Prognostic Value of Severity Score Change for Septic Shock in the Emergency Room

Abstract
:1. Introduction
2. Materials and Methods
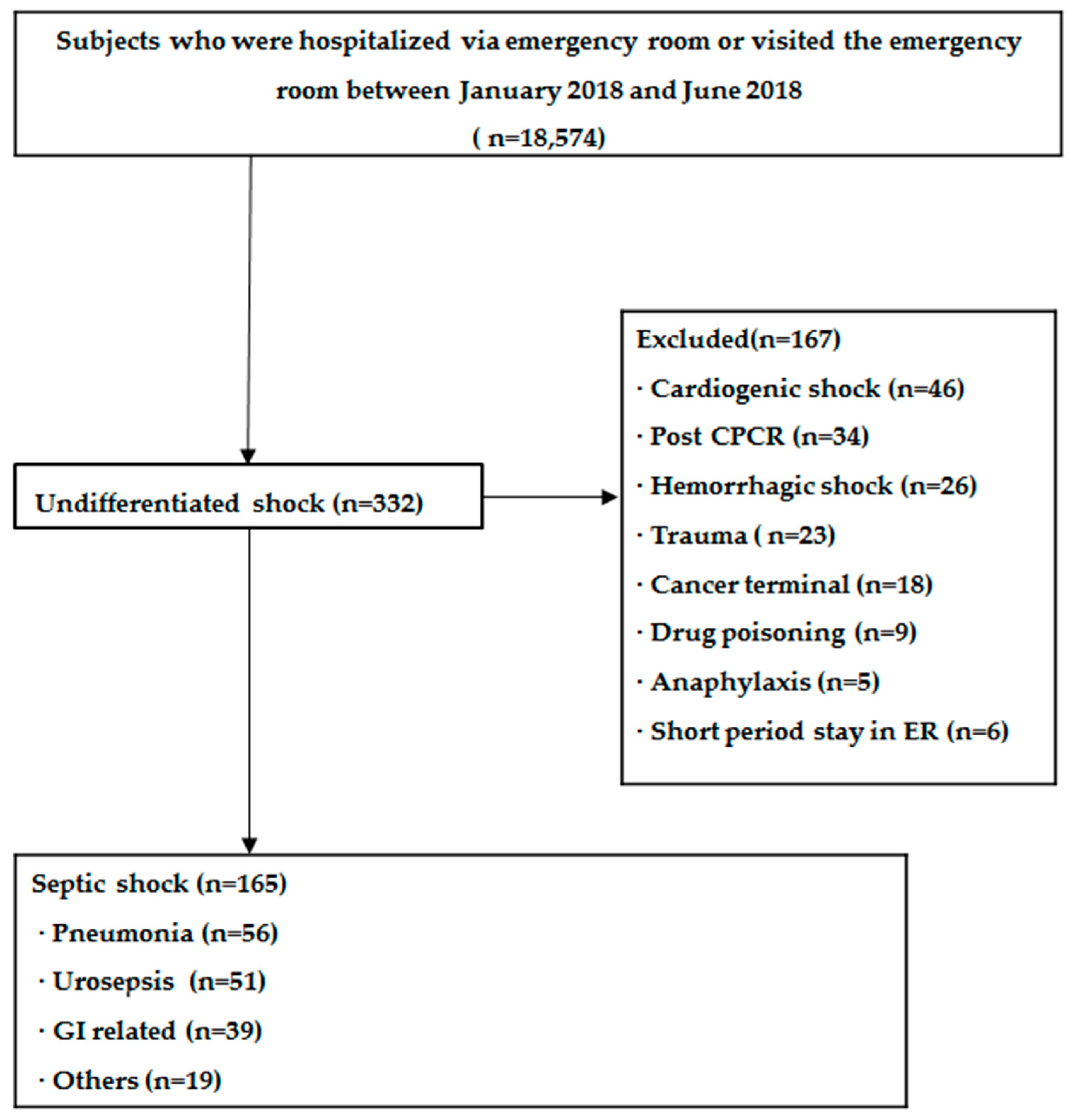
2.1. Patients
2.2. Scores and Outcome Assessment
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
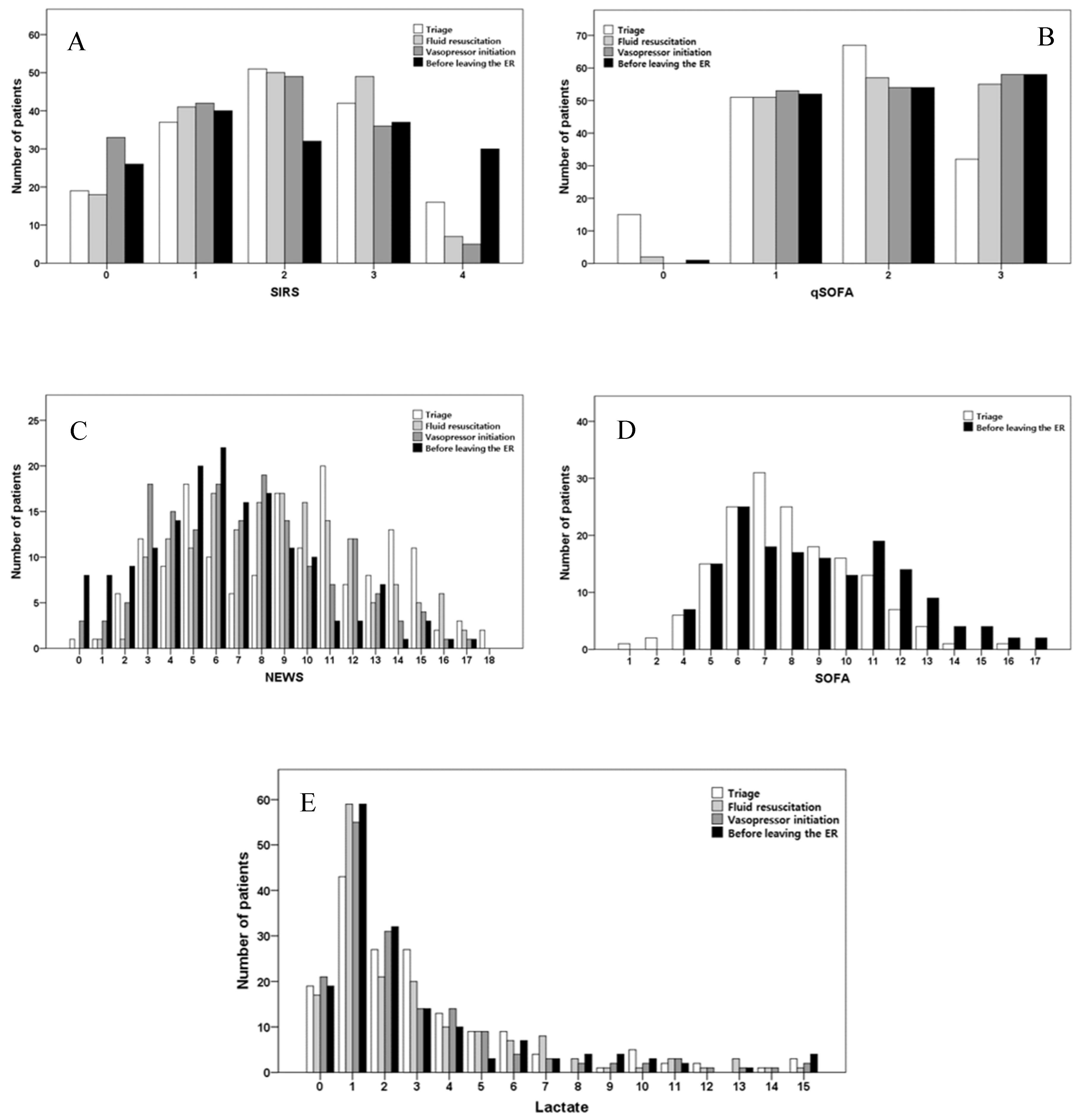
3.2. Distribution of Patients According to Severity Scores
3.3. Sequential Changes in Severity Indicators
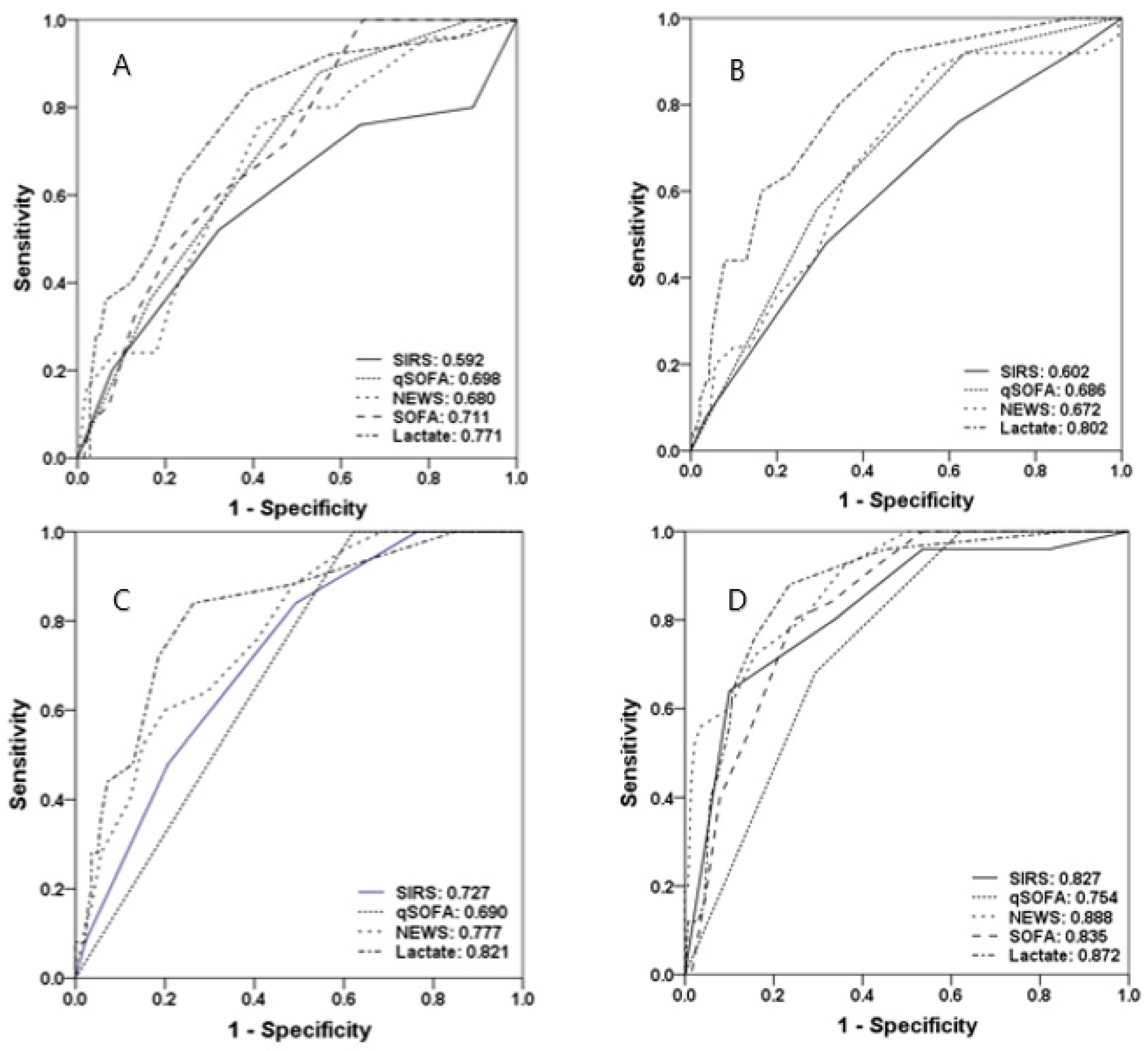
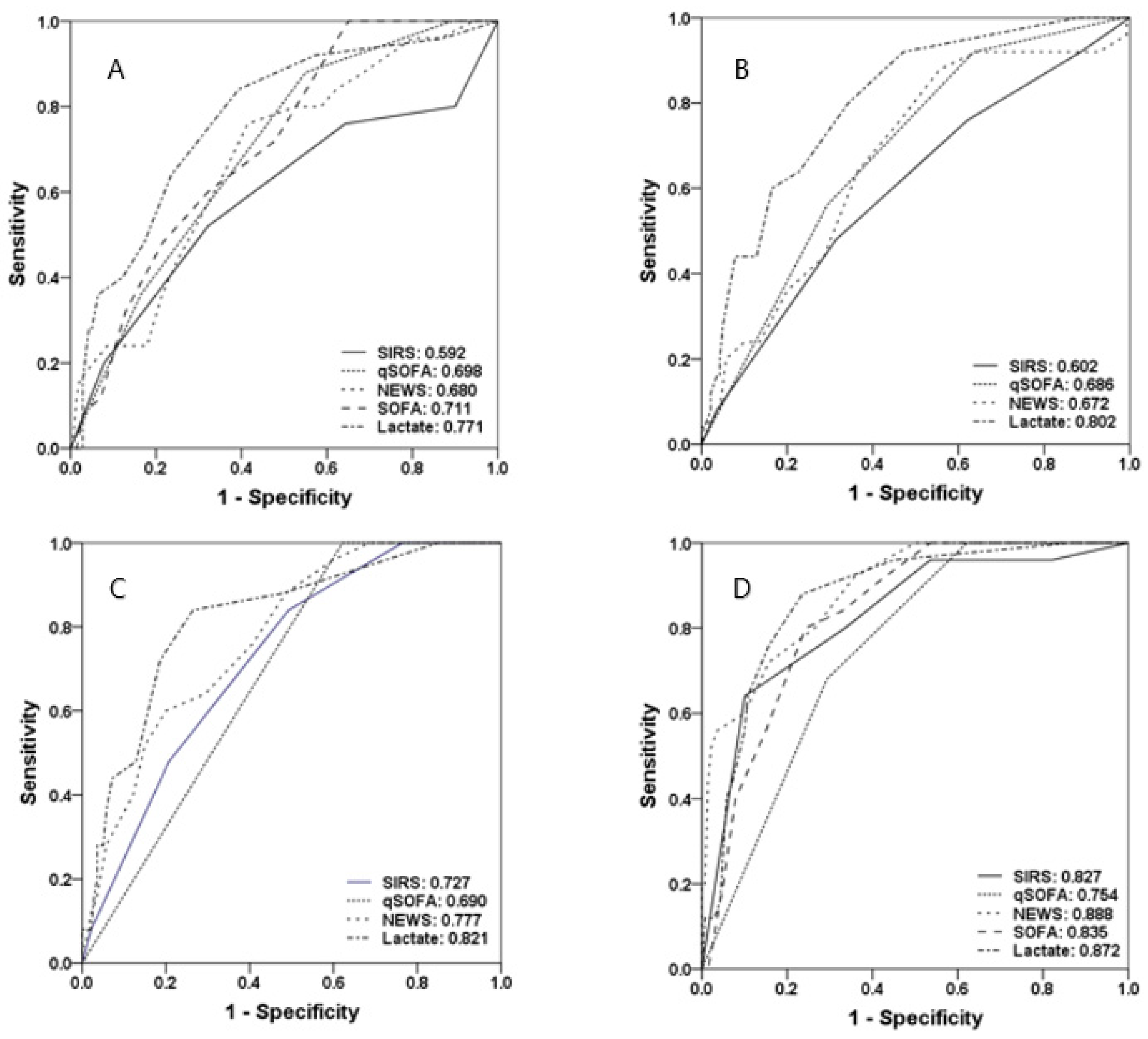
3.4. Predictive Values of Severity Scores and Lactate Levels for Mortality within Seven Days
3.5. Predictive Values of Severity Scores and Lactate Levels for In-Hospital Mortality, Mechanical Ventilation, and ICU Admission
3.6. Predictive Value of Maximum and Difference Value of Severity Score
3.7. Predictive Value of Combination of Severity Score and Lactate
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liu, V.; Escobar, G.J.; Greene, J.D.; Soule, J.; Whippy, A.; Angus, D.C.; Iwashyna, T.J. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014, 312, 90–92. [Google Scholar] [CrossRef] [Green Version]
- Churpek, M.M.; Yuen, T.C.; Winslow, C.; Robicsek, A.A.; Meltzer, D.O.; Gibbons, R.D.; Edelson, D.P. Multicenter development and validation of a risk stratification tool for ward patients. Am. J. Respir. Crit. Care Med. 2014, 190, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Escobar, G.J.; LaGuardia, J.C.; Turk, B.J.; Ragins, A.; Kipnis, P.; Draper, D. