MPG and NPRL3 Polymorphisms Are Associated with Ischemic Stroke Susceptibility and Post-Stroke Mortality

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Whole-Exome Sequencing (WES) Analysis
2.3. Genotyping
2.4. Post-Stroke Mortality
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison of the Frequencies of NPRL3 and MPG Polymorphisms between Patients with Ischemic Stroke, Subtypes, and Controls
3.3. Haplotype Analyses of NPRL3 and MPG Polymorphisms between Ischemic Stroke Patients and Controls
3.4. Combined Effects of NPRL3 and MPG Polymorphisms and Clinical Factors
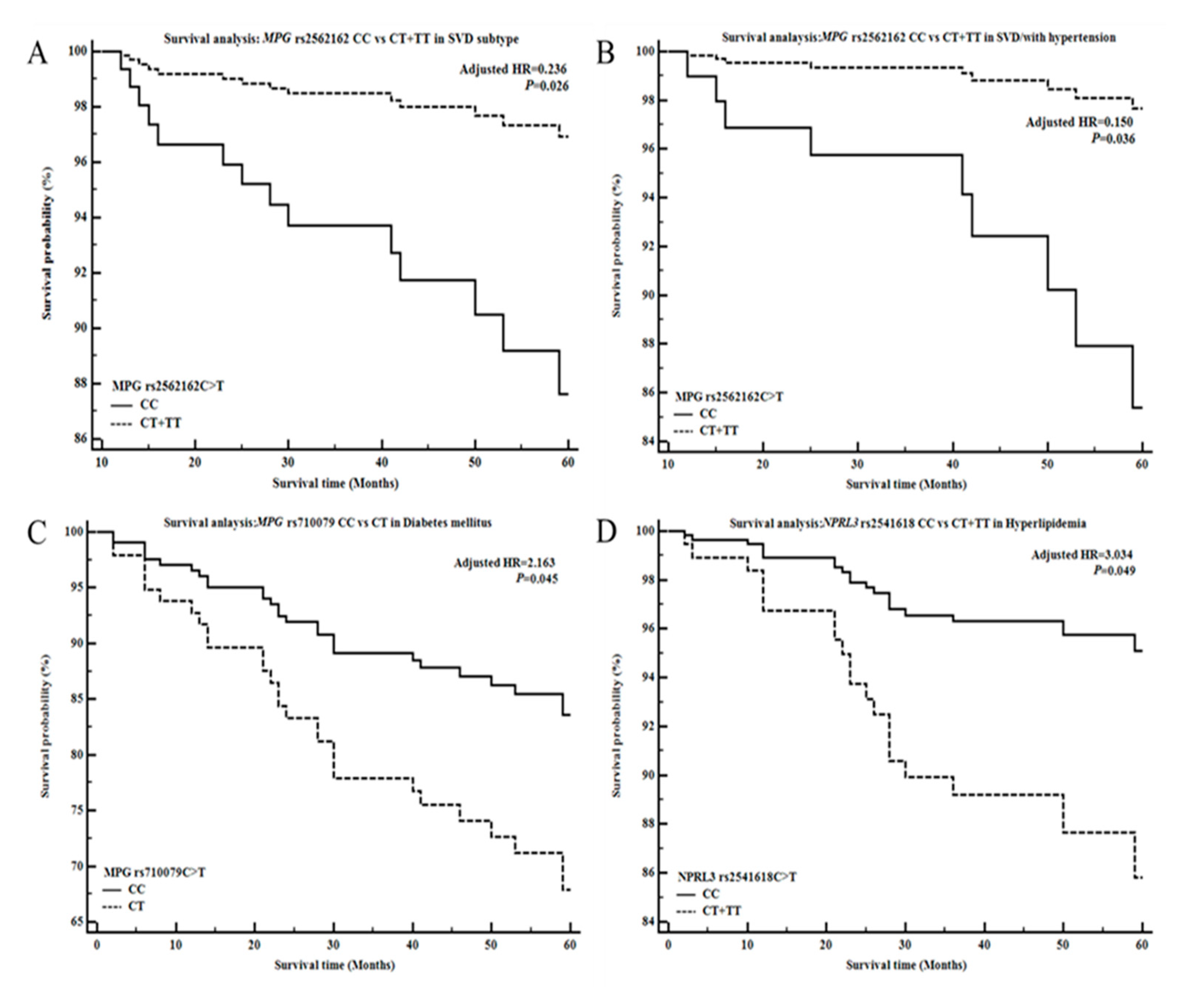
3.5. Analysis of NPRL3 and MPG Polymorphisms with Respect to Survival in Ischemic Stroke Patients and Subtypes
3.6. Clinical Factors in Ischemic Stroke Patients, Subtypes Stratified by NPRL3 and MPG Polymorphisms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
References
- Jiang, T.; Tan, M.S.; Tan, L.; Yu, J.T. Application of next-generation sequencing technologies in Neurology. Ann. Transl. Med. 2014, 2, 125. [Google Scholar] [PubMed]
- Fu, W.; O’Connor, T.D.; Jun, G.; Kang, H.M.; Abecasis, G.; Leal, S.M.; Gabriel, S.; Rieder, M.J.; Altshuler, D.; Shendure, J.; et al. Analysis of 6515 exomes reveals the recent origin of most human protein-coding variants. Nature 2013, 493, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.J.; Markkandan, K.; Baek, I.P.; Mun, S.; Lee, W.; Kim, H.S.; Han, K. An efficient and tunable parameter to improve variant calling for whole genome and exome sequencing data. Genes Genom. 2018, 40, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, S.; Akhtar, Z.; Latif, M.; Hassan, M.; Faisal, M.; Iqbal, F. A novel nonsense mutation in NPR2 gene causing Acromesomelic dysplasia, type Maroteaux in a consanguineous family in Southern Punjab (Pakistan). Genes Genom. 2020, 42, 847–854. [Google Scholar] [CrossRef]
- Rabbani, B.; Tekin, M.; Mahdieh, N. The promise of whole-exome sequencing in medical genetics. J. Hum. Genet. 2014, 59, 5–15. [Google Scholar] [CrossRef]
- Leung, G.K.C.; Mak, C.C.Y.; Fung, J.L.F.; Wong, W.H.S.; Tsang, M.H.Y.; Yu, M.H.C.; Pei, S.L.C.; Yeung, K.S.; Mok, G.T.K.; Lee, C.P.; et al. Identifying the genetic causes for prenatally diagnosed structural congenital anomalies (SCAs) by whole-exome sequencing (WES). BMC Med. Genom. 2018, 11, 93. [Google Scholar] [CrossRef]
- Zheng, G.X.; Lau, B.T.; Schnall-Levin, M.; Jarosz, M.; Bell, J.M.; Hindson, C.M.; Kyriazopoulou-Panagiotopoulou, S.; Masquelier, D.A.; Merrill, L.; Terry, J.M.; et al. Haplotyping germline and cancer genomes with high-throughput linked-read sequencing. Nat. Biotechnol. 2016, 34, 303–311. [Google Scholar] [CrossRef]
- Rimmer, A.; Phan, H.; Mathieson, I.; Iqbal, Z.; Twigg, S.R.F.; Consortium, W.G.S.; Wilkie, A.O.M.; McVean, G.; Lunter, G. Integrating mapping-, assembly- and haplotype-based approaches for calling variants in clinical sequencing applications. Nat. Genet. 2014, 46, 912–918. [Google Scholar] [CrossRef]
- Bis, J.C.; Jian, X.; Kunkle, B.W.; Chen, Y.; Hamilton-Nelson, K.L.; Bush, W.S.; Salerno, W.J.; Lancour, D.; Ma, Y.; Renton, A.E.; et al. Whole exome sequencing study identifies novel rare and common Alzheimer’s-Associated variants involved in immune response and transcriptional regulation. Mol. Psychiatry 2018, 25, 1859–1875. [Google Scholar] [CrossRef]
