The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis at Baseline
3.2. Surgical Parameters
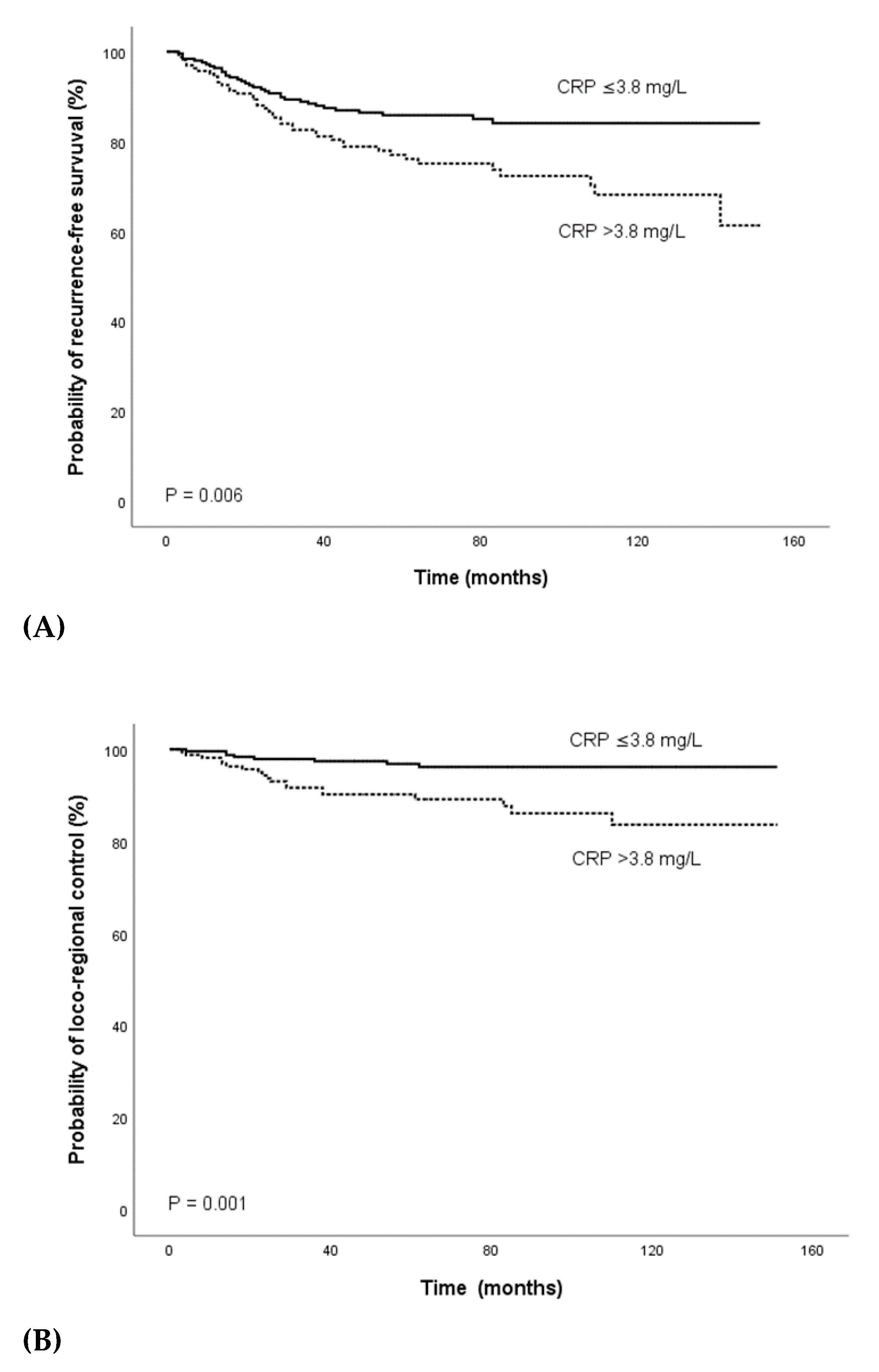
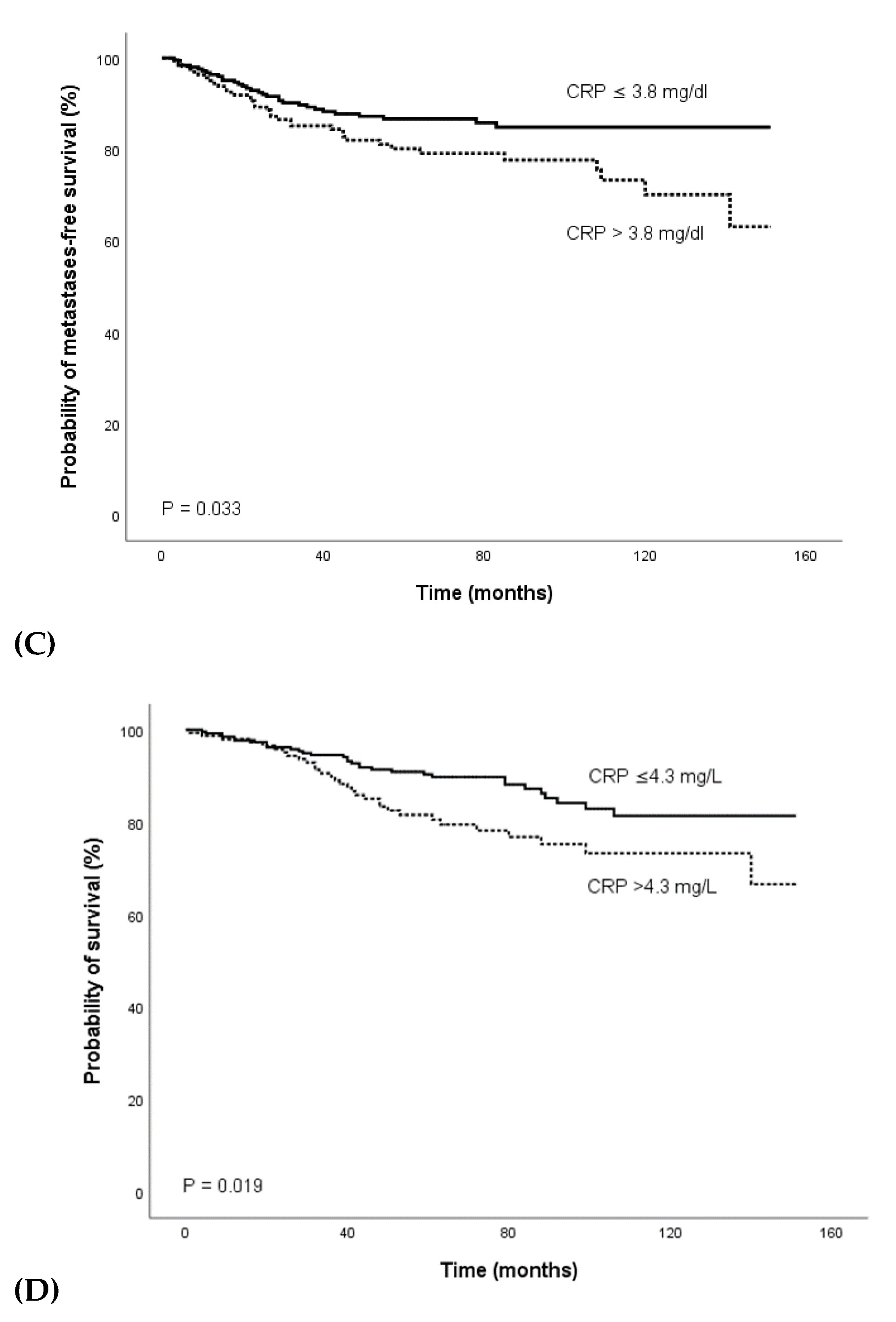
3.3. Outcome
3.4. Predictors of Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Neoadjuvant radiochemotherapy with subsequent surgical resection | Metastatic disease (n = 52) |
| Secondary malignancies (n = 60) | |
| No surgical resection (n = 4) | |
| No concurrent chemotherapy (n = 1) |
References
- Saad El Din, K.; Loree, J.M.; Sayre, E.C.; Gill, S.; Brown, C.J.; Dau, H.; De Vera, M.A. Trends in the epidemiology of young-onset colorectal cancer: A worldwide systematic review. BMC Cancer 2020, 20, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoffel, E.M.; Murphy, C.C. Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults. Gastroenterology 2020, 158, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rodel, C.; Cervantes, A.; Arnold, D.; Committee, E.G. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2018, 16, 874–901. [Google Scholar] [CrossRef] [Green Version]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. German Rectal Cancer Study, G., Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [Green Version]
- Crane, C.H.; Skibber, J.M.; Feig, B.W.; Vauthey, J.N.; Thames, H.D.; Curley, S.A.; Rodriguez-Bigas, M.A.; Wolff, R.A.; Ellis, L.M.; Delclos, M.E.; et al. Response to preoperative chemoradiation increases the use of sphincter-preserving surgery in patients with locally advanced low rectal carcinoma. Cancer 2003, 97, 517–524. [Google Scholar] [CrossRef]
- Wagman, R.; Minsky, B.D.; Cohen, A.M.; Guillem, J.G.; Paty, P.P. Sphincter preservation in rectal cancer with preoperative radiation therapy and coloanal anastomosis: Long term follow-up. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 51–57. [Google Scholar] [CrossRef]
- Partl, R.; Magyar, M.; Hassler, E.; Langsenlehner, T.; Kapp, K.S. Clinical parameters predictive for sphincter-preserving surgery and prognostic outcome in patients with locally advanced low rectal cancer. Radiat. Oncol. 2020, 15, 99. [Google Scholar] [CrossRef]
- Spolverato, G.; Pucciarelli, S.; Bertorelle, R.; De Rossi, A.; Nitti, D. Predictive factors of the response of rectal cancer to neoadjuvant radiochemotherapy. Cancers 2011, 3, 2176–2194. [Google Scholar] [CrossRef] [Green Version]
- Pepys, M.B.; Baltz, M.L. Acute phase proteins with special reference to C-reactive protein and related proteins (pentaxins) and serum amyloid A protein. Adv. Immunol. 1983, 34, 141–212. [Google Scholar]
