Endoscopic Ultrasonography Findings of Early and Suspected Early Chronic Pancreatitis

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
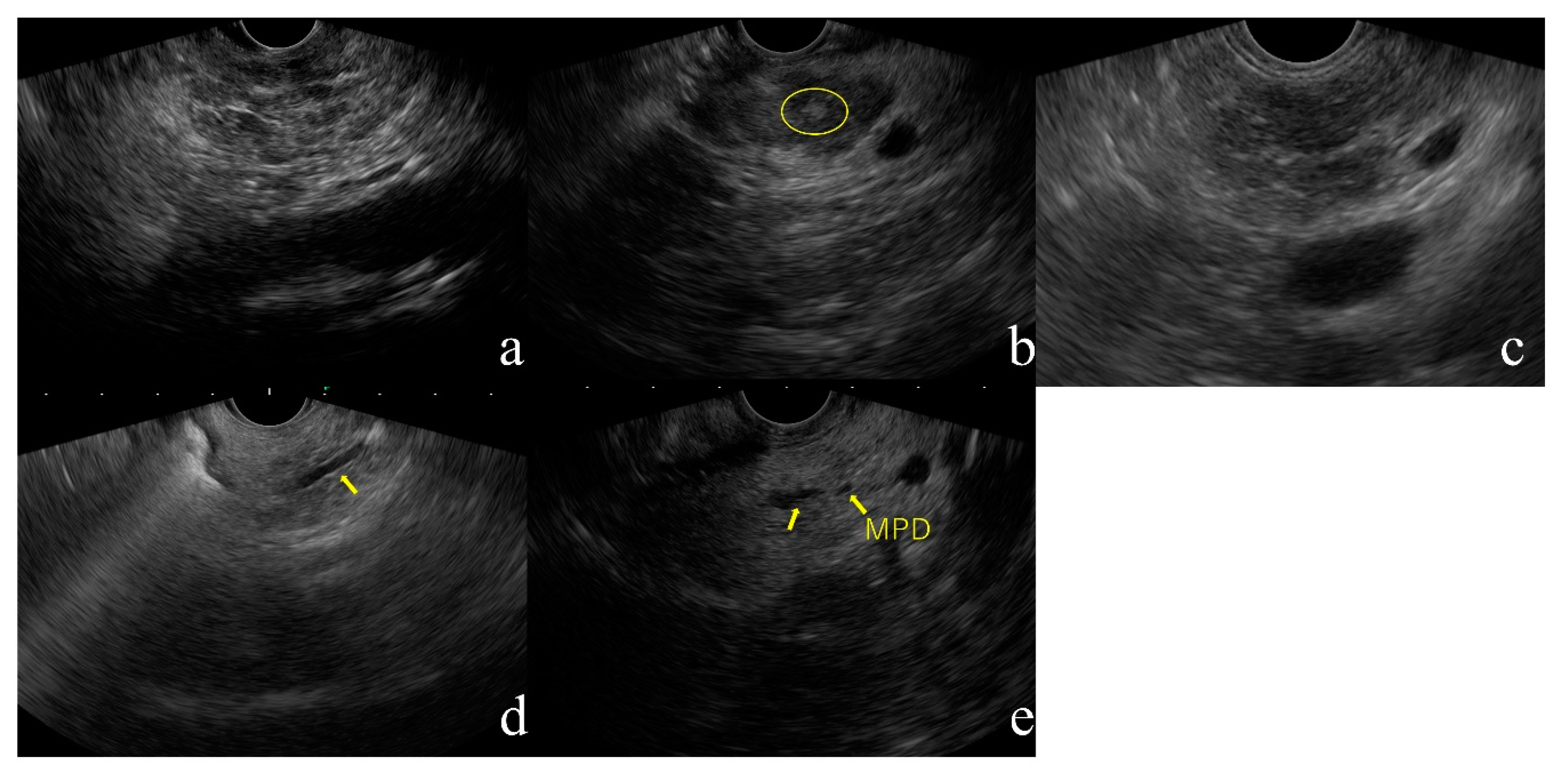
2.1. EUS Findings of Early CP
- 1.
- Lobularity (Figure 1a)
- 2.
- Hyperechoic foci without shadowing (Figure 1b)
- 3.
- Strands (Figure 1c)
- 4.
- Hyperechoic MPD margin (Figure 1d)
- 5.