- Jia, X.; Zhang, F.; Bai, J.; Gao, L.; Zhang, X.; Sun, H.; Sun, D.; Guan, R.; Sun, W.; Xu, L.; et al. Combinational analysis of linkage and exome sequencing identifies the causative mutation in a Chinese family with congenital cataract. BMC Med. Genet. 2013, 14, 107. [Google Scholar] [CrossRef]
- Scherrer, N.; Fays, F.; Mueller, B.; Luft, A.; Fluri, F.; Christ-Crain, M.; Devaux, Y.; Katan, M. MicroRNA 150-5p Improves Risk Classification for Mortality within 90 Days after Acute Ischemic Stroke. J. Stroke 2017, 19, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.O.; Bae, J.; Kim, J.; Oh, S.H.; An, H.J.; Han, I.B.; Oh, D.; Kim, O.J.; Kim, N.K. Association of MicroRNA Biogenesis Genes Polymorphisms with Ischemic Stroke Susceptibility and Post-Stroke Mortality. J. Stroke 2018, 20, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Venketasubramanian, N.; Yoon, B.W.; Pandian, J.; Navarro, J.C. Stroke Epidemiology in South, East, and South-East Asia: A Review. J. Stroke 2017, 19, 286–294. [Google Scholar] [CrossRef]
- Mustacchi, P. Risk factors in stroke. West. J. Med. 1985, 143, 186–192. [Google Scholar] [PubMed]
- Kannel, W.B.; McGee, D.L. Diabetes and cardiovascular disease. The Framingham study. JAMA 1979, 241, 2035–2038. [Google Scholar] [CrossRef] [PubMed]
- Kulshreshtha, A.; Vaccarino, V.; Goyal, A.; McClellan, W.; Nahab, F.; Howard, V.J.; Judd, S.E. Family history of stroke and cardiovascular health in a national cohort. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2015, 24, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Cui, R.; Iso, H.; Yamagishi, K.; Saito, I.; Kokubo, Y.; Inoue, M.; Tsugane, S.; Group, J.S. High serum total cholesterol levels is a risk factor of ischemic stroke for general Japanese population: The JPHC study. Atherosclerosis 2012, 221, 565–569. [Google Scholar] [CrossRef]
- Albertsen, I.E.; Overvad, T.F.; Lip, G.Y.; Larsen, T.B. Smoking, atrial fibrillation, and ischemic stroke: A confluence of epidemics. Curr. Opin. Cardiol. 2015, 30, 512–517. [Google Scholar] [CrossRef]
- Shekelle, R.B.; Ostfeld, A.M.; Klawans, H.L., Jr. Hypertension and risk of stroke in an elderly population. Stroke 1974, 5, 71–75. [Google Scholar] [CrossRef]
- Jimenez-Conde, J.; Biffi, A.; Rahman, R.; Kanakis, A.; Butler, C.; Sonni, S.; Massasa, E.; Cloonan, L.; Gilson, A.; Capozzo, K.; et al. Hyperlipidemia and reduced white matter hyperintensity volume in patients with ischemic stroke. Stroke 2010, 41, 437–442. [Google Scholar] [CrossRef]
- Kurl, S.; Laukkanen, J.A.; Niskanen, L.; Laaksonen, D.; Sivenius, J.; Nyyssonen, K.; Salonen, J.T. Metabolic syndrome and the risk of stroke in middle-aged men. Stroke 2006, 37, 806–811. [Google Scholar] [CrossRef] [PubMed]
- Mouradian, M.S.; Majumdar, S.R.; Senthilselvan, A.; Khan, K.; Shuaib, A. How well are hypertension, hyperlipidemia, diabetes, and smoking managed after a stroke or transient ischemic attack? Stroke 2002, 33, 1656–1659. [Google Scholar] [CrossRef] [PubMed]
- Mohr, J.P.; Caplan, L.R.; Melski, J.W.; Goldstein, R.J.; Duncan, G.W.; Kistler, J.P.; Pessin, M.S.; Bleich, H.L. The Harvard Cooperative Stroke Registry: A prospective registry. Neurology 1978, 28, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Stegner, D.; Nieswandt, B. Platelet receptor signaling in thrombus formation. J. Mol. Med. 2011, 89, 109–121. [Google Scholar] [CrossRef]
