Midshaft Clavicle Fractures Treated Nonoperatively Using Figure-of-Eight Bandage: Are Fracture Type, Shortening, and Displacement Radiographic Predictors of Failure?


 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
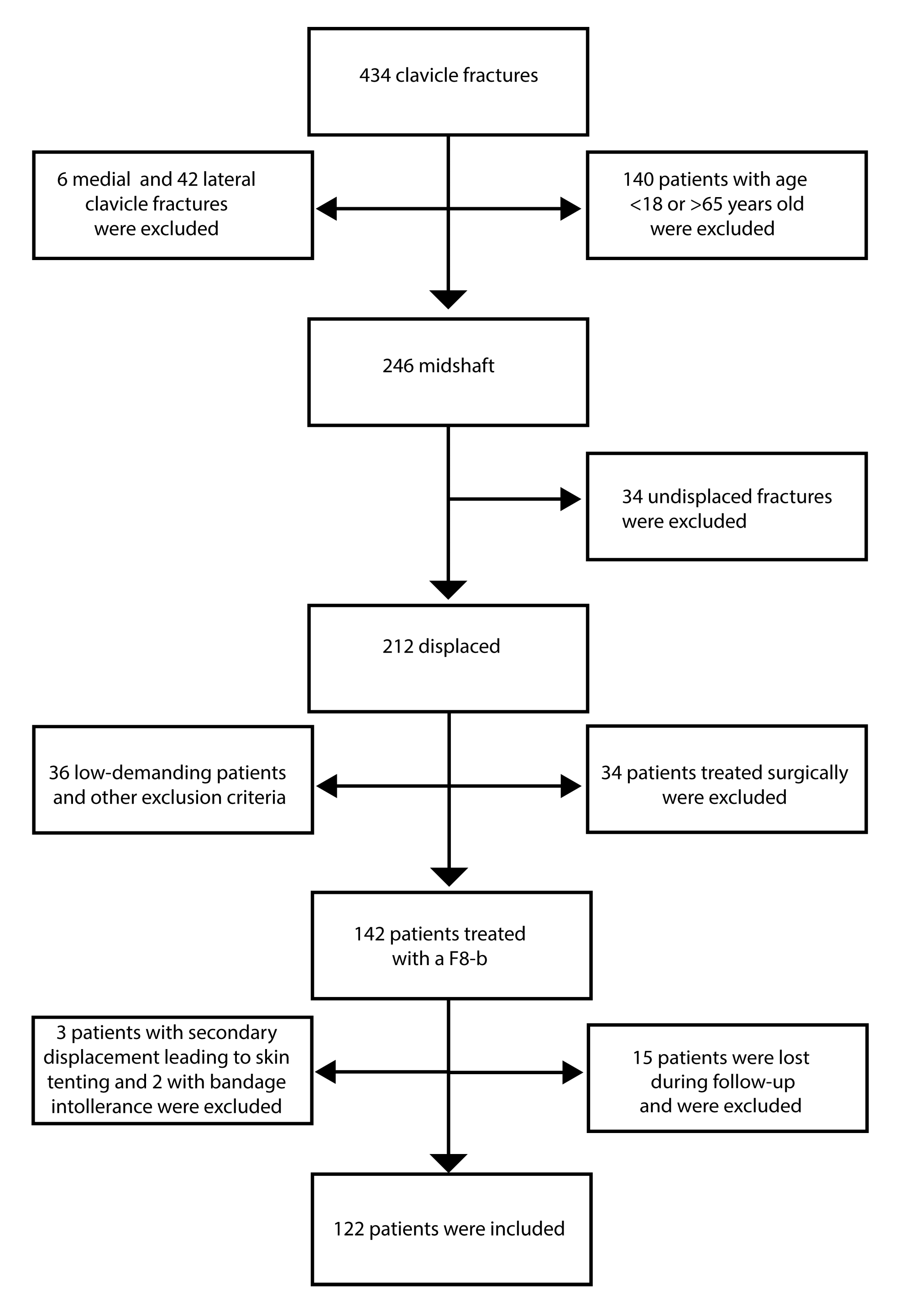
2.1. Study Population
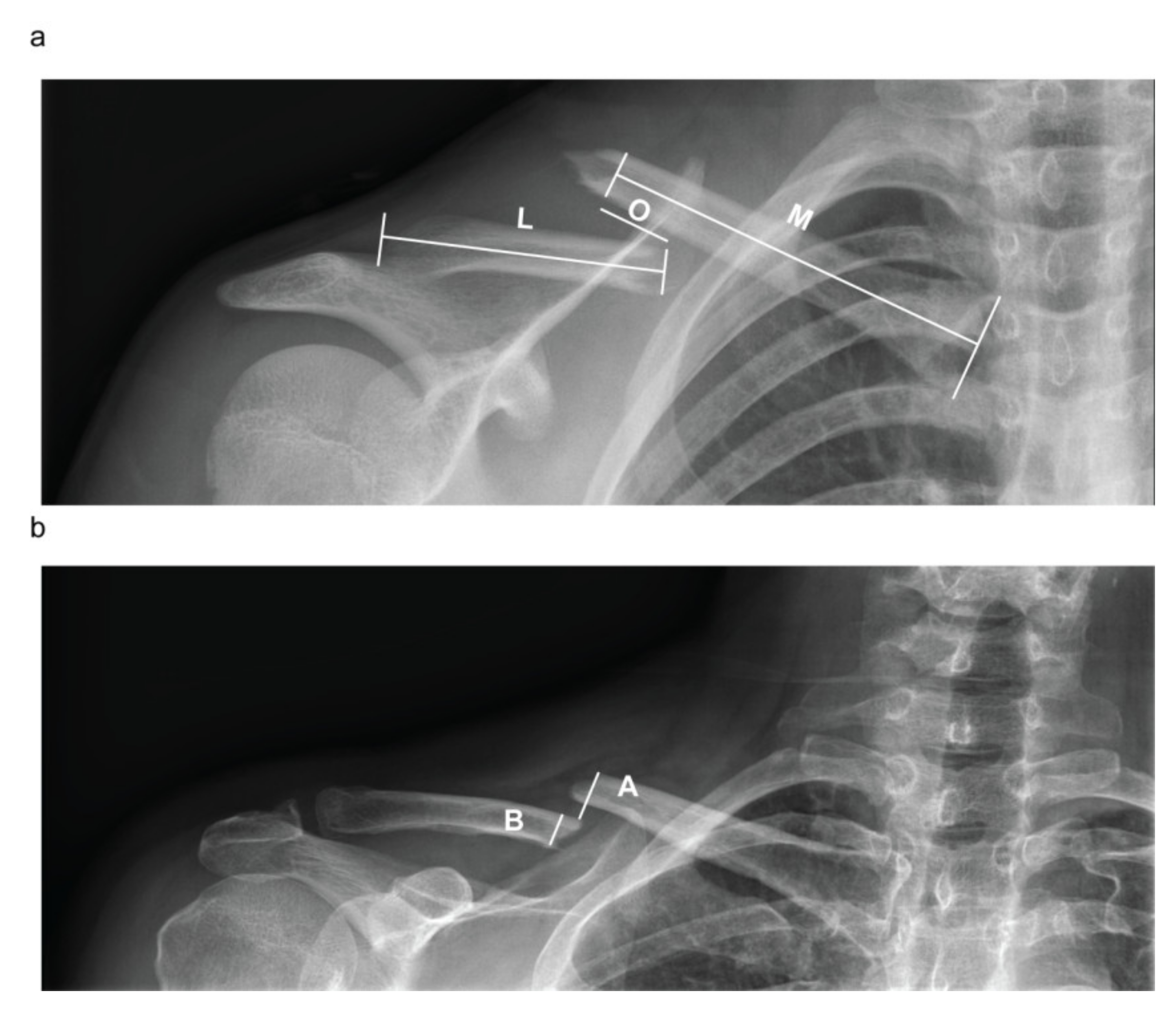
2.2. Patient Assessment and Evaluation of the Radiographic Outcomes
2.3. Nonoperative Treatment and Follow-Up Program
2.4. Statistical Analysis
3. Results
Patient Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Coppa, V.; Dei Giudici, L.; Cecconi, S.; Marinelli, M.; Gigante, A. Midshaft clavicle fractures treatment: Threaded Kirschner wire versus conservative approach. Strateg. Trauma Limb Reconstr. (Online) 2017, 12, 141–150. [Google Scholar]
- Nordqvist, A.; Petersson, C. The incidence of fractures of the clavicle. Clin. Orthop. Relat. Res. 1994, 127–132. [Google Scholar] [CrossRef]
- Postacchini, F.; Gumina, S.; De Santis, P.; Albo, F. Epidemiology of clavicle fractures. J. Shoulder Elb. Surg. 2002, 11, 452–456. [Google Scholar] [CrossRef]
- Herteleer, M.; Winckelmans, T.; Hoekstra, H.; Nijs, S. Epidemiology of clavicle fractures in a level 1 trauma center in Belgium. Eur. J. Trauma Emerg. Surg. 2017, 44, 717–726. [Google Scholar] [CrossRef]
- Robinson, C.M. Fractures of the clavicle in the adult. Epidemiology and classification. J. Bone Jt. Surg. Br. Vol. 1998, 80, 476–484. [Google Scholar] [CrossRef]
- Ledger, M.; Leeks, N.; Ackland, T.; Wang, A. Short malunions of the clavicle: An anatomic and functional study. J. Shoulder Elb. Surg. 2005, 14, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Naveen, B.M.; Joshi, G.R.; Harikrishnan, B. Management of mid-shaft clavicular fractures: Comparison between non-operative treatment and plate fixation in 60 patients. Strateg. Trauma Limb Reconstr. (Online) 2017, 12, 11–18. [Google Scholar] [CrossRef]
- Oki, S.; Matsumura, N.; Kiriyama, Y.; Iwamoto, T.; Sato, K.; Nagura, T. Three-Dimensional Deformities of Nonoperative Midshaft Clavicle Fractures: A Surface Matching Analysis. J. Orthop. Trauma 2017, 31, e385–e389. [Google Scholar] [CrossRef]
