
Children’s Headache Through Drawings: A Narrative Review and a Portrait Gallery

 , and
, and
Abstract
1. Introduction
2. Review of Literature
2.1. Headache in Children’s Drawings
- High diagnostic sensitivity: the study by Stafstrom et al. [11] reported a sensitivity of 93% and a specificity of 83% in using drawings for headache diagnosis.
- Symbolic and chromatic elements: Drawings frequently included elements such as lightning bolts, tears, and dark colors associated with migraines. For instance, Mosquera et al. (2008) [17] observed that 75% of children with migraines depicted unilateral pain, while 60% used symbolic elements like lightning bolts or tears. Similarly, Wojaczynska-Stanek et al. (2008) [16] found that 73% of children with headaches used dark colors, suggesting a correlation between color tone and pain intensity.
2.2. Drawing Use in the Adult Population
2.3. The Use of Pain Charts
2.4. Children’s Pain Perception and Expression
3. Correlation Between the Clinical Phenotypes and the Graphic Representation of Pain
3.1. Migraine with Aura in Children
- Gradual appearance of a symptom over five minutes or more;
- At least two symptoms occurring sequentially;
- Each symptom lasts between 5 and 60 min;
- At least one aura symptom is unilateral;
- At least one positive symptom (e.g., flickering lights, tingling);
- The aura is followed by or coincides with a headache within one hour.
- Blurred vision;
- Zigzag lines;
- Scotomata (partial vision loss);
- Scintillations (flashes of light);
- Black dots;
- Kaleidoscopic patterns;
- Size perception distortions (micropsia/macropsia).
3.2. Neurological Mechanisms of Aura
3.3. Differential Diagnosis Between Visual Hallucinations in Migraine with Aura and Epilepsy
3.4. Migraine Triggers in Children
4. Future Directions
5. Gallery
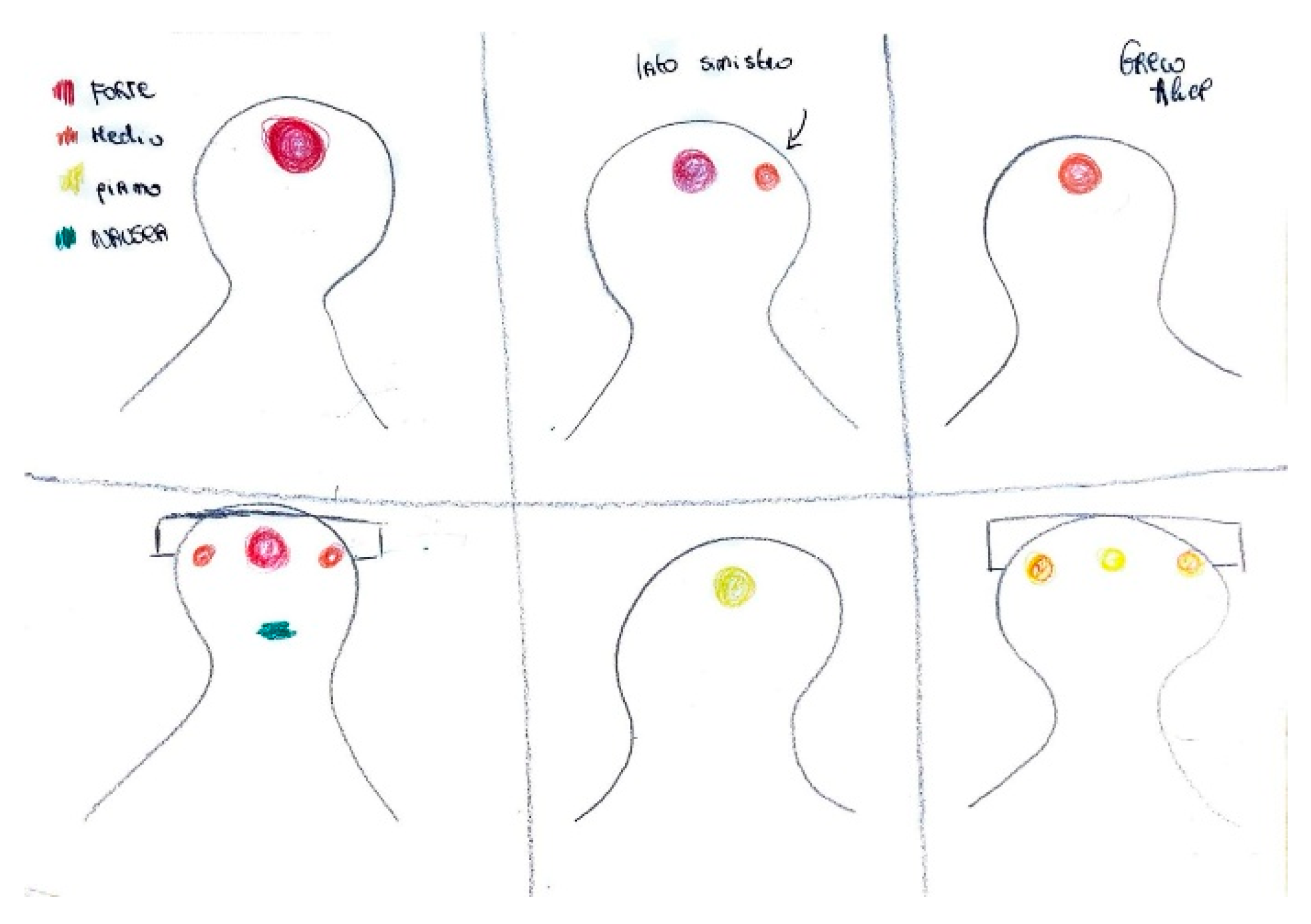
5.1. Intensity of Pain
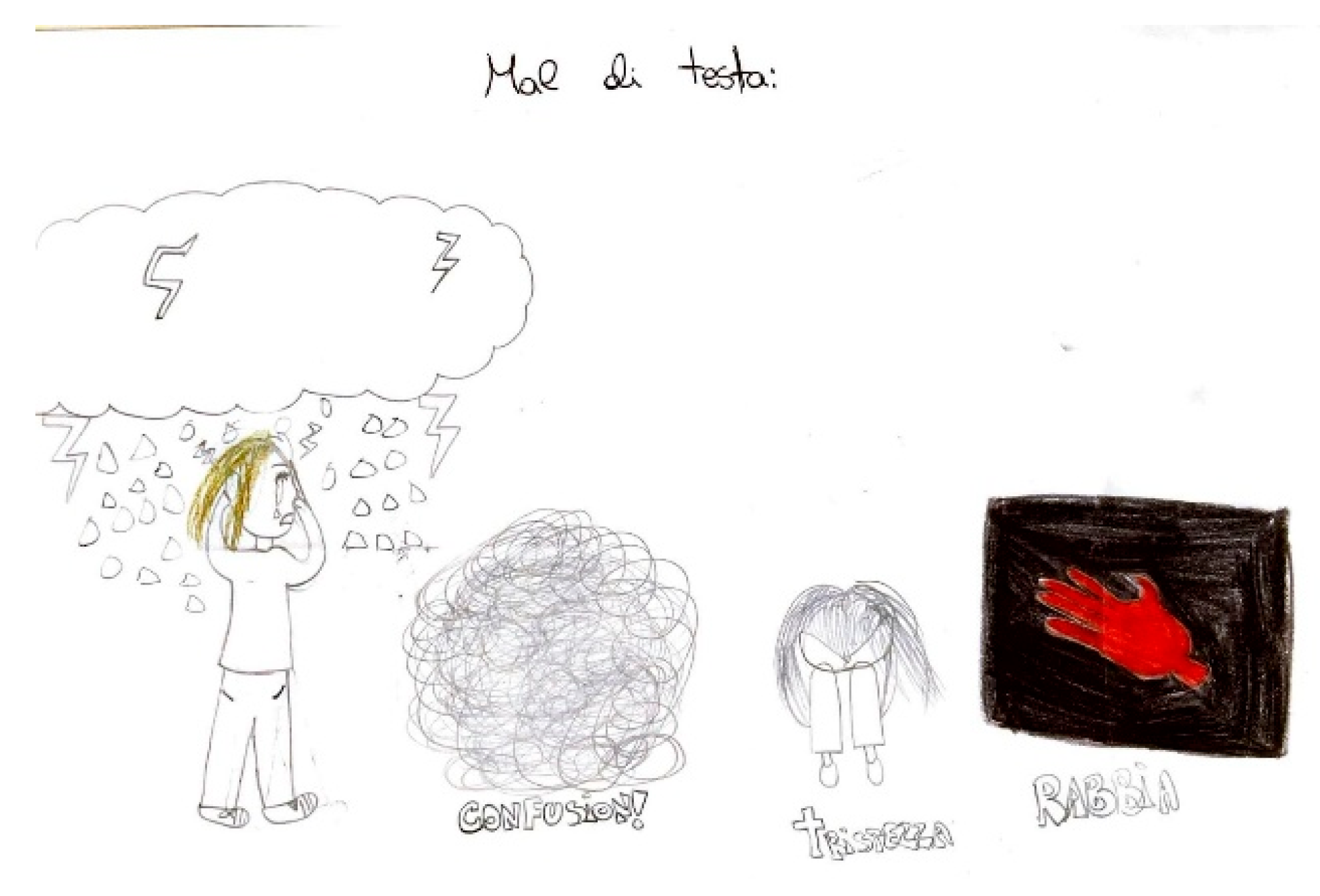
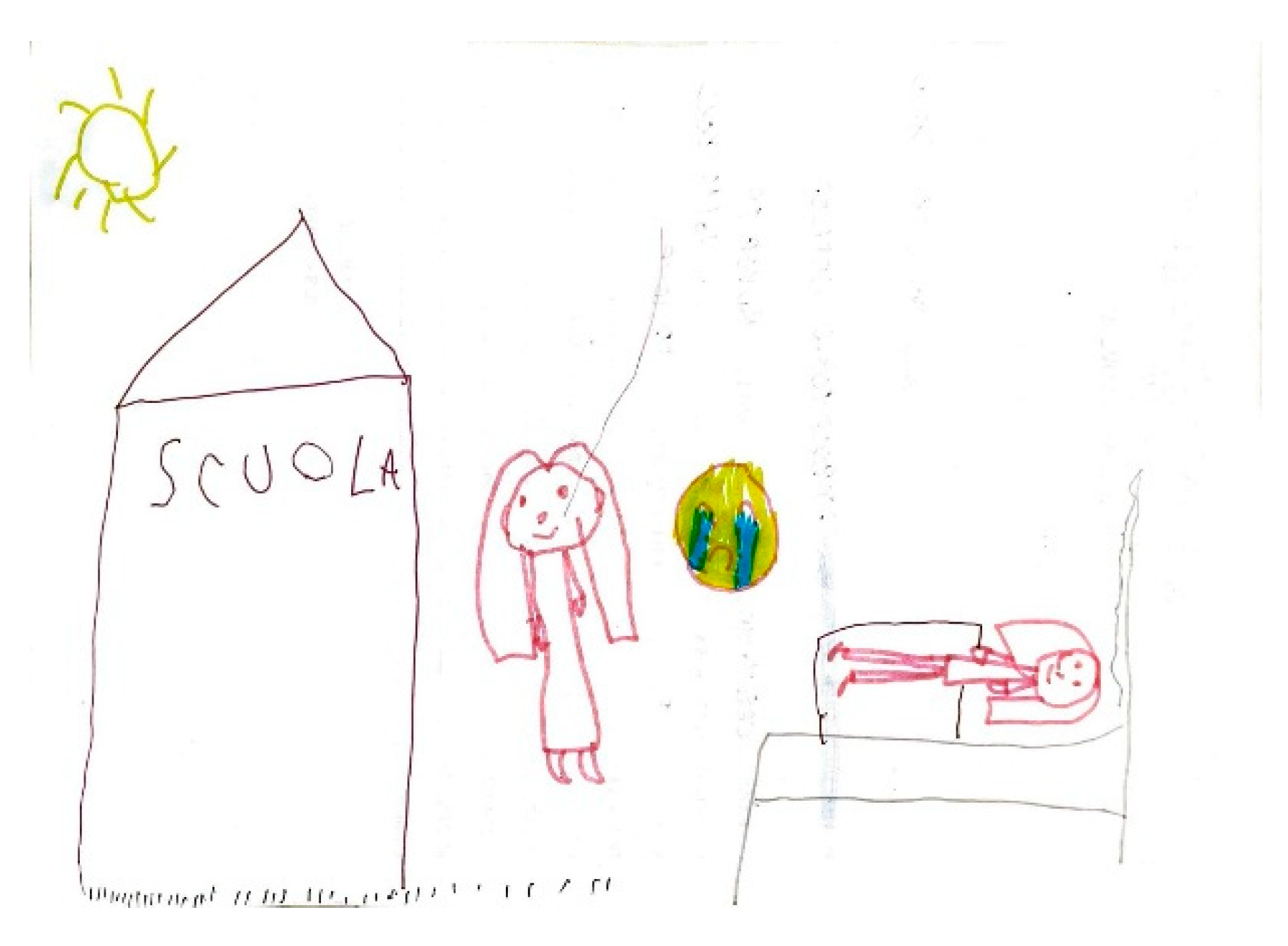
5.2. Related Symptoms and Behaviors
5.3. Aura
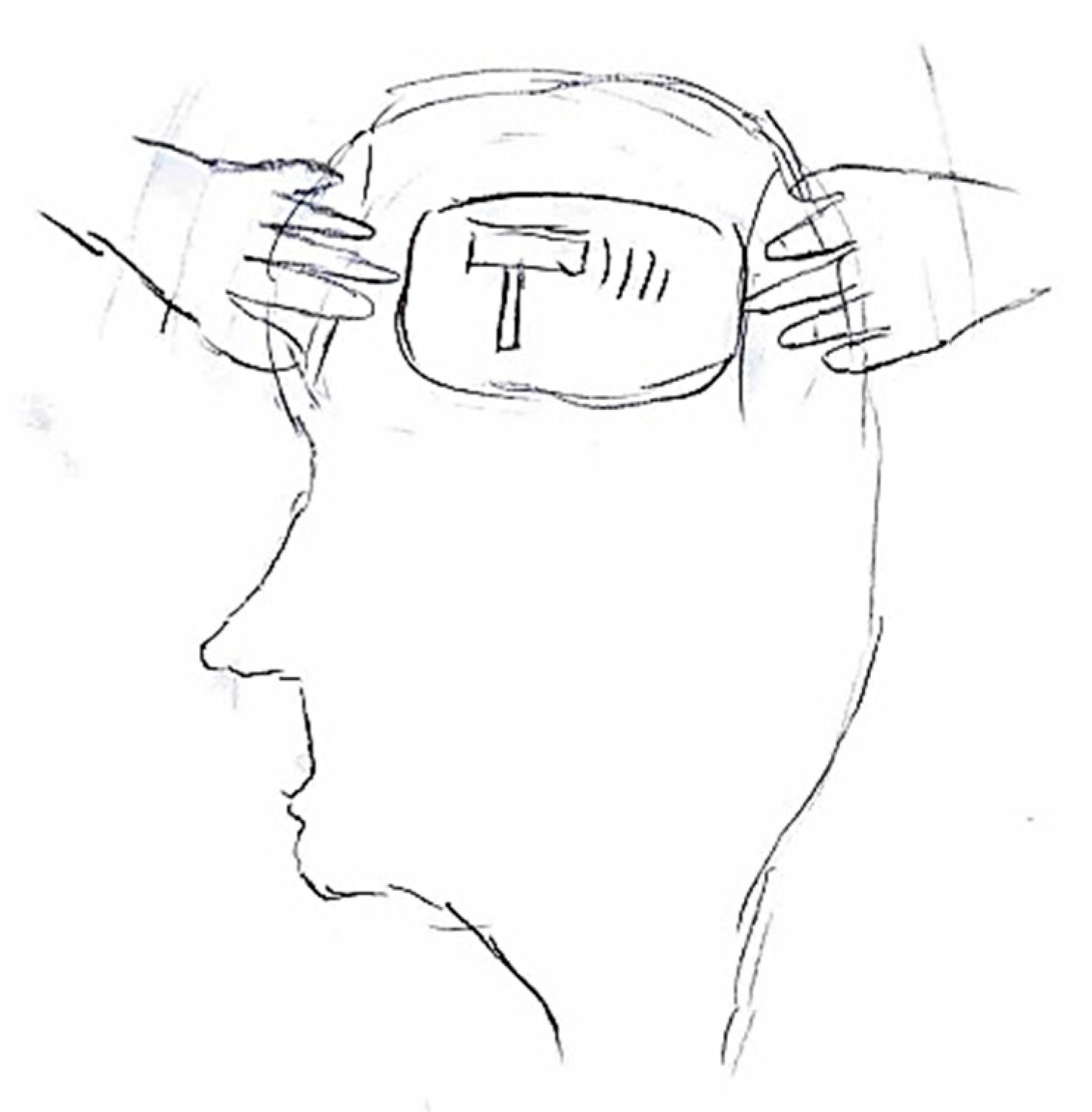
5.4. Alleviating Factors and Therapies