- Shah, A.B.; Beamer, N.; Coull, B.M. Enhanced in vivo platelet activation in subtypes of ischemic stroke. Stroke 1985, 16, 643–647. [Google Scholar] [CrossRef]
- Nurden, P.; Poujol, C.; Nurden, A.T. The evolution of megakaryocytes to platelets. Baillieres Clin. Haematol. 1997, 10, 1–27. [Google Scholar] [CrossRef]
- Raslova, H.; Baccini, V.; Loussaief, L.; Comba, B.; Larghero, J.; Debili, N.; Vainchenker, W. Mammalian target of rapamycin (mTOR) regulates both proliferation of megakaryocyte progenitors and late stages of megakaryocyte differentiation. Blood 2006, 107, 2303–2310. [Google Scholar] [CrossRef]
- Maiese, K. Cutting through the complexities of mTOR for the treatment of stroke. Curr. Neurovasc. Res. 2014, 11, 177–186. [Google Scholar] [CrossRef]
- Xie, R.; Wang, P.; Ji, X.; Zhao, H. Ischemic post-conditioning facilitates brain recovery after stroke by promoting Akt/mTOR activity in nude rats. J. Neurochem. 2013, 127, 723–732. [Google Scholar] [CrossRef]
- Sykora, P.; Wilson, D.M., 3rd; Bohr, V.A. Base excision repair in the mammalian brain: Implication for age related neurodegeneration. Mech. Ageing Dev. 2013, 134, 440–448. [Google Scholar] [CrossRef]
- He, W.; Huang, P.; Liu, D.; Zhong, L.; Yu, R.; Li, J. Polymorphism of the XRCC1 Gene Is Associated with Susceptibility and Short-Term Recovery of Ischemic Stroke. Int. J. Environ. Res. Public Health 2016, 13, 1016. [Google Scholar] [CrossRef] [PubMed]
- Canugovi, C.; Misiak, M.; Ferrarelli, L.K.; Croteau, D.L.; Bohr, V.A. The role of DNA repair in brain related disease pathology. DNA Repair 2013, 12, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Abner, C.W.; Lau, A.Y.; Ellenberger, T.; Bloom, L.B. Base excision and DNA binding activities of human alkyladenine DNA glycosylase are sensitive to the base paired with a lesion. J. Biol. Chem. 2001, 276, 13379–13387. [Google Scholar] [CrossRef] [PubMed]
- Hedglin, M.; O’Brien, P.J. Human alkyladenine DNA glycosylase employs a processive search for DNA damage. Biochemistry 2008, 47, 11434–11445. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.; Chetram, M.A.; Woodrick, J.; Mitra, P.S.; Manthena, P.V.; Khatkar, P.; Dakshanamurthy, S.; Dixon, M.; Karmahapatra, S.K.; Nuthalapati, N.K.; et al. Germ line variants of human N-methylpurine DNA glycosylase show impaired DNA repair activity and facilitate 1,N6-ethenoadenine-induced mutations. J. Biol. Chem. 2015, 290, 4966–4980. [Google Scholar] [CrossRef]
- Nandagopal, N.; Roux, P.P. Regulation of global and specific mRNA translation by the mTOR signaling pathway. Translation 2015, 3, e983402. [Google Scholar] [CrossRef]
- Bar-Peled, L.; Chantranupong, L.; Cherniack, A.D.; Chen, W.W.; Ottina, K.A.; Grabiner, B.C.; Spear, E.D.; Carter, S.L.; Meyerson, M.; Sabatini, D.M. A tumor suppressor complex with GAP activity for the Rag GTPases that signal amino acid sufficiency to mTORC1. Science 2013, 340, 1100–1106. [Google Scholar] [CrossRef]
- Adams, H.P. Jr.; Biller, J. Classification of subtypes of ischemic stroke: History of the trial of org 10172 in acute stroke treatment classification. Stroke 2015, 46, e114–e117. [Google Scholar] [CrossRef]
