Guyader, D.; Renversez, J.C.; et al. Comparison of nine blood tests and transient elastography for liver fibrosis in chronic hepatitis C: The ANRS HCEP-23 study. J. Hepatol. 2012, 56, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.A.; Gurusamy, K.S.; Ntaoula, S.; Cholongitas, E.; Davidson, B.R.; Burroughs, A.K. Elastography for the diagnosis of severity of fibrosis in chronic liver disease: A meta-analysis of diagnostic accuracy. J. Hepatol. 2011, 54, 650–659. [Google Scholar] [CrossRef]
- Kumada, H.; Okanoue, T.; Onji, M.; Moriwaki, H.; Izumi, N.; Tanaka, E.; Chayama, K.; Sakisaka, S.; Takehara, T.; Oketani, M.; et al. Guidelines for the treatment of chronic hepatitis and cirrhosis due to hepatitis C virus infection for the fiscal year 2008 in Japan. Hepatol. Res. 2010, 40, 8–13. [Google Scholar] [CrossRef]
- Kappus, M.R.; Mendoza, M.S.; Nguyen, D.; Medici, V.; McClave, S.A. Sarcopenia in Patients with Chronic Liver Disease: Can It Be Altered by Diet and Exercise? Curr. Gastroenterol. Rep. 2016, 18, 43. [Google Scholar] [CrossRef]
- Kokudo, N.; Hasegawa, K.; Akahane, M.; Igaki, H.; Izumi, N.; Ichida, T.; Uemoto, S.; Kaneko, S.; Kawasaki, S.; Ku, Y.; et al. Evidence-based Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2013 update (3rd JSH-HCC Guidelines). Hepatol. Res. 2015. [Google Scholar] [CrossRef]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef]
- Mikdashi, J. Measuring and monitoring health-related quality of life responsiveness in systemic lupus erythematosus patients: Current perspectives. Patient Relat. Outcome Meas. 2018, 9, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Behboodi, M.Z.; Fereidooni, B.; Saffari, M.; Montazeri, A. Measures of health-related quality of life in PCOS women: A systematic review. Int. J. Womens Health. 2018, 10, 397–408. [Google Scholar] [CrossRef]
- Fukuhara, S.; Ware, J.E., Jr.; Kosinski, M.; Wada, S.; Gandek, B. Psychometric and clinical tests of validity of the Japanese SF-36 Health Survey. J. Clin. Epidemiol. 1998, 51, 1045–1053. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramírez-Vélez, R.; Peterson, M.D.; Lobelo, F.; Cavero-Redondo, I.; Correa-Bautista, J.E.; Martínez-Vizcaíno, V. Handgrip and knee extension strength as predictors of cancer mortality: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2018, 28, 1852–1858. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef]
- Cooper, R.; Kuh, D.; Hardy, R. Mortality Review Group; FALCon and HALCyon Study Teams. Objectively measured physical capability levels and mortality: Systematic review and meta-analysis. BMJ 2010, 341, c4467. [Google Scholar]
- Norman, K.; Stobäus, N.; Gonzalez, M.C.; Schulzke, J.D.; Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 2011, 30, 135–142. [Google Scholar] [CrossRef]
- Knudsen, A.W.; Naver, A.; Bisgaard, K.; Nordgaard-Lassen, I.; Becker, U.; Krag, A.; Slinde, F. Nutrition impact symptoms, handgrip strength and nutritional risk in hospitalized patients with gastroenterological and liver diseases. Scand J. Gastroenterol. 2015, 50, 1191–1198. [Google Scholar] [CrossRef]
- Rosenberg, I. Summary comments: Epidemiological and methodological problems in determining nutritional status of older persons. Am. J. Clin. Nutr. 1989, 50, 1231–1233. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number or |
|---|---|
| Median Value (IQR) | |
| Age (years) | 64 (54, 71) |
| Sex, male/female | 199/212 |
| Body mass index (kg/m2) | 22.6 (20.5, 25.5) |