5.5. Expression of Pain
5.6. Representation of Pain in Adolescents
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ICHD-3 | International Classification of Headache Disorders |
| PPV | positive predictive value |
| IHS | International Headache Society |
| CSD | cortical spreading depression |
References
- Dao, J.M.; Qubty, W. Headache Diagnosis in Children and Adolescents. Curr. Pain Headache Rep. 2018, 22, 17. [Google Scholar] [CrossRef]
- Onofri, A.; Pensato, U.; Rosignoli, C.; Wells-Gatnik, W.; Stanyer, E.; Ornello, R.; Chen, H.Z.; De Santis, F.; Torrente, A.; Mikulenka, P.; et al. Primary headache epidemiology in children and adolescents: A systematic review and meta-analysis. J. Headache Pain 2023, 24, 8. [Google Scholar] [CrossRef] [PubMed]
- Özge, A.; Faedda, N.; Abu-Arafeh, I.; Gelfand, A.A.; Goadsby, P.J.; Cuvellier, J.C.; Valeriani, M.; Sergeev, A.; Barlow, K.; Uludüz, D.; et al. Experts’ opinion about the primary headache diagnostic criteria of the ICHD-3rd edition beta in children and adolescents. J. Headache Pain 2017, 18, 109. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.W.; Patton, S.R.; Hommel, K.A.; Hershey, A.D. Quality of Life in Childhood Migraines: Clinical Impact and Comparison to Other Chronic Illnesses. Pediatrics 2003, 112, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Papetti, L.; Salfa, I.; Battan, B.; Moavero, R.; Termine, C.; Bartoli, B.; Di Nunzio, F.; Tarantino, S.; Di Loro, P.A.; Vigevano, F.; et al. Features of Primary Chronic Headache in Children and Adolescents and Validity of Ichd 3 Criteria. Front. Neurol. 2019, 10, 92. [Google Scholar] [CrossRef]
- Abu-Arafeh, I.; Callaghan, M. Short Migraine Attacks of less than 2 h Duration in Children and Adolescents. Cephalalgia 2004, 24, 333–338. [Google Scholar] [CrossRef]
- de Grauw, T.J.; Hershey, A.D.; Powers, S.W.; Bentti, A. Diagnosis of Migraine in Children Attending a Pediatric Headache Clinic. Headache 1999, 39, 481–485. [Google Scholar] [CrossRef]
- Chakravarty, A.; Mukherjee, A.; Roy, D. Migraine pain location: How do children differ from adults? J. Headache Pain 2008, 9, 375–379. [Google Scholar] [CrossRef]