- Ricos, M.G.; Hodgson, B.L.; Pippucci, T.; Saidin, A.; Ong, Y.S.; Heron, S.E.; Licchetta, L.; Bisulli, F.; Bayly, M.A.; Hughes, J.; et al. Mutations in the mammalian target of rapamycin pathway regulators NPRL2 and NPRL3 cause focal epilepsy. Ann. Neurol. 2016, 79, 120–131. [Google Scholar] [CrossRef]
- Weiner, G.M.; Ducruet, A.F. Mammalian target of rapamycin (mTOR) activity promotes neuronal survival in stroke with or without ischemic postconditioning. Neurosurgery 2015, 76, N19–N20. [Google Scholar] [CrossRef][Green Version]
- Cocito, L.; Loeb, C. Focal epilepsy as a possible sign of transient subclinical ischemia. Eur. Neurol. 1989, 29, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Swarowska, M.; Janowska, A.; Polczak, A.; Klimkowicz-Mrowiec, A.; Pera, J.; Slowik, A.; Dziedzic, T. The sustained increase of plasma fibrinogen during ischemic stroke predicts worse outcome independently of baseline fibrinogen level. Inflammation 2014, 37, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Storhaug, H.M.; Norvik, J.V.; Toft, I.; Eriksen, B.O.; Lochen, M.L.; Zykova, S.; Solbu, M.; White, S.; Chadban, S.; Jenssen, T. Uric acid is a risk factor for ischemic stroke and all-cause mortality in the general population: A gender specific analysis from The Tromso Study. BMC Cardiovasc. Disord. 2013, 13, 115. [Google Scholar] [CrossRef]
- Orhan, G.; Elkama, A.; Mungan, S.O.; Eruyar, E.; Karahalil, B. The impact of detoxifying and repair gene polymorphisms on oxidative stress in ischemic stroke. Neurol. Sci. 2016, 37, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Mahabir, S.; Abnet, C.C.; Qiao, Y.L.; Ratnasinghe, L.D.; Dawsey, S.M.; Dong, Z.W.; Taylor, P.R.; Mark, S.D. A prospective study of polymorphisms of DNA repair genes XRCC1, XPD23 and APE/ref-1 and risk of stroke in Linxian, China. J. Epidemiol. Community Health 2007, 61, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Hu, X.; Gan, Y.; Gao, Y.; Liang, W.; Chen, J. Mechanistic insight into DNA damage and repair in ischemic stroke: Exploiting the base excision repair pathway as a model of neuroprotection. Antioxid. Redox Signal. 2011, 14, 1905–1918. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimkhani, M.R.; Daneshmand, A.; Mazumder, A.; Allocca, M.; Calvo, J.A.; Abolhassani, N.; Jhun, I.; Muthupalani, S.; Ayata, C.; Samson, L.D. Aag-initiated base excision repair promotes ischemia reperfusion injury in liver, brain, and kidney. Proc. Natl. Acad. Sci. USA 2014, 111, E4878–E4886. [Google Scholar] [CrossRef]
- Cho, A.H.; Suh, D.C.; Kim, G.E.; Kim, J.S.; Lee, D.H.; Kwon, S.U.; Park, S.M.; Kang, D.W. MRI evidence of reperfusion injury associated with neurological deficits after carotid revascularization procedures. Eur. J. Neurol. 2009, 16, 1066–1069. [Google Scholar] [CrossRef]
- Oberheiden, T.; Blahak, C.; Nguyen, X.D.; Fatar, M.; Elmas, E.; Morper, N.; Dempfle, C.E.; Bazner, H.; Hennerici, M.; Borggrefe, M.; et al. Activation of platelets and cellular coagulation in cerebral small-vessel disease. Blood Coagul. Fibrinolysis 2010, 21, 729–735. [Google Scholar] [CrossRef]
- Pinto, A.; Tuttolomondo, A.; Di Raimondo, D.; Fernandez, P.; Licata, G. Risk factors profile and clinical outcome of ischemic stroke patients admitted in a Department of Internal Medicine and classified by TOAST classification. Int. Angiol. 2006, 25, 261–267. [Google Scholar]