- Dilated side branches (Figure 1e)
2.2. Definition and Assessment of Early CP
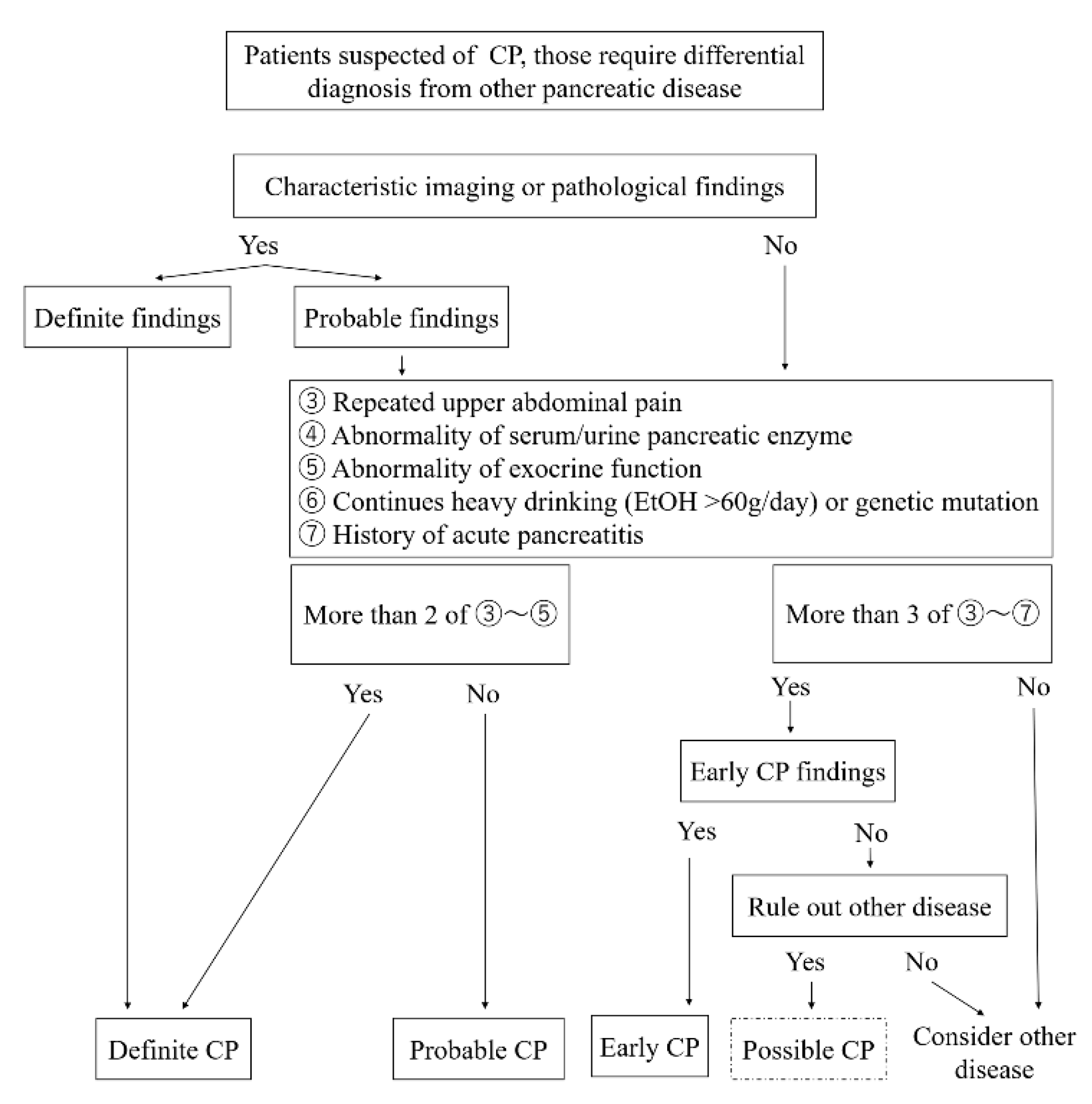
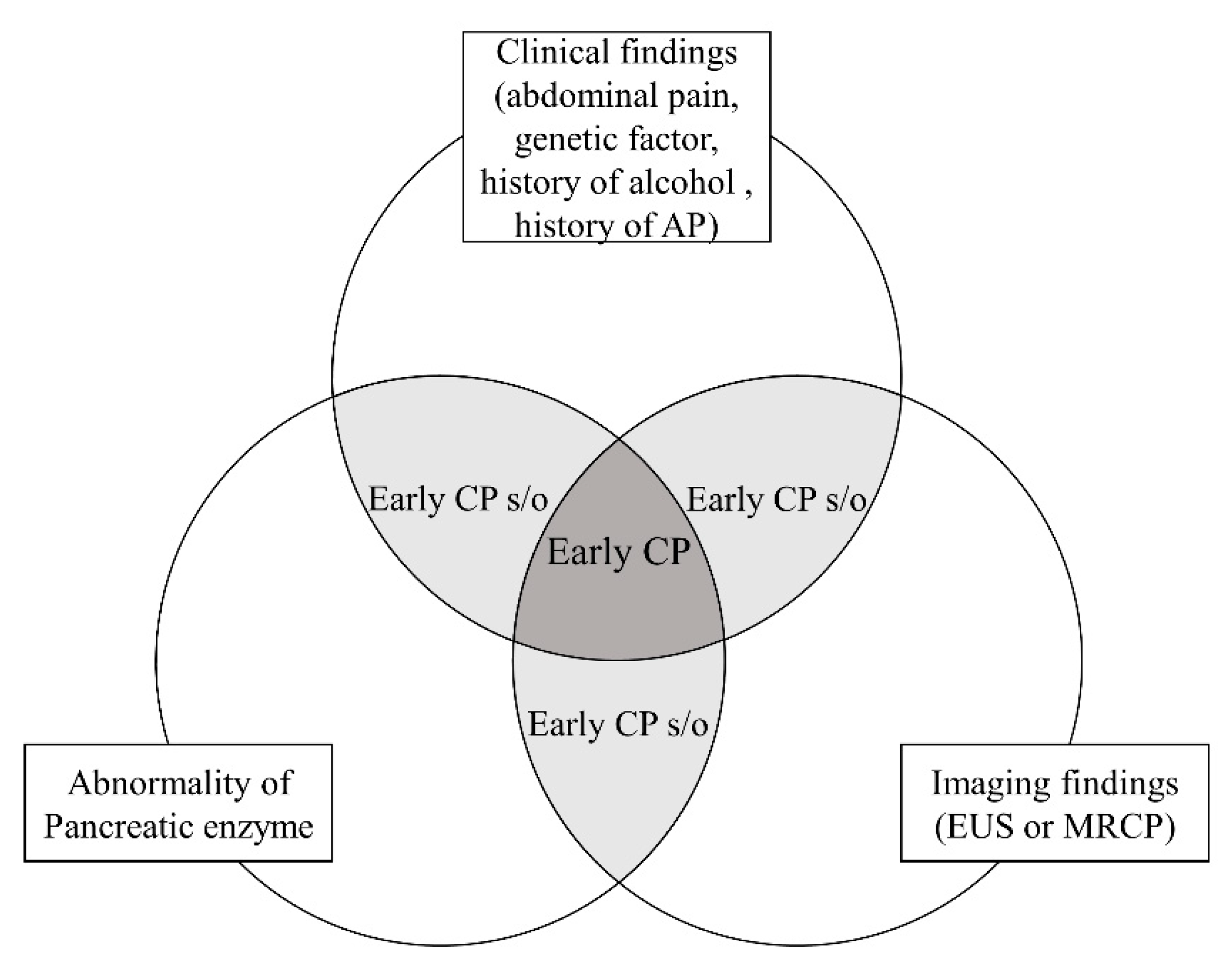
2.3. Japanese Diagnostic Criteria for Early CP
2.4. Limitations of the Diagnostic Criteria for Early CP
2.5. EUS-Elastography
2.6. The Future of Diagnosis in Early CP
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Phillips, A.E.; Faghih, M.; Kuhlmann, L.; Larsen, I.M.; Drewes, A.M.; Singh, V.K.; Yadav, D.; Olesen, S.S.; Pancreatic Quantitative Sensory Testing (P-QST) Consortium. A clinically feasible method for the assessment and characterization of pain in patients with chronic pancreatitis. Pancreatology 2020, 20, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Drewes, A.M.; Bouwense, S.A.W.; Campbell, C.M.; Ceyhan, G.O.; Delhaye, M.; Demir, I.E.; Garg, P.K.; van Goor, H.; Halloran, C.; Isaji, S.; et al. Guidelines for the understanding and management of pain in chronic pancreatitis. Pancreatology 2017, 17, 720–731. [Google Scholar] [CrossRef]
- Machicado, J.D.; Amann, S.T.; Anderson, M.A.; Abberbock, J.; Sherman, S.; Conwell, D.L.; Cote, G.A.; Singh, V.K.; Lewis, M.D.; Alkaade, S.; et al. Quality of Life in Chronic Pancreatitis is Determined by Constant Pain, Disability/Unemployment, Current Smoking, and Associated Co-Morbidities. Am. J. Gastroenterol. 2017, 112, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Talamini, G.; Falconi, M.; Bassi, C.; Sartori, N.; Salvia, R.; Caldiron, E.; Frulloni, L.; Di Francesco, V.; Vaona, B.; Bovo, P.; et al. Incidence of cancer in the course of chronic pancreatitis. Am. J. Gastroenterol. 1999, 94, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Malka, D.; Hammel, P.; Maire, F.; Rufat, P.; Madeira, I.; Pessione, F.; Levy, P.; Ruszniewski, P. Risk of pancreatic adenocarcinoma in chronic pancreatitis. Gut 2002, 51, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Bang, U.C.; Benfield, T.; Hyldstrup, L.; Bendtsen, F.; Beck Jensen, J.E. Mortality, cancer, and comorbidities associated with chronic pancreatitis: A Danish nationwide matched-cohort study. Gastroenterology 2014, 146, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Shimosegawa, T.; Kataoka, K.; Kamisawa, T.; Miyakawa, H.; Ohara, H.; Ito, T.; Naruse, S.; Sata, N.; Suda, K.; Hirota, M.; et al. The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J. Gastroenterol. 2010, 45, 584–591. [Google Scholar] [CrossRef]
- Axon, A.T.; Classen, M.; Cotton, P.B.; Cremer, M.; Freeny, P.C.; Lees, W.R. Pancreatography in chronic pancreatitis: International definitions. Gut 1984, 25, 1107–1112. [Google Scholar] [CrossRef]