- Chakravarty, A.; Mukherjee, A.; Roy, D. Migraine Pain Location at Onset and During Established Headaches in Children and Adolescents: A Clinic-Based Study from Eastern India. Cephalalgia 2007, 27, 1109–1114. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Stafstrom, C.E.; Rostasy, K.; Minster, A. The Usefulness of Children’s Drawings in the Diagnosis of Headache. Pediatrics 2002, 109, 460–472. [Google Scholar] [CrossRef] [PubMed]
- Karsan, N.; Prabhakar, P.; Goadsby, P.J. Extended Phenotyping of Migraine in Children: A Cross-Sectional Study in a Specialist Children’s Headache Clinic. Pediatr. Neurol. 2024, 156, 33–40. [Google Scholar] [CrossRef]
- Raieli, V.; Compagno, A.; Pandolfi, E.; La Vecchia, M.; Puma, D.; La Franca, G.; Ragusa, D. Headache: What Do Children and Mothers Expect From Pediatricians? Headache J. Head Face Pain 2010, 50, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Unruh, A.; McGrath, P.; Cunningham, J.S.; Humphreys, P. Children’s drawings of their pain. Pain 1983, 17, 385–392. [Google Scholar] [CrossRef]
- Stafstrom, C.E.; Goldenholz, S.R.; Dulli, D.A. Serial Headache Drawings by Children With Migraine: Correlation With Clinical Headache Status. J. Child Neurol. 2005, 20, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Wojaczyńska-Stanek, K.; Koprowski, R.; Wróbel, Z.; Gola, M. Headache in Children’s Drawings. J. Child Neurol. 2008, 23, 184–191. [Google Scholar] [CrossRef]
- Mosquera, M.S.; Martino, G.H. Children and adolescent’s drawing for the diagnosis of migraine. Arch. Argent. Pediatr. 2008, 106, 11–18. [Google Scholar]
- Pavlidis, E.; Cordori, C.; Spagnoli, C.; Pini, L.A.; Pisani, F.; Mazzotta, S. Children’s Headache: Drawings in the Diagnostic Work Up. Neuropediatrics 2015, 46, 261–268. [Google Scholar] [CrossRef]
- Yilmaz, A.; Gunce, E.; Kirci, N.; Zeynep Goker, Z. Pictures portrayed by children with migraine with aura: A Turkish case series. Neurological Sci. 2019, 40, 839–845. [Google Scholar] [CrossRef]