- Van Tongel, A.; De Wilde, L. Sternoclavicular joint injuries: A literature review. Muscles Ligaments Tendons J. 2011, 1, 100–105. [Google Scholar]
- Lenza, M.; Belloti, J.C.; Andriolo, R.B.; Faloppa, F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst. Rev. 2014, Cd007121. [Google Scholar] [CrossRef]
- McKee, R.C.; Whelan, D.B.; Schemitsch, E.H.; McKee, M.D. Operative versus nonoperative care of displaced midshaft clavicular fractures: A meta-analysis of randomized clinical trials. J. Bone Jt. Surg. Am. Vol. 2012, 94, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Rehn, C.H.; Kirkegaard, M.; Viberg, B.; Larsen, M.S. Operative versus nonoperative treatment of displaced midshaft clavicle fractures in adults: A systematic review. Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 2014, 24, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Guo, W.J.; Li, A.B.; Cheng, G.J.; Lei, T.; Zhao, Y.M. Operative versus nonoperative treatment for displaced midshaft clavicle fractures: A meta-analysis based on current evidence. Clinics 2015, 70, 584–592. [Google Scholar] [CrossRef]
- Hoogervorst, P.; van Schie, P.; van den Bekerom, M.P. Midshaft clavicle fractures: Current concepts. EFORT Open Rev. 2018, 3, 374–380. [Google Scholar] [CrossRef]
- Frima, H.; van Heijl, M.; Michelitsch, C.; van der Meijden, O.; Beeres, F.J.P.; Houwert, R.M.; Sommer, C. Clavicle fractures in adults; current concepts. Eur. J. Trauma Emerg. Surg. 2020, 46, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Neer, C.S., 2nd. Nonunion of the clavicle. J. Am. Med. Assoc. 1960, 172, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Rowe, C.R. An atlas of anatomy and treatment of midclavicular fractures. Clin. Orthop. Relat. Res. 1968, 58, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Tagliapietra, J.; Angelini, A.; Belluzzi, E.; Pozzuoli, A.; Berizzi, A.; Ruggieri, P. The challenging management of a delayed union midshaft clavicle fracture complicated by an acute pseudoaneurysm of the subclavian artery in a superelderly diabetic patient. Aging Clin. Exp. Res. 2019, 31, 567–569. [Google Scholar] [CrossRef]
