Association of Serum Calprotectin Concentrations with Mortality in Critically Ill and Septic Patients


 ,
,  , ,
, , 
 and
and
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Patients’ Characteristics
2.2. Calprotectin Measurements
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
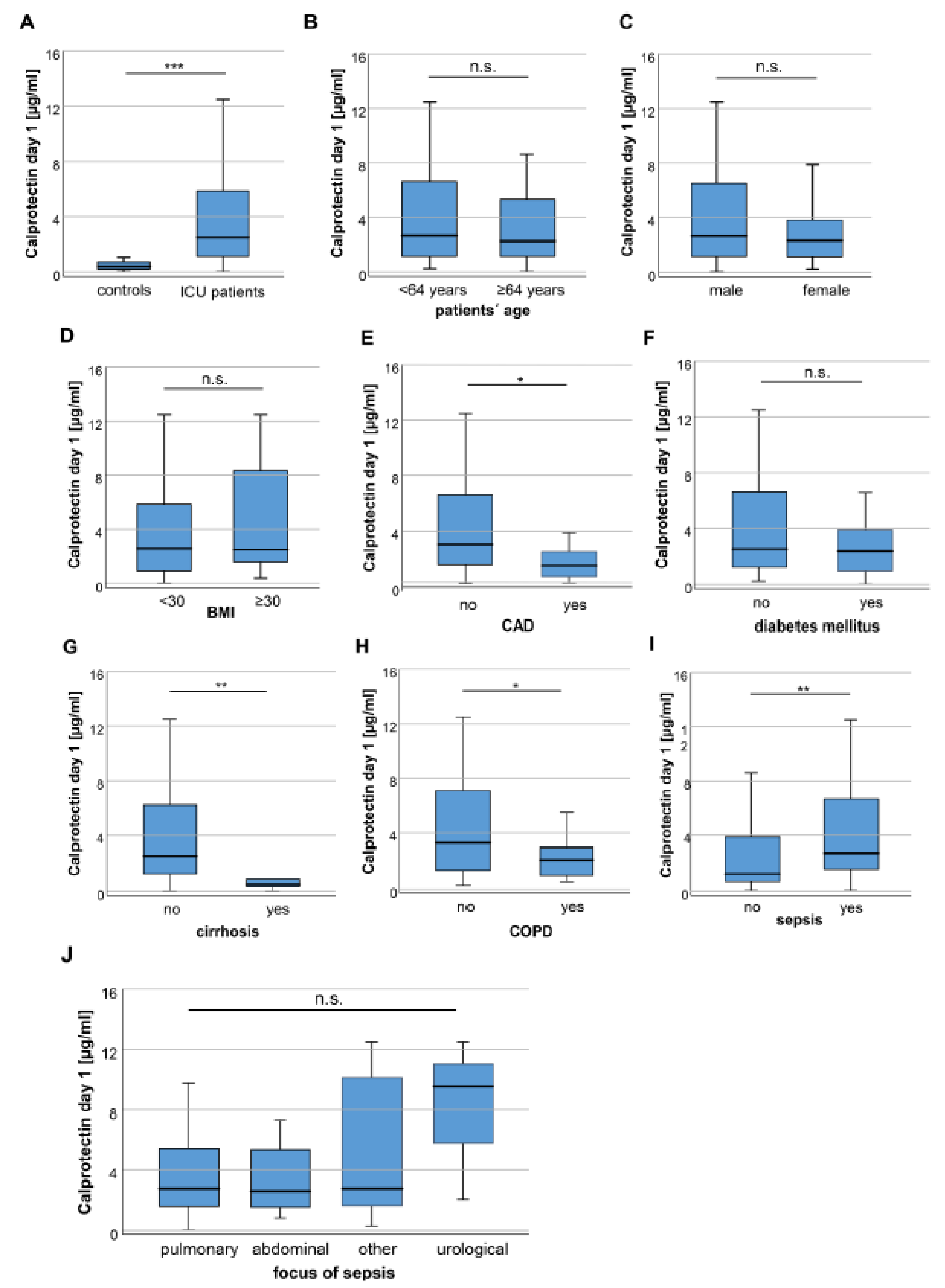
3.2. Calprotectin Serum Concentrations Are Increased in Critically Ill and Septic Patients
3.3. Calprotectin Serum Concentrations in ICU Patients Positively Correlate with Markers of Systemic Inflammation and Parameters of Mechanical Ventilation
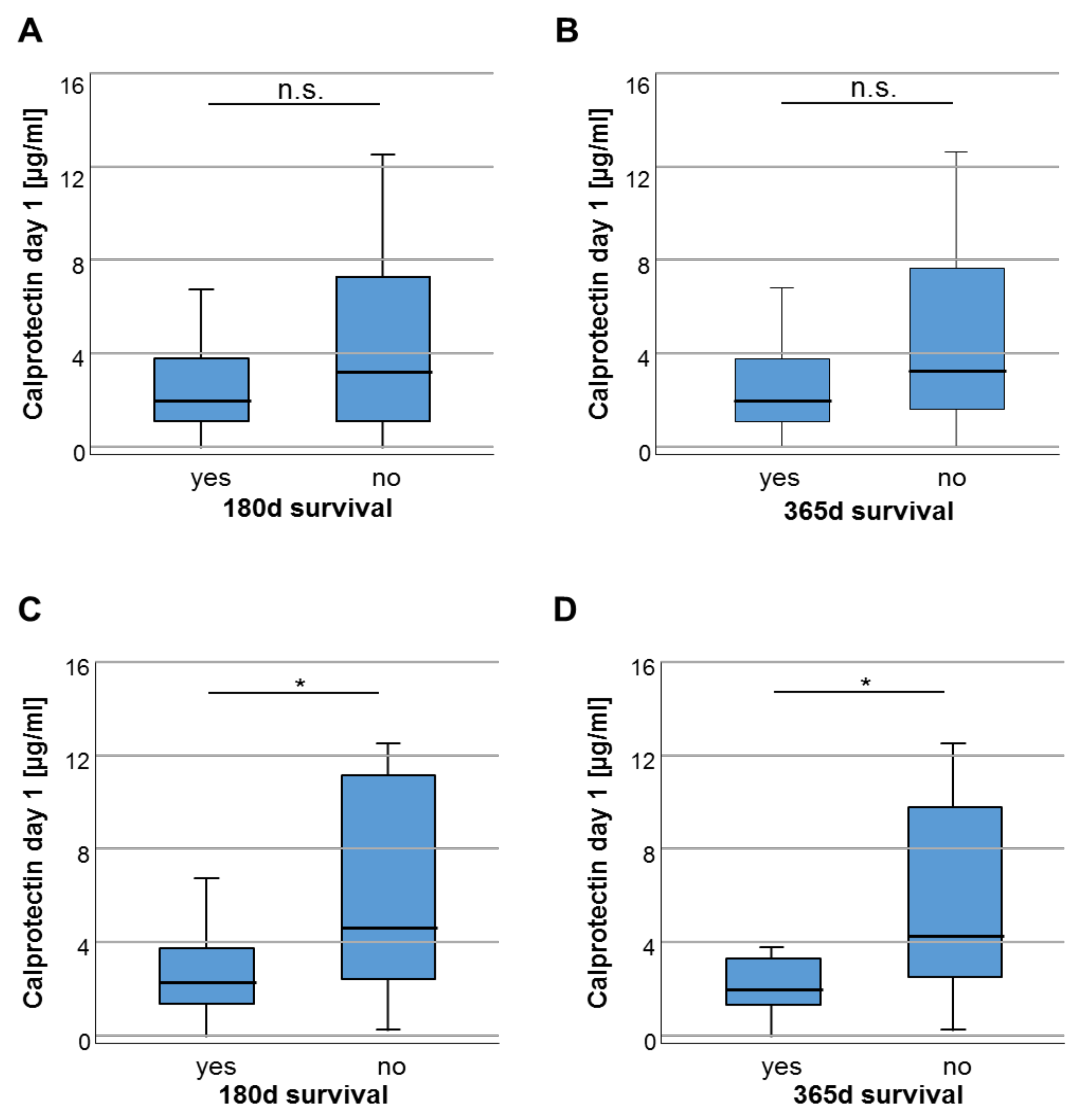
3.4. Baseline Calprotectin Serum Soncentrations Predict Long-Term Survival in Septic Patients
3.5. Increasing Calprotectin Serum Concentrations during the Course of Critical Illness Indicate an Improved Overall Survival
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ICU | medical intensive care unit |
| APACHE | acute physiology and chronic health evaluation score |
| SOFA | sequential organ failure assessment score |
| SAPS2 | simplified acute physiology score |
| BMI | body mass index |
| CAD | coronary artery disease |
| COPD | chronic obstructive pulmonary disease |
| CRP | C-reactive protein |
| IL-6 | interleukin 6 |
| RRT | renal replacement therapy |
| GFR | glomerular filtration rate |
| AST | aspartate aminotransferase |
| BNP | brain natriuretic peptide |
| LDH | lactate dehydrogenase |
| FiO2 | inspiratory oxygen fraction |
| Pmax | maximum airway pressure |
| PEEP | positive end-expiratory pressure |
| OS | overall survival |
References
- Striz, I.; Trebichavsky, I. Calprotectin—A pleiotropic molecule in acute and chronic inflammation. Physiol. Res. 2004, 53, 245–253. [Google Scholar] [PubMed]
- Fagerhol, M.K.; Dale, I.; Andersson, T. A radioimmunoassay for a granulocyte protein as a marker in studies on the turnover of such cells. Bull. Eur. Physiopathol. Respir. 1980, 16 Suppl, 273–282. [Google Scholar]
- Roseth, A.G.; Aadland, E.; Jahnsen, J.; Raknerud, N. Assessment of disease activity in ulcerative colitis by faecal calprotectin, a novel granulocyte marker protein. Digestion 1997, 58, 176–180. [Google Scholar] [CrossRef]
