Cardiovascular Diseases and Type D Personality: Systematic Review and Meta-Analysis of the Literature of the Last 10 Years

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Strategies and Eligibility Criteria
2.2. Eligibility Criteria
2.3. Data Selection Process and Data Extraction
2.4. Qualitative Assessment: Risk of Bias of the Included Studies
2.5. Meta-Analysis Strategy
3. Results
3.1. Selection of the Studies
3.2. Results of the Selected Studies
3.2.1. Demographic Data
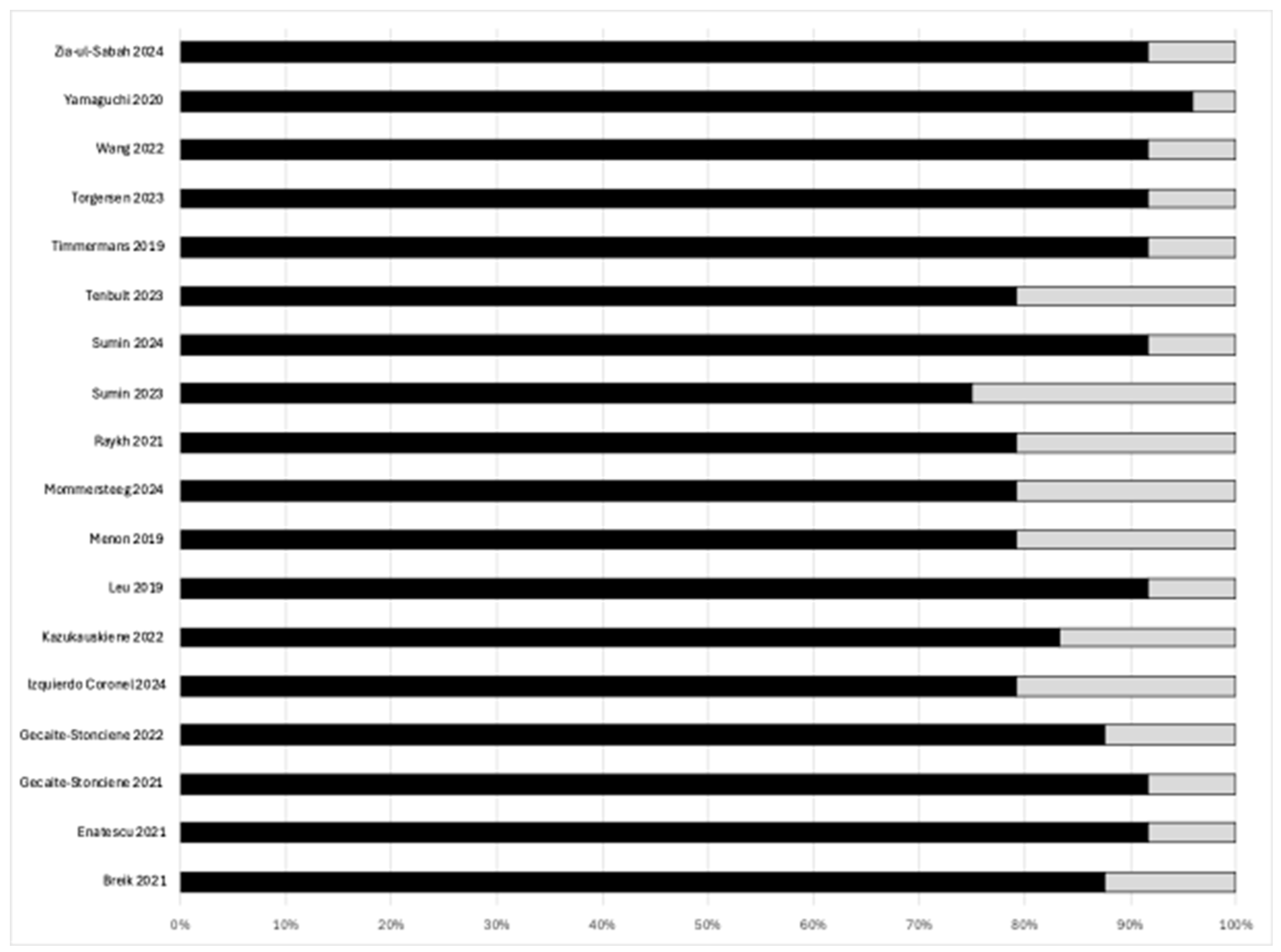
3.2.2. Qualitative Assessment
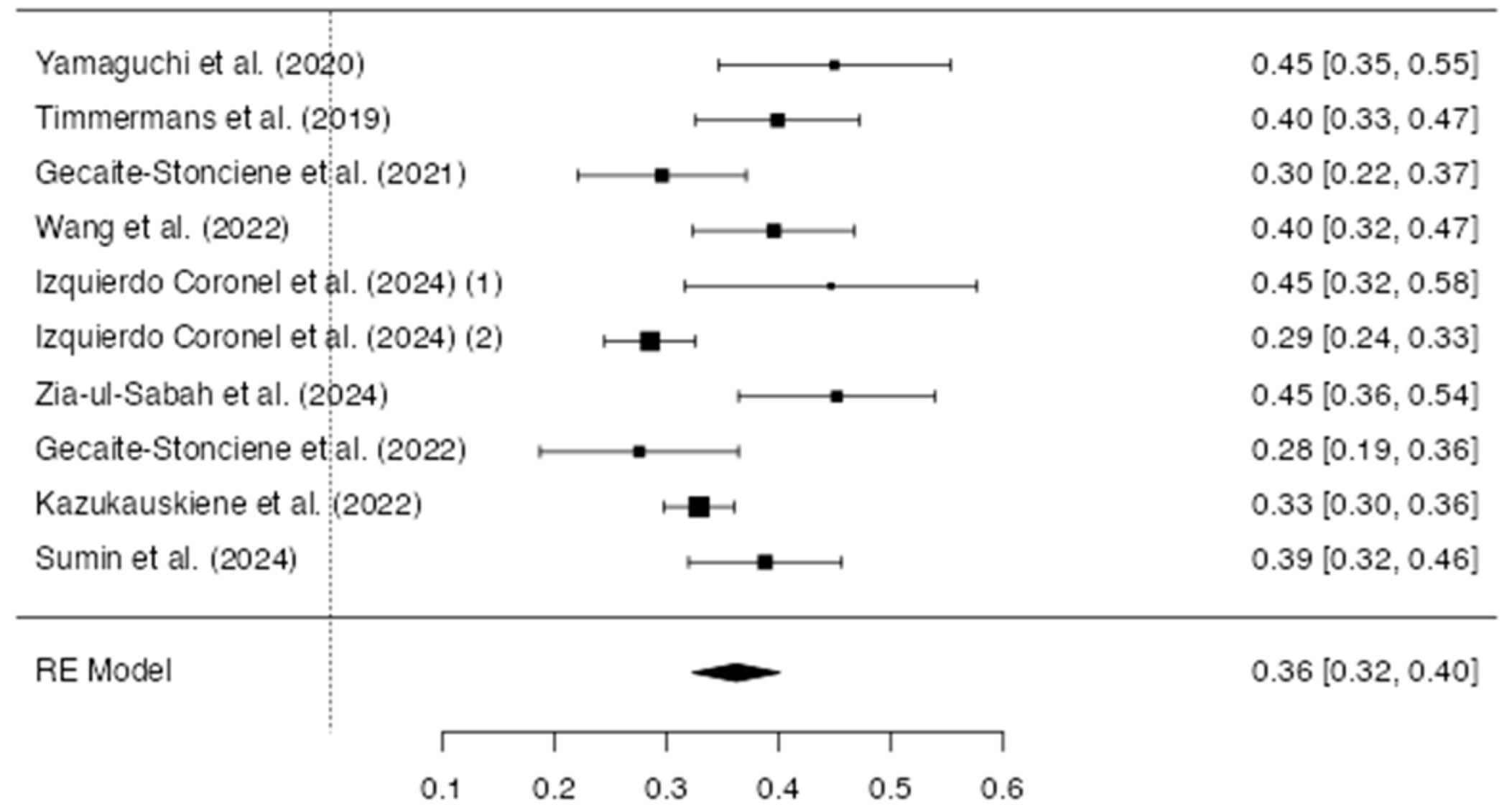