- Robinson, C.M.; Goudie, E.B.; Murray, I.R.; Jenkins, P.J.; Ahktar, M.A.; Read, E.O.; Foster, C.J.; Clark, K.; Brooksbank, A.J.; Arthur, A.; et al. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: A multicenter, randomized, controlled trial. J. Bone Jt. Surg. Am. Vol. 2013, 95, 1576–1584. [Google Scholar] [CrossRef]
- Tamaoki, M.J.S.; Matsunaga, F.T.; Costa, A.; Netto, N.A.; Matsumoto, M.H.; Belloti, J.C. Treatment of Displaced Midshaft Clavicle Fractures: Figure-of-Eight Harness Versus Anterior Plate Osteosynthesis: A Randomized Controlled Trial. J. Bone Jt. Surg. Am. Vol. 2017, 99, 1159–1165. [Google Scholar] [CrossRef]
- Zlowodzki, M.; Zelle, B.A.; Cole, P.A.; Jeray, K.; McKee, M.D. Treatment of acute midshaft clavicle fractures: Systematic review of 2144 fractures: On behalf of the Evidence-Based Orthopaedic Trauma Working Group. J. Orthop. Trauma 2005, 19, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Nowak, J.; Holgersson, M.; Larsson, S. Can we predict long-term sequelae after fractures of the clavicle based on initial findings? A prospective study with nine to ten years of follow-up. J. Shoulder Elb. Surg. 2004, 13, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, A.; Troelsen, A.; Ban, I. Predictors associated with nonunion and symptomatic malunion following non-operative treatment of displaced midshaft clavicle fractures—A systematic review of the literature. Int. Orthop. 2014, 38, 2543–2549. [Google Scholar] [CrossRef] [PubMed]
- Housner, J.A.; Kuhn, J.E. Clavicle fractures: Individualizing treatment for fracture type. Physician Sportsmed. 2003, 31, 30–36. [Google Scholar] [CrossRef]
- Lenza, M.; Faloppa, F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst. Rev. 2016, 12, Cd007121. [Google Scholar] [CrossRef]
- Onizuka, N.; Anderson, J.P.; Gilbertson, J.A.; MacCormick, L.M.; Cole, P.A. Displacement of diaphyseal clavicle fractures related to patient position and progressive displacement in the peri-injury period. J. Shoulder Elb. Surg. 2018, 27, 667–673. [Google Scholar] [CrossRef]