- Sipponen, T.; Savilahti, E.; Kolho, K.L.; Nuutinen, H.; Turunen, U.; Farkkila, M. Crohn’s disease activity assessed by fecal calprotectin and lactoferrin: Correlation with crohn’s disease activity index and endoscopic findings. Inflamm. Bowel Dis. 2008, 14, 40–46. [Google Scholar] [CrossRef]
- Kang, K.Y.; Woo, J.W.; Park, S.H. S100a8/a9 as a biomarker for synovial inflammation and joint damage in patients with rheumatoid arthritis. Korean J. Intern. Med. 2014, 29, 12–19. [Google Scholar] [CrossRef]
- Soyfoo, M.S.; Roth, J.; Vogl, T.; Pochet, R.; Decaux, G. Phagocyte-specific s100a8/a9 protein levels during disease exacerbations and infections in systemic lupus erythematosus. J. Rheumatol. 2009, 36, 2190–2194. [Google Scholar] [CrossRef]
- De Jong, H.K.; Achouiti, A.; Koh, G.C.; Parry, C.M.; Baker, S.; Faiz, M.A.; van Dissel, J.T.; Vollaard, A.M.; van Leeuwen, E.M.; Roelofs, J.J.; et al. Expression and function of s100a8/a9 (calprotectin) in human typhoid fever and the murine salmonella model. PLoS Negl. Trop. Dis. 2015, 9, e0003663. [Google Scholar] [CrossRef]
- Raju, M.S.; Kamaraju, R.S.; Sritharan, V.; Rajkumar, K.; Natarajan, S.; Kumar, A.D.; Burgula, S. Continuous evaluation of changes in the serum proteome from early to late stages of sepsis caused by klebsiella pneumoniae. Mol. Med. Rep. 2016, 13, 4835–4844. [Google Scholar] [CrossRef]
- Natesan, M.; Corea, E.; Krishnananthasivam, S.; Sathkumara, H.D.; Dankmeyer, J.L.; Dyas, B.K.; Amemiya, K.; De Silva, A.D.; Ulrich, R.G. Calprotectin as a biomarker for melioidosis disease progression and management. J. Clin. Microbiol. 2017, 55, 1205–1210. [Google Scholar] [CrossRef]
- Njunge, J.M.; Gwela, A.; Kibinge, N.K.; Ngari, M.; Nyamako, L.; Nyatichi, E.; Thitiri, J.; Gonzales, G.B.; Bandsma, R.H.J.; Walson, J.L.; et al. Biomarkers of post-discharge mortality among children with complicated severe acute malnutrition. Sci. Rep. 2019, 9, 5981. [Google Scholar] [CrossRef]
- Zhang, L.N.; Wang, X.H.; Wu, L.; Huang, L.; Zhao, C.G.; Peng, Q.Y.; Ai, Y.H. Diagnostic and predictive levels of calcium-binding protein a8 and tumor necrosis factor receptor-associated factor 6 in sepsis-associated encephalopathy: A prospective observational study. Chin. Med. J. 2016, 129, 1674–1681. [Google Scholar] [CrossRef]