- García-Ron, A.; Arias-Vivas, E.; Bote-Gascón, M.; González-García, N.; Porta-Etessam, J. Usefulness of spontaneous drawing in the diagnostic guidance of pediatric patients with headache. Rev. Neurol. 2024, 79, 265–271. [Google Scholar] [CrossRef]
- Buture, A.; Boland, J.W.; Ahmed, F.; Dikomitis, L. Images depicting headache pain—A tool to aid the diagnosis of cluster headache: A pilot study. J. Multidiscip. Healthc. 2019, 12, 691–698. [Google Scholar] [CrossRef] [PubMed]
- von Baeyer, C.L.; Lin, V.; Seidman, L.C.; Tsao, J.C.; Zeltzer, L.K. Pain Charts (Body Maps or Manikins) In Assessment of the Location of Pediatric Pain. Pain Manag. 2011, 1, 61–68. [Google Scholar] [CrossRef]
- Paananen, M.V.; Auvinen, J.P.; Taimela, S.P.; Tammelin, T.H.; Kantomaa, M.T.; Ebeling, H.E.; Taanila, A.M.; Zitting, P.J.; Karppinen, J.I. Psychosocial, mechanical, and metabolic factors in adolescents’ musculoskeletal pain in multiple locations: A cross-sectional study. Eur. J. Pain 2009, 14, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Bienvenu, M.; Jacquet, D.; Michelutti, M.; Wood, C. L’Expression Verbale de la Douleur chez l’Enfant: Comparaison Intermodale entre Sensation de Douleur et Manipulation Tactile. Pain Res. Manag. 2011, 16, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Mazur, A.; Radziewicz Winnicki, I.; Szczepański, T.T. Pain management in children. Ann. Agric. Environ. Med. 2013, 1, 28–34. [Google Scholar]
- Meldrum, M.L.; Tsao, J.C.-I.; Zeltzer, L.K. “I Can’t Be What I Want to Be”: Children’s Narratives of Chronic Pain Experiences and Treatment Outcomes. Pain Med. 2009, 10, 1018–1034. [Google Scholar] [CrossRef]
- Savedra, M.; Gibbons, P.; Tesler, M.; Ward, J.; Wegner, C. How do children describe pain? A tentative assessment. Pain 1982, 14, 95–104. [Google Scholar] [CrossRef]
- Hermann, C.; Blanchard, E.B. Biofeedback in the Treatment of Headache and Other Childhood Pain. Appl. Psychophysiol. Biofeedback 2002, 27, 143–162. [Google Scholar] [CrossRef]
- Robins, P.M.; Smith, S.M.; Glutting, J.J.; Bishop, C.T. A Randomized Controlled Trial of a Cognitive-Behavioral Family Intervention for Pediatric Recurrent Abdominal Pain. J. Pediatr. Psychol. 2005, 30, 397–408. [Google Scholar] [CrossRef]