- Stegeman, S.A.; Fernandes, N.C.; Krijnen, P.; Schipper, I.B. Online radiographic survey of midshaft clavicular fractures: No consensus on treatment for displaced fractures. Acta Orthop. Belg. 2014, 80, 161–165. [Google Scholar]
- van der Meijden, O.A.; Gaskill, T.R.; Millett, P.J. Treatment of clavicle fractures: Current concepts review. J. Shoulder Elb. Surg. 2012, 21, 423–429. [Google Scholar] [CrossRef]
- Marsh, J.L.; Slongo, T.F.; Agel, J.; Broderick, J.S.; Creevey, W.; DeCoster, T.A.; Prokuski, L.; Sirkin, M.S.; Ziran, B.; Henley, B.; et al. Fracture and dislocation classification compendium—2007: Orthopaedic Trauma Association classification, database and outcomes committee. J. Orthop. Trauma 2007, 21 (Suppl. S10), S1–S133. [Google Scholar] [CrossRef]
- Woltz, S.; Stegeman, S.A.; Krijnen, P.; van Dijkman, B.A.; van Thiel, T.P.; Schep, N.W.; de Rijcke, P.A.; Frolke, J.P.; Schipper, I.B. Plate Fixation Compared with Nonoperative Treatment for Displaced Midshaft Clavicular Fractures: A Multicenter Randomized Controlled Trial. J. Bone Jt. Surg. Am. Vol. 2017, 99, 106–112. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Louviere, J.J.; Hensher, D.A.; Swait, J.D. Stated Choice Methods: Analysis and Applications; Cambridge University Press: Cambridge, UK, 2000. [Google Scholar]
- Hill, J.M.; McGuire, M.H.; Crosby, L.A. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J. Bone Jt. Surg. Br. Vol. 1997, 79, 537–539. [Google Scholar] [CrossRef]
- Kirmani, S.J.; Pillai, S.K.; Madegowda, B.R.; Shahane, S.A. Vertical fragment in adult midshaft clavicle fractures: An indicator for surgical intervention. Orthopedics 2009, 32, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, K.J.; Remes, V.; Pajarinen, J.; Savolainen, V.; Bjorkenheim, J.M.; Paavola, M. Sling compared with plate osteosynthesis for treatment of displaced midshaft clavicular fractures: A randomized clinical trial. J. Bone Jt. Surg. Am. Vol. 2012, 94, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, G.S.d.L.; Tamaoki, M.J.S.; Dragone, B.; Utino, A.Y.; Netto, N.A.; Matsumoto, M.H.; Matsunaga, F.T. Correlation of the degree of clavicle shortening after non-surgical treatment of midshaft fractures with upper limb function. BMC Musculoskel. Disord. 2015, 16, 151. [Google Scholar] [CrossRef] [PubMed]
