
Predisposing Anatomical Patellofemoral Factors for Subsequent Patellar Dislocation

 , , and
, , and 
Abstract
1. Introduction
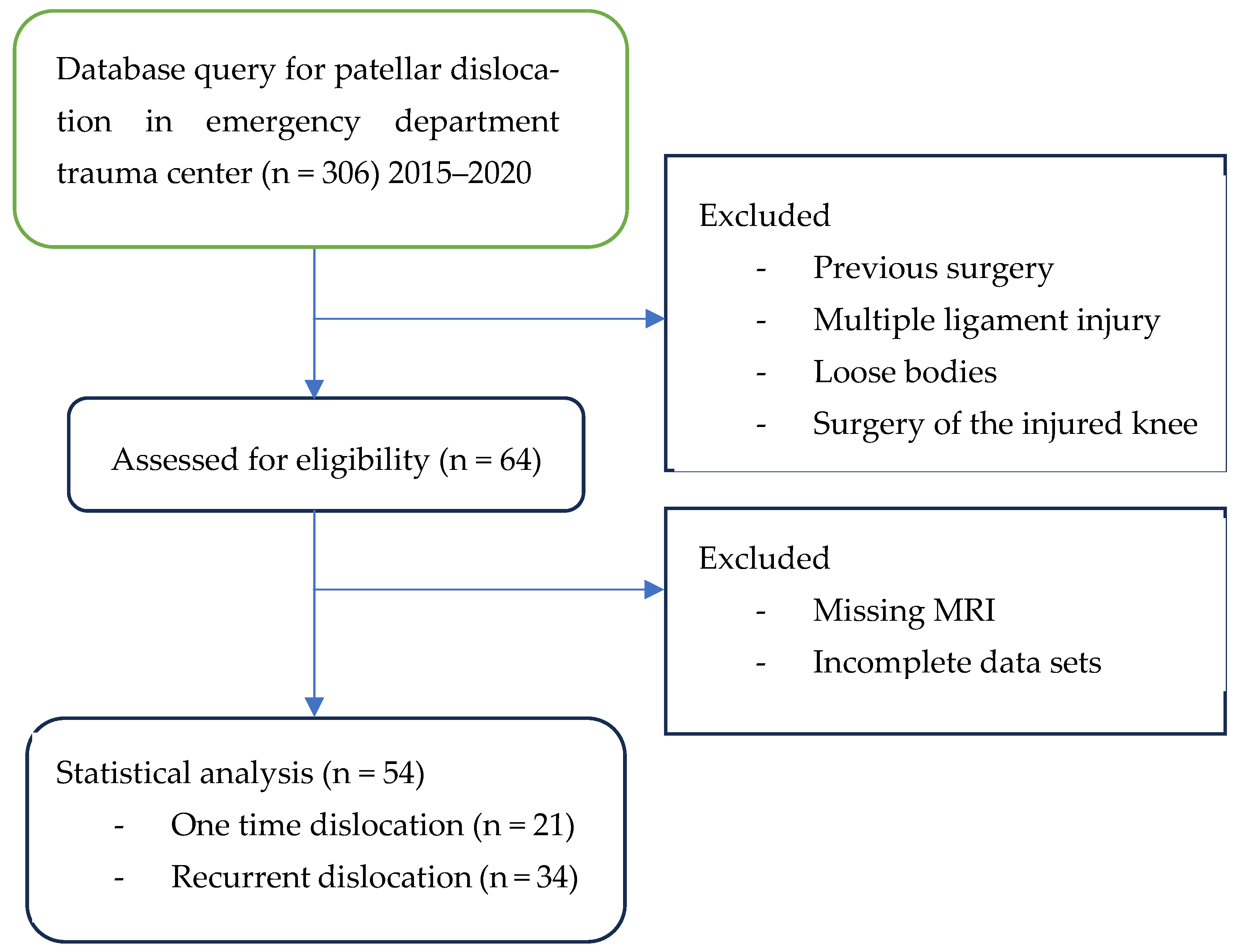
2. Materials and Methods
2.1. MRI Technique
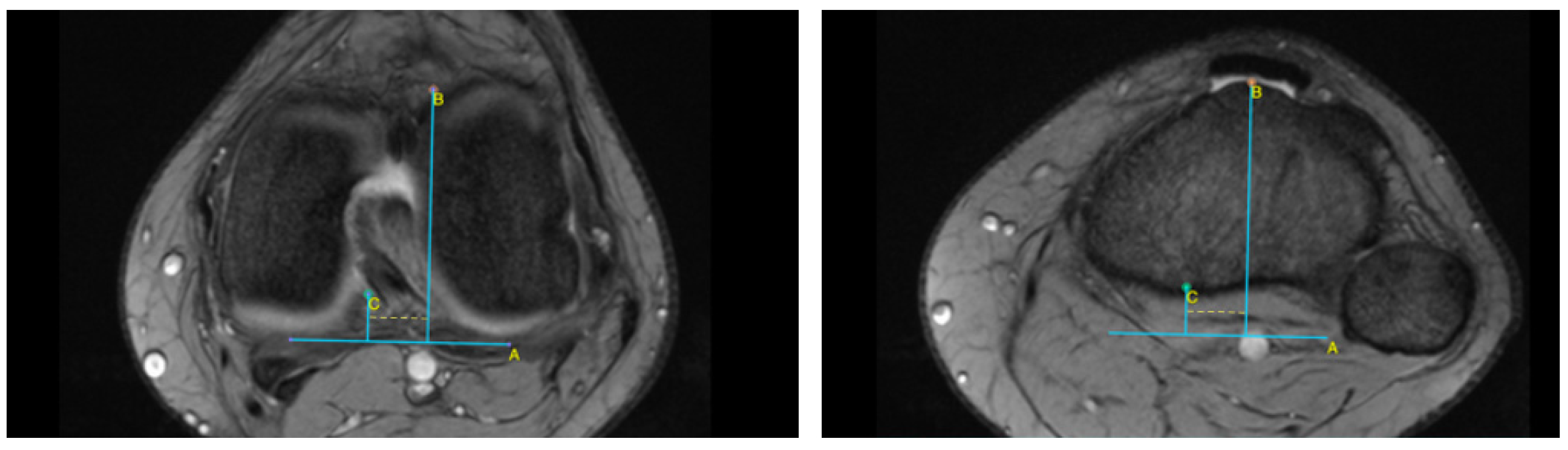
2.2. MRI Analysis
2.3. Statistical Analysis
3. Results
3.1. Subsequent Dislocation
3.2. Return to Activity (In the Whole Study Population)
3.3. Dejour Dysplasia
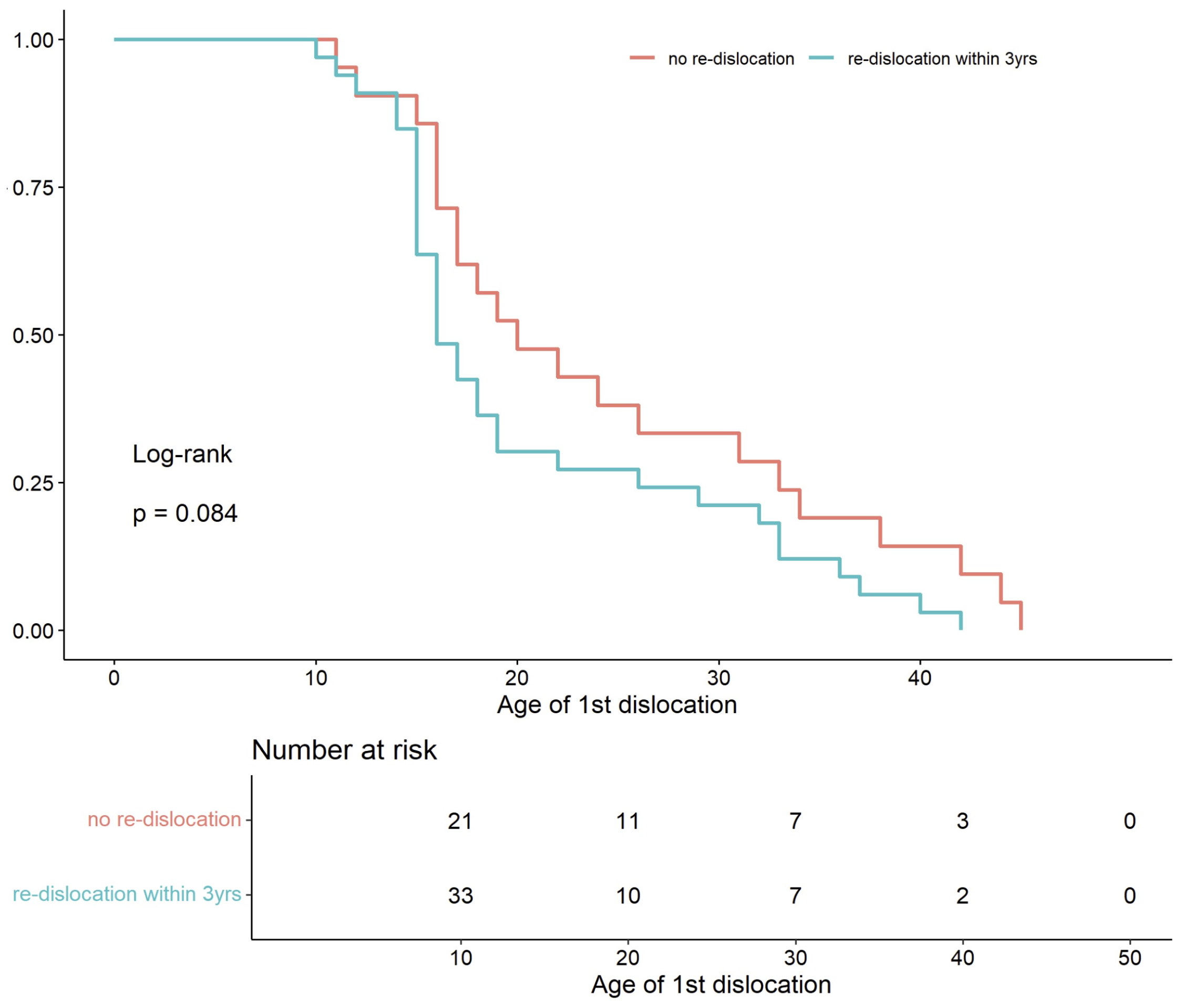
3.4. Age
3.5. Correlation
3.6. Interaction Effects on Recurrence Risk
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MRI | Magnetic resonance Imaging. |
| TT–TG | tibial tuberosity–trochlear groove |
| TT–PCL | tibial tuberosity–posterior cruciate ligament |
| IS | Insall–Salvati ratio |
| SA | Sulcus angle |
| PTA | patellar tilt angle |
References
- Stefancin, J.J.; Parker, R.D. First-Time Traumatic Patellar Dislocation: A Systematic Review. Clin. Orthop. Relat. Res. 2007, 455, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Veshohilova, T.P. Effect of combined use of steroid preparations with pyrroxane on the gonadotropic function of the hypophysis. Akush. Ginekol. 1975, 10, 10–12. [Google Scholar]
