Simple Stepwise Approach to Differentiate Cyst-Like Soft-Tissue Masses by Using Time-Resolved Magnetic Resonance Angiography

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. MRI Protocol
2.4. Imaging Features
2.5. Histopathology Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Bermejo, A.; De Bustamante, T.D.; Martinez, A.; Carrera, R.; Zabia, E.; Manjon, P. MR imaging in the evaluation of cystic-appearing soft-tissue masses of the extremities. Radiographics 2013, 33, 833–855. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.S.; Hochman, M.G. Soft-tissue tumors and tumorlike lesions: A systematic imaging approach. Radiology 2009, 253, 297–316. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D.M.; Bridge, J.A.; Hogendoorn, P.C.W.; Mertens, F.; World Health Organization; International Agency for Research on Cancer. WHO Classification of Tumours of Soft Tissue and Bone; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Petscavage-Thomas, J.M.; Walker, E.A.; Logie, C.I.; Clarke, L.E.; Duryea, D.M.; Murphey, M.D. Soft-tissue myxomatous lesions: Review of salient imaging features with pathologic comparison. Radiographics 2014, 34, 964–980. [Google Scholar] [CrossRef]
- Murphey, M.D.; Fairbairn, K.J.; Parman, L.M.; Baxter, K.G.; Parsa, M.B.; Smith, W.S. From the archives of the AFIP. Musculoskeletal angiomatous lesions: Radiologic-pathologic correlation. Radiographics 1995, 15, 893–917. [Google Scholar] [CrossRef] [PubMed]
- Olsen, K.I.; Stacy, G.S.; Montag, A. Soft-tissue cavernous hemangioma. Radiographics 2004, 24, 849–854. [Google Scholar] [CrossRef]
- Kaplan, P.A.; Williams, S.M. Mucocutaneous and peripheral soft-tissue hemangiomas: MR imaging. Radiology 1987, 163, 163–166. [Google Scholar] [CrossRef]
- Ma, L.D.; McCarthy, E.F.; Bluemke, D.A.; Frassica, F.J. Differentiation of benign from malignant musculoskeletal lesions using MR imaging: Pitfalls in MR evaluation of lesions with a cystic appearance. AJR Am. J. Roentgenol. 1998, 170, 1251–1258. [Google Scholar] [CrossRef]
- Paltiel, H.J.; Burrows, P.E.; Kozakewich, H.P.; Zurakowski, D.; Mulliken, J.B. Soft-tissue vascular anomalies: Utility of US for diagnosis. Radiology 2000, 214, 747–754. [Google Scholar] [CrossRef]
- Robinson, J.L.; Learch, T.J. Vascular lesions presenting as musculoskeletal neoplasms. AJR Am. J. Roentgenol. 2011, 197, W141–W148. [Google Scholar] [CrossRef]
- Bartley, O.; Wickbom, I. Angiography in Soft Tissue Hemangiomas. Acta Radiol. 1959, 51, 81–94. [Google Scholar] [CrossRef]
- Lois, J.F.; Fischer, H.J.; Deutsch, L.S.; Stambuk, E.C.; Gomes, A.S. Angiography in soft tissue sarcomas. Cardiovasc. Interv. Radiol. 1984, 7, 309–316. [Google Scholar] [CrossRef]