- Fuglesang, H.F.S.; Flugsrud, G.B.; Randsborg, P.-H.; Stavem, K.; Utvåg, S.E. Radiological and functional outcomes 2.7 years following conservatively treated completely displaced midshaft clavicle fractures. Arch. Orthop. Trauma Surg. 2016, 136, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Murray, I.R.; Foster, C.J.; Eros, A.; Robinson, C.M. Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. J. Bone Jt. Surg. Am. Vol. 2013, 95, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, B.P.; McLaren, A.; Richardson, M.; McLemore, R. Clavicular length: The assumption of symmetry. Orthopedics 2013, 36, e343–e347. [Google Scholar] [CrossRef][Green Version]
- De Giorgi, S.; Notarnicola, A.; Tafuri, S.; Solarino, G.; Moretti, L.; Moretti, B. Conservative treatment of fractures of the clavicle. BMC Res. Notes 2011, 4, 333. [Google Scholar] [CrossRef]
- Andermahr, J.; Jubel, A.; Elsner, A.; Prokop, A.; Tsikaras, P.; Jupiter, J.; Koebke, J. Malunion of the clavicle causes significant glenoid malposition: A quantitative anatomic investigation. Surg. Radiol. Anat. SRA 2006, 28, 447–456. [Google Scholar] [CrossRef]
- Hillen, R.J.; Burger, B.J.; Poll, R.G.; van Dijk, C.N.; Veeger, D.H. The effect of experimental shortening of the clavicle on shoulder kinematics. Clin. Biomech. (BristolAvon) 2012, 27, 777–781. [Google Scholar] [CrossRef]
- Su, W.R.; Chen, W.L.; Chen, R.H.; Hong, C.K.; Jou, I.M.; Lin, C.L. Evaluation of three-dimensional scapular kinematics and shoulder function in patients with short malunion of clavicle fractures. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2016, 21, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Lazarides, S.; Zafiropoulos, G. Conservative treatment of fractures at the middle third of the clavicle: The relevance of shortening and clinical outcome. J. Shoulder Elb. Surg. 2006, 15, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Heuer, H.J.; Boykin, R.E.; Petit, C.J.; Hardt, J.; Millett, P.J. Decision-making in the treatment of diaphyseal clavicle fractures: Is there agreement among surgeons? Results of a survey on surgeons’ treatment preferences. J. Shoulder Elb. Surg. 2014, 23, e23–e33. [Google Scholar] [CrossRef] [PubMed]