- Frokjaer, J.B.; Akisik, F.; Farooq, A.; Akpinar, B.; Dasyam, A.; Drewes, A.M.; Haldorsen, I.S.; Morana, G.; Neoptolemos, J.P.; Olesen, S.S.; et al. Guidelines for the Diagnostic Cross Sectional Imaging and Severity Scoring of Chronic Pancreatitis. Pancreatology 2018, 18, 764–773. [Google Scholar] [CrossRef]
- Yoshida, T.; Yamashita, Y.; Kitano, M. Endoscopic Ultrasound for Early Diagnosis of Pancreatic Cancer. Diagnostics 2019, 9, 81. [Google Scholar] [CrossRef]
- Dominguez-Munoz, J.E.; Drewes, A.M.; Lindkvist, B.; Ewald, N.; Czakó, L.; Rosendahl, J.; Löhr, J.M.; Löhr, M.; Besselink, M.; Mayerle, J.; et al. Recommendations from the United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis. Pancreatology 2018, 18, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Raimondo, M.; Wallace, M.B. Diagnosis of early chronic pancreatitis by endoscopic ultrasound. Are we there yet? JOP 2004, 5, 1–7. [Google Scholar] [PubMed]
- Catalano, M.F.; Sahai, A.; Levy, M.; Romagnuolo, J.; Wiersema, M.; Brugge, W.; Freeman, M.; Yamao, K.; Canto, M.; Hernandez, L.V. EUS-based criteria for the diagnosis of chronic pancreatitis: The Rosemont classification. Gastrointest. Endosc. 2009, 69, 1251–1261. [Google Scholar] [CrossRef]
- Dancygier, H. Endoscopic ultrasonography in chronic pancreatitis. Gastrointest. Endosc. Clin. N. Am. 1995, 5, 795–804. [Google Scholar] [CrossRef]
- Catalano, M.F.; Geenen, J.E. Diagnosis of chronic pancreatitis by endoscopic ultrasonography. Endoscopy 1998, 30 (Suppl. 1), A111–A115. [Google Scholar] [CrossRef]
- Sahai, A.V.; Zimmerman, M.; Aabakken, L.; Tarnasky, P.R.; Cunningham, J.T.; van Velse, A.; Hawes, R.H.; Hoffman, B.J. Prospective assessment of the ability of endoscopic ultrasound to diagnose, exclude, or establish the severity of chronic pancreatitis found by endoscopic retrograde cholangiopancreatography. Gastrointest. Endosc. 1998, 48, 18–25. [Google Scholar] [CrossRef]
- Catalano, M.F.; Lahoti, S.; Geenen, J.E.; Hogan, W.J. Prospective evaluation of endoscopic ultrasonography, endoscopic retrograde pancreatography, and secretin test in the diagnosis of chronic pancreatitis. Gastrointest. Endosc. 1998, 48, 11–17. [Google Scholar] [CrossRef]
- Irisawa, A.; Mishra, G.; Hernandez, L.V.; Bhutani, M.S. Quantitative analysis of endosonographic parenchymal echogenicity in patients with chronic pancreatitis. J. Gastroenterol. Hepatol. 2004, 19, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Irisawa, A.; Katakura, K.; Ohira, H.; Sato, A.; Bhutani, M.S.; Hernandez, L.V.; Koizumi, M. Usefulness of endoscopic ultrasound to diagnose the severity of chronic pancreatitis. J. Gastroenterol. 2007, 42 (Suppl. 17), 90–94. [Google Scholar] [CrossRef]