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J. Hosp. Med. 2012, 7, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Kause, J.; Smith, G.; Prytherch, D.; Parr, M.; Flabouris, A.; Hillman, K.; Intensive Care, S.; Australian and New Zealand Intensive Care Society Clinical Trials Group. A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom--the ACADEMIA study. Resuscitation 2004, 62, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Goulden, R.; Hoyle, M.C.; Monis, J.; Railton, D.; Riley, V.; Martin, P.; Martina, R.; Nsutebu, E. qSOFA, SIRS and NEWS for predicting inhospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg. Med. J. 2018, 35, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Baumann, B.M.; Greenwood, J.C.; Lewis, K.; Nuckton, T.J.; Darger, B.; Shofer, F.S.; Troeger, D.; Jung, S.Y.; Kilgannon, J.H.; Rodriguez, R.M. Combining qSOFA criteria with initial lactate levels: Improved screening of septic patients for critical illness. Am. J. Emerg. Med. 2020, 38, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Churpek, M.M.; Zadravecz, F.J.; Winslow, C.; Howell, M.D.; Edelson, D.P. Incidence and Prognostic Value of the Systemic Inflammatory Response Syndrome and Organ Dysfunctions in Ward Patients. Am. J. Respir. Crit. Care Med. 2015, 192, 958–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.L.; Martin, G.S.; Levy, M.M. qSOFA does not replace SIRS in the definition of sepsis. Crit. Care 2016, 20, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- William, B.; Albert, G.; Ball, C.; Bell, D.; Binks, R.; Durham, L.; Eddleston, J.; Edwards, N.; Evans, D.; Jones, M.; et al. National Early Warning