- Vogl, T.; Tenbrock, K.; Ludwig, S.; Leukert, N.; Ehrhardt, C.; van Zoelen, M.A.; Nacken, W.; Foell, D.; van der Poll, T.; Sorg, C.; et al. Mrp8 and mrp14 are endogenous activators of toll-like receptor 4, promoting lethal, endotoxin-induced shock. Nat. Med. 2007, 13, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Ehrchen, J.M.; Sunderkotter, C.; Foell, D.; Vogl, T.; Roth, J. The endogenous toll-like receptor 4 agonist s100a8/s100a9 (calprotectin) as innate amplifier of infection, autoimmunity, and cancer. J. Leukoc. Biol. 2009, 86, 557–566. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Liu, V.X.; Lu, Y.; Carey, K.A.; Gilbert, E.R.; Afshar, M.; Akel, M.; Shah, N.S.; Dolan, J.; Winslow, C.; Kipnis, P.; et al. Comparison of early warning scoring systems for hospitalized patients with and without infection at risk for in-hospital mortality and transfer to the intensive care unit. JAMA Netw. Open 2020, 3, e205191. [Google Scholar] [CrossRef] [PubMed]
- Shahsavarinia, K.; Moharramzadeh, P.; Arvanagi, R.J.; Mahmoodpoor, A. Qsofa score for prediction of sepsis outcome in emergency department. Pak. J. Med. Sci. 2020, 36, 668–672. [Google Scholar] [CrossRef]
- Larsson, A.; Tyden, J.; Johansson, J.; Lipcsey, M.; Bergquist, M.; Kultima, K.; Mandic-Havelka, A. Calprotectin is superior to procalcitonin as a sepsis marker and predictor of 30-day mortality in intensive care patients. Scand. J. Clin. Lab. Investig. 2020, 80, 156–161. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Gyorffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff finder: A comprehensive and straightforward web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef]
- Decembrino, L.; De Amici, M.; Pozzi, M.; De Silvestri, A.; Stronati, M. Serum calprotectin: A potential biomarker for neonatal sepsis. J. Immunol. Res. 2015, 2015, 147973. [Google Scholar] [CrossRef]
- Jonsson, N.; Nilsen, T.; Gille-Johnson, P.; Bell, M.; Martling, C.R.; Larsson, A.; Martensson, J. Calprotectin as an early biomarker of bacterial infections in critically ill patients: An exploratory cohort assessment. Crit. Care Resusc. 2017, 19, 205–213. [Google Scholar]