- Jongudomkarn, D.; Aungsupakorn, N.; Camfield, L. The meanings of pain: A qualitative study of the perspectives of children living with pain in north-eastern Thailand. Nurs. Health Sci. 2006, 8, 156–163. [Google Scholar] [CrossRef]
- Kortesluoma, R.-L.; Nikkonen, M.; Serlo, W. “You Just Have to Make the Pain Go Away”—Children’s Experiences of Pain Management. Pain Manag. Nurs. 2008, 9, 143–149.e5. [Google Scholar] [CrossRef] [PubMed]
- Kortesluoma, R.-L.; Punamäki, R.-L.; Nikkonen, M. Hospitalized children drawing their pain: The contents and cognitive and emotional characteristics of pain drawings. J. Child Health Care 2008, 12, 284–300. [Google Scholar] [CrossRef]
- Ebrahimpour, F.; Pashaeypoor, S.; Salisu, W.J.; Cheraghi, M.A.; Hosseini, A.S.S. Children’s description of pain through drawings and dialogs: A concept analysis. Nurs. Open 2019, 6, 301–312. [Google Scholar] [CrossRef]
- Correnti, E.; Cascio, S.L.; Cernigliaro, F.; Rossi, R.; D’agnano, D.; Grasso, G.; Pellegrino, A.; Lauria, B.; Santangelo, A.; Santangelo, G.; et al. Idiopathic Non-Dental Facial Pain Syndromes in Italian Children: A Clinical Case Series. Life 2023, 13, 861. [Google Scholar] [CrossRef] [PubMed]
- Frattale, I.; Sciruicchio, V.; D’aGnano, D.; Raieli, V.; Cascio, S.L.; Santangelo, G.; Correnti, E.; Ursitti, F.; Sforza, G.; Monte, G.; et al. Diagnosing migraine in children and adolescence using ID migraine: Results of an Italian multicenter validation. Neurol. Sci. 2025, 46, 3213–3220. [Google Scholar] [CrossRef]
- Lewis, D.W.; Middlebrook, M.T.; Mehallick, L.; Rauch, T.M.; Deline, C.; Thomas, E.F. Pediatric Headaches: What Do the Children Want? Headache 1996, 36, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, H.F.; Lebel, A. Pediatric Episodic Migraine with Aura: A Unique Entity? Children 2021, 8, 228. [Google Scholar] [CrossRef]
- Balestri, M.; Papetti, L.; Maiorani, D.; Capuano, A.; Tarantino, S.; Battan, B.; Vigevano, F.; Valeriani, M. Features of aura in paediatric migraine diagnosed using the ICHD 3 beta criteria. Cephalalgia 2018, 38, 1742–1747. [Google Scholar] [CrossRef]