Score (NEWS): Standardizing the Assessment of Acute Illness Severity in the NHS. Report of a Working Party; The Royal College of Physicians: London, UK, 2014. Available online: http://health.gov.ie/wp-content/uploads/2015/01/NEWSFull-ReportAugust2014.pdf.2013 (accessed on 23 September 2020).
- Liu, V.X.; Lu, Y.; Carey, K.A.; Gilbert, E.R.; Afshar, M.; Akel, M.; Shah, N.S.; Dolan, J.; Winslow, C.; Kipnis, P.; et al. Comparison of Early Warning Scoring Systems for Hospitalized Patients With and Without Infection at Risk for In-Hospital Mortality and Transfer to the Intensive Care Unit. JAMA Netw Open 2020, 3, e205191. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Quinten, V.M.; van Meurs, M.; Olgers, T.J.; Vonk, J.M.; Ligtenberg, J.J.M.; Ter Maaten, J.C. Repeated vital sign measurements in the emergency department predict patient deterioration within 72 hours: A prospective observational study. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, R.M.; Greenwood, J.C.; Nuckton, T.J.; Darger, B.; Shofer, F.S.; Troeger, D.; Jung, S.Y.; Speich, K.G.; Valencia, J.; Kilgannon, J.H.; et al. Comparison of qSOFA with current emergency department tools for screening of patients with sepsis for critical illness. Emerg. Med. J. 2018, 35, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.; Yoon, J.; Lee, J.B.; Jin, Y.; Jeong, T.; Park, B. Predictive value of the National Early Warning Score-Lactate for mortality and the need for critical care among general emergency department patients. J. Crit. Care 2016, 36, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Schulte-Hubbert, B.; Meiswinkel, N.; Kutschan, U.; Kolditz, M. Prognostic value of blood pressure drops during the first 24 h after hospital admission for risk stratification of community-acquired pneumonia: A retrospective cohort study. Infection 2020, 48, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Kamikawa, Y.; Hayashi, H. Predicting in-hospital mortality among non-trauma patients based on vital sign changes between prehospital and in-hospital: An observational cohort study. PLoS ONE 2019, 14, e0211580. [Google Scholar] [CrossRef] [PubMed]
- Levin, N.; Horton, D.; Sanford, M.; Horne, B.; Saseendran, M.; Graves, K.; White, M.; Tonna, J.E. Failure of vital sign normalization is more strongly associated than single measures with mortality and outcomes. Am. J. Emerg. Med. 2019. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Sex (%) | |
| Female | 87 (53) |
| Male | 78 (47) |
| Age (year), median (IQR) | 76 (64–84) |
| Charlson comorbidity index | 6 (5–7) |
| Final diagnosis (%) | |
| Pneumonia | 56 (34) |
| Urosepsis | 51 (31) |
| Intra-abdominal infection | 39 (24) |
| Others | 19 (11) |
| Procalcitonin (ng/mL) | 4.24 (0.99–24.13) |
| Duration of symptoms, median (IQR)(hour) | 24 (7–48) |
| Initial management | |
| Fluid loading (mL) | 2000 (1500–2500) |
| Time to antibiotic prescription, median (IQR)(hour) | 1.5 (0.5–2.5) |
| Time to the initiation of vasopressors (norepinephrine), median (IQR)(hour) | 3 (2–6) |
| Disposition | |
| Length of ER stay (hours) | 21 (10–34) |
| Length of hospital stay (days) | 13 (7–20) |