- Korosec, F.R.; Frayne, R.; Grist, T.M.; Mistretta, C.A. Time-resolved contrast-enhanced 3D MR angiography. Magn. Reson. Med. 1996, 36, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Flors, L.; Leiva-Salinas, C.; Maged, I.M.; Norton, P.T.; Matsumoto, A.H.; Angle, J.F.; Hugo Bonatti, M.; Park, A.W.; Ahmad, E.A.; Bozlar, U.; et al. MR imaging of soft-tissue vascular malformations: Diagnosis, classification, and therapy follow-up. Radiographics 2011, 31, 1321–1340. [Google Scholar] [CrossRef] [PubMed]
- Fayad, L.M.; Mugera, C.; Soldatos, T.; Flammang, A.; del Grande, F. Technical innovation in dynamic contrast-enhanced magnetic resonance imaging of musculoskeletal tumors: An MR angiographic sequence using a sparse k-space sampling strategy. Skelet. Radiol. 2013, 42, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Mell, M.; Tefera, G.; Thornton, F.; Siepman, D.; Turnipseed, W. Clinical utility of time-resolved imaging of contrast kinetics (TRICKS) magnetic resonance angiography for infrageniculate arterial occlusive disease. J. Vasc. Surg. 2007, 45, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Jin, T.; Wu, G.; Li, X.; Feng, X. Evaluation of vascular invasion in patients with musculoskeletal tumors of lower extremities: Use of time-resolved 3D MR angiography at 3-T. Acta Radiol. 2018, 59, 586–592. [Google Scholar] [CrossRef]
- Lin, Y.C.; Chuang, W.Y.; Hu, C.H.; Cheung, Y.C.; Ng, S.H.; Lin, G.; Juan, Y.H. Ulnar arterial epithelioid hemangioma: A unique demonstration using time-resolved MR angiography. Int. J. Cardiol. 2016, 223, 18–20. [Google Scholar] [CrossRef]
- Kramer, U.; Ernemann, U.; Fenchel, M.; Seeger, A.; Laub, G.; Claussen, C.D.; Miller, S. Pretreatment evaluation of peripheral vascular malformations using low-dose contrast-enhanced time-resolved 3D MR angiography: Initial results in 22 patients. AJR Am. J. Roentgenol. 2011, 196, 702–711. [Google Scholar] [CrossRef]
- Teo, E.L.; Strouse, P.J.; Hernandez, R.J. MR imaging differentiation of soft-tissue hemangiomas from malignant soft-tissue masses. AJR Am. J. Roentgenol. 2000, 174, 1623–1628. [Google Scholar] [CrossRef]
- Suh, J.S.; Hwang, G.; Hahn, S.B. Soft tissue hemangiomas: MR manifestations in 23 patients. Skelet. Radiol. 1994, 23, 621–625. [Google Scholar] [CrossRef]
- Buetow, P.C.; Kransdorf, M.J.; Moser, R.P., Jr.; Jelinek, J.S.; Berrey, B.H. Radiologic appearance of intramuscular hemangioma with emphasis on MR imaging. AJR Am. J. Roentgenol. 1990, 154, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Allen, P.W.; Enzinger, F.M. Hemangioma of skeletal muscle. An analysis of 89 cases. Cancer 1972, 29, 8–22. [Google Scholar] [CrossRef]