- Bartakova, E.; Stefan, M.; Stranikova, A.; Pospisilova, L.; Arientova, S.; Beran, O.; Blahutova, M.; Maca, J.; Holub, M. Calprotectin and calgranulin c serum levels in bacterial sepsis. Diagn. Microbiol. Infect. Dis. 2019, 93, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Li, J.; Han, Y.; Zhao, S.; Zheng, Y.; Sui, F.; Xin, X.; Ma, W.; Jiang, Y.; Yao, Y.; et al. Serum calprotectin expression as a diagnostic marker for sepsis in postoperative intensive care unit patients. J. Interferon Cytokine Res. Off. J. Int. Soc. Interferon Cytokine Res. 2016, 36, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, L.; Nybo, M.; Poulsen, M.K.; Henriksen, J.E.; Dahl, J.; Rasmussen, L.M. Plasma calprotectin and its association with cardiovascular disease manifestations, obesity and the metabolic syndrome in type 2 diabetes mellitus patients. BMC Cardiovasc. Disord. 2014, 14, 196. [Google Scholar] [CrossRef] [PubMed]
- Homann, C.; Garred, P.; Graudal, N.; Hasselqvist, P.; Christiansen, M.; Fagerhol, M.K.; Thomsen, A.C. Plasma calprotectin: A new prognostic marker of survival in alcohol-induced cirrhosis. Hepatology 1995, 21, 979–985. [Google Scholar] [CrossRef]
- Pouwels, S.D.; Nawijn, M.C.; Bathoorn, E.; Riezebos-Brilman, A.; van Oosterhout, A.J.; Kerstjens, H.A.; Heijink, I.H. Increased serum levels of ll37, hmgb1 and s100a9 during exacerbation in copd patients. Eur. Respir. J. 2015, 45, 1482–1485. [Google Scholar] [CrossRef]
- Lorey, M.B.; Rossi, K.; Eklund, K.K.; Nyman, T.A.; Matikainen, S. Global characterization of protein secretion from human macrophages following non-canonical caspase-4/5 inflammasome activation. Mol. Cell. Proteom. 2017, 16, S187–S199. [Google Scholar] [CrossRef]
- Lee, C.W.; Kou, H.W.; Chou, H.S.; Chou, H.H.; Huang, S.F.; Chang, C.H.; Wu, C.H.; Yu, M.C.; Tsai, H.I. A combination of sofa score and biomarkers gives a better prediction of septic aki and in-hospital mortality in critically ill surgical patients: A pilot study. World J. Emerg. Surg. Wjes 2018, 13, 41. [Google Scholar] [CrossRef]
- Mikacenic, C.; Moore, R.; Dmyterko, V.; West, T.E.; Altemeier, W.A.; Liles, W.C.; Lood, C. Neutrophil extracellular traps (nets) are increased in the alveolar spaces of patients with ventilator-associated pneumonia. Crit. Care 2018, 22, 358. [Google Scholar] [CrossRef]
- Kuipers, M.T.; Vogl, T.; Aslami, H.; Jongsma, G.; van den Berg, E.; Vlaar, A.P.; Roelofs, J.J.; Juffermans, N.P.; Schultz, M.J.; van der Poll, T.; et al. High levels of s100a8/a9 proteins aggravate ventilator-induced lung injury via tlr4 signaling. PLoS ONE 2013, 8, e68694. [Google Scholar] [CrossRef]