- Achyut, B.R.; Bader, D.A.; Robles, A.I.; Wangsa, D.; Harris, C.C.; Ried, T.; Yang, L. Inflammation-mediated genetic and epigenetic alterations drive cancer development in the neighboring epithelium upon stromal abrogation of TGF-beta signaling. PLoS Genet. 2013, 9, e1003251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Landskron, G.; De la Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic Inflammation and Cytokines in the Tumor Microenvironment. J. Immunol. Res. 2014, 2014, 149185. [Google Scholar] [CrossRef] [Green Version]
- Kawanami, D.; Maemura, K.; Takeda, N.; Harada, T.; Nojiri, T.; Saito, T.; Manabe, I.; Imai, Y.; Nagai, R. C-reactive protein induces VCAM-1 gene expression through NF-kappaB activation in vascular endothelial cells. Atherosclerosis 2006, 185, 39–46. [Google Scholar] [CrossRef]
- St. Hill, C.A. Interactions between endothelial selectins and cancer cells regulate metastasis. Front. Biosci. 2011, 16, 3233–3251. [Google Scholar] [CrossRef]
- Salama, P.; Phillips, M.; Grieu, F.; Morris, M.; Zeps, N.; Joseph, D.; Platell, C.; Iacopetta, B. Tumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancer. J. Clin. Oncol. 2009, 27, 186–192. [Google Scholar] [CrossRef]
- Ling, A.; Edin, S.; Wikberg, M.L.; Oberg, A.; Palmqvist, R. The intratumoural subsite and relation of CD8(+) and FOXP3(+) T lymphocytes in colorectal cancer provide important prognostic clues. Br. J. Cancer 2014, 110, 2551–2559. [Google Scholar] [CrossRef] [Green Version]
- Gunnarsson, U.; Strigard, K.; Edin, S.; Gkekas, I.; Mustonen, H.; Kaprio, T.; Bockelman, C.; Hagstrom, J.; Palmqvist, R.; Haglund, C. Association between local immune cell infiltration, mismatch repair status and systemic inflammatory response in colorectal cancer. J. Transl. Med. 2020, 18, 178. [Google Scholar] [CrossRef] [Green Version]
- Knittelfelder, O.; Delago, D.; Jakse, G.; Lukasiak, K.; Thurner, E.M.; Thurnher, D.; Pichler, M.; Renner, W.; Stranzl-Lawatsch, H.; Langsenlehner, T. The Pre-Treatment C-Reactive Protein Represents a Prognostic Factor in Patients with Oral and Oropharyngeal Cancer Treated with Radiotherapy. Cancers 2020, 12, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagaoka, S.; Yoshida, T.; Akiyoshi, J.; Akiba, J.; Torimura, T.; Adachi, H.; Kurogi, J.; Tajiri, N.; Inoue, K.; Niizeki, T.; et al. Serum C-reactive protein levels predict survival in hepatocellular carcinoma. Liver Int. 2007, 27, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Pine, S.R.; Mechanic, L.E.; Enewold, L.; Chaturvedi, A.K.; Katki, H.A.; Zheng, Y.L.; Bowman, E.D.; Engels, E.A.; Caporaso, N.E.; Harris, C.C. Increased levels of circulating interleukin 6, interleukin 8, C-reactive protein, and risk of lung cancer. J. Natl. Cancer Inst. 2011, 103, 1112–1122. [Google Scholar] [CrossRef] [PubMed]
