

Physiological and Oxidative Stress in General and Spinal Anesthesia for Elective Cesarean Section in Women: Is There Any Difference?

 , , , , , , , , ,
, , , , , , , , ,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Selection of Participants
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Study Sample
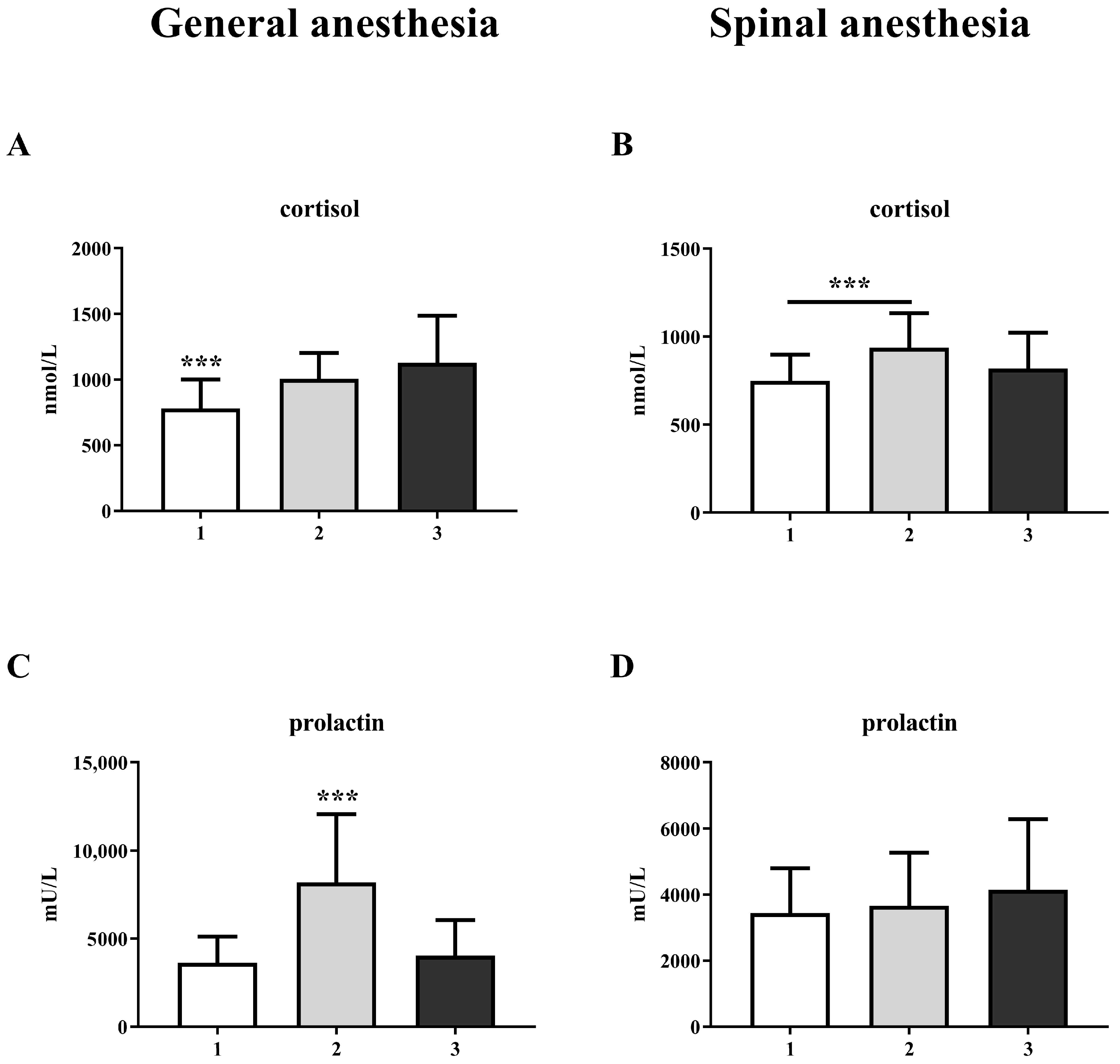
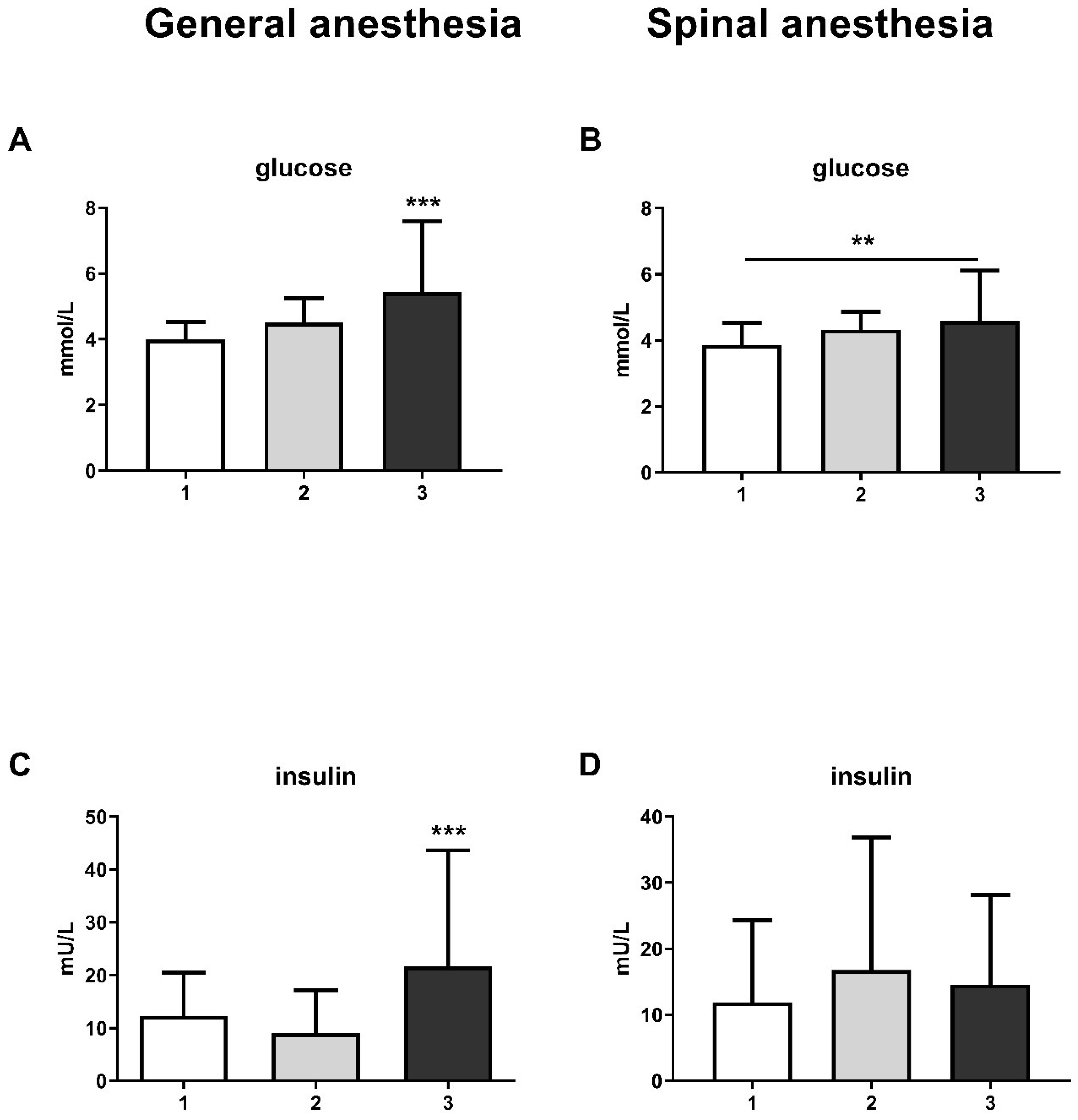
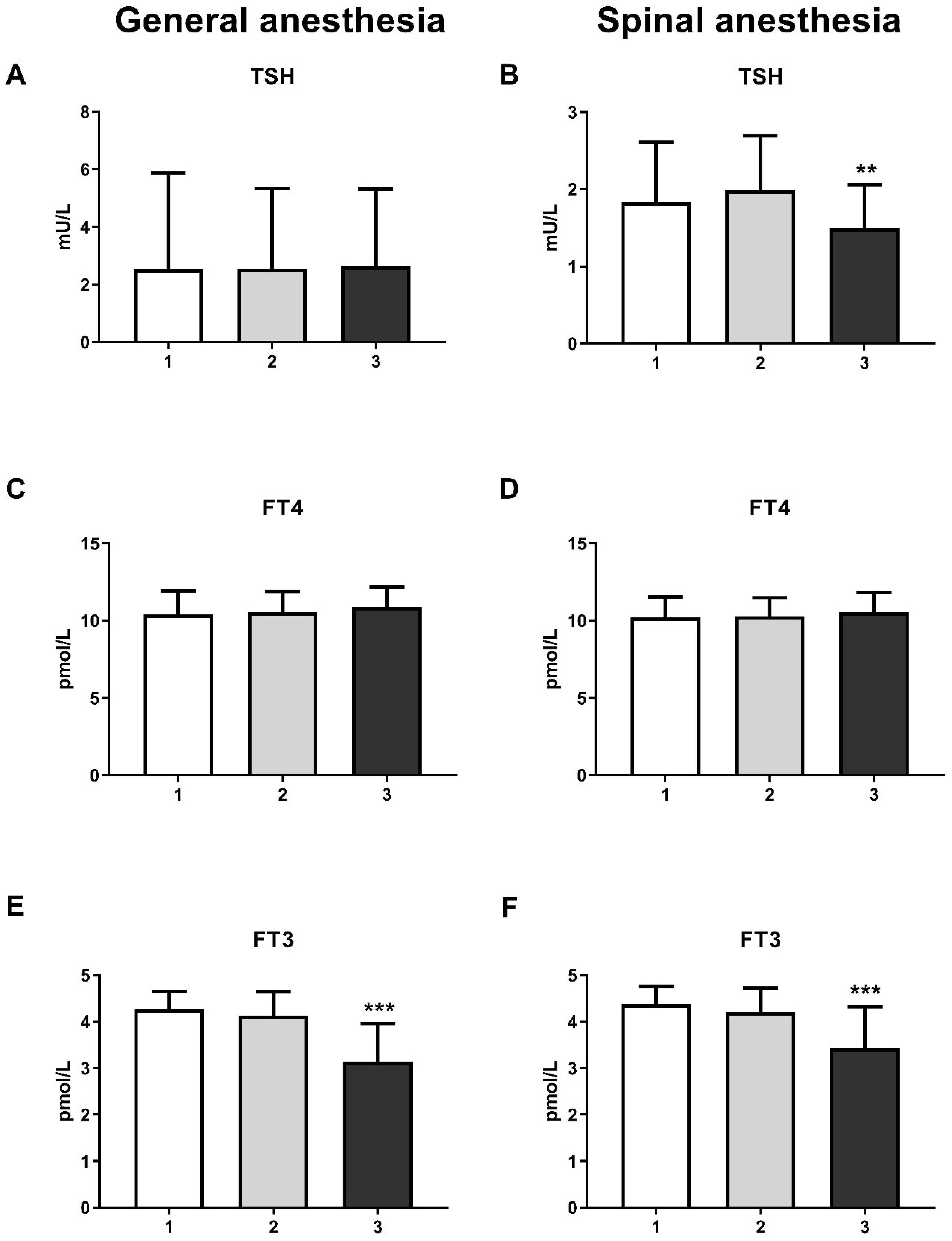
3.2. Laboratory Findings/Biochemical Parameters Associated with Stress
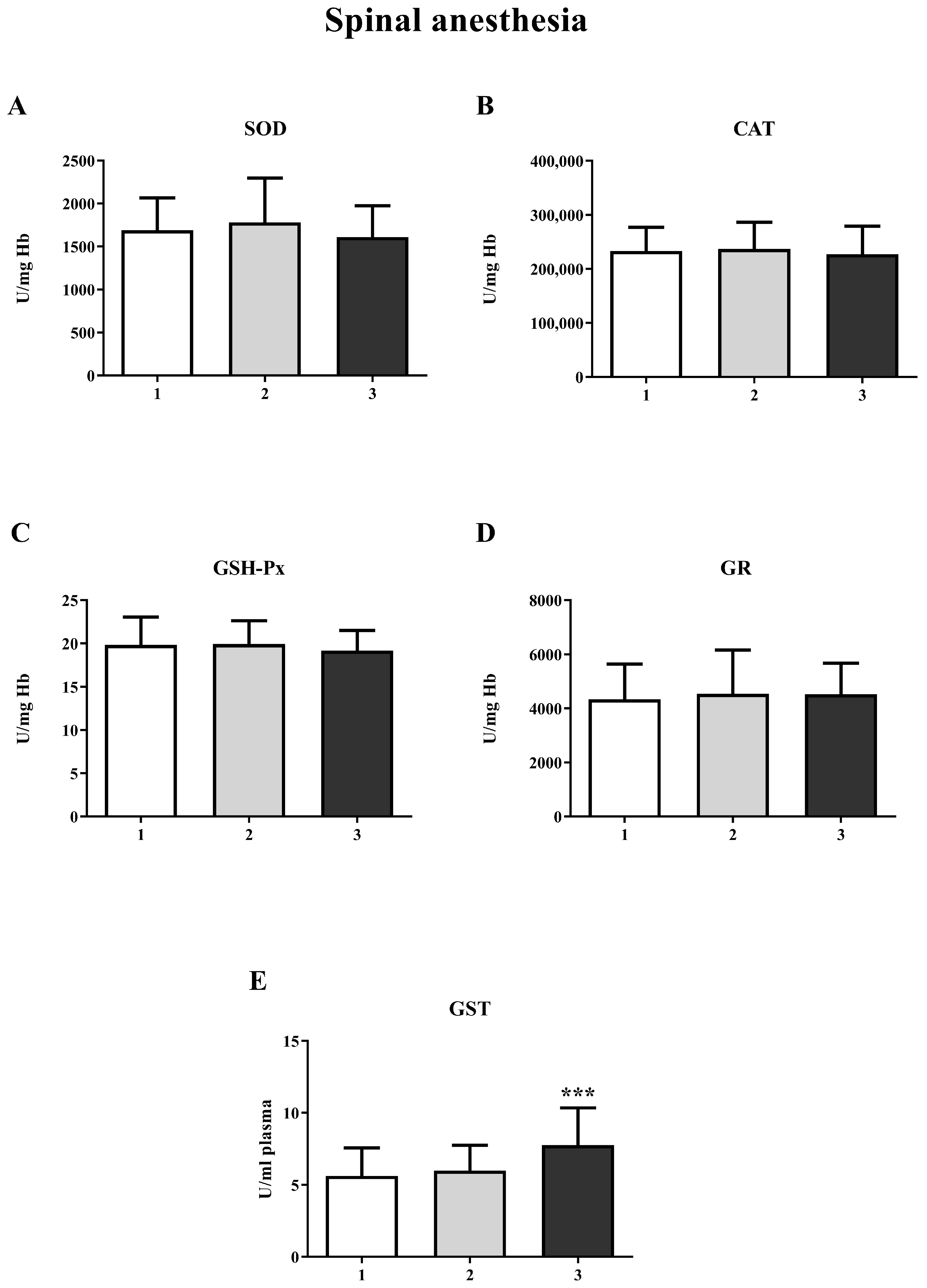
3.3. Analysis of Changes in Biomarkers of Oxidative Stress over Three Measurements Between Groups
3.4. Predictors of Changes in Biomarkers of Oxidative Stress over Three Measurements Between Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Betran, A.P.; Ye, J.; Moller, A.B.; Zhang, J.; Gulmezoglu, A.M.; Torloni, M.R. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLoS ONE 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed]
- Chien, P. Global Rising Rates of Caesarean Sections. BJOG 2021, 128, 781–782. [Google Scholar] [CrossRef] [PubMed]
- Sandall, J.; Tribe, R.-M.; Avery, L.; Mola, G.; Visser, G.-H.; Homer, C.-S.; Gibbons, D.; Kelly, N.-M.; Kennedy, H.-P.; Kidanto, H.; et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet 2018, 392, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Mhyre, J.M.; Sultan, P. General Anesthesia for Cesarean Delivery: Occasionally Essential but Best Avoided. Anesthesiology 2019, 130, 864–866. [Google Scholar] [CrossRef]
- Cusack, B.; Buggy, D.J. Anaesthesia, Analgesia, and the Surgical Stress Response. BJA Educ. 2020, 20, 321–328. [Google Scholar] [CrossRef]
- Traynor, A.J.; Aragon, M.; Ghosh, D.; Choi, R.S.; Dingmann, C.; Vu Tran, Z.; Bucklin, B.A. Obstetric Anesthesia Workforce Survey: A 30-Year Update. Anesth. Analg. 2016, 122, 1939–1946. [Google Scholar] [CrossRef]