- Shi, H.; Zuo, Y.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.N.; Woodard, W.; Lezak, S.P.; Lugogo, N.L.; et al. Neutrophil calprotectin identifies severe pulmonary disease in covid-19. MedRxiv Prepr. Serv. Health Sci. 2020. [Google Scholar] [CrossRef]
- Gao, S.; Yang, Y.; Fu, Y.; Guo, W.; Liu, G. Diagnostic and prognostic value of myeloid-related protein complex 8/14 for sepsis. Am. J. Emerg. Med. 2015, 33, 1278–1282. [Google Scholar] [CrossRef]
- Pruenster, M.; Vogl, T.; Roth, J.; Sperandio, M. S100a8/a9: From basic science to clinical application. Pharmacol. Ther. 2016, 167, 120–131. [Google Scholar] [CrossRef]
- Dreschers, S.; Ohl, K.; Lehrke, M.; Mollmann, J.; Denecke, B.; Costa, I.; Vogl, T.; Viemann, D.; Roth, J.; Orlikowsky, T.; et al. Impaired cellular energy metabolism in cord blood macrophages contributes to abortive response toward inflammatory threats. Nat. Commun. 2019, 10, 1685. [Google Scholar] [CrossRef]
- Coveney, A.P.; Wang, W.; Kelly, J.; Liu, J.H.; Blankson, S.; Wu, Q.D.; Redmond, H.P.; Wang, J.H. Myeloid-related protein 8 induces self-tolerance and cross-tolerance to bacterial infection via tlr4- and tlr2-mediated signal pathways. Sci. Rep. 2015, 5, 13694. [Google Scholar] [CrossRef]
- Otsuka, K.; Terasaki, F.; Ikemoto, M.; Fujita, S.; Tsukada, B.; Katashima, T.; Kanzaki, Y.; Sohmiya, K.; Kono, T.; Toko, H.; et al. Suppression of inflammation in rat autoimmune myocarditis by s100a8/a9 through modulation of the proinflammatory cytokine network. Eur. J. Heart Fail. 2009, 11, 229–237. [Google Scholar] [CrossRef]
- Lusitani, D.; Malawista, S.E.; Montgomery, R.R. Calprotectin, an abundant cytosolic protein from human polymorphonuclear leukocytes, inhibits the growth of borrelia burgdorferi. Infect. Immun. 2003, 71, 4711–4716. [Google Scholar] [CrossRef]
- Damo, S.M.; Kehl-Fie, T.E.; Sugitani, N.; Holt, M.E.; Rathi, S.; Murphy, W.J.; Zhang, Y.; Betz, C.; Hench, L.; Fritz, G.; et al. Molecular basis for manganese sequestration by calprotectin and roles in the innate immune response to invading bacterial pathogens. Proc. Natl. Acad. Sci. USA 2013, 110, 3841–3846. [Google Scholar] [CrossRef]
