

A Multimodal Approach to Managing Severe Psoriasis Vulgaris: A Case Report Leveraging Natural Therapies for Flare Control


 , ,
, ,
Abstract
1. Introduction
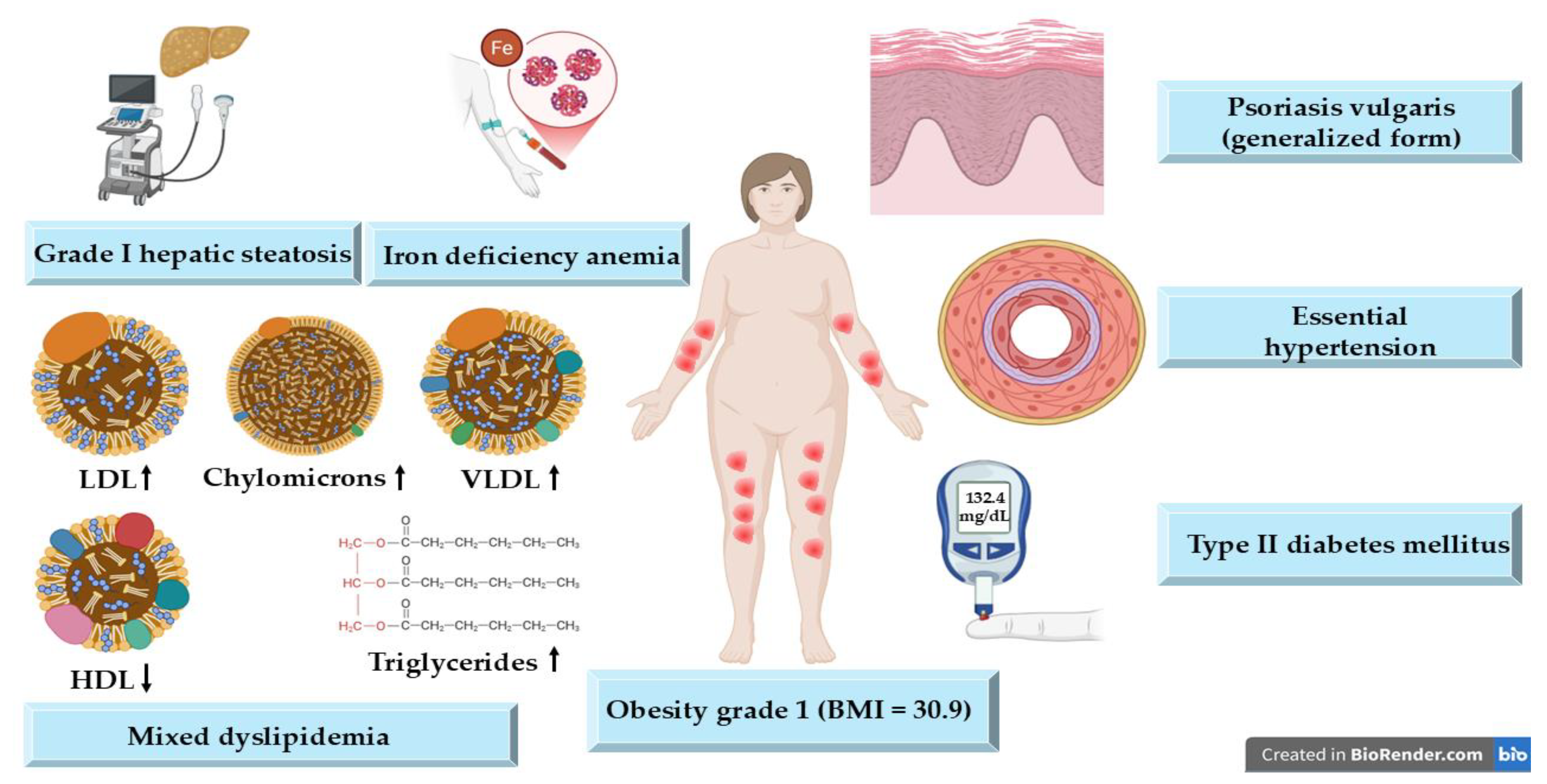
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PASI | Psoriasis Area and Severity Index |
| DLQI | Dermatology Life Quality Index |
| TNF- α | Tumor necrosis factor alpha |
| IL | Interleukin |
| ESR | Erythrocyte sedimentation rate |
| CRP | C-reactive protein |
| VLCKD | Very low-calorie ketogenic diet |
| BMI | Body mass index |
| JAK | Janus kinase |
| GPX | Glutathione peroxidase |
| ROS | Reactive oxygen species |
References
- Sieminska, I.; Pieniawska, M.; Grzywa, T.M. The Immunology of Psoriasis-Current Concepts in Pathogenesis. Clin. Rev. Allergy Immunol. 2024, 66, 164–191. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, G.W.; Lebwohl, M. Psoriasis: Overview and Diagnosis. In Evidence-Based Psoriasis Diagnosis and Treatment; Springer: Cham, Switzerland, 2018; pp. 1–16. [Google Scholar]
- Sarac, G.; Koca, T.T.; Baglan, T. A Brief Summary of Clinical Types of Psoriasis. North Clin. Istanb. 2016, 3, 79–82. [Google Scholar] [PubMed]
- Kim, W.B.; Jerome, D.; Yeung, J. Diagnosis and Management of Psoriasis. Can. Fam. Physician 2017, 63, 278–285. [Google Scholar] [PubMed]
- Manchanda, Y.; De, A.; Das, S.; Chakraborty, D. Disease Assessment in Psoriasis. Indian J. Dermatol. 2023, 68, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Marani, A.; Martina, E.; Diotallevi, F.; Radi, G.; Offidani, A. Psoriasis as an Immune-Mediated and Inflammatory Systemic Disease: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2021, 9, 1511. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Moreno, A.; Krueger, J.G. The Imbalance between Type 17 T-Cells and Regulatory Immune Cell Subsets in Psoriasis Vulgaris. Front. Immunol. 2022, 13, 1005115. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, F.; Verduci, C.; Laconi, E.; Mangione, A.; Dondi, C.; Del Vecchio, M.; Carlevatti, V.; Zovi, A.; Capuozzo, M.; Langella, R. Current Therapeutic Overview and Future Perspectives Regarding the Treatment of Psoriasis. Int. Immunopharmacol. 2024, 143, 113388. [Google Scholar] [CrossRef] [PubMed]
- Elmets, C.A.; Korman, N.J.; Prater, E.F.; Wong, E.B.; Rupani, R.N.; Kivelevitch, D.; Armstrong, A.W.; Connor, C.; Cordoro, K.M.; Davis, D.M.R.; et al. Joint AAD–NPF Guidelines of Care for the Management and Treatment of Psoriasis with Topical Therapy and Alternative Medicine Modalities for Psoriasis Severity Measures. J. Am. Acad. Dermatol. 2021, 84, 432–470. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, H.; Nagpal, M.; Singh, M.; Dhingra, G.A.; Aggarwal, G. Treatment of Psoriasis: A Comprehensive Review of Entire Therapies. Curr. Drug Saf. 2020, 15, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Loft, N.; Egeberg, A.; Rasmussen, M.K.; Bryld, L.E.; Nissen, C.V.; Dam, T.N.; Ajgeiy, K.K.; Iversen, L.; Skov, L. Prevalence and Characterization of Treatment-Refractory Psoriasis and Super-Responders to Biologic Treatment: A Nationwide Study. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Radu, A.; Tit, D.M.; Endres, L.M.; Radu, A.-F.; Vesa, C.M.; Bungau, S.G. Naturally Derived Bioactive Compounds as Precision Modulators of Immune and Inflammatory Mechanisms in Psoriatic Conditions. Inflammopharmacology 2024, 33, 527–549. [Google Scholar] [CrossRef] [PubMed]
- Abu-al-Basal, M.A. Histological Evaluation of the Healing Properties of Dead Sea Black Mud on Full-Thickness Excision Cutaneous Wounds in BALB/c Mice. Pakistan J. Biol. Sci. PJBS 2012, 15, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.; Bartholomew, E.; Yeroushalmi, S.; Hakimi, M.; Bhutani, T.; Liao, W. Dietary Intervention and Supplements in the Management of Psoriasis: Current Perspectives. Psoriasis 2022, 12, 151–176. [Google Scholar] [CrossRef] [PubMed]
- Rousset, L.; Halioua, B. Stress and Psoriasis. Int. J. Dermatol. 2018, 57, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, L.; Olszewska, M.; Goldust, M.; Waśkiel-Burnat, A.; Warszawik-Hendzel, O.; Dorożyński, P.; Turło, J.; Rakowska, A. Efficacy and Safety of Different Formulations of Calcipotriol/Betamethasone Dipropionate in Psoriasis: Gel, Foam, and Ointment. J. Clin. Med. 2021, 10, 5589. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Gracia-Cazaña, T.; Kurzen, H.; Galván, J. Calcipotriol/Betamethasone Dipropionate for the Treatment of Psoriasis: Mechanism of Action and Evidence of Efficacy and Safety versus Topical Corticosteroids. J. Clin. Med. 2024, 13, 4484. [Google Scholar] [CrossRef] [PubMed]
- Del Rosso, J.Q. Topical Corticosteroid Therapy for Psoriasis—A Review of Clobetasol Propionate 0.025% Cream and the Clinical Relevance of Penetration Modification. J. Clin. Aesthet. Dermatol. 2020, 13, 22–29. [Google Scholar] [PubMed]
- Shalaby, R.A.; El-Gazayerly, O.; Abdallah, M. Cubosomal Betamethasone-Salicylic Acid Nano Drug Delivery System for Enhanced Management of Scalp Psoriasis. Int. J. Nanomed. 2022, 17, 1659–1677. [Google Scholar] [CrossRef] [PubMed]
- Dallo, M.; Patel, K.; Hebert, A.A. Topical Antibiotic Treatment in Dermatology. Antibiotics 2023, 12, 188. [Google Scholar] [CrossRef] [PubMed]