- Guglielminotti, J.; Landau, R.; Li, G. Adverse Events and Factors Associated with Potentially Avoidable Use of General Anesthesia in Cesarean Deliveries. Anesthesiology 2019, 130, 912–922. [Google Scholar] [CrossRef]
- Ring, L.; Landau, R.; Delgado, C. The Current Role of General Anesthesia for Cesarean Delivery. Curr. Anesth. Rep. 2021, 11, 18–27. [Google Scholar] [CrossRef]
- Sung, T.-Y.; Jee, Y.-S.; You, H.-J.; Cho, C.-K. Comparison of the effect of general and spinal anesthesia for elective cesarean section on maternal and fetal outcomes: A retrospective cohort study. Anesth. Pain. Med. 2021, 16, 49–55. [Google Scholar] [CrossRef]
- Finnerty, C.C.; Mabvuure, N.T.; Ali, A.; Kozar, R.A.; Herndon, D.N. The Surgically Induced Stress Response. JPEN J. Parenter. Enter. Nutr. 2013, 37, 21S–29S. [Google Scholar] [CrossRef]
- Desborough, J.-P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef]
- Solberg, R.; Perrone, S.; Saugstad, O.D.; Buonocore, G. Risks and Benefits of Oxygen in the Delivery Room. J. Matern. Fetal Neonatal Med. 2012, 25, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Raptova, R.; Alomar, S.-Y.; Alwasel, S.-H.; Nepovimova, E.; Kuca, K.; Valko, M. Reactive oxygen species, toxicity, oxidative stress, and antioxidants: Chronic diseases and aging. Arch. Toxicol. 2023, 97, 2499–2574. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Alomar, S.-Y.; Alwasel, S.-H.; Nepovimova, E.; Kuca, K.; Valko, M. Several lines of antioxidant defense against oxidative stress: Antioxidant enzymes, nanomaterials with multiple enzyme-mimicking activities, and low-molecular-weight antioxidants. Arch. Toxicol. 2024, 98, 1323–1367. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y. Oxidative Stress Due to Anesthesia and Surgical Trauma and Comparison of the Effects of Propofol and Thiopental in Dogs. J. Vet. Med. Sci. 2012, 74, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, D.; Mendonca, V.; Murthy, B.V.S. A Review of ASA Physical Status–Historical Perspectives and Modern Developments. Anaesthesia 2019, 74, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Jakovljević, D.; Nikolić, M.; Jovanović, V.; Vidonja Uzelac, T.; Nikolić-Kokić, A.; Novaković, E.; Miljević, Č.; Milovanović, M.; Blagojević, D. Influence of Long-Term Anti-Seizure Medications on Redox Parameters in Human Blood. Pharmaceuticals 2024, 17, 130. [Google Scholar] [CrossRef]
- Tatalović, N.; Vidonja Uzelac, T.; Mijović, M.; Koželj, G.; Nikolić-Kokić, A.; Oreščanin Dušić, Z.; Bresjanac, M.; Blagojević, D. Ibogaine Has Sex-Specific Plasma Bioavailability, Histopathological and Redox/Antioxidant Effects in Rat Liver and Kidneys: A Study on Females. Life 2022, 12, 16. [Google Scholar] [CrossRef]
- Vidonja Uzelac, T.; Tatalović, T.; Mijović, M.; Koželj, G.; Nikolić-Kokić, A.; Oreščanin Dušić, Z.; Bresjanac, M.; Blagojević, D. Effects of Ibogaine Per Os Application on Redox Homeostasis in Rat Liver and Erythrocytes. Arch. Biol. Sci. 2019, 71, 133–144. [Google Scholar] [CrossRef]
- Kovačević, R.; Andrić, N. Gonadotropin-Releasing Hormone, Gonadotropins and Prolactine. In Biology of the Female Reproductive System, 1st ed.; Kovačević, R., Andrić, N., Eds.; University of Novi Sad Faculty of Natural Sciences and Mathematics: Novi Sad, Serbia, 2024; pp. 92–100. [Google Scholar]
- Iwasaki, M.; Edmondson, M.; Sakamoto, A.; Ma, D. Anesthesia, Surgical Stress, and “Long-Term” Outcomes. Acta Anaesthesiol. Taiwanica 2015, 53, 99–104. [Google Scholar] [CrossRef]