| Outcome (%) | |
| Mortality within 7 days | 25 (15) |
| In-hospital mortality | 45 (27) |
| Use of M/V | 48 (29) |
| Admission to the ICU | 74 (45) |
| SIRS score ≥2 (%) | 109 (66) |
| SIRS score, median (IQR) | 2 (1–3) |
| qSOFA score ≥2 (%) | 99 (60) |
| qSOFA score, median (IQR) | 2 (1–2) |
| NEWS ≥5 (%) | 136 (82) |
| NEWS, median (IQR) | 9 (5–12) |
| SOFA score ≥2 (%) | 164 (99) |
| SOFA score, median (IQR) | 8 (6–10) |
| Lactate ≥4 mmol/L (%) | 103 (62) |
| Lactate, median (IQR) | 2.8 (1.4–4.4) |
| Time (Hour) | SIRS | qSOFA | NEWS | SOFA | Lactate (mmol/L) | |
|---|---|---|---|---|---|---|
| Triage | ||||||
| Mean ± SD | - | 1.99 ± 1.16 | 1.70 ± 0.88 | 8.96 ± 4.25 | 7.89 ± 2.46 | 3.59 ± 3.14 |
| Median (IQR) | - | 2 (1–3) | 2 (1–2) | 9 (5–12) | 8 (6–10) | 2.8 (1.4–4.4) |
| Fluid resuscitation | ||||||
| Mean ± SD | 2.32 ± 1.75 | 1.92 ± 1.07 | 2.00 ± 0.83 | 8.70 ± 3.66 | - | 3.41 ± 3.15 |
| Median (IQR) | 2 (1–3) | 2 (1–3) | 2 (1–3) | 9 (6–11) | - | 2.4 (1.2–4.4) |
| Initiation of vasopressors | ||||||
| Mean ± SD | 5.89 ± 3.34 | 1.62 ± 1.12 | 2.03 ± 0.82 | 7.27 ± 3.69 | - | 3.15 ± 3.06 |
| Median (IQR) | 5 (4–7) | 2 (1–2) | 2 (1–3) | 7 (4–10) | - | 2.0 (1.1–4.0) |
| Before leaving the ER | ||||||
| Mean ± SD | 11.11 ± 4.72 | 2.03 ± 1.35 | 2.02 ± 0.83 | 6.34 ± 3.65 | 8.88 ± 3.08 | 3.24 ± 3.25 |
| Median (IQR) | 10 (8–14) | 2 (1–3) | 2 (1–3) | 6 (4–8) | 9 (6–11) | 2.0 (1.0–3.9) |
| Maximum | - | 4 | 3 | 18 | 17 | 15 |
| Δ from the triage value to the maximum value | - | 0.75 ± 0.90 | 0.56 ± 0.65 | 1.55 ± 2.22 | 1.37 ± 1.75 | 0.82 ± 1.63 |