- Dominguez-Munoz, J.E.; Alvarez-Castro, A.; Larino-Noia, J.; Nieto, L.; Iglesias-Garcia, J. Endoscopic ultrasonography of the pancreas as an indirect method to predict pancreatic exocrine insufficiency in patients with chronic pancreatitis. Pancreas 2012, 41, 724–728. [Google Scholar] [CrossRef]
- Sato, A.; Irisawa, A.; Bhutani, M.S.; Shibukawa, G.; Yamabe, A.; Fujisawa, M.; Igarashi, R.; Arakawa, N.; Yoshida, Y.; Abe, Y.; et al. Significance of normal appearance on endoscopic ultrasonography in the diagnosis of early chronic pancreatitis. Endosc. Ultrasound 2018, 7, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Albashir, S.; Bronner, M.P.; Parsi, M.A.; Walsh, R.M.; Stevens, T. Endoscopic ultrasound, secretin endoscopic pancreatic function test, and histology: Correlation in chronic pancreatitis. Am. J. Gastroenterol. 2010, 105, 2498–2503. [Google Scholar] [CrossRef] [PubMed]
- Varadarajulu, S.; Eltoum, I.; Tamhane, A.; Eloubeidi, M.A. Histopathologic correlates of noncalcific chronic pancreatitis by EUS: A prospective tissue characterization study. Gastrointest. Endosc. 2007, 66, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Rajan, E.; Clain, J.E.; Levy, M.J.; Norton, I.D.; Wang, K.K.; Wiersema, M.J.; Vazquez-Sequeiros, E.; Nelson, B.J.; Jondal, M.L.; Kendall, R.K.; et al. Age-related changes in the pancreas identified by EUS: A prospective evaluation. Gastrointest. Endosc. 2005, 61, 401–406. [Google Scholar] [CrossRef]
- Ammann, R.W.; Heitz, P.U.; Kloppel, G. Course of alcoholic chronic pancreatitis: A prospective clinicomorphological long-term study. Gastroenterology 1996, 111, 224–231. [Google Scholar] [CrossRef]
- Conwell, D.L.; Lee, L.S.; Yadav, D.; Longnecker, D.S.; Miller, F.H.; Mortele, K.J.; Levy, M.J.; Kwon, R.; Lieb, J.G.; Stevens, T.; et al. American Pancreatic Association Practice Guidelines in Chronic Pancreatitis: Evidence-based report on diagnostic guidelines. Pancreas 2014, 43, 1143–1162. [Google Scholar] [CrossRef]
- Lohr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Haas, S.; Akisik, F.; Kartalis, N.; Iglesias-Garcia, J.; et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United Eur. Gastroenterol. J. 2017, 5, 153–199. [Google Scholar] [CrossRef]
- Whitcomb, D.C.; Frulloni, L.; Garg, P.; Greer, J.B.; Schneider, A.; Yadav, D.; Shimosegawa, T. Chronic pancreatitis: An international draft consensus proposal for a new mechanistic definition. Pancreatology 2016, 16, 218–224. [Google Scholar] [CrossRef]