- Dai, R.; Wu, Y.; Jiang, Y.; Huang, H.; Meng, Q.; Shi, W.; Ren, S.; Ao, Y. Epidemiology of Lateral Patellar Dislocation Including Bone Bruise Incidence: Five Years of Data from a Trauma Center. Orthop. Surg. 2024, 16, 437–443. [Google Scholar] [CrossRef]
- Danielsen, O.; Poulsen, T.A.; Eysturoy, N.H.; Mortensen, E.S.; Hölmich, P.; Barfod, K.W. Trochlea Dysplasia, Increased TT-TG Distance and Patella Alta Are Risk Factors for Developing First-time and Recurrent Patella Dislocation: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 3806–3846. [Google Scholar] [CrossRef]
- Sillanpää, P.; Mattila, V.M.; Iivonen, T.; Visuri, T.; Pihlajamäki, H. Incidence and Risk Factors of Acute Traumatic Primary Patellar Dislocation. Med. Sci. Sports Exerc. 2008, 40, 606–611. [Google Scholar] [CrossRef]
- Atkin, D.M.; Fithian, D.C.; Marangi, K.S.; Stone, M.L.; Dobson, B.E.; Mendelsohn, C. Characteristics of Patients with Primary Acute Lateral Patellar Dislocation and Their Recovery within the First 6 Months of Injury. Am. J. Sports Med. 2000, 28, 472–479. [Google Scholar] [CrossRef]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and Natural History of Acute Patellar Dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef]