| Δ from the triage value to the value measured before leaving the ER | - | 0.04 ± 1.49 | 0.32 ± 0.76 | −2.62 ± 3.88 | 0.99 ± 2.19 | −0.36 ± 2.35 |
| Maximum | From the Triage Value to the Maximum Value (Δ) | From the Triage Value to the Value Measured before Leaving the ER (Δ) | |
|---|---|---|---|
| AUROCs for the prediction of mortality within 7 days | |||
| SIRS | 0.768 (0.661–0.876) | 0.680 (0.564–0.797) | 0.746 (0.652–0.839) |
| qSOFA | 0.718 (0.627–0.809) | 0.513 (0.394–0.632) | 0.551 (0.435–0.666) |
| NEWS | 0.745 (0.652–0.838) | 0.576 (0.452–0.700) | 0.707 (0.592–0.821) |
| SOFA | 0.811 (0.735–0.887) | 0.746 (0.649–0.843) | 0.764 (0.679–0.848) |
| Lactate | 0.848 (0.777–0.919) | 0.723 (0.603–0.843) | 0.622 (0.472–0.772) |
| AUROCs for the prediction of in-hospital mortality, M/V, admission to ICU | |||
| SIRS | 0.641 (0.556–0.727) | 0.592 (0.506–0.679) | 0.634 (0.550–0.719) |
| qSOFA | 0.773 (0.699–0.847) | 0.535 (0.446–0.624) | 0.602 (0.516–0.688) |
| NEWS | 0.795 (0.727–0.863) | 0.534 (0.445–0.622) | 0.521 (0.433–0.609) |
| SOFA | 0.843 (0.783–0.903) | 0.725 (0.647–0.803) | 0.741 (0.665–0.817) |
| Lactate | 0.800 (0.733–0.867) | 0.678 (0.597–0.758) | 0.544 (0.457–0.632) |
| ER Triage | Fluid Resuscitation | Initiation of Vasopressor | Before Leaving ER | |
|---|---|---|---|---|
| AUROCs for the prediction of mortality within 7 days | ||||
| SIRS + lactate | 0.764 (0.661–0.867) | 0.798 (0.710–0.886) | 0.825 (0.742–0.908) | 0.882 (0.804–0.960) |
| qSOFA + lactate | 0.787 (0.697–0.877) | 0.827 (0.758–0.897) | 0.830 (0.758–0.903) | 0.872 (0.808–0.935) |