- Di Raimondo, D.; Tuttolomondo, A.; Buttà, C.; Casuccio, A.; Giarrusso, L.; Miceli, G.; Licata, G.; Pinto, A. Metabolic and anti-inflammatory effects of a home-based programme of aerobic physical exercise. Int. J. Clin. Pract. 2013, 67, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Maida, C.; Pinto, A. Diabetic foot syndrome as a possible cardiovascular marker in diabetic patients. J. Diabetes Res. 2015, 2015, 268390. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Maida, C.; Pinto, A. Diabetic foot syndrome: Immune-inflammatory features as possible cardiovascular markers in diabetes. World J. Orthop. 2015, 6, 62–76. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Controls (n = 417) | Stroke Patients (n = 519) | Pa | LAD Patients (n = 207) | Pa | SVD Patients (n = 149) | Pa | CE Patients (n = 53) | Pa |
|---|---|---|---|---|---|---|---|---|---|
| Males, n (%) | 173 (41.5) | 229 (44.1) | 0.609 | 89 (43.0) | 0.819 | 72 (48.3) | 0.368 | 21 (39.6) | 0.866 |
| Age, (years, mean ± SD) | 63.05 ± 11.00 | 63.29 ± 11.95 | 0.747 | 64.36 ± 11.81 | 0.172 | 60.76 ± 11.63 | 0.032 | 66.58 ± 12.55 | 0.031 |
| Smoking, n (%) | 140 (33.6) | 194 (37.4) | 0.405 | 77 (37.2) | 0.535 | 54 (36.2) | 0.682 | 16 (30.2) | 0.724 |
| MetS, n (%) | 94 (22.5) | 238 (45.9) | <0.0001 | 112 (54.1) | <0.0001 | 68 (45.6) | 0.0001 | 20 (37.7) | 0.070 |
| HTN, n (%) | 171 (41.0) | 331 (63.8) | 0.0001 | 131 (63.3) | 0.003 | 92 (61.7) | 0.011 | 30 (56.6) | 0.189 |
| DM, n (%) | 56 (13.4) | 142 (27.4) | <0.0001 | 55 (26.6) | 0.001 | 47 (31.5) | <0.0001 | 12 (22.6) | 0.132 |
| Hyperlipidemia, n (%) | 95 (22.8) | 156 (30.1) | 0.057 | 70 (33.8) | 0.027 | 44 (29.5) | 0.207 | 10 (18.9) | 0.603 |
| Genotypes | Controls (n = 417) | Stroke Patients (n = 519) | AOR (95% CI) * | P† | P‡ |
|---|---|---|---|---|---|
| NPRL3 rs2541618 C>T | |||||
| CC | 205 (49.2) | 225 (43.4) | 1.000 (reference) | ||
| CT | 178 (42.7) | 238 (45.9) | 1.270 (0.944–1.710) | 0.115 | 0.153 |
| TT | 34 (8.2) | 56 (10.8) | 1.679 (1.011–2.787) | 0.045 | 0.180 |
| Additive (CC vs. CT vs. TT) | 1.205 (0.979–1.485) | 0.079 | 0.161 | ||
| Dominant (CC vs. CT+TT) | 1.333 (1.004–1.770) | 0.047 | 0.094 | ||
| Recessive (CC+CT vs. TT) | 1.504 (0.924–2.449) | 0.101 | 0.366 | ||
| HWE-P | 0.591 | 0.555 | |||
| NPRL3 rs75187722 G>A | |||||
| GG | 333 (79.9) | 438 (84.4) | 1.000 (reference) | ||
| GA | 82 (19.7) | 77 (14.8) | 0.638 (0.438–0.931) | 0.020 | 0.080 |
| AA | 2 (0.5) | 4 (0.8) | 0.979 (0.172–5.586) | 0.981 | 0.981 |
| Additive (GG vs. GA vs. AA) | 0.742 (0.531–1.037) | 0.081 | 0.161 | ||
| Dominant (GG vs. GA+AA) | 0.650 (0.448–0.942) | 0.023 | 0.092 | ||
| Recessive (GG+GA vs. AA) | 1.060 (0.186–6.039) | 0.948 | 0.948 | ||
| HWE-P | 0.197 | 0.762 | |||
| MPG rs2562162 C>T | |||||
| CC | 239 (57.3) | 266 (51.3) | 1.000 (reference) | ||
| CT | 151 (36.2) | 217 (41.8) | 1.265 (0.950–1.684) | 0.107 | 0.153 |
| TT | 27 (6.5) | 36 (6.9) | 1.213 (0.696–2.114) | 0.495 | 0.661 |
| Additive (CC vs. CT vs. TT) | 1.175 (0.944–1.463) | 0.149 | 0.198 | ||
| Dominant (CC vs. CT+TT) | 1.252 (0.954–1.643) | 0.106 | 0.141 | ||
| Recessive (CC+CT vs. TT) | 1.105 (0.642–1.901) | 0.719 | 0.948 | ||
| HWE-P | 0.633 | 0.355 | |||
| MPG rs710079 C>T | |||||
| CC | 290 (69.5) | 376 (72.4) | 1.000 (reference) | ||