- E Youssef, P.; Mack, K.J. Episodic and chronic migraine in children. Dev. Med. Child Neurol. 2020, 62, 34–41. [Google Scholar] [CrossRef]
- Fischer-Schulte, L.H.; Peng, K.-P. Migraine prodromes and migraine triggers. Handb. Clin. Neurol. 2023, 198, 135–148. [Google Scholar] [CrossRef]
- Charles, A.C.; Baca, S.M. Cortical spreading depression and migraine. Nat. Rev. Neurol. 2013, 9, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.A.; Panonnummal, R. Cortical spreading depression: Culprits and mechanisms. Exp. Brain Res. 2022, 240, 733–749. [Google Scholar] [CrossRef] [PubMed]
- D’agnano, D.; Cascio, S.L.; Correnti, E.; Raieli, V.; Sciruicchio, V. A Narrative Review of Visual Hallucinations in Migraine and Epilepsy: Similarities and Differences in Children and Adolescents. Brain Sci. 2023, 13, 643. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Liu, S.; Tao, F. Current Trends in Pediatric Migraine: Clinical Insights and Therapeutic Strategies. Brain Sci. 2025, 15, 280. [Google Scholar] [CrossRef]
- Orak, S.A.; Polat, M.; Pak, M.; Kubur, Ç.Ç.; Atasever, A.K.; Yilmaz, C.; Taneli, F.; Angin, A.; Özyurt, B.C. Can serum neuropeptide levels help diagnose pediatric migraine? A prospective case–control study. Headache, 2025; ahead of print. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | Age and Gender | Materials Methods | Results | |
|---|---|---|---|---|
| Unruh et al. (1983) [14] | 109 | 5–18 years; 66 females, 43 males | Children were asked to draw their pain and how they experience it. Drawings were analyzed for symbolic and emotional elements. | 32% of children depicted actions or instruments causing pain, 19% personified the pain, 25% used abstract representations, and 11% localized the pain on the body. Children with migraine frequently depicted themselves relieving their pain (48%) compared to those with musculo-skeletal pain (31%). Red and black were the most dominant colors. |