- Whitcomb, D.C.; Shimosegawa, T.; Chari, S.T.; Forsmark, C.E.; Frulloni, L.; Garg, P.; Hegyi, P.; Hirooka, Y.; Irisawa, A.; Ishikawa, T.; et al. International consensus statements on early chronic Pancreatitis. Recommendations from the working group for the international consensus guidelines for chronic pancreatitis in collaboration with The International Association of Pancreatology, American Pancreatic Association, Japan Pancreas Society, PancreasFest Working Group and European Pancreatic Club. Pancreatology 2018. [Google Scholar] [CrossRef]
- Masamune, A.; Nabeshima, T.; Kikuta, K.; Hamada, S.; Nakano, E.; Kume, K.; Kanno, A.; Sato, A.; Tachibana, Y.; Inatomi, O.; et al. Prospective study of early chronic pancreatitis diagnosed based on the Japanese diagnostic criteria. J. Gastroenterol. 2019, 54, 928–935. [Google Scholar] [CrossRef]
- Hashimoto, S.; Futagami, S.; Yamawaki, H.; Kaneko, K.; Kodaka, Y.; Wakabayashi, M.; Sakasegawa, N.; Agawa, S.; Higuchi, K.; Akimoto, T.; et al. Epigastric pain syndrome accompanying pancreatic enzyme abnormalities was overlapped with early chronic pancreatitis using endosonography. J. Clin. Biochem. Nutr. 2017, 61, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Yamawaki, H.; Futagami, S.; Kaneko, K.; Agawa, S.; Higuchi, K.; Murakami, M.; Wakabayashi, M.; Sakasegawa, N.; Kodaka, Y.; Ueki, N.; et al. Camostat Mesilate, Pancrelipase, and Rabeprazole Combination Therapy Improves Epigastric Pain in Early Chronic Pancreatitis and Functional Dyspepsia with Pancreatic Enzyme Abnormalities. Digestion 2019, 99, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Sheel, A.R.G.; Baron, R.D.; Sarantitis, I.; Ramesh, J.; Ghaneh, P.; Raraty, M.G.T.; Yip, V.; Sutton, R.; Goulden, M.R.; Campbell, F.; et al. The diagnostic value of Rosemont and Japanese diagnostic criteria for ‘indeterminate’, ‘suggestive’, ‘possible’ and ‘early’ chronic pancreatitis. Pancreatology 2018, 18, 774–784. [Google Scholar] [CrossRef] [PubMed]
- Masamune, A.; Irisawa, A.; Kikuda, K.; Ikeura, T.; Isaji, S.; Ishiguro, Y.; Itoi, T.; Ito, T.; Inui, K.; Ohara, H.; et al. Clinical Diagnostic Criteria for Chronic Pancreatitis 2019. Suizo 2019, 34, 279–281. (In Japanese) [Google Scholar] [CrossRef]
- Zou, W.B.; Tang, X.Y.; Zhou, D.Z.; Qian, Y.Y.; Hu, L.H.; Yu, F.F.; Yu, D.; Wu, H.; Deng, S.J.; Lin, J.H.; et al. SPINK1, PRSS1, CTRC, and CFTR Genotypes Influence Disease Onset and Clinical Outcomes in Chronic Pancreatitis. Clin. Transl. Gastroenterol. 2018, 9, 204. [Google Scholar] [CrossRef]
- Tang, X.Y.; Zou, W.B.; Yu, F.F.; Wang, L.; Ru, N.; Zhu, J.H.; Li, Z.S.; Liao, Z. Meta-analysis of the impact of the SPINK1 c.194+2T>C variant in chronic pancreatitis. Dig. Liver Dis. 2020, 52, 143–148. [Google Scholar] [CrossRef]
- Sisman, G.; Tugcu, M.; Ayla, K.; Sebati, O.; Senturk, H. Mutation analysis of PRSS1, SPINK1 and CFTR gene in patients with alcoholic and idiopathic chronic pancreatitis: A single center study. Turk. J. Gastroenterol. 2015, 26, 176–180. [Google Scholar] [CrossRef]