- Balamurugan, D.; Nayak, C.; Chattopadhyay, A.; Karuppusamy, A.; Ambrose, M.M.; Kumar, A.; Singh, N.K.; Koley, M.; Saha, S. Individualized Homeopathic Medicines in the Treatment of Psoriasis Vulgaris: Double-Blind, Randomized, Placebo-Controlled Trial. Complement. Med. Res. 2023, 30, 317–331. [Google Scholar] [CrossRef] [PubMed]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Badri, T.; Kumar, P.; Oakley, A.M. Plaque Psoriasis. Pract. Nurs. 2023, 19, 560–565. [Google Scholar]
- Prieto-Pérez, R.; Solano-López, G.; Cabaleiro, T.; Román, M.; Ochoa, D.; Talegón, M.; Baniandrés, O.; López-Estebaranz, J.L.; de la Cueva, P.; Daudén, E.; et al. Polymorphisms Associated with Age at Onset in Patients with Moderate-to-Severe Plaque Psoriasis. J. Immunol. Res. 2015, 2015, 101879. [Google Scholar] [CrossRef] [PubMed]
- Potestio, L.; Lauletta, G.; Tommasino, N.; Portarapillo, A.; Salsano, A.; Battista, T.; Martora, F.; Megna, M. Risk Factors for Psoriasis Flares: A Narrative Review. Psoriasis 2024, 14, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Keenan, E.L.; Granstein, R.D. Proinflammatory Cytokines and Neuropeptides in Psoriasis, Depression, and Anxiety. Acta Physiol. 2025, 241, e70019. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; Thaçi, D.; Warren, R.B. Addressing Challenges Associated with Long-Term Topical Treatment and Benefits of Proactive Management in Patients with Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Cîrstea, N.; Radu, A.; Vesa, C.; Radu, A.F.; Bungau, A.F.; Tit, D.M.; Cseppento, C.D.N.; Tarce, A.G.; Bungau, S.G. Current Insights on Treatment Adherence in Prevalent Dermatological Conditions and Strategies To Optimize Adherence Rates. Cureus 2024, 16, 869764. [Google Scholar] [CrossRef] [PubMed]
- Agnihotri, S.; Kaur, J.; Masand, P.; Anurag; Parihar, V.K.; Sharma, A. Vitamins Strategies for Psoriasis: An Update on Current Scientific Evidence. J. Holist. Integr. Pharm. 2023, 4, 299–309. [Google Scholar] [CrossRef]
- Elkhawaga, O.Y.; Ellety, M.M.; Mofty, S.O.; Ghanem, M.S.; Mohamed, A.O. Review of Natural Compounds for Potential Psoriasis Treatment. Inflammopharmacology 2023, 31, 1183–1198. [Google Scholar] [CrossRef] [PubMed]
- Maheswari, A.; Dutta, B. Correlation of Hypocalcaemia with Severity and Type of Psoriasis: A Cross-Sectional Study. IP Indian J. Clin. Exp. Dermatol. 2021, 7, 164–168. [Google Scholar] [CrossRef]
- Patra, P.; Harrison, T. Trace Elements in Psoriasis Presentation and Treatment. Arch. Dermatol. Res. 2024, 316, 728. [Google Scholar] [CrossRef] [PubMed]