- Simard, J.C.; Simon, M.M.; Tessier, P.A.; Girard, D. Damage-associated molecular pattern s100a9 increases bactericidal activity of human neutrophils by enhancing phagocytosis. J. Immunol. 2011, 186, 3622–3631. [Google Scholar] [CrossRef]
- Achouiti, A.; Vogl, T.; Urban, C.F.; Rohm, M.; Hommes, T.J.; van Zoelen, M.A.; Florquin, S.; Roth, J.; van’t Veer, C.; de Vos, A.F.; et al. Myeloid-related protein-14 contributes to protective immunity in gram-negative pneumonia derived sepsis. PLoS Pathog. 2012, 8, e1002987. [Google Scholar] [CrossRef] [PubMed]
- Achouiti, A.; Vogl, T.; Van der Meer, A.J.; Stroo, I.; Florquin, S.; de Boer, O.J.; Roth, J.; Zeerleder, S.; van’t Veer, C.; de Vos, A.F.; et al. Myeloid-related protein-14 deficiency promotes inflammation in staphylococcal pneumonia. Eur. Respir. J. 2015, 46, 464–473. [Google Scholar] [CrossRef]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; Groupdagger, P. Probast: A tool to assess the risk of bias and applicability of prediction model studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients |
|---|---|
| Number | 165 |
| Gender | |
| Female (%) | 40.6 |
| Male (%) | 59.4 |
| Age, median in years (range) | 64 (18–90) |
| BMI, median (range) | 25.8 (15.9–86.5) |
| Diabetes mellitus type 2 (%) | 31.6 |
| Coronary artery disease (%) | 22.3 |
| COPD (%) | 29.8 |
| Malignant disease (%) | 10 |
| Solid tumour | 5 |
| Hematological malignancy | 4 |
| Main diagnosis/reason for admission (%) | |
| Sepsis | 65.5 |
| Infectious focus of sepsis (%) | |
| Pulmonary | 55.6 |
| Abdominal | 19.4 |
| Urinary tract | 2.8 |
| other | 22.2 |
| Liver cirrhosis | 4.2 |
| Cardiopulmonary disease | 13.9 |
| Acute liver failure | 1.2 |
| Acute pancreatitis | 5.5 |
| Gastrointestinal bleeding | 2.4 |
| Other | 7.3 |
| APACHE-II score at day 1 | 17 (3–43) |
| <17 (%) | 50.7 |
| >17 (%) | 49.3 |
| SOFA score at day 1 | 9 (0–17) |
| <9 (%) | 56.6 |
| >9 (%) | 43.4 |
| Mechanical ventilation demand (%) at day 1 | 41.8 |
| Vasopressor demand (%) at day 1 | 62.4 |
| Death on ICU (%) | 19.4 |
| 30 d mortality (%) | 23.7 |
| 90 d mortality (%) | 32.3 |
| 180 d mortality (%) | 40.4 |
| 365 d mortality (%) | 57.0 |
| long-term mortality (%) | 40.0 |
| Calprotectin [µg/mL] | |
| Day 1 | 2.482 (0.004–12.5) |