- Mujagić, Z.; Čičko, E.; Vegar-Brozović, V.; Prašo, M. Serum Levels of Cortisol and Prolactin in Patients Treated Under Total Intravenous Anesthesia with Propofol-Fentanyl and Under Balanced Anesthesia with Isoflurane-Fentanyl. Open Med. J. 2008, 3, 459–463. [Google Scholar] [CrossRef]
- Risberg, A.; Sjoquist, M.; Wedenberg, K.; Larsson, A. Elevated Glucose Levels in Early Puerperium, and Association with High Cortisol Levels During Parturition. Scand. J. Clin. Lab. Investig. 2016, 76, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, D.S.; Daily, J.W.; Kim, S.H. Serum Prolactin Concentrations Determine Whether They Improve or Impair B-Cell Function and Insulin Sensitivity in Diabetic Rats. Diabetes Metab. Res. Rev. 2011, 27, 564–574. [Google Scholar] [CrossRef]
- Fujinaka, Y.; Takane, K.; Yamashita, H.; Vasavada, R.C. Lactogens Promote Beta Cell Survival Through JAK2/STAT5 Activation and Bcl-XL Upregulation. J. Biol. Chem. 2007, 282, 30707–30717. [Google Scholar] [CrossRef]
- Berinder, K.; Nystrom, T.; Hoybye, C.; Hall, K.; Hulting, A.L. Insulin Sensitivity and Lipid Profile in Prolactinoma Patients Before and After Normalization of Prolactin by Dopamine Agonist Therapy. Pituitary 2011, 14, 199–207. [Google Scholar] [CrossRef]
- Milosavljevic, S.B.; Pavlovic, A.P.; Trpkovic, S.V.; Ilic, A.N.; Sekulic, A.D. Influence of Spinal and General Anaesthesia on the Metabolic, Hormonal, and Haemodynamic Response in Elective Surgical Patients. Med. Sci. Monit. 2014, 20, 1833–1840. [Google Scholar] [CrossRef]
- Brown, E.D.L.; Obeng-Gyasi, B.; Hall, J.E.; Shekhar, S. The Thyroid Hormone Axis and Female Reproduction. Int. J. Mol. Sci. 2023, 24, 9815. [Google Scholar] [CrossRef]
- Ortiga-Carvalho, T.M.; Chiamolera, M.I.; Pazos-Moura, C.C.; Wondisford, F.E. Hypothalamus-Pituitary-Thyroid Axis. Compr. Physiol. 2016, 6, 1387–1428. [Google Scholar] [CrossRef]