- Toiyama, Y.; Inoue, Y.; Saigusa, S.; Kawamura, M.; Kawamoto, A.; Okugawa, Y.; Hiro, J.; Tanaka, K.; Mohri, Y.; Kusunoki, M. C-reactive protein as predictor of recurrence in patients with rectal cancer undergoing chemoradiotherapy followed by surgery. Anticancer Res. 2013, 33, 5065–5074. [Google Scholar]
- Buijsen, J.; van Stiphout, R.G.; Menheere, P.P.; Lammering, G.; Lambin, P. Blood biomarkers are helpful in the prediction of response to chemoradiation in rectal cancer: A prospective, hypothesis driven study on patients with locally advanced rectal cancer. Radiother. Oncol. 2014, 111, 237–242. [Google Scholar] [CrossRef]
- Sobin, L.H.; Wittekind, C. TNM Classification of Malignant Tumours, 6th ed.; Wiley: Lissabon, Portugal, 2002. [Google Scholar]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; John Wiley & Sons: New Jersey, NJ, USA, 2010. [Google Scholar]
- Thurner, E.M.; Krenn-Pilko, S.; Langsenlehner, U.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The association of an elevated plasma fibrinogen level with cancer-specific and overall survival in prostate cancer patients. World J. Urol. 2015, 33, 1467–1473. [Google Scholar] [CrossRef]
- Holzinger, D.; Danilovic, I.; Seemann, R.; Kornek, G.; Engelmann, J.; Pillerstorff, R.; Holawe, S.; Psyrri, A.; Erovic, B.M.; Farwell, G.; et al. Prognostic Impact of Pretreatment Plasma Fibrinogen in Patients with Locally Advanced Oral and Oropharyngeal Cancer. PLoS ONE 2016, 11, e0158697. [Google Scholar] [CrossRef]
- Groblewska, M.; Mroczko, B.; Wereszczynska-Siemiatkowska, U.; Kedra, B.; Lukaszewicz, M.; Baniukiewicz, A.; Szmitkowski, M. Serum interleukin 6 (IL-6) and C-reactive protein (CRP) levels in colorectal adenoma and cancer patients. Clin. Chem. Lab. Med. 2008, 46, 1423–1428. [Google Scholar] [CrossRef]
- Soucek, L.; Lawlor, E.R.; Soto, D.; Shchors, K.; Swigart, L.B.; Evan, G.I. Mast cells are required for angiogenesis and macroscopic expansion of Myc-induced pancreatic islet tumors. Nat. Med. 2007, 13, 1211–1218. [Google Scholar] [CrossRef]
- Sparmann, A.; Bar-Sagi, D. Ras-induced interleukin-8 expression plays a critical role in tumor growth and angiogenesis. Cancer Cell. 2004, 6, 447–458. [Google Scholar] [CrossRef] [Green Version]