- Gravesen, K.S.; Kallemose, T.; Blønd, L.; Troelsen, A.; Barfod, K.W. High Incidence of Acute and Recurrent Patellar Dislocations: A Retrospective Nationwide Epidemiological Study Involving 24.154 Primary Dislocations. Knee Surg. Sports Traumatol. Arthrosc. 2017, 26, 1204–1209. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, M.; Owens, B.D.; Burks, R.; Sturdivant, R.X.; Cameron, K.L. Incidence of Acute Traumatic Patellar Dislocation among Active-Duty United States Military Service Members. Am. J. Sports Med. 2010, 38, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Goutallier, D.; Bernageau, J.; Lecudonnec, B. [The measurement of the tibial tuberosity. Patella groove distanced technique and results (author’s transl)]. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1978, 64, 423–428. [Google Scholar]
- Seitlinger, G.; Scheurecker, G.; Högler, R.; Labey, L.; Innocenti, B.; Hofmann, S. Tibial Tubercle–Posterior Cruciate Ligament Distance: A New Measurement to Define the Position of the Tibial Tubercle in Patients with Patellar Dislocation. Am. J. Sports Med. 2012, 40, 1119–1125. [Google Scholar] [CrossRef]
- Van Huyssteen, A.L.; Hendrix, M.R.G.; Barnett, A.J.; Wakeley, C.J.; Eldridge, J.D.J. Cartilage-Bone Mismatch in the Dysplastic Trochlea: AN MRI STUDY. J. Bone Jt. Surgery. Br. Vol. 2006, 88-B, 688–691. [Google Scholar] [CrossRef]
- Grelsamer, R.P.; Weinstein, C.H.; Gould, J.; Dubey, A. Patellar Tilt: The Physical Examination Correlates with MR Imaging. Knee 2008, 15, 3–8. [Google Scholar] [CrossRef]
- Biedert, R.M.; Albrecht, S. The Patellotrochlear Index: A New Index for Assessing Patellar Height. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 707–712. [Google Scholar] [CrossRef]
- Insall, J.; Salvati, E. Patella Position in the Normal Knee Joint. Radiology 1971, 101, 101–104. [Google Scholar] [CrossRef]
- Dejour, D.H.; De Sanctis, E.G.; Müller, J.H.; Deroche, E.; Pineda, T.; Guarino, A.; Toanen, C.; Patellofemoral Imaging Group. Adapting the Dejour Classification of Trochlear Dysplasia from Qualitative Radiograph- and CT-based Assessments to Quantitative MRI-based Measurements. Knee Surg. Sports Traumatol. Arthrosc. 2024, 33, ksa.12539. [Google Scholar] [CrossRef]
- R Core Team (2023) R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023.