- Masamune, A.; Kikuta, K.; Hamada, S.; Nakano, E.; Kume, K.; Inui, A.; Shimizu, T.; Takeyama, Y.; Nio, M.; Shimosegawa, T. Nationwide survey of hereditary pancreatitis in Japan. J. Gastroenterol. 2018, 53, 152–160. [Google Scholar] [CrossRef]
- Kumar, S.; Ooi, C.Y.; Werlin, S.; Abu-El-Haija, M.; Barth, B.; Bellin, M.D.; Durie, P.R.; Fishman, D.S.; Freedman, S.D.; Gariepy, C.; et al. Risk Factors Associated With Pediatric Acute Recurrent and Chronic Pancreatitis: Lessons From INSPPIRE. JAMA Pediatr. 2016, 170, 562–569. [Google Scholar] [CrossRef]
- Giefer, M.J.; Lowe, M.E.; Werlin, S.L.; Zimmerman, B.; Wilschanski, M.; Troendle, D.; Schwarzenberg, S.J.; Pohl, J.F.; Palermo, J.; Ooi, C.Y.; et al. Early-Onset Acute Recurrent and Chronic Pancreatitis Is Associated with PRSS1 or CTRC Gene Mutations. J. Pediatr. 2017, 186, 95–100. [Google Scholar] [CrossRef]
- Ito, T.; Ikeura, T.; Tanaka, T.; Mitsuyama, T.; Miyoshi, H.; Shimatani, M.; Uchida, K.; Takaoka, M.; Okazaki, K. Magnetic resonance cholangiopancreatography findings in early chronic pancreatitis diagnosed according to the Japanese Diagnostic Criteria. Pancreatology 2020, 20, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Gardner, T.B.; Gordon, S.R. Interobserver agreement for pancreatic endoscopic ultrasonography determined by same day back-to-back examinations. J. Clin. Gastroenterol. 2011, 45, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Stevens, T.; Lopez, R.; Adler, D.G.; Al-Haddad, M.A.; Conway, J.; Dewitt, J.M.; Forsmark, C.E.; Kahaleh, M.; Lee, L.S.; Levy, M.J.; et al. Multicenter comparison of the interobserver agreement of standard EUS scoring and Rosemont classification scoring for diagnosis of chronic pancreatitis. Gastrointest. Endosc. 2010, 71, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.J.; Lakhtakia, S.; Kida, M.; Lesmana, C.R.A.; Ang, T.L.; Vu, C.K.F.; Aye, T.T.; Park, S.H.; Almadi, M.A.; Chong, C.C.; et al. Defining the endoscopic ultrasound features of chronic pancreatitis in Asians: A multicenter validation study. Endoscopy 2020. [Google Scholar] [CrossRef] [PubMed]
- Costache, M.I.; Dumitrescu, D.; Saftoiu, A. Technique of qualitative and semiquantitative EUS elastography in pancreatic examination. Endosc. Ultrasound 2017, 6, S111–S114. [Google Scholar] [CrossRef]
- Janssen, J.; Papavassiliou, I. Effect of aging and diffuse chronic pancreatitis on pancreas elasticity evaluated using semiquantitative EUS elastography. Ultraschall Med. 2014, 35, 253–258. [Google Scholar] [CrossRef]