- Lenza, M.; Taniguchi, L.F.P.; Ferretti, M. Figure-of-eight bandage versus arm sling for treating middle-third clavicle fractures in adults: Study protocol for a randomised controlled trial. Trials 2016, 17, 229. [Google Scholar] [CrossRef] [PubMed]
- Ersen, A.; Atalar, A.C.; Birisik, F.; Saglam, Y.; Demirhan, M. Comparison of simple arm sling and figure of eight clavicular bandage for midshaft clavicular fractures: A randomised controlled study. Bone Jt. J. 2015, 97-b, 1562–1565. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Enrolled (122) | |
|---|---|
| Age, mean (SD) Median (range) | 37 (12.7) 38 (62–18) |
| Sex, Female (%) Male (%) | 19 (15.6) 103 (84.4) |
| Type of fractures (FT), number (%) A1 A2 A3 B1 B2 B3 | 9 (7.4) 31 (25.4) 12 (9.8) 10 (8.2) 23 (18.9) 37 (30.3) |
| Type of fractures (FT), number (%) A B | 52 (42.6) 70 (57.4) |
| Fracture healed within 12 weeks, number (%) Delayed union Nonunion | 81 (66.4) 24 (19.7) 17 (13.9) |
| Initial shortening % (IS), median (range) | 0 (12–0) |
| Residual shortening % (RS), median (range) | 0 (12–0) |
| Initial displacement % (ID), median (range) | 114.5 (230–16) |
| Residual displacement % (RD), median (range) | 100 (185–10) |
| Variable | Healed Fracture (81/122) | Delayed Union (24/122) | Nonunion (17/122) | p-Value (Kruskal–Wallis) |
|---|---|---|---|---|
| Age, mean (SD) Median (range) | 37.4 (11.7) 38 (61–18) | 36.2 (14.5) 36.5 (62–18) | 39.5 (14.5) 38 (60–18) | 0.720 |
| Type of fracture, % (number/total n =122) A1 A2 A3 B1 B2 B3 | 66.7 (6/9) 67.7 (21/31) 25 (3/12) 60 (6/10) 86.7 (20/23) 67.6 (25/37) | 11.1 (1/9) 19.4 (6/31) 33.3 (4/12) 30 (3/10) 8.7 (2/23) 21.6 (8/37) | 22.2 (2/9) 12.9 (4/31) 41.7 (5/12) 10 (1/10) 4.3 (1/23) 10.8 (4/37) | 0.494 |
| Type of fracture (FT), % (number/total n =122) A B | 57.7 (30/52) 72.8 (51/70) | 21.15 (11/52) 18.6 (13/70) | 21.15 (11/52) 8.6 (6/70) | χ2 0.10 |