- Kim, J.S.; Chandler, A.; Borzykowski, R.; Thornhill, B.; Taragin, B.H. Maximizing time-resolved MRA for differentiation of hemangiomas, vascular malformations and vascularized tumors. Pediatr. Radiol. 2012, 42, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Navarro, O.M.; Laffan, E.E.; Ngan, B.Y. Pediatric soft-tissue tumors and pseudo-tumors: MR imaging features with pathologic correlation: part 1. Imaging approach, pseudotumors, vascular lesions, and adipocytic tumors. Radiographics 2009, 29, 887–906. [Google Scholar] [CrossRef] [PubMed]
- Gaballah, A.H.; Jensen, C.T.; Palmquist, S.; Pickhardt, P.J.; Duran, A.; Broering, G.; Elsayes, K.M. Angiosarcoma: clinical and imaging features from head to toe. Br. J. Radiol. 2017, 90, 20170039. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histologic Diagnosis | Number of Cases |
|---|---|
| Vascular lesion | - |
| Hemangioma | 20 |
| Lymphatic malformation | 2 |
| Benign solid lesion | - |
| Benign peripheral nerve sheath tumor | 12 |
| Glomus tumor/myopericytoma | 8 |
| Tenosynovial giant cell tumor | 1 |
| Fibromatosis | 1 |
| Malignant solid lesion | - |
| Infantile fibrosarcoma | 1 |
| Myxofibrosarcoma | 6 |
| Malignant giant cell tumor | 1 |
| Malignant peripheral nerve sheath tumor | 2 |
| Undifferentiated pleomorphic sarcoma | 1 |
| Squamous cell carcinoma | 1 |
| Sarcoma of uncertain differentiation | 2 |
| Myxoid liposarcoma | 2 |
| True cyst | - |
| Ganglion/synovial cyst | 10 |
| Abscess | 6 |
| Epidermoid cyst | 2 |
| Hematoma | 2 |
| Imaging Feature | Vascular Lesion (n = 22) | Solid Lesion (n = 38) | True Cyst (n = 20) | p Value |
|---|---|---|---|---|
| Size (cm) | 0.32 | |||
| Median | 2.9 | 3.0 | 3.9 | |
| Range | 0.7–10.8 | 0.3–17.2 | 0.7–10.3 | |
| T1 hyperintensity | 0.77 | |||
| Absence | 9 | 19 | 10 | |
| Presence | 13 | 19 | 10 | |
| T2 composition | 0.01 * | |||
| Homogeneous | 1 | 11 | 9 | |
| Heterogeneous | 21 | 27 | 11 | |
| Perilesional edema | 0.10 | |||
| Absence | 16 | 20 | 8 | |
| Presence | 6 | 18 | 12 | |
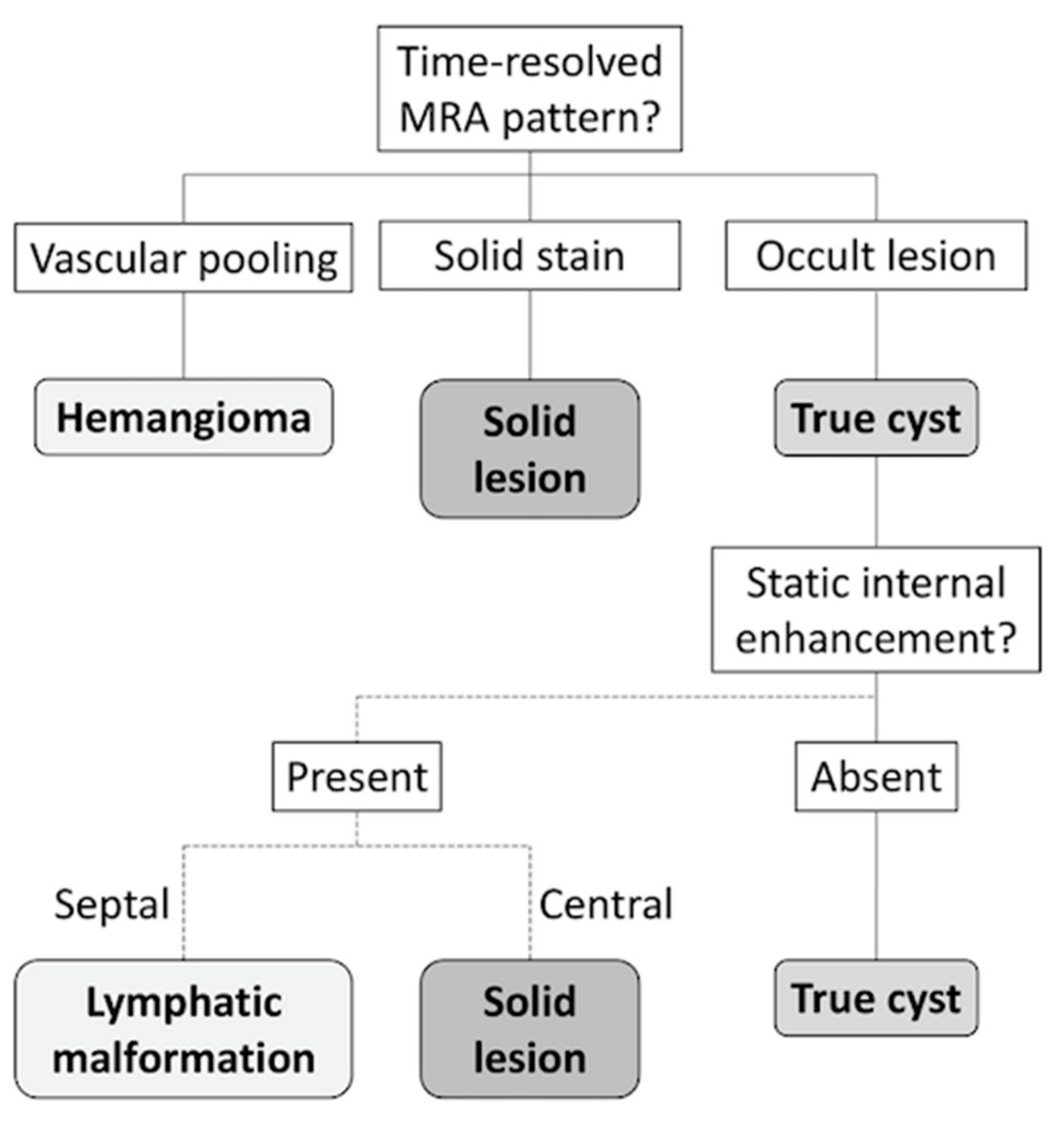
| Time-resolved MRA | <0.001 * | |||
| Vascular pooling | 19 † | 1 | 0 | |
| Solid stain | 1 | 31 | 7 | |
| Occult lesion | 2 | 6 | 13 | |
| Static enhancement | <0.001 * | |||
| Marked | 15 | 28 | 2 | |
| Mild–moderate | 6 ‡ | 10 | 3 | |
| Absent | 1 | 0 | 15 |
| Vascular Lesion | Solid Lesion | True Cyst | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value |
| Size (cm) | 1.0 | 0.8–1.2 | 0.984 | 0.9 | 0.8–1.1 | 0.488 | 1.1 | 0.9–1.3 | 0.437 |
| T1 hyperintensity | 1.4 | 0.5–3.9 | 0.468 | 0.8 | 0.3–2.0 | 0.670 | 0.9 | 0.3–2.4 | 0.796 |
| T2 heterogeneous | 1.7 | 0.9–3.3 | 0.100 | 0.8 | 0.5–1.5 | 0.550 | 0.7 | 0.4–1.3 | 0.305 |
| Perilesional edema | 0.4 | 0.1–1.0 | 0.055 | 1.2 | 0.5–2.9 | 0.686 | 2.2 | 2.2–6.3 | 0.124 |
| Time-resolved MRA | |||||||||
| Vascular pooling | 722.0 | 42.8 to >999.9 | <0.001 * | Ref | <0.1 | <0.1–0.0 | 0.998 | ||