- Huntington, L.S.; Webster, K.E.; Devitt, B.M.; Scanlon, J.P.; Feller, J.A. Factors Associated with an Increased Risk of Recurrence After a First-Time Patellar Dislocation: A Systematic Review and Meta-Analysis. Am. J. Sports Med. 2020, 48, 2552–2562. [Google Scholar] [CrossRef] [PubMed]
- Dejour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Factors of Patellar Instability: An Anatomic Radiographic Study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hing, C.B.; Shepstone, L.; Marshall, T.; Donell, S.T. A Laterally Positioned Concave Trochlear Groove Prevents Patellar Dislocation. Clin. Orthop. Relat. Res. 2006, 447, 187–194. [Google Scholar] [CrossRef]
- Jaquith, B.P.; Parikh, S.N. Predictors of Recurrent Patellar Instability in Children and Adolescents After First-Time Dislocation. J. Pediatr. Orthop. 2017, 37, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Lewallen, L.; McIntosh, A.; Dahm, D. First-Time Patellofemoral Dislocation: Risk Factors for Recurrent Instability. J. Knee Surg. 2015, 28, 303–310. [Google Scholar] [CrossRef]
- Frings, J.; Balcarek, P.; Tscholl, P.; Liebensteiner, M.; Dirisamer, F.; Koenen, P. Conservative Versus Surgical Treatment for Primary Patellar Dislocation. Dtsch. Ärzteblatt Int. 2020, 117, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Frosch, S.; Balcarek, P.; Walde, T.; Schüttrumpf, J.; Wachowski, M.; Ferleman, K.-G.; Stürmer, K.; Frosch, K.-H. Die Therapie der Patellaluxation: Eine systematische Literaturanalyse. Z. Orthop. Unf. 2011, 149, 630–645. [Google Scholar] [CrossRef]
- Johnson, D.S.; Turner, P.G. Management of the First-Time Lateral Patellar Dislocation. Knee 2019, 26, 1161–1165. [Google Scholar] [CrossRef]
- Sinikumpu, J.; Nicolaou, N. Current Concepts in the Treatment of First-Time Patella Dislocation in Children and Adolescents. J. Child. Orthop. 2023, 17, 28–33. [Google Scholar] [CrossRef]
- Sakai, N.; Luo, Z.-P.; Rand, J.A.; An, K.-N. The Influence of Weakness in the Vastus Medialis Oblique Muscle on the Patellofemoral Joint: An in Vitro Biomechanical Study. Clin. Biomech. 2000, 15, 335–339. [Google Scholar] [CrossRef]
- Honkonen, E.E.; Sillanpää, P.J.; Reito, A.; Kiekara, T.; Mäenpää, H.; Mattila, P.V.M. Assessing Femoral Anteversion in Patients with Bilateral Recurrent Patellar Dislocations. Orthop. J. Sports Med. 2024, 12, 23259671241300319. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Yang, A. Patellar Dislocations: Review of Current Literature and Return to Play Potential. Curr. Phys. Med. Rehabil. Rep. 2018, 6, 161–170. [Google Scholar] [CrossRef]
- Flores, G.W.; De Oliveira, D.F.; Ramos, A.P.S.; Sanada, L.S.; Migliorini, F.; Maffulli, N.; Okubo, R. Conservative Management Following Patellar Dislocation: A Level I Systematic Review. J. Orthop. Surg. Res. 2023, 18, 393. [Google Scholar] [CrossRef]
- Dejour, D.H.; Deroche, É. Trochleoplasty: Indications in Patellar Dislocation with High-Grade Dysplasia. Surg. Technique. Orthop. Traumatol. Surg. Res. 2022, 108, 103160. [Google Scholar] [CrossRef]
- Zhang, G.; Ding, H.; Li, E.; Zheng, L.; Bai, Z.; Shi, H.; Fan, F.; Guo, D. Incidence of Second-time Lateral Patellar Dislocation Is Associated with Anatomic Factors, Age and Injury Patterns of Medial Patellofemoral Ligament in First-time Lateral Patellar Dislocation: A Prospective Magnetic Resonance Imaging Study with 5-year Follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Kang, K.; Li, T.; Lu, B.; Dong, J.; Gao, S. Surgical versus Non-Surgical Management for Primary Patellar Dislocations: An up-to-Date Meta-Analysis. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Ménétrey, J.; Putman, S.; Gard, S. Return to Sport after Patellar Dislocation or Following Surgery for Patellofemoral Instability. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2320–2326. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients |
|---|---|
| Sex: | |
| Female Male | 31 23 |
| Age at the time of first dislocation | 19.2 (6–44) |
| Mean age | 22.2 (6–44) |
| Right knee | 23 |
| Left knee | 31 |
| Return to activity: Primary dislocation Recurrent dislocation | 13 (62%) 10 (18%) |
| Control Group | Study Group | |
|---|---|---|
| Patients | 21 (39%) | 33 (61%) |
| Female | 18 (55%) | 13 (62%) |
| No return to activity | 8 (38%) | 23 (70%) |
| Return to sport | 13 (62%) | 10 (30%) |
| Subsequent Dislocation | Control Group | p | |
|---|---|---|---|
| TTPCL | 20.88 ± 5.46 | 23.24 ± 4.81 | 0.11 |
| SAb | 148.26 ± 13.82 | 149.93 ± 10.66 | 0.64 |
| SAc | 156.06 ± 12.43 | 159.01 ± 10.69 | 0.37 |
| Patella length | 39.42 ± 3.74 | 41.86 ± 5.41 | 0.06 |
| Patellar tendon length | 54.15 ± 6.91 | 59.14 ± 5.88 | 0.008 * |
| I-S ratio | 1.38 ± 0.17 | 1.43 ± 0.18 | 0.32 |
| overlap | 0.31 ± 0.1 | 0.28 ± 0.05 | 0.3 |
| TTTG | PTA | Age | |
|---|---|---|---|
| Subsequent dislocation group | 10.12 ± 4.46 | 20.74 ± 10.84 | 17.21 ± 7.76 |
| Control group | 12.29 ± 4.63 | 22.64 ± 7.61 | 22.42 ± 11.36 |
| U-Test p | 0.046 | 0.41 | 0.09 |
| TTPCL | SAb | SAc | Patellar Tendon Length | I-S Ratio | |
|---|---|---|---|---|---|
| Successful return to activity group | 21.41 ± 4.85 | 150.60 ± 10.78 | 158.62 ± 10.85 | 55.23 ± 7.37 | 1.39 ± 0.19 |
| Unsuccessful return to activity group | 22.30 ± 5.66 | 146.62 ± 13.72 | 155.30 ± 12.38 | 57.26 ± 6.55 | 1.41 ± 0.16 |
| t-Test p | 0.55 | 0.26 | 0.31 | 0.29 | 0.56 |
| Age | TTTG | PTA | Patella Length | |
|---|---|---|---|---|
| Successful return to activity group | 19.29 ± 9.81 | 10.87 ± 4.54 | 21.63 ± 8.3 | 40.06 ± 4.8 |
| Unsuccessful return to activity group | 19.17 ± 9.56 | 11.09 ± 4.72 | 21.29 ± 10.72 | 40.78 ± 4.46 |
| U-Test p | 1.0 | 0.68 | 0.93 | 0.85 |
| Dejour Type | No Recurrence | Recurrence | Total |
|---|---|---|---|
| A | 9 | 6 | 15 |
| B | 3 | 5 | 8 |
| C | 6 | 11 | 17 |
| D | 2 | 4 | 6 |
| Factor | OR | 95% CI | p-Value |
|---|---|---|---|
| return to previous level of activity | 0.27 | 0.081–0.826 | 0.0249 |
| patella length return to previous level of activity | 1.1389 | 1.0345–1.2879 | 0.01649 |
| PTA Overlap | 97.398 | 4.344–2.46 × 104 | 0.02126 |
| PTA patella ligament length overlap | 1.1159 | 1.0406–1.2855 | 0.02569 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kupczak, A.; Wilk, B.; Tramś, E.; Liszka, M.; Machnio, B.; Jasiniewska, A.; Białecki, J.; Kamiński, R. Predisposing Anatomical Patellofemoral Factors for Subsequent Patellar Dislocation. Life 2025, 15, 1239. https://doi.org/10.3390/life15081239
Kupczak A, Wilk B, Tramś E, Liszka M, Machnio B, Jasiniewska A, Białecki J, Kamiński R. Predisposing Anatomical Patellofemoral Factors for Subsequent Patellar Dislocation. Life. 2025; 15(8):1239. https://doi.org/10.3390/life15081239
Chicago/Turabian StyleKupczak, Anna, Bartłomiej Wilk, Ewa Tramś, Maciej Liszka, Bartosz Machnio, Aleksandra Jasiniewska, Jerzy Białecki, and Rafał Kamiński. 2025. "Predisposing Anatomical Patellofemoral Factors for Subsequent Patellar Dislocation" Life 15, no. 8: 1239. https://doi.org/10.3390/life15081239
APA StyleKupczak, A., Wilk, B., Tramś, E., Liszka, M., Machnio, B., Jasiniewska, A., Białecki, J., & Kamiński, R. (2025). Predisposing Anatomical Patellofemoral Factors for Subsequent Patellar Dislocation. Life, 15(8), 1239. https://doi.org/10.3390/life15081239