- Balkwill, F. Cancer and the chemokine network. Nat. Rev. Cancer 2004, 4, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Kuper, H.; Adami, H.O.; Trichopoulos, D. Infections as a major preventable cause of human cancer. J. Intern. Med. 2000, 248, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Wahl, L.M.; Kleinman, H.K. Tumor-associated macrophages as targets for cancer therapy. J. Natl. Cancer Inst. 1998, 90, 1583–1584. [Google Scholar] [CrossRef] [Green Version]
- Asegaonkar, S.B.; Asegaonkar, B.N.; Takalkar, U.V.; Advani, S.; Thorat, A.P. C-Reactive Protein and Breast Cancer: New Insights from Old Molecule. Int. J. Breast Cancer 2015, 2015, 145647. [Google Scholar] [CrossRef] [Green Version]
- Okugawa, Y.; Toiyama, Y.; Fujikawa, H.; Ide, S.; Yamamoto, A.; Omura, Y.; Yin, C.; Kusunoki, K.; Kusunoki, Y.; Yasuda, H.; et al. Prognostic Potential of Lymphocyte-C-Reactive Protein Ratio in Patients with Rectal Cancer Receiving Preoperative Chemoradiotherapy. J. Gastrointest. Surg. 2020. [Google Scholar] [CrossRef]
- Zhou, Q.P.; Li, X.J. C-Reactive Protein to Albumin Ratio in Colorectal Cancer: A Meta-Analysis of Prognostic Value. Dose Response 2019, 17, 1559325819889814. [Google Scholar] [CrossRef]
- Egenvall, M.; Morner, M.; Martling, A.; Gunnarsson, U. Prediction of outcome after curative surgery for colorectal cancer: Preoperative haemoglobin, C-reactive protein and albumin. Colorectal Dis. 2018, 20, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Nozoe, T.; Matsumata, T.; Kitamura, M.; Sugimachi, K. Significance of preoperative elevation of serum C-reactive protein as an indicator for prognosis in colorectal cancer. Am. J. Surg. 1998, 176, 335–338. [Google Scholar] [CrossRef]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Horie, T.; Kubota, K. Inflammation-based prognostic score is a novel predictor of postoperative outcome in patients with colorectal cancer. Ann. Surg. 2007, 246, 1047–1051. [Google Scholar] [CrossRef] [PubMed]
- Dreanic, J.; Maillet, M.; Dhooge, M.; Mir, O.; Brezault, C.; Goldwasser, F.; Chaussade, S.; Coriat, R. Prognostic value of the Glasgow Prognostic Score in metastatic colorectal cancer in the era of anti-EGFR therapies. Med. Oncol. 2013, 30, 656. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Huang, J.; Zhu, J.; Shen, H. Elevated pre-treatment levels of high sensitivity C-reactive protein as a potential prognosticator in patients with colorectal cancer. Exp. Med. 2013, 6, 1369–1374. [Google Scholar] [CrossRef] [PubMed]