| Stafstrom et al. (2002) [11] | 226 | 4–19 years; 105 males and 121 females | Children created drawings depicting pain localization, intensity, and related emotions. Two pediatric neurologists analyzed the drawings against clinical diagnosis. | Headache drawings showed a sensitivity of 93% and a specificity of 83% compared to clinical diagnosis. A total of 90% included precise pain localization; 78% showed emotional content; 68% included metaphorical elements like lightning bolts linked to migraines. |
| Wojaczynska-Stanek et al. (2008) [16] | 124 | 5–18 years; 68 females, 56 males | 124 children (40 migraines, 47 tension headaches, 37 others) provided pain drawings, analyzed for patterns in localization, color, and symbolic elements. | Pain localization in 68% of drawings, symbolic elements in 25%, and 73% dark colors; migraines often had unilateral depictions. |
| Mosquera et al. (2008) [17] | 48 | 5–19 years; gender not specified | Children drew their headache perceptions. Drawings were evaluated by a pediatric neurologist and compared with clinical findings. | 75% depicted unilateral pain, 60% used symbolic elements (lightning bolts, tears), 80% used black or gray, correlating with migraine characteristics. |
| Mazzotta et al. (2015) [18] | 67 | 6–14 years; gender not specified | 67 children with headaches and 90 controls created drawings. Two child neuropsychiatrists blinded to clinical data analyzed the patterns. | 78% of drawings localized pain; 48% included symbolic imagery (e.g., lightning bolts). Sensitivity for migraines: 85.71%; tension headaches: 81.48%. |
| Yilmaz et al. (2019) [19] | 5 | 14–18 years; 3 females, 2 males | Adolescents with migraines and visual aura were asked to depict their symptoms, focusing on visual disturbances like zigzag lines and scotomas. | 100% depicted visual aura symptoms, including zigzag lines and scotomas, confirming their diagnostic value for adolescents. |
| Garcia-Ron et al. (2024) [20] | 132 | 12 years (mean); 61.1% females | Children with headaches drew their pain experiences without instructions. Neuropediatricians and neurologists assessed the drawings for diagnostic insights. | 78.5% concordance for migraines and 78.6% for tension headaches; migraine features like aura and nausea showed 100% diagnostic match. |