| NEWS + lactate | 0.757 (0.655–0.859) | 0.805 (0.721–0.890) | 0.844 (0.768–0.920) | 0.909 (0.855–0.963) |
| SOFA + lactate | 0.809 (0.728–0.891) | 0.885 (0.832–0.939) | ||
| AUROCs for the prediction of in-hospital mortality, M/V, admission to ICU | ||||
| SIRS + lactate | 0.728 (0.651–0.805) | 0.738 (0.662–0.814) | 0.799 (0.731–0.867) | 0.815 (0.751–0.880) |
| qSOFA + lactate | 0.776 (0.707–0.845) | 0.822 (0.760–0.885) | 0.871 (0.818–0.924) | 0.882 (0.831–0.933) |
| NEWS + lactate | 0.768 (0.697–0.838) | 0.801 (0.736–0.867) | 0.854 (0.797–0.910) | 0.854 (0.799–0.910) |
| SOFA + lactate | 0.798 (0.731–0.864) | 0.881 (0.829–0.932) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, T.S.; Park, H.W.; Park, H.Y.; Park, Y.S. Prognostic Value of Severity Score Change for Septic Shock in the Emergency Room. Diagnostics 2020, 10, 743. https://doi.org/10.3390/diagnostics10100743
Hwang TS, Park HW, Park HY, Park YS. Prognostic Value of Severity Score Change for Septic Shock in the Emergency Room. Diagnostics. 2020; 10(10):743. https://doi.org/10.3390/diagnostics10100743
Chicago/Turabian StyleHwang, Tae Sik, Hyun Woo Park, Ha Young Park, and Young Sook Park. 2020. "Prognostic Value of Severity Score Change for Septic Shock in the Emergency Room" Diagnostics 10, no. 10: 743. https://doi.org/10.3390/diagnostics10100743
APA StyleHwang, T. S., Park, H. W., Park, H. Y., & Park, Y. S. (2020). Prognostic Value of Severity Score Change for Septic Shock in the Emergency Room. Diagnostics, 10(10), 743. https://doi.org/10.3390/diagnostics10100743