- Toiyama, Y.; Fujikawa, H.; Koike, Y.; Saigusa, S.; Inoue, Y.; Tanaka, K.; Mohri, Y.; Miki, C.; Kusunoki, M. Evaluation of preoperative C-reactive protein aids in predicting poor survival in patients with curative colorectal cancer with poor lymph node assessment. Oncol. Lett. 2013, 5, 1881–1888. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.R.; Han, Y.D.; Min, B.S. C-Reactive Protein Level Predicts Survival Outcomes in Rectal Cancer Patients Undergoing Total Mesorectal Excision After Preoperative Chemoradiation Therapy. Ann. Surg. Oncol. 2018, 25, 3898–3905. [Google Scholar] [CrossRef]
- Giessen, C.; Nagel, D.; Glas, M.; Spelsberg, F.; Lau-Werner, U.; Modest, D.P.; Michl, M.; Heinemann, V.; Stieber, P.; Schulz, C. Evaluation of preoperative serum markers for individual patient prognosis in stage I-III rectal cancer. Tumour Biol. 2014, 35, 10237–10248. [Google Scholar] [CrossRef]
- Nikberg, M.; Kindler, C.; Chabok, A.; Letocha, H.; Shetye, J.; Smedh, K. Circumferential resection margin as a prognostic marker in the modern multidisciplinary management of rectal cancer. Dis. Colon Rectum 2015, 58, 275–282. [Google Scholar] [CrossRef]
- Brouwer, N.P.M.; Stijns, R.C.H.; Lemmens, V.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Futterer, J.J.; Tanis, P.J.; Verhoeven, R.H.A.; de Wilt, J.H.W. Clinical lymph node staging in colorectal cancer; a flip of the coin? Eur. J. Surg. Oncol. 2018, 44, 1241–1246. [Google Scholar] [CrossRef]
- Black, S.; Kushner, I.; Samols, D. C-reactive Protein. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef] [Green Version]
- Nimptsch, K.; Aleksandrova, K.; Boeing, H.; Janke, J.; Lee, Y.-A.; Jenab, M.; Bueno-de-Mesquita, H.B.; Jansen, E.H.J.M.; Tsilidis, K.K.; Trichopoulou, A.; et al. Association of CRP genetic variants with blood concentrations of C-reactive protein and colorectal cancer risk. Int. J. Cancer 2015, 136, 1181–1192. [Google Scholar] [CrossRef] [Green Version]
- Perkins, N.D. Oncogenes, tumor suppressors and p52 NF-kappaB. Oncogene 2003, 22, 7553–7556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Wezeman, M.; Zhang, X.; Lin, P.; Wang, M.; Qian, J.; Wan, B.; Kwak, L.W.; Yu, L.; Yi, Q. Human C-reactive protein binds activating Fcgamma receptors and protects myeloma tumor cells from apoptosis. Cancer Cell 2007, 12, 252–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, K. C-reactive protein (CRP)-lowering agents. Cardiovasc. Drug Rev. 2006, 24, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.A.; Cole, B.F.; Sandler, R.S.; Haile, R.W.; Ahnen, D.; Bresalier, R.; McKeown-Eyssen, G.; Summers, R.W.; Rothstein, R.; Burke, C.A.; et al. A randomized trial of aspirin to prevent colorectal adenomas. N. Engl. J. Med. 2003, 348, 891–899. [Google Scholar] [CrossRef]