- Polosa, P.; Vigneri, R.; Papalia, D.; Squatrito, S.; Motta, L. Inhibition by L-Triiodothyronine and Dexamethasone of TSH Response to Thyrotropin Releasing Hormon in Man. Ann. Endocrinol. 1972, 33, 593–597. [Google Scholar]
- Köhrle, J.; Frädrich, C. Deiodinases Control Local Cellular and Systemic Thyroid Hormone Availability. Free Radic. Biol. Med. 2022, 193, 59–79. [Google Scholar] [CrossRef]
- Aremu, P.; Ajayi, A.; Ben-Azu, B.; Orewole, O.; Umukoro, S. Spinal and General Anesthesia Produces Differential Effects on Oxidative Stress and Inflammatory Cytokines in Orthopedic Patients. Drug Metab. Pers. Ther. 2021, 36, 17–23. [Google Scholar] [CrossRef]
- Zhang, Y.; Zuo, Y.; Li, B.; Xie, J.; Ma, Z.; Thirupathi, A.; Yu, P.; Gao, G.; Shi, M.; Zhou, C.; et al. Propofol Prevents Oxidative Stress and Apoptosis by Regulating Iron Homeostasis and Targeting JAK/STAT3 Signaling in SH-SY5Y Cells. Brain Res. Bull. 2019, 153, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Zhuo, Q.; Zhou, Y.; Qian, Y. Propofol Protects Human Cardiac Cells Against Chemical Hypoxiainduced Injury by Regulating the JNK Signaling Pathways. Exp. Ther. Med. 2020, 19, 1864–1870. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, M.C. Effect of Propofol on Oxidative Stress Status in Erythrocytes from Dogs Under General Anesthesia. Acta Vet. Scand. 2012, 54, 76. [Google Scholar] [CrossRef] [PubMed]
- Vona, R.; Pallotta, L.; Cappelletti, M.; Severi, C.; Matarrese, P. The Impact of Oxidative Stress in Human Pathology: Focus on Gastrointestinal Disorders. Antioxidants 2021, 10, 201. [Google Scholar] [CrossRef]
- Kükürt, A.; Gelen, V.; Başer, Ö.-F.; Deveci, H.-A.; Karapehlivan, M. Thiols: Role in Oxidative Stress-Related Disorders. In Accenting Lipid Peroxidation; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Kotani, Y.; Shimazawa, M.; Yoshimura, S.; Iwama, T.; Hara, H. The Experimental and Clinical Pharmacology of Propofol, an Anesthetic Agent with Neuroprotective Properties. CNS Neurosci. Ther. 2008, 14, 95–106. [Google Scholar] [CrossRef]