- Masson, L.; Saillard, C.; Ping Man, S.L.; Baggio, R.; Kammerer-Jacquet, S.-F.; Adamski, H.; Dupuy, A. A Pustular Psoriasis Flare Treated with Calcium Supplementation. JAAD Case Rep. 2021, 12, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Altemani, A.; Alsaedi, E.; Aldawish, R.; Alharbi, M.; Alzahrani, R.; Alatawi, S.; Altemani, S.; Alanazi, A.H. The Association of Psoriasis, Diabetes Mellitus, and Hypertension: A Meta-Analysis. Cureus 2023, 15, e48855. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, S.; Dharmaraj, S. Selenium and Selenoproteins: It’s Role in Regulation of Inflammation. Inflammopharmacology 2020, 28, 667–695. [Google Scholar] [CrossRef] [PubMed]
- Dębniak, T.; Baszuk, P.; Duchnik, E.; Rowińska, K.; Rogoża-Janiszewska, E.; Boer, M.; Kiedrowicz, M.; Marchlewicz, M.; Watola, D.; Feherpataky, M.; et al. Selenium and Arsenic Levels, Prevalence of Common Variants of Genes Involved in Their Metabolism, and Psoriasis Disease. Biomedicines 2024, 12, 1082. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Ai, P.; Lei, S.; Zhou, F.; Chen, S.; Zhang, Y. Selenium Levels and Skin Diseases: Systematic Review and Meta-Analysis. J. Trace Elem. Med. Biol. 2020, 62, 126548. [Google Scholar] [CrossRef] [PubMed]
- Duchnik, E.; Kruk, J.; Tuchowska, A.; Marchlewicz, M. The Impact of Diet and Physical Activity on Psoriasis: A Narrative Review of the Current Evidence. Nutrients 2023, 15, 840. [Google Scholar] [CrossRef] [PubMed]
- Gangadevi, V.; Thatikonda, S.; Pooladanda, V.; Devabattula, G.; Godugu, C. Selenium Nanoparticles Produce a Beneficial Effect in Psoriasis by Reducing Epidermal Hyperproliferation and Inflammation. J. Nanobiotechnol. 2021, 19, 101. [Google Scholar] [CrossRef] [PubMed]
- Piquero-Casals, J.; Morgado-Carrasco, D.; Granger, C.; Trullàs, C.; Jesús-Silva, A.; Krutmann, J. Urea in Dermatology: A Review of Its Emollient, Moisturizing, Keratolytic, Skin Barrier Enhancing and Antimicrobial Properties. Dermatol. Ther. 2021, 11, 1905–1915. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, T.; Petersen, A.; Houborg, H.I.; Rønsholdt, A.B.; Lybaek, D.; Steiniche, T.; Bregnhøj, A.; Iversen, L.; Johansen, C. Climatotherapy at the Dead Sea for Psoriasis Is a Highly Effective Anti-Inflammatory Treatment in the Short Term: An Immunohistochemical Study. Exp. Dermatol. 2022, 31, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Halevy, S.; Giryes, H.; Friger, M.; Sukenik, S. Dead Sea Bath Salt for the Treatment of Psoriasis Vulgaris: A Double-Blind Controlled Study. J. Eur. Acad. Dermatol. Venereol. 1997, 9, 237–242. [Google Scholar] [CrossRef]
- Hamed, S.; Almalty, A.-M.; Alkhatib, H.S. The Cutaneous Effects of Long-Term Use of Dead Sea Mud on Healthy Skin: A 4-Week Study. Int. J. Dermatol. 2021, 60, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Dai, D.; Ma, X.; Yan, X.; Bao, X. The Biological Role of Dead Sea Water in Skin Health: A Review. Cosmetics 2023, 10, 21. [Google Scholar] [CrossRef]