| Solid stain | Ref | 73.6 | 8.5–635.8 | <0.001 * | Ref | ||||
| Occult lesion | 4.0 | 0.3–47.0 | 0.270 | 7.6 | 0.8–70.2 | 0.074 | 7.4 | 2.2–24.7 | 0.001 * |
| Static enhancement | |||||||||
| Marked | 7.5 | 0.9–62.3 | 0.062 | Ref | 0.2 | <0.1–1.6 | 0.146 | ||
| Mild–moderate | 6.9 | 0.7–65.3 | 0.091 | 0.7 | 0.2–2.0 | 0.476 | Ref | ||
| Absent | Ref | <0.1 | <0.1–0.0 | 0.998 | 80.0 | 7.5–856.0 | <0.001 ** |
| Type of Mass/Imaging Feature | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) |
|---|---|---|---|---|---|
| Vascular lesion | |||||
| Vascular pooling on MRA | 86 (65–97; 19/22) | 98 (91–100; 57/58) | 95 (75–100; 57/60) | 95 (86–99; 19/20) | 95 (88–99; 76/80) |
| Marked enhancement | 68 (45–86; 15/22) | 48 (35–62; 28/58) | 33 (20–49; 15/45) | 80 (63–92; 28/35) | 54 (42–65; 43/80) |
| Solid lesion | |||||
| Solid stain on MRA | 82 (66–92; 31/38) | 81 (66–91; 34/42) | 79 (64–91; 31/39) | 83 (68–93; 34/41) | 81 (71–89; 65/80) |
| Mild–moderate enhancement | 26 (13–43; 10/38) | 79 (63–90; 33/42) | 53 (29–76; 10/19) | 54 (41–67; 33/61) | 54 (42–65; 43/80) |
| True cyst | |||||
| Occult lesion on MRA | 65 (41–85; 13/20) | 87 (75–94; 52/60) | 62 (38–82; 13/21) | 88 (77–95; 52/59) | 81 (71–89; 65/80) |
| Absent enhancement | 75 (51–91; 15/20) | 98 (91–100; 59/60) | 94 (70–100; 15/16) | 92 (83–97; 59/64) | 93 (84–97; 74/80) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-C.; Juan, Y.-H.; Ng, S.-H.; Lo, T.-C.; Chuang, W.-Y.; Chen, C.-C.; Liau, C.-T.; Lin, G.; Lin, Y.-J.; Lin, Y.-C. Simple Stepwise Approach to Differentiate Cyst-Like Soft-Tissue Masses by Using Time-Resolved Magnetic Resonance Angiography. Diagnostics 2020, 10, 1094. https://doi.org/10.3390/diagnostics10121094
Lai Y-C, Juan Y-H, Ng S-H, Lo T-C, Chuang W-Y, Chen C-C, Liau C-T, Lin G, Lin Y-J, Lin Y-C. Simple Stepwise Approach to Differentiate Cyst-Like Soft-Tissue Masses by Using Time-Resolved Magnetic Resonance Angiography. Diagnostics. 2020; 10(12):1094. https://doi.org/10.3390/diagnostics10121094
Chicago/Turabian StyleLai, Ying-Chieh, Yu-Hsiang Juan, Shu-Hang Ng, Tzu-Chin Lo, Wen-Yu Chuang, Chun-Chieh Chen, Chi-Ting Liau, Gigin Lin, Yu-Jr Lin, and Yu-Ching Lin. 2020. "Simple Stepwise Approach to Differentiate Cyst-Like Soft-Tissue Masses by Using Time-Resolved Magnetic Resonance Angiography" Diagnostics 10, no. 12: 1094. https://doi.org/10.3390/diagnostics10121094
APA StyleLai, Y.-C., Juan, Y.-H., Ng, S.-H., Lo, T.-C., Chuang, W.-Y., Chen, C.-C., Liau, C.-T., Lin, G., Lin, Y.-J., & Lin, Y.-C. (2020). Simple Stepwise Approach to Differentiate Cyst-Like Soft-Tissue Masses by Using Time-Resolved Magnetic Resonance Angiography. Diagnostics, 10(12), 1094. https://doi.org/10.3390/diagnostics10121094