- Inanır, A.; Sogut, E.; Ayan, M.; Inanır, S. Evaluation of Pain Intensity and Oxidative Stress Levels in Patients with Inflammatory and Non-Inflammatory Back Pain. Eur. J. Gen. Med. 2013, 10, 185–190. [Google Scholar] [CrossRef]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased Oxidative Stress in Obesity and Its Impact on Metabolic Syndrome. J. Clin. Investig. 2017, 114, 1752–1761. [Google Scholar] [CrossRef]
- Bogdanović Pristov, J.; Opačić, M.; Bajčetić, M.; Mandić, V.; Maglić, D.; Miković, Ž.; Spasojević, I. Oxidative Status of Maternal Blood in Pregnancies Burdened by Inherited Thrombophilias. PLoS ONE 2020, 15, e0234253. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | General Anesthesia Group (n = 51) | Spinal Anesthesia Group (n = 50) | Total | p |
|---|---|---|---|---|
| Age (years) | 33.1 ± 0.7 | 33.2 ± 0.6 | 33.1 ± 0.46 | 0.879 |
| Place of residence (%) | 0.057 | |||
| House | 27 (52.9) | 35 (71.4) | 62 (61.4) | |
| Apartment | 24 (47.1) | 14 (28.6) | 38 (37.6) | |
| Body mass index (kg/m2) | 28.6 ± 0.64 | 28.4 ± 0.56 | 28.5 ± 0.42 | 0.734 |
| Body mass index categories (%) | 0.828 | |||
| Underweight | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Normal weight | 8 (15.7) | 10 (20.0) | 18 (17.8) | |
| Overweight | 30 (58.8) | 25 (50.0) | 55 (54.5) | |
| Obese | 13 (25.5) | 15 (30.0) | 28 (27.7) | |
| Waist circumference (cm) | 102.7 ± 1.29 | 101.5 ± 1.04 | 102.1 ± 0.82 | 0.482 |
| Smoking status (%) | 0.147 | |||
| No | 25 (49.0) | 33 (66.0) | 58 (57.4) | |
| Yes | 13 (25.5) | 6 (12.0) | 19 (18.8) | |
| Ex smoker | 13 (25.5) | 11 (22.0) | 24 (23.8) | |
| Alcohol consumption (%) | 0.989 | |||
| No | 50 (98.0) | 49 (98.0) | 99 (98.0) | |