- Li Pomi, F.; Papa, V.; Borgia, F.; Vaccaro, M.; Allegra, A.; Cicero, N.; Gangemi, S. Rosmarinus officinalis and Skin: Antioxidant Activity and Possible Therapeutical Role in Cutaneous Diseases. Antioxidants 2023, 12, 680. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lu, J. Rosemary (Rosmarinus officinalis L.) Polyphenols and Inflammatory Bowel Diseases: Major Phytochemicals, Functional Properties, and Health Effects. Fitoterapia 2024, 177, 106074. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, J.R.; Camargo, S.E.A.; De Oliveira, L.D. Rosmarinus officinalis L. (Rosemary) as Therapeutic and Prophylactic Agent. J. Biomed. Sci. 2019, 26, 5. [Google Scholar] [CrossRef] [PubMed]
- Nieto, G.; Ros, G.; Castillo, J. Antioxidant and Antimicrobial Properties of Rosemary (Rosmarinus officinalis, L.): A Review. Medicines 2018, 5, 98. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, J.R.; de Jesus, D.; Figueira, L.W.; de Oliveira, F.E.; Pacheco Soares, C.; Camargo, S.E.A.; Jorge, A.O.C.; de Oliveira, L.D. Biological Activities of Rosmarinus officinalis L. (Rosemary) Extract as Analyzed in Microorganisms and Cells. Exp. Biol. Med. 2017, 242, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Sahlabgi, A.; Lupuliasa, D.; Stanciu, G.; Lupșor, S.; Vlaia, L.L.; Rotariu, R.; Predescu, N.C.; Rădulescu, C.; Olteanu, R.-L.; Stănescu, S.-G.; et al. The Development and Comparative Evaluation of Rosemary Hydroalcoholic Macerate-Based Dermatocosmetic Preparations: A Study on Antioxidant, Antimicrobial, and Anti-Inflammatory Properties. Gels 2025, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- de Macedo, L.M.; Santos, É.M.d.; Militão, L.; Tundisi, L.L.; Ataide, J.A.; Souto, E.B.; Mazzola, P.G. Rosemary (Rosmarinus officinalis L., Syn Salvia rosmarinus Spenn.) and Its Topical Applications: A Review. Plants 2020, 9, 651. [Google Scholar] [CrossRef] [PubMed]
- Harit, M.K.; Mundhe, N.; Tamoli, S.S.; Pawar, V.; Bhapkar, V.; Kolhe, G.; Mahadik, S.; Kulkarni, A.; Agarwal, A. Randomized, Double-Blind, Placebo-Controlled, Clinical Study of Passiflora Incarnata in Participants With Stress and Sleep Problems. Cureus 2024, 16, e56530. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, J.; Sun, X.; Liu, L.; Zhang, M.; Yu, Y.; Gao, P.; Hong, S.; Li, X. Evidence-Based Dietary Recommendations for Patients with Psoriasis: A Systematic Review. Clin. Nutr. 2025, 47, 68–82. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Megna, M.; Cacciapuoti, S.; Frias-Toral, E.; Fabbrocini, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Very Low-Calorie Ketogenic Diet (VLCKD) in Patients with Psoriasis and Obesity: An Update for Dermatologists and Nutritionists. Crit. Rev. Food Sci. Nutr. 2022, 62, 398–414. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Active Substance | Concentration | Pharmaceutical Form | Mechanism of Action | Reference |