| Localization of pain | Unilateral: (Migraine–PPV 63.6%) [11]
|
| Quality of pain | Pulsating: (Migraine–PPV 83.2%) [11]
|
| Intensity of pain | (Migraine–PPV n.a.) Lower:
|
| Aggravation by or causing avoidance of routine physical activity |
|
| Nausea | (Migraine–PPV 90.9%) [11]
|
| Vomiting | (Migraine–PPV 90.9%) [11]
|
| Photophobia | (Migraine–PPV 91.3%) [11]
|
| Phonophobia | (Migraine–PPV 80%) [11]
|
| Visual aura | (Migraine–PPV 95%) [11]
|
| Sensory aura | (Migraine–PPV n.a.)
|
| Aphasia or Disartria | (Migraine–PPV n.a.)
|
| Motor aura | (Migraine–PPV 63.6%) [11]
|
| Brainstem aura | (Migraine–PPV n.a.)
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferro, F.; Gaspari, C.; Manfrè, G.; Cernigliaro, F.; D’Agnano, D.; Panzica, R.; Correnti, E.; Ruta, M.R.; Marchese, F.; Pitino, R.; et al. Children’s Headache Through Drawings: A Narrative Review and a Portrait Gallery. Life 2025, 15, 996. https://doi.org/10.3390/life15070996
Ferro F, Gaspari C, Manfrè G, Cernigliaro F, D’Agnano D, Panzica R, Correnti E, Ruta MR, Marchese F, Pitino R, et al. Children’s Headache Through Drawings: A Narrative Review and a Portrait Gallery. Life. 2025; 15(7):996. https://doi.org/10.3390/life15070996
Chicago/Turabian StyleFerro, Floriana, Caterina Gaspari, Giulia Manfrè, Federica Cernigliaro, Daniela D’Agnano, Ruben Panzica, Edvige Correnti, Maria Rosita Ruta, Francesca Marchese, Renata Pitino, and et al. 2025. "Children’s Headache Through Drawings: A Narrative Review and a Portrait Gallery" Life 15, no. 7: 996. https://doi.org/10.3390/life15070996
APA StyleFerro, F., Gaspari, C., Manfrè, G., Cernigliaro, F., D’Agnano, D., Panzica, R., Correnti, E., Ruta, M. R., Marchese, F., Pitino, R., Capizzi, M., Santangelo, G., Versace, A., Sciruicchio, V., & Raieli, V. (2025). Children’s Headache Through Drawings: A Narrative Review and a Portrait Gallery. Life, 15(7), 996. https://doi.org/10.3390/life15070996