| CT | 118 (28.3) | 136 (26.2) | 0.962 (0.709–1.304) | 0.801 | 0.801 |
| TT | 9 (2.2) | 7 (1.3) | 0.500 (0.174–1.436) | 0.198 | 0.396 |
| Additive (CC vs. CT vs. TT) | 0.893 (0.680–1.172) | 0.413 | 0.413 | ||
| Dominant (CC vs. CT+TT) | 0.925 (0.686–1.246) | 0.606 | 0.606 | ||
| Recessive (CC+CT vs. TT) | 0.489 (0.170–1.401) | 0.183 | 0.366 | ||
| HWE-P | 0.454 | 0.173 | |||
| Genotype | Controls (n = 417) | LAD (n = 207) | AOR (95% CI) * | P† | P‡ | SVD (n = 149) | AOR (95% CI) * | P† | P‡ | CE (n = 53) | AOR (95% CI) * | P† | P‡ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NPRL3 rs2541618 C>T | |||||||||||||
| CC | 205 (49.2) | 93 (44.9) | 1.000 (reference) | 57 (38.3) | 1.000 (reference) | 22 (41.5) | 1.000 (reference) | ||||||
| CT | 178 (42.7) | 89 (43.0) | 1.040 (0.717–1.509) | 0.835 | 0.870 | 73 (49.0) | 1.375 (0.902–2.097) | 0.138 | 0.185 | 27 (50.9) | 1.402 (0.766–2.568) | 0.274 | 0.737 |
| TT | 34 (8.2) | 25 (12.1) | 1.860 (1.015–3.408) | 0.045 | 0.178 | 19 (12.8) | 2.406 (1.225–4.725) | 0.011 | 0.043 | 4 (7.5) | 1.069 (0.329–3.480) | 0.911 | 0.911 |
| Additive (CC vs. CT vs. TT) | 1.237 (0.946–1.618) | 0.120 | 0.239 | 1.496 (1.102–2.031) | 0.010 | 0.037 | 1.172 (0.747–1.838) | 0.490 | 0.927 | ||||
| Dominant (CC vs. CT+TT) | 1.159 (0.815–1.647) | 0.411 | 0.548 | 1.524 (1.019–2.279) | 0.041 | 0.054 | 1.342 (0.747–2.412) | 0.326 | 0.775 | ||||
| Recessive (CC+CT vs. TT) | 1.832 (1.028–3.262) | 0.040 | 0.160 | 2.059 (1.087–3.899) | 0.027 | 0.106 | 0.893 (0.295–2.701) | 0.841 | 0.841 | ||||
| NPRL3 rs75187722 G>A | |||||||||||||
| GG | 333 (79.9) | 179 (86.5) | 1.000 (reference) | 130 (87.2) | 1.000 (reference) | 43 (81.1) | 1.000 (reference) | ||||||
| GA | 82 (19.7) | 28 (13.5) | 0.622 (0.380–1.017) | 0.058 | 0.207 | 18 (12.1) | 0.474 (0.261–0.860) | 0.014 | 0.056 | 9 (17.0) | 0.835 (0.388–1.797) | 0.644 | 0.737 |
| AA | 2 (0.5) | 0 (0.0) | NA | 0.995 | 0.995 | 1 (0.7) | 1.301 (0.112–15.114) | 0.834 | 0.834 | 1 (1.9) | 2.829 (0.238–33.596) | 0.410 | 0.911 |
| Additive (GG vs. GA vs. AA) | 0.599 (0.370–0.968) | 0.037 | 0.146 | 0.535 (0.306–0.934) | 0.028 | 0.037 | 0.969 (0.491–1.914) | 0.927 | 0.927 | ||||
| Dominant (GG vs. GA+AA) | 0.606 (0.371–0.989) | 0.045 | 0.180 | 0.495 (0.277–0.886) | 0.018 | 0.044 | 0.898 (0.429–1.878) | 0.775 | 0.775 | ||||
| Recessive (GG+GA vs. AA) | NA | 0.996 | 0.996 | 1.468 (0.127–16.980) | 0.759 | 0.759 | 2.690 (0.230–31.473) | 0.430 | 0.841 | ||||
| MPG rs2562162 C>T | |||||||||||||
| CC | 239 (57.3) | 105 (50.7) | 1.000 (reference) | 65 (43.6) | 1.000 (reference) | 28 (52.8) | 1.000 (reference) | ||||||
| CT | 151 (36.2) | 88 (42.5) | 1.359 (0.940–1.965) | 0.103 | 0.207 | 72 (48.3) | 1.569 (1.038–2.372) | 0.033 | 0.066 | 20 (37.7) | 1.156 (0.621–2.152) | 0.647 | 0.737 |
| TT | 27 (6.5) | 14 (6.8) | 1.189 (0.576–2.452) | 0.640 | 0.853 | 12 (8.1) | 1.708 (0.786–3.708) | 0.176 | 0.343 | 5 (9.4) | 1.276 (0.440–3.697) | 0.654 | 0.911 |
| Additive (CC vs. CT vs. TT) | 1.212 (0.916–1.605) | 0.179 | 0.239 | 1.422 (1.040–1.945) | 0.027 | 0.037 | 1.121 (0.718–1.753) | 0.615 | 0.927 | ||||
| Dominant (CC vs. CT+TT) | 1.332 (0.937–1.894) | 0.110 | 0.219 | 1.589 (1.069–2.363) | 0.022 | 0.044 | 1.153 (0.643–2.067) | 0.633 | 0.775 | ||||
| Recessive (CC+CT vs. TT) | 1.052 (0.522–2.121) | 0.886 | 0.996 | 1.412 (0.665–2.996) | 0.369 | 0.492 | 1.179 (0.421–3.300) | 0.754 | 0.841 | ||||