- Dominguez-Munoz, J.E.; Iglesias-Garcia, J.; Castineira Alvarino, M.; Luaces Regueira, M.; Larino-Noia, J. EUS elastography to predict pancreatic exocrine insufficiency in patients with chronic pancreatitis. Gastrointest. Endosc. 2015, 81, 136–142. [Google Scholar] [CrossRef]
- Dominguez-Munoz, J.E. Predicting Pancreatic Exocrine Insufficiency with EUS Elastography. Gastroenterol. Hepatol. 2016, 12, 511–512. [Google Scholar]
- Kim, S.Y.; Cho, J.H.; Kim, Y.J.; Kim, E.J.; Park, J.Y.; Jeon, T.J.; Kim, Y.S. Diagnostic efficacy of quantitative endoscopic ultrasound elastography for differentiating pancreatic disease. J. Gastroenterol. Hepatol. 2017, 32, 1115–1122. [Google Scholar] [CrossRef]
- Kuwahara, T.; Hirooka, Y.; Kawashima, H.; Ohno, E.; Ishikawa, T.; Kawai, M.; Suhara, H.; Takeyama, T.; Hashizume, K.; Koya, T.; et al. Quantitative diagnosis of chronic pancreatitis using EUS elastography. J. Gastroenterol. 2017, 52, 868–874. [Google Scholar] [CrossRef]
- Yashima, Y.; Sasahira, N.; Isayama, H.; Kogure, H.; Ikeda, H.; Hirano, K.; Mizuno, S.; Yagioka, H.; Kawakubo, K.; Sasaki, T.; et al. Acoustic radiation force impulse elastography for noninvasive assessment of chronic pancreatitis. J. Gastroenterol. 2012, 47, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Goertz, R.S.; Schuderer, J.; Strobel, D.; Pfeifer, L.; Neurath, M.F.; Wildner, D. Acoustic radiation force impulse shear wave elastography (ARFI) of acute and chronic pancreatitis and pancreatic tumor. Eur. J. Radiol. 2016, 85, 2211–2216. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Tanioka, K.; Kawaji, Y.; Tamura, T.; Nuta, J.; Hatamaru, K.; Itonaga, M.; Yoshida, T.; Ida, Y.; Maekita, T.; et al. Utility of Elastography with Endoscopic Ultrasonography Shear-Wave Measurement for Diagnosing Chronic Pancreatitis. Gut Liver 2019. [Google Scholar] [CrossRef] [PubMed]
- Tirkes, T.; Yadav, D.; Conwell, D.L.; Territo, P.R.; Zhao, X.; Venkatesh, S.K.; Kolipaka, A.; Li, L.; Pisegna, J.R.; Pandol, S.J.; et al. Magnetic resonance imaging as a non-invasive method for the assessment of pancreatic fibrosis (MINIMAP): A comprehensive study design from the consortium for the study of chronic pancreatitis, diabetes, and pancreatic cancer. Abdom. Radiol. 2019, 44, 2809–2821. [Google Scholar] [CrossRef]
- Zhang, J.; Zhu, L.; Yao, L.; Ding, X.; Chen, D.; Wu, H.; Lu, Z.; Zhou, W.; Zhang, L.; An, P.; et al. Deep learning-based pancreas segmentation and station recognition system in EUS: Development and validation of a useful training tool (with video). Gastrointest. Endosc. 2020, 92, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Kuwahara, T.; Hara, K.; Mizuno, N.; Haba, S.; Okuno, N.; Koda, H.; Miyano, A.; Fumihara, D. Current status of artificial intelligence analysis for endoscopic ultrasonography. Dig. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parenchymal Criteria |