| Initial shortening % (IS), median (range) | 0 (12–0) | 3.85 (11–0) | 2 (10–0) | 0.15 |
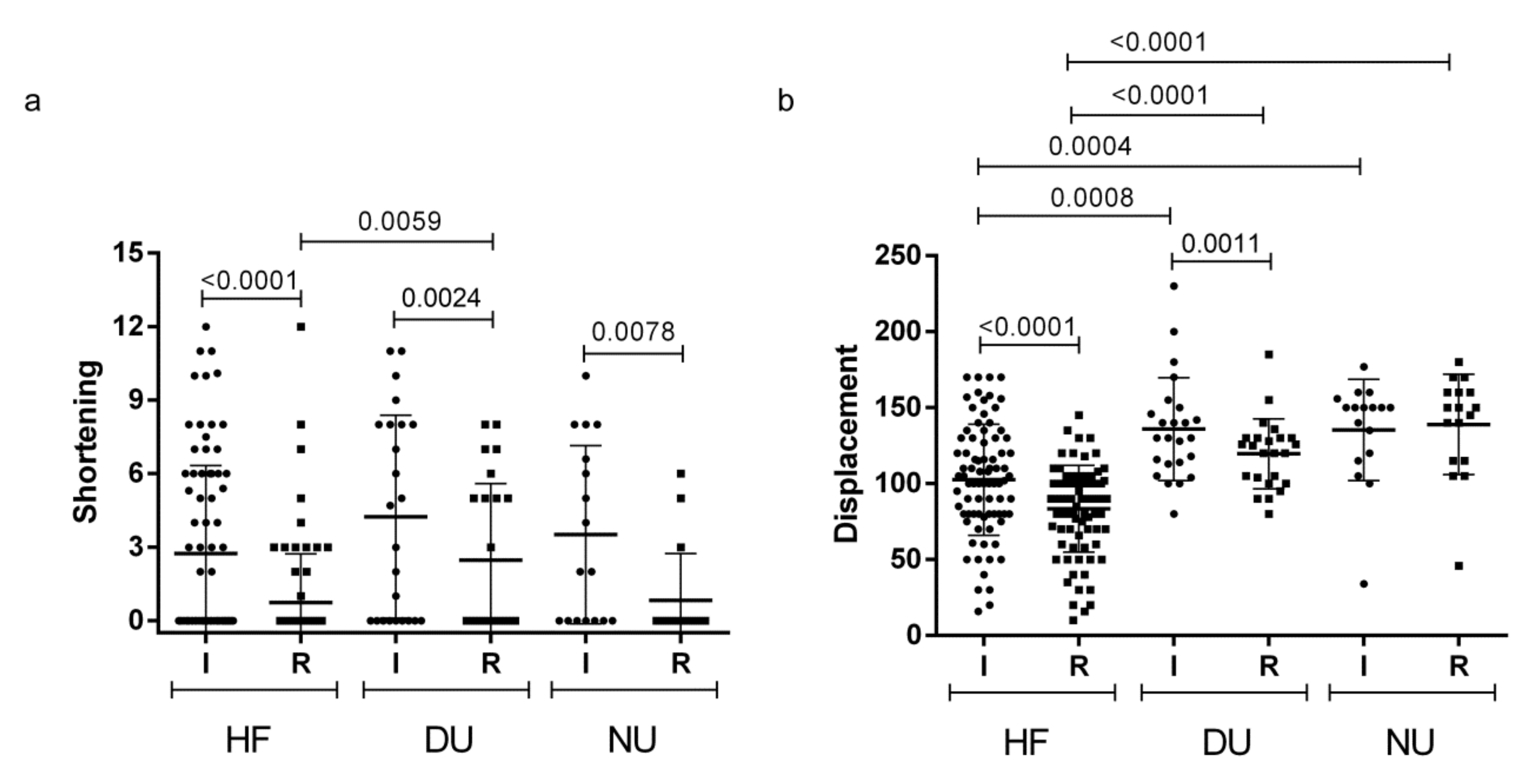
| Residual shortening % (RS), median (range) | 0 (12–0) | 0 (8–0) | 0 (6–0) | 0.014 * 0.0059 § 1 # 0.06571 |
| Initial displacement % (ID), median (range) | 102 (170–16) | 130 (230–80) | 150 (177–34) | <0.0001 * 0.0008 § 0.0004 # 0.890 |
| Residual displacement % (RD), median (range) | 90 (145–10) | 122.5 (185–80) | 150 (180–46) | <0.0001 * <0.0000 § <0.0000 # 0.2425 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tagliapietra, J.; Belluzzi, E.; Biz, C.; Angelini, A.; Fantoni, I.; Scioni, M.; Bolzan, M.; Berizzi, A.; Ruggieri, P. Midshaft Clavicle Fractures Treated Nonoperatively Using Figure-of-Eight Bandage: Are Fracture Type, Shortening, and Displacement Radiographic Predictors of Failure? Diagnostics 2020, 10, 788. https://doi.org/10.3390/diagnostics10100788
Tagliapietra J, Belluzzi E, Biz C, Angelini A, Fantoni I, Scioni M, Bolzan M, Berizzi A, Ruggieri P. Midshaft Clavicle Fractures Treated Nonoperatively Using Figure-of-Eight Bandage: Are Fracture Type, Shortening, and Displacement Radiographic Predictors of Failure? Diagnostics. 2020; 10(10):788. https://doi.org/10.3390/diagnostics10100788
Chicago/Turabian StyleTagliapietra, Jacopo, Elisa Belluzzi, Carlo Biz, Andrea Angelini, Ilaria Fantoni, Manuela Scioni, Mario Bolzan, Antonio Berizzi, and Pietro Ruggieri. 2020. "Midshaft Clavicle Fractures Treated Nonoperatively Using Figure-of-Eight Bandage: Are Fracture Type, Shortening, and Displacement Radiographic Predictors of Failure?" Diagnostics 10, no. 10: 788. https://doi.org/10.3390/diagnostics10100788
APA StyleTagliapietra, J., Belluzzi, E., Biz, C., Angelini, A., Fantoni, I., Scioni, M., Bolzan, M., Berizzi, A., & Ruggieri, P. (2020). Midshaft Clavicle Fractures Treated Nonoperatively Using Figure-of-Eight Bandage: Are Fracture Type, Shortening, and Displacement Radiographic Predictors of Failure? Diagnostics, 10(10), 788. https://doi.org/10.3390/diagnostics10100788