| MPG rs710079 C>T | |||||||||||||
| CC | 290 (69.5) | 151 (72.9) | 1.000 (reference) | 115 (77.2) | 1.000 (reference) | 38 (71.7) | 1.000 (reference) | ||||||
| CT | 118 (28.3) | 55 (26.6) | 0.968 (0.652–1.436) | 0.870 | 0.870 | 33 (22.1) | 0.797 (0.499–1.274) | 0.344 | 0.344 | 14 (26.4) | 0.893 (0.461–1.728) | 0.737 | 0.737 |
| TT | 9 (2.2) | 1 (0.5) | 0.217 (0.026–1.825) | 0.160 | 0.319 | 1 (0.7) | 0.293 (0.035–2.453) | 0.257 | 0.343 | 1 (1.9) | 0.819 (0.098–6.834) | 0.854 | 0.911 |
| Additive (CC vs. CT vs. TT) | 0.858 (0.598–1.231) | 0.406 | 0.406 | 0.738 (0.482–1.129) | 0.161 | 0.161 | 0.894 (0.501–1.594) | 0.704 | 0.927 | ||||
| Dominant (CC vs. CT+TT) | 0.910 (0.616–1.344) | 0.636 | 0.636 | 0.754 (0.476–1.196) | 0.230 | 0.230 | 0.891 (0.468–1.695) | 0.725 | 0.775 | ||||
| Recessive (CC+CT vs. TT) | 0.211 (0.025–1.760) | 0.151 | 0.301 | 0.294 (0.035–2.488) | 0.261 | 0.492 | 0.780 (0.094–6.509) | 0.818 | 0.841 | ||||
| Haplotypes | Controls (2n = 834) | Stroke (2n = 1038) | OR (95% CI) | P | P * |
|---|---|---|---|---|---|
| NPRL3 rs2541618 C>T/NPRL3 rs75187722 G>A/MPG rs2562162 C>T/MPG rs710079 C>T | |||||
| C-G-C-C | 418 (50.1) | 525 (50.6) | 1.000 (reference) | ||
| C-A-C-C | 21 (2.6) | 10 (1.0) | 0.379 (0.177–0.814) | 0.010 | 0.129 |
| C-A-T-T | 4 (0.4) | 0 (0.0) | 0.088 (0.005–1.649) | 0.039 | 0.254 |
| T-A-C-C | 2 (0.3) | 10 (1.0) | 3.981 (0.867–18.270) | 0.077 | 0.335 |
| NPRL3 rs2541618 C>T/NPRL3 rs75187722 G>A/MPG rs2562162 C>T | |||||
| C-G-C | 469 (56.2) | 568 (54.7) | 1.000 (reference) | ||
| C-A-T | 9 (1.1) | 4 (0.4) | 0.367 (0.112–1.200) | 0.098 | 0.196 |
| T-G-T | 162 (19.5) | 243 (23.4) | 1.239 (0.981–1.564) | 0.072 | 0.196 |
| T-A-C | 0 (0.0) | 7 (0.6) | 12.390 (0.705–217.600) | 0.019 | 0.112 |
| NPRL3 rs2541618 C>T/NPRL3 rs75187722 G>A/MPG rs710079 C>T | |||||
| C-G-C | 446 (53.5) | 568 (54.7) | 1.000 (reference) | ||
| C-G-T | 56 (6.7) | 49 (4.8) | 0.687 (0.459–1.028) | 0.067 | 0.133 |
| C-A-C | 29 (3.5) | 10 (1.0) | 0.271 (0.131–0.562) | 0.0002 | 0.001 |
| T-A-C | 0 (0.0) | 14 (1.4) | 22.780 (1.354–383.100) | 0.001 | 0.002 |
| NPRL3 rs2541618 C>T/MPG rs2562162 C>T/MPG rs710079 C>T | |||||
| C-C-C | 440 (52.8) | 532 (51.3) | 1.000 (reference) | ||
| T-T-C | 159 (19.1) | 237 (22.8) | 1.233 (0.972–1.563) | 0.084 | 0.586 |
| NPRL3 rs2541618 C>T/NPRL3 rs75187722 G>A | |||||
| C-G | 502 (60.2) | 608 (58.6) | 1.000 (reference) | ||
| T-A | 0 (0.0) | 5 (0.5) | 9.084 (0.501–164.800) | 0.068 | 0.154 |
| NPRL3 rs2541618 C>T/MPG rs2562162 C>T | |||||
| C-C | 545 (65.4) | 642 (61.9) | 1.000 (reference) | ||
| T-T | 162 (19.5) | 243 (23.4) | 1.273 (1.012–1.602) | 0.039 | 0.116 |
| NPRL3 rs75187722 G>A/MPG rs2562162 C>T | |||||
| G-C | 553 (66.3) | 669 (64.5) | 1.000 (reference) | ||
| G-T | 195 (23.4) | 284 (27.3) | 1.204 (0.972–1.492) | 0.090 | 0.147 |
| A-T | 10 (1.2) | 5 (0.5) | 0.413 (0.140–1.217) | 0.098 | 0.147 |
| Characteristics | NPRL3 rs2541618 CC | NPRL3 rs2541618 CT+TT | NPRL3 rs75187722 GG | NPRL3 rs75187722 GA+AA | MPG rs2562162 CC | MPG rs2562162 CT+TT | MPG rs710079 CC | MPG rs710079 CT+TT |
|---|---|---|---|---|---|---|---|---|
| Age (936) | ||||||||
| <63 | 1.000 (reference) | 1.436 (0.951–2.167) | 1.000 (reference) | 0.589 (0.343–1.014) | 1.000 (reference) | 1.435 (0.952–2.164) | 1.000 (reference) | 0.903 (0.573–1.424) |