|---|
| Major A |
| Hyperechoic foci (>2 mm in length/width with shadowing) |
| Major B |
| Lobularity (≥3 contiguous lobules = “with honeycombing”) |
| Minor |
| Cyst (anechoic, round/elliptical with or without septations) |
| Hyperechoic strands (≥3 mm in at least 2 different directions with respect to the imaged plane) |
| Hyperechoic foci (>2 mm in length/width with no shadowing) Lobularity (noncontiguous lobules = “without honeycombing”) |
| Duct Criteria |
| Major A |
| MPD calculi (echogenic structure(s) within the MPD with acoustic shadowing) |
| Minor |
| MPD dilation (≥3.5 mm in body or >1.5 mm in tail) |
| Irregular MPD contour (uneven or irregular outline and ectatic course) |
| Dilated side branches (>3 tubular anechoic structures each measuring ≥1 mm in width, budding from the MPD) |
| Hyperechoic MPD margin (echogenic, distinct structure >50% of entire MPD in the body and tail) |
| Diagnostic Items for CP |
|---|
|
|
|
|
|
|
|
| Definite CP: either a or b |
| a. Definite findings of (1) or (2) |
| b. Probable findings of (1) or (2), plus more than two items among (3), (4), and (5) |
| Probable CP |
| Probable findings of (1) or (2) |
| Early CP |
| More than three items among (3)–(7) plus image findings of early CP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takasaki, Y.; Ishii, S.; Fujisawa, T.; Ushio, M.; Takahashi, S.; Yamagata, W.; Ito, K.; Suzuki, A.; Ochiai, K.; Tomishima, K.; et al. Endoscopic Ultrasonography Findings of Early and Suspected Early Chronic Pancreatitis. Diagnostics 2020, 10, 1018. https://doi.org/10.3390/diagnostics10121018
Takasaki Y, Ishii S, Fujisawa T, Ushio M, Takahashi S, Yamagata W, Ito K, Suzuki A, Ochiai K, Tomishima K, et al. Endoscopic Ultrasonography Findings of Early and Suspected Early Chronic Pancreatitis. Diagnostics. 2020; 10(12):1018. https://doi.org/10.3390/diagnostics10121018
Chicago/Turabian StyleTakasaki, Yusuke, Shigeto Ishii, Toshio Fujisawa, Mako Ushio, Sho Takahashi, Wataru Yamagata, Koichi Ito, Akinori Suzuki, Kazushige Ochiai, Ko Tomishima, and et al. 2020. "Endoscopic Ultrasonography Findings of Early and Suspected Early Chronic Pancreatitis" Diagnostics 10, no. 12: 1018. https://doi.org/10.3390/diagnostics10121018
APA StyleTakasaki, Y., Ishii, S., Fujisawa, T., Ushio, M., Takahashi, S., Yamagata, W., Ito, K., Suzuki, A., Ochiai, K., Tomishima, K., Saito, H., & Isayama, H. (2020). Endoscopic Ultrasonography Findings of Early and Suspected Early Chronic Pancreatitis. Diagnostics, 10(12), 1018. https://doi.org/10.3390/diagnostics10121018