|---|---|---|---|---|
| Calcipotriol (vitamin D3 analogue) | 50 µg | Gel | Binds retinoid X receptor, regulates cell differentiation and immune function | [16] |
| Betamethasone Dipropionate | 0.5 mg | Gel | Inhibition of T-cell activation, reduced production of pro-inflammatory cytokines, induction of apoptosis and inhibition of proliferation | [17] |
| Clobetasol Propionate | 0.5 mg | Cream | Stabilizes cell membranes, modulates immune cells, reduces inflammation and proliferation | [18] |
| Salicylic acid | 20 mg | Cutaneous solution | Keratolytic action | [19] |
| Gentamicin sulphate | 1 mg | Cream | Inhibition of protein synthesis by targeting the 30S ribosomal subunit | [20] |
| Calcarea carbonica | 200 C | Granules | Overall impact on systemic predispositions, inflammation, and skin texture | [21] |
| Parameter | Value | Reference Range |
|---|---|---|
| CRP | 0.4 mg/dL | <0.5 mg/dL |
| ESR | 40 mm/h | <30 mm/h |
| Fibrinogen | 340 mg/dL | 200–400 mg/dL |
| Glucose | 132.4 mg/dL | 60–99 mg/dL |
| Serum iron | 30 µg/dL | 34–145 µg/dL |
| Total cholesterol | 280 mg/dL | <200 mg/dL |
| Triglycerides | 185 mg/dL | <150 mg/dL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radu, A.; Jurca, T.; Radu, A.-F.; Bodog, T.M.; Bodog, R.F.; Endres, L. A Multimodal Approach to Managing Severe Psoriasis Vulgaris: A Case Report Leveraging Natural Therapies for Flare Control. Life 2025, 15, 1186. https://doi.org/10.3390/life15081186
Radu A, Jurca T, Radu A-F, Bodog TM, Bodog RF, Endres L. A Multimodal Approach to Managing Severe Psoriasis Vulgaris: A Case Report Leveraging Natural Therapies for Flare Control. Life. 2025; 15(8):1186. https://doi.org/10.3390/life15081186
Chicago/Turabian StyleRadu, Ada, Tunde Jurca, Andrei-Flavius Radu, Teodora Maria Bodog, Ruxandra Florina Bodog, and Laura Endres. 2025. "A Multimodal Approach to Managing Severe Psoriasis Vulgaris: A Case Report Leveraging Natural Therapies for Flare Control" Life 15, no. 8: 1186. https://doi.org/10.3390/life15081186
APA StyleRadu, A., Jurca, T., Radu, A.-F., Bodog, T. M., Bodog, R. F., & Endres, L. (2025). A Multimodal Approach to Managing Severe Psoriasis Vulgaris: A Case Report Leveraging Natural Therapies for Flare Control. Life, 15(8), 1186. https://doi.org/10.3390/life15081186