- Benamouzig, R.; Deyra, J.; Martin, A.; Girard, B.; Jullian, E.; Piednoir, B.; Couturier, D.; Coste, T.; Little, J.; Chaussade, S. Daily soluble aspirin and prevention of colorectal adenoma recurrence: One-year results of the APACC trial. Gastroenterology 2003, 125, 328–336. [Google Scholar] [CrossRef]
- Kashfi, K. Anti-inflammatory agents as cancer therapeutics. Adv. Pharm. 2009, 57, 31–89. [Google Scholar]
- Zhang, Z.; Chen, F.; Shang, L. Advances in antitumor effects of NSAIDs. Cancer Manag. Res. 2018, 10, 4631–4640. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.K.; Oza, A.M.; Siu, L.L. The statins as anticancer agents. Clin. Cancer Res. 2003, 9, 10–19. [Google Scholar]
- Armstrong, D.; Raissouni, S.; Price Hiller, J.; Mercer, J.; Powell, E.; MacLean, A.; Jiang, M.; Doll, C.; Goodwin, R.; Batuyong, E.; et al. Predictors of Pathologic Complete Response After Neoadjuvant Treatment for Rectal Cancer: A Multicenter Study. Clin. Colorectal Cancer 2015, 14, 291–295. [Google Scholar] [CrossRef]
- Ihara, K.; Yamaguchi, S.; Shida, Y.; Ogata, H.; Domeki, Y.; Okamoto, K.; Nakajima, M.; Sasaki, K.; Tsuchioka, T.; Kato, H. Poor nutritional status before and during chemotherapy leads to worse prognosis in unresectable advanced or recurrent colorectal cancer. Int. Surg. 2015, 7, 58543–58552. [Google Scholar] [CrossRef] [Green Version]
- Blauwhoff-Buskermolen, S.; Versteeg, K.S.; de van der Schueren, M.A.; den Braver, N.R.; Berkhof, J.; Langius, J.A.; Verheul, H.M. Loss of Muscle Mass During Chemotherapy Is Predictive for Poor Survival of Patients With Metastatic Colorectal Cancer. J. Clin. Oncol. 2016, 34, 1339–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, Y.J.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Kang, J. Prognostic impact of persistent lower neutrophil-to-lymphocyte ratio during preoperative chemoradiotherapy in locally advanced rectal cancer patients: A propensity score matching analysis. PLoS ONE 2019, 14, e0214415. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Huh, J.W.; Lee, W.Y.; Yun, S.H.; Kim, H.C.; Cho, Y.B.; Park, Y.A.; Shin, J.K. Prognostic value of serum inflammatory markers in colorectal cancer. Int. J. Colorectal Dis. 2020, 35, 1211–1219. [Google Scholar] [CrossRef] [PubMed]


| Criterion | Value |
|---|---|
| Number of patients | 423 |
| Sex | |
| Male Female | 279 (66.0%) 144 (34.0%) |