| Liver disease etiology | 258/59/8/86 |
| (HCV/HBV/HCV and HBV/NBNC) | |
| Grip strength (kg, male) | 34.3 (28.65, 41.2) |
| Grip strength (kg, female) | 20.95 (17.5375, 23.875) |
| Presence of LC, yes/no | 160/251 |
| Total bilirubin (mg/dL) | 0.8 (0.6, 1.0) |
| Serum albumin (g/dL) | 4.2 (3.9, 4.5) |
| Prothrombin time (%) | 90.0 (80.2, 98.0) |
| Platelet count (×104/mm3) | 16.6 (11.8, 21.1) |
| SMI (kg/m2, male) | 7.50 (6.97, 7.98) |
| SMI (kg/m2, female) | 5.92 (5.46, 6.46) |
| Physical component summary score | 51.1 (41.6, 54.3) |
| Mental component summary score | 52.3 (44.2, 58.7) |
| AST (IU/L) | 27 (21, 40) |
| ALT (IU/L) | 24 (16, 41) |
| HbA1c (NGSP) | 5.7 (5.4, 6.0) |
| eGFR (ml/min/1.73 m2) | 82 (71, 95) |
| Alpha-fetoprotein (ng/mL) | 3.4 (2.3, 5.8) |
| BTR | 5.64 (4.31, 6.835) |
| Variable | Univariate | Multivariate Analysis | ||
|---|---|---|---|---|
| p Value | HR | 95% CI | p Value | |
| Age ≥64 years | <0.0001 | 1.160 | 0.898–1.497 | 0.2559 |
| Sex | 0.1137 | |||
| Body mass index ≥22.6 kg/m2 | 0.5752 | |||
| GS decrease | 0.0057 | 1.413 | 1.025–1.920 | 0.0350 |
| SMI decrease | 0.0982 | |||
| Total bilirubin ≥0.8 mg/dL | 0.0232 | |||
| Serum albumin ≥4.2 g/dL | <0.0001 | 0.969 | 0.748–1.251 | 0.8081 |
| Prothrombin time ≥90.0% | <0.0001 | 0.740 | 0.564–0.970 | 0.0293 |
| Platelet count ≥16.6 × 104/mm3 | <0.0001 | 0.994 | 0.760–1.299 | 0.9628 |
| PCS ≥51.1 | 0.0318 | |||
| MCS ≥52.3 | 0.7995 | |||
| AST ≥27 IU/L | 0.0008 | 1.190 | 0.934–1.515 | 0.1582 |
| ALT ≥24 IU/L | 0.0494 | |||
| Alpha fetoprotein ≥3.4 ng/mL | 0.1106 | |||
| HbA1c (NGSP) ≥5.7 | 0.0868 | |||
| eGFR ≥82 mL/min/1.73 m2 | 0.3744 | |||
| BTR ≥5.64 | <0.0001 | 0.988 | 0.770–1.271 | 0.9234 |
| Variable | Multivariate Analysis | ||
|---|---|---|---|
| HR | 95% CI | p Value | |
| Age ≥64 years | 1.165 | 0.902–1.504 | 0.2424 |
| GS decrease | 1.304 | 1.006–1.604 | 0.0460 |
| Serum albumin ≥4.2 g/dL | 0.954 | 0.737–1.233 | 0.7208 |
| Prothrombin time ≥90.0% | 0.742 | 0.566–0.973 | 0.0310 |
| Platelet count ≥16.6 × 104/mm3 | 0.999 | 0.766–1.305 | 0.9952 |
| AST ≥27 IU/L | 1.173 | 0.920–1.493 | 0.1972 |
| BTR ≥5.64 | 0.967 | 0.754–1.244 | 0.7946 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoh, K.; Nishikawa, H.; Enomoto, H.; Iwata, Y.; Ikeda, N.; Aizawa, N.; Nishimura, T.; Iijima, H.; Nishiguchi, S. Grip Strength: A Useful Marker for Composite Hepatic Events in Patients with Chronic Liver Diseases. Diagnostics 2020, 10, 238. https://doi.org/10.3390/diagnostics10040238
Yoh K, Nishikawa H, Enomoto H, Iwata Y, Ikeda N, Aizawa N, Nishimura T, Iijima H, Nishiguchi S. Grip Strength: A Useful Marker for Composite Hepatic Events in Patients with Chronic Liver Diseases. Diagnostics. 2020; 10(4):238. https://doi.org/10.3390/diagnostics10040238
Chicago/Turabian StyleYoh, Kazunori, Hiroki Nishikawa, Hirayuki Enomoto, Yoshinori Iwata, Naoto Ikeda, Nobuhiro Aizawa, Takashi Nishimura, Hiroko Iijima, and Shuhei Nishiguchi. 2020. "Grip Strength: A Useful Marker for Composite Hepatic Events in Patients with Chronic Liver Diseases" Diagnostics 10, no. 4: 238. https://doi.org/10.3390/diagnostics10040238
APA StyleYoh, K., Nishikawa, H., Enomoto, H., Iwata, Y., Ikeda, N., Aizawa, N., Nishimura, T., Iijima, H., & Nishiguchi, S. (2020). Grip Strength: A Useful Marker for Composite Hepatic Events in Patients with Chronic Liver Diseases. Diagnostics, 10(4), 238. https://doi.org/10.3390/diagnostics10040238