| Day 7 | 4.073 (0.544–3.023) |
| All Patients | Sepsis | |||||
|---|---|---|---|---|---|---|
| r | 95% CI | p | r | 95% CI | p | |
| Baseline Characteristics | ||||||
| Age | −28.25 | −68.75–12.25 | 0.170 | −40.14 | −91.61–11.33 | 0.125 |
| BMI | 51.24 | −8.66–111.14 | 0.093 | 40.29 | −25.54–106.13 | 0.227 |
| ICU Days | 4.95 | −29.50–39.39 | 0.777 | −22.81 | −62.51–16.88 | 0.257 |
| Hospital days | 15.180 | −12.25–42.61 | 0.275 | −2.30 | −35.45–30.86 | 0.890 |
| Markers of Inflammation | ||||||
| Leukocytes | 39.37 | −17.32–96.06 | 0.172 | 25.53 | −39.0–90.03 | 0.434 |
| CRP | 17.63 | 10.64–24.62 | <0.001 *** | 17.67 | 7.01–28.33 | 0.001 ** |
| Procalcitonin | 18.38 | −4.0–40.73 | 0.106 | 15.16 | −9.35–39.67 | 0.221 |
| IL-6 | −0.12 | −0.37–0.13 | 0.340 | −0.151 | −0.413–0.11 | 0.255 |
| Markers of Organ Dysfunction | ||||||
| Creatinine | 287.92 | −7.14–582.98 | 0.056 | 221.73 | −129.37–572.84 | 0.213 |
| GFR | −27.21 | −66.69–12.27 | 0.175 | −20.08 | −69.79–29.62 | 0.423 |
| Duration of RRT in Days | 186.97 | 59.41–314.53 | 0.004 ** | 130.45 | −10.99–272.0 | 0.070 |
| Urea | 12.74 | 1.22–24.26 | 0.030 * | 10.79 | −4.09–25.66 | 0.153 |
| Sodium | −43.85 | −148.60–60.91 | 0.409 | −38.57 | −163.89–86.76 | 0.543 |
| Kalium | −560.22 | −1465.68–345.23 | 0.223 | −556.72 | −1764.11–650.67 | 0.362 |
| AST | −0.190 | −1.02–0.64 | 0.650 | 0.045 | −2.52–2.62 | 0.972 |
| Bilirubin Total | −26.53 | −335.50–282.44 | 0.865 | 579.00 | −116.06–1274.06 | 0.101 |
| LDH | 0.90 | −0.37–2.17 | 0.165 | 3.77 | −0.171–7.72 | 0.061 |
| Lactate | 114.17 | −158.44–386.78 | 0.409 | 185.17 | −180.55–550.89 | 0.317 |
| NT-proBNP | 0.032 | −0.06–0.13 | 0.503 | 0.024 | −0.09–0.13 | 0.671 |
| Clinical Scores | ||||||
| APACHE II | −25.23 | −110.75–60.29 | 0.560 | −89.70 | −202.80–23.40 | 0.118 |
| SOFA | −30.19 | −229.89–169.51 | 0.764 | −151.36 | −481.0–162.07 | 0.323 |
| SAPS2 | −43.06 | −124.12–38.00 | 0.291 | −18.56 | −119.84–82.73 | 0.711 |
| Mechanical Ventilation Parameters | ||||||
| FiO2 at Day 1 | 64.23 | 33.13–95.33 | <0.001 *** | 52.61 | 10.0–95.22 | 0.017 * |
| Pmax at Day 1 | 106.58 | 23.98–189.19 | 0.012 * | 114.37 | 15.37–213.37 | 0.025* |
| PEEP at Day 1 | 315.12 | 145.40–484.83 | <0.001 *** | 358.23 | 159.59–556.86 | 0.001 ** |