| ≥63 | 0.903 (0.594–1.373) | 0.996 (0.655–1.515) | 0.762 (0.554–1.049) | 0.746 (0.443–1.255) | 0.866 (0.583–1.288) | 1.086 (0.712–1.656) | 0.785 (0.558–1.104) | 0.778 (0.501–1.207) |
| Sex (936) | ||||||||
| Male | 1.000 (reference) | 1.581 (1.033–2.421) | 1.000 (reference) | 0.544 (0.310–0.957) | 1.000 (reference) | 1.461 (0.953–2.239) | 1.000 (reference) | 0.866 (0.540–1.388) |
| Female | 1.254 (0.769–2.044) | 1.325 (0.823–2.134) | 0.890 (0.618–1.281) | 1.031 (0.586–1.812) | 0.957 (0.601–1.525) | 1.546 (0.945–2.531) | 0.946 (0.641–1.394) | 1.002 (0.606–1.657) |
| Hypertension (936) | ||||||||
| No | 1.000 (reference) | 1.060 (0.714–1.574) | 1.000 (reference) | 0.993 (0.598–1.650) | 1.000 (reference) | 1.415 (0.948–2.110) | 1.000 (reference) | 1.093 (0.715–1.672) |
| Yes | 2.085 (1.399–3.105) | 3.120 (2.116–4.599) | 2.811 (2.069–3.819) | 1.339 (0.808–2.218) | 2.725 (1.878–3.955) | 3.256 (2.193–4.833) | 2.720 (1.958–3.777) | 2.000 (1.290–3.100) |
| Diabetes mellitus (936) | ||||||||
| No | 1.000 (reference) | 1.154 (0.853–1.561) | 1.000 (reference) | 0.681 (0.454–1.020) | 1.000 (reference) | 1.184 (0.873–1.605) | 1.000 (reference) | 0.829 (0.596–1.154) |
| Yes | 2.019 (1.217–3.351) | 2.904 (1.758–4.796) | 2.048 (1.378–3.042) | 1.724 (0.833–3.567) | 1.788 (1.107–2.888) | 2.984 (1.759–5.063) | 1.779 (1.187–2.666) | 2.883 (1.410–5.893) |
| Hyperlipidemia (936) | ||||||||
| No | 1.000 (reference) | 1.180 (0.862–1.616) | 1.000 (reference) | 0.594 (0.394–0.897) | 1.000 (reference) | 1.340 (0.976–1.839) | 1.000 (reference) | 0.821 (0.582–1.159) |
| Yes | 1.311 (0.834–2.059) | 1.769 (1.143–2.736) | 1.258 (0.894–1.771) | 1.555 (0.770–3.140) | 1.601 (1.048–2.446) | 1.739 (1.107–2.733) | 1.270 (0.881–1.832) | 1.533 (0.891–2.637) |
| Smoking (930) | ||||||||
| No | 1.000 (reference) | 1.260 (0.900–1.764) | 1.000 (reference) | 0.799 (0.517–1.237) | 1.000 (reference) | 1.261 (0.899–1.769) | 1.000 (reference) | 0.989 (0.682–1.434) |
| Yes | 1.478 (0.904–2.416) | 1.649 (1.033–2.632) | 1.216 (0.848–1.743) | 0.880 (0.467–1.659) | 1.212 (0.766–1.917) | 1.946 (1.172–3.229) | 1.303 (0.888–1.912) | 1.095 (0.654–1.835) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, C.S.; Bae, J.; Kim, I.J.; Kim, J.; Oh, S.H.; Kim, O.J.; Kim, N.K. MPG and NPRL3 Polymorphisms Are Associated with Ischemic Stroke Susceptibility and Post-Stroke Mortality. Diagnostics 2020, 10, 947. https://doi.org/10.3390/diagnostics10110947
Ryu CS, Bae J, Kim IJ, Kim J, Oh SH, Kim OJ, Kim NK. MPG and NPRL3 Polymorphisms Are Associated with Ischemic Stroke Susceptibility and Post-Stroke Mortality. Diagnostics. 2020; 10(11):947. https://doi.org/10.3390/diagnostics10110947
Chicago/Turabian StyleRyu, Chang Soo, Jinkun Bae, In Jai Kim, Jinkwon Kim, Seung Hun Oh, Ok Joon Kim, and Nam Keun Kim. 2020. "MPG and NPRL3 Polymorphisms Are Associated with Ischemic Stroke Susceptibility and Post-Stroke Mortality" Diagnostics 10, no. 11: 947. https://doi.org/10.3390/diagnostics10110947
APA StyleRyu, C. S., Bae, J., Kim, I. J., Kim, J., Oh, S. H., Kim, O. J., & Kim, N. K. (2020). MPG and NPRL3 Polymorphisms Are Associated with Ischemic Stroke Susceptibility and Post-Stroke Mortality. Diagnostics, 10(11), 947. https://doi.org/10.3390/diagnostics10110947