| Age; median (mean ± SD) | 66.00 (64.7 ± 11.0) |
| BMI; median (mean ± SD) | 26.1 (26.4 ± 4.40) |
| Co-morbidities | |
| Yes | 91 (21.5%) |
| No | 328 (77.5%) |
| Smoking status | |
| Former * or never Current | 357 (84.4%) 65 (15.4%) |
| Tumor site | |
| < 6 cm ab ano 6–18 cm ab ano | 235 (55.6%) 188 (44.4%) |
| Tumor grade | |
| G1/2 G3/4 | 396 (93.6%) 27 (6.4%) |
| Clinical tumor stage | |
| T1/2 ** T3 T4 | 20 (4.7%) 358 (84.6%) 45 (10.6%) |
| Clinical nodal involvement | |
| Yes No | 246 (58.2%) 177 (41.8%) |
| Clinical stage | |
| Stage II Stage III | 178 (42.1%) 245 (57.9%) |
| MRI-defined involvement of CRM *** | |
| Yes | 49 (11.6%) |
| No | 190 (44.9%) |
| Extramural venous involvement *** | |
| Yes | 2 (0.5%) |
| No | 235 (55.6%) |
| LDH, median (mean ± SD) | 174.0 (186.9 ± 56.5) |
| CEA, median (mean ± SD) | 3.3 (9.6 ± 44.6) |
| CA 19-9, median (mean ± SD) | 8.7 (26.7 ± 70.7) |
| CRP pre-treatment, median (mean ± SD) | 2.8 (7.7 ± 16.8) |
| CRP post-treatment, median (mean ± SD | 4.2 (7.5 ± 11.0) |
| Recurrence-Free Survival | Loco-Regional Control | Metastases-Free Survival | Overall Survival | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Criterion | HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| Sex | |||||||||
| Female Male | 1 0.906 (0.567–1.447) | 0.679 | 1 1.554 (0.657–3.675) | 0.316 | 1 0.840 (0.514–1.373) | 0.487 | 1 1.458 (0.836–2.543) | 0.184 | |
| Age (continuous) | 1.001 (0.980–1.022) | 0.914 | 0.995 (0.961–1.029) | 0.760 | 1.001 (0.979–1.023) | 0.934 | 1.039 (1.013–1.066) | 0.003 | |
| BMI (continuous) | 0.963 (0.903–1.027) | 0.249 | 0.954 (0.856–1.064) | 0.401 | 0.977 (0.914–1.044) | 0.488 | 1.000 (0.937–1.067) | 0.998 | |
| Co-morbidities | |||||||||
| No Yes | 0.982 (0.556–1.733) | 0.949 | 0.878 (0.332–2.322) | 0.794 | 1.155 (0.648–2.058) | 0.625 | 1.475 (0.845–2.575) | 0.172 | |
| Smoking status | |||||||||
| Former/never Current | 1 1.492 (0.847–2.629) | 0.166 | 1 1.724 (0.696–4.275) | 0.239 | 1 1.583 (0.878–2.855) | 0.127 | 1 0.751 (0.342–1.648) | 0.475 | |
| Tumor site | |||||||||
| < 6cm ab ano 6–18 cm ab ano | 1 0.981 (0.622–1.548) | 0.935 | 1 0.733 (0.335–1.600) | 0.435 | 1 1.143 (0.707–1.846) | 0.585 | 1 1.439 (0.876–2.362) | 0.150 | |
| Tumor grade | |||||||||
| G1/2 G3/4 | 1 0.793 (0.290–2.171) | 0.652 | 1 0.544 (0.074–4.012) | 0.551 | 1 0.669 (0.210–2.129) | 0.496 | 1 0.486 (0.119–1.989) | 0.316 | |
| Tumor stage | |||||||||
| T1/2 T3 T4 | 1 1.577 (0.385–6.462) 4.073 (0.930–7.828) | 0.527 0.062 | 1 n.a. * n.a. * | 0.943 0.939 | 1 1.441 (0.351–5.917) 3.209 (0.717–14.36) | 0.612 0.127 | 1 0.852 (0.266–2.733) 1.450 (0.392–5.362) | 0.788 0.578 | |