| Duration of Mechanical Ventilation in Days | −0.23 | −1.95–1.50 | 0.796 | −1.38 | −3.33–0.58 | 0.166 |
| Parameter | Univariate Cox Regression | Multivariate Stepwise Backward Cox Regression | ||
|---|---|---|---|---|
| p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | |
| Calprotectin delta # | 0.004 ** | 0.850 (0.761–0.948) | 0.001 ** | 0.815 (0.720–0.922) |
| Age | 0.002 ** | 1.041 (1.014–1.068) | 0.001 ** | 1.043 (1.018–1.070) |
| Sex | 0.518 | 0.811 (0.429–1.532) | ||
| BMI | 0.119 | 0.955 (0.901–1.012) | 0.016 * | 0.921 (0.860–0.985) |
| CRP | 0.113 | 1.003 (0.999–1.007) | 0.140 | 1.003 (0.999–1.007) |
| Procalcitonin | 0.851 | 1.001 (0.990–1.012) | ||
| Creatinine | 0.498 | 1.039 (0.931–1.159) | ||
| Bilirubin | 0.339 | 1.167 (0.850–1.601) | ||
| Lactate | 0.295 | 1.081 (0.935–1.249) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wirtz, T.H.; Buendgens, L.; Weiskirchen, R.; Loosen, S.H.; Haehnsen, N.; Puengel, T.; Abu Jhaisha, S.; Brozat, J.F.; Hohlstein, P.; Koek, G.; et al. Association of Serum Calprotectin Concentrations with Mortality in Critically Ill and Septic Patients. Diagnostics 2020, 10, 990. https://doi.org/10.3390/diagnostics10110990
Wirtz TH, Buendgens L, Weiskirchen R, Loosen SH, Haehnsen N, Puengel T, Abu Jhaisha S, Brozat JF, Hohlstein P, Koek G, et al. Association of Serum Calprotectin Concentrations with Mortality in Critically Ill and Septic Patients. Diagnostics. 2020; 10(11):990. https://doi.org/10.3390/diagnostics10110990
Chicago/Turabian StyleWirtz, Theresa H., Lukas Buendgens, Ralf Weiskirchen, Sven H. Loosen, Nina Haehnsen, Tobias Puengel, Samira Abu Jhaisha, Jonathan F. Brozat, Philipp Hohlstein, Ger Koek, and et al. 2020. "Association of Serum Calprotectin Concentrations with Mortality in Critically Ill and Septic Patients" Diagnostics 10, no. 11: 990. https://doi.org/10.3390/diagnostics10110990
APA StyleWirtz, T. H., Buendgens, L., Weiskirchen, R., Loosen, S. H., Haehnsen, N., Puengel, T., Abu Jhaisha, S., Brozat, J. F., Hohlstein, P., Koek, G., Eisert, A., Mohr, R., Roderburg, C., Luedde, T., Trautwein, C., Tacke, F., & Koch, A. (2020). Association of Serum Calprotectin Concentrations with Mortality in Critically Ill and Septic Patients. Diagnostics, 10(11), 990. https://doi.org/10.3390/diagnostics10110990