| Yes | 1 (2.0) | 1 (2.0) | 2 (2.0) | |
| Level of physical activity (%) | 0.811 | |||
| Low | 28 (54.9) | 28 (56.0) | 56 (55.4) | |
| Medium | 22 (43.1) | 20 (40.0) | 42 (41.6) | |
| High | 1 (2.0) | 2 (4.0) | 3 (3.0) | |
| Presence of comorbidity (%) | 0.469 | |||
| No | 28 (54.9) | 31 (62.0) | 59 (58.4) | |
| Yes | 23 (45.1) | 19 (38.0) | 42 (41.6) | |
| Type of comorbidity | 0.423 | |||
| Hypertension | 2 (3.9) | 2 (4.0) | 4 (4.0) | |
| Obesity | 10 (19.6) | 8 (16.0) | 18 (17.8) | |
| Diabetes | 0 (0.0) | 1 (2.0) | 1 (1.0) | |
| Insulin resistance | 7 (13.7) | 6 (12.0) | 13 (12.9) | |
| Asthma | 0 (0.0) | 2 (4.0) | 2 (2.0) | |
| Hypothireosis | 5 (9.8) | 9 (18.0) | 14 (13.9) | |
| Thrombophilia | 3 (5.9) | 4 (8.0) | 7 (6.9) | |
| Allergies (%) | 0.796 | |||
| No | 44 (86.3) | 44 (88.0) | 88 (87.1) | |
| Yes | 7 (13.7) | 6 (12.0) | 13 (12.9) | |
| Family history for cardiovascular disease, neurodegenerative or malignant diseases (%) | 0.197 | |||
| Yes | 31 (60.8) | 24 (48.0) | 46 (45.5) | |
| No | 20 (39.2) | 26 (52.0) | 55 (54.5) | |
| Previous surgical procedures (%) | 0.309 | |||
| Yes | 9 (17.6) | 13 (26.0) | 22 (21.8) | |
| No | 42 (82.4) | 37 (74.0) | 79 (79.2) | |
| Gestational week | 0.506 | |||
| 37 | 1 (2.0) | 0 (0.0) | 1 (1.0) | |
| 38 | 6 (11.8) | 2 (4.0) | 8 (7.9) | |
| 39 | 24 (47.1) | 25 (50.0) | 49 (48.5) | |
| 40 | 18 (35.3) | 20 (40.0) | 38 (37.6) | |
| 41 | 2 (3.9) | 3 (6.0) | 5 (5.0) |
| GST | CAT | GSH-Px | GR | SOD | SH Groups | Non-Protein SH |
|---|---|---|---|---|---|---|
| BMI Smoking status Neutrophils Lymphocytes * Bicarbonates Potassium C-reactive protein Cortisol Prolactin | Thrombophilia Lymphocytes Potassium Lipase Alanine transaminase TSH | Presence of comorbidity Hypothireosis Thrombophilia Alanine transaminase * TSH | Omega-3 supplementation Obesity ** Thrombophilia ** Leukocytes * Aspartate transferase | Folic acid supplementation Magnesium supplementation Potassium | Place of residence Comorbid allergies Hemoglobin Hematocrit Neutrophils Leukocytes | Hypothireosis Thrombophilia Lipase Insulin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimic, N.D.; Maric, G.D.; Orescanin Dusic, Z.S.; Grahovac, T.M.; Vidonja Uzelac, T.F.; Djuric, M.D.; Nenadic, I.B.; Bobos, M.M.; Stevanovic, P.D.; Mihajlovic, S.J.; et al. Physiological and Oxidative Stress in General and Spinal Anesthesia for Elective Cesarean Section in Women: Is There Any Difference? Life 2025, 15, 1158. https://doi.org/10.3390/life15081158
Dimic ND, Maric GD, Orescanin Dusic ZS, Grahovac TM, Vidonja Uzelac TF, Djuric MD, Nenadic IB, Bobos MM, Stevanovic PD, Mihajlovic SJ, et al. Physiological and Oxidative Stress in General and Spinal Anesthesia for Elective Cesarean Section in Women: Is There Any Difference? Life. 2025; 15(8):1158. https://doi.org/10.3390/life15081158
Chicago/Turabian StyleDimic, Nemanja D., Gorica D. Maric, Zorana S. Orescanin Dusic, Tanja M. Grahovac, Teodora F. Vidonja Uzelac, Marko D. Djuric, Irina B. Nenadic, Marina M. Bobos, Predrag D. Stevanovic, Sladjana J. Mihajlovic, and et al. 2025. "Physiological and Oxidative Stress in General and Spinal Anesthesia for Elective Cesarean Section in Women: Is There Any Difference?" Life 15, no. 8: 1158. https://doi.org/10.3390/life15081158
APA StyleDimic, N. D., Maric, G. D., Orescanin Dusic, Z. S., Grahovac, T. M., Vidonja Uzelac, T. F., Djuric, M. D., Nenadic, I. B., Bobos, M. M., Stevanovic, P. D., Mihajlovic, S. J., & Stojanovic, M. M. (2025). Physiological and Oxidative Stress in General and Spinal Anesthesia for Elective Cesarean Section in Women: Is There Any Difference? Life, 15(8), 1158. https://doi.org/10.3390/life15081158