| Nodal involvement | |||||||||
| No Yes | 1 1.226 (0.770–1.952) | 0.390 | 1 1.837 (0.804–4.198) | 0.149 | 1 1.136 (0.697–1.851) | 0.610 | 1 0.997 (0.606–1.639) | 0.990 | |
| Clinical stage | |||||||||
| II III | 1 1.174 (0.739–1.863) | 0.497 | 1 1.563 (0.702–3.480) | 0.275 | 1 1.080 (0.665–1.756) | 0.756 | 1 1.012 (0.616–1.665) | 0.961 | |
| mrCRM | |||||||||
| No Yes | 1 2.082 (1.106–3.919) | 0.023 | 1 1.305 (0.428–3.978) | 0.639 | 1 2.089 (1.052–4.147) | 0.035 | 1 1.164 (0.507–2.669) | 0.721 | |
| EVMI | |||||||||
| No Yes | 1 n.a. * | 0.646 | 1 n.a. * | 0.777 | 1 n.a. * | 0.674 | 1 n.a. * | 0.664 | |
| LDH (continuous) | 1.002 (0.998–1.006) | 0.305 | 0.994 (0.985–1.003) | 0.219 | 1.003 (0.999–1.007) | 0.108 | 1.001 (0.996–1.005) | 0.758 | |
| CEA (continuous) | 1.005 (1.002–1.008) | <0.001 | 1.001 (0.993–1.010) | 0.767 | 1.006 (1.003–1.008) | <0.001 | 1.005 (1.002–1.008) | <0.001 | |
| CA 19-9 (continuous) | 1.002 (0.999–1.004) | 0.138 | 1.002 (0.997–1.006) | 0.527 | 1.002 (0.999–1.005) | 0.127 | 1.000 (0.996–1.004) | 0.918 | |
| Pre-nRCT CRP (continuous) | 1.015 (1.006–1.023) | <0.001 | 1.015 (1.004–1.027) | 0.009 | 1.014 (1.004–1.023) | 0.004 | 1.016 (1.007–1.024) | <0.001 | |
| Post-nRCT CRP (continuous) | 1.011 (0.993–1.030) | 0.227 | 1.020 (0.996–1.045) | 0.103 | 1.013 (0.995–1.032) | 0.160 | 1.001 (0.978–1.025) | 0.915 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Partl, R.; Lukasiak, K.; Thurner, E.-M.; Renner, W.; Stranzl-Lawatsch, H.; Langsenlehner, T. The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy. Diagnostics 2020, 10, 780. https://doi.org/10.3390/diagnostics10100780
Partl R, Lukasiak K, Thurner E-M, Renner W, Stranzl-Lawatsch H, Langsenlehner T. The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy. Diagnostics. 2020; 10(10):780. https://doi.org/10.3390/diagnostics10100780
Chicago/Turabian StylePartl, Richard, Katarzyna Lukasiak, Eva-Maria Thurner, Wilfried Renner, Heidi Stranzl-Lawatsch, and Tanja Langsenlehner. 2020. "The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy" Diagnostics 10, no. 10: 780. https://doi.org/10.3390/diagnostics10100780
APA StylePartl, R., Lukasiak, K., Thurner, E.-M., Renner, W., Stranzl-Lawatsch, H., & Langsenlehner, T. (2020). The Elevated Pre-Treatment C-Reactive Protein Predicts Poor Prognosis in Patients with Locally Advanced Rectal Cancer Treated with Neo-Adjuvant Radiochemotherapy. Diagnostics, 10(10), 780. https://doi.org/10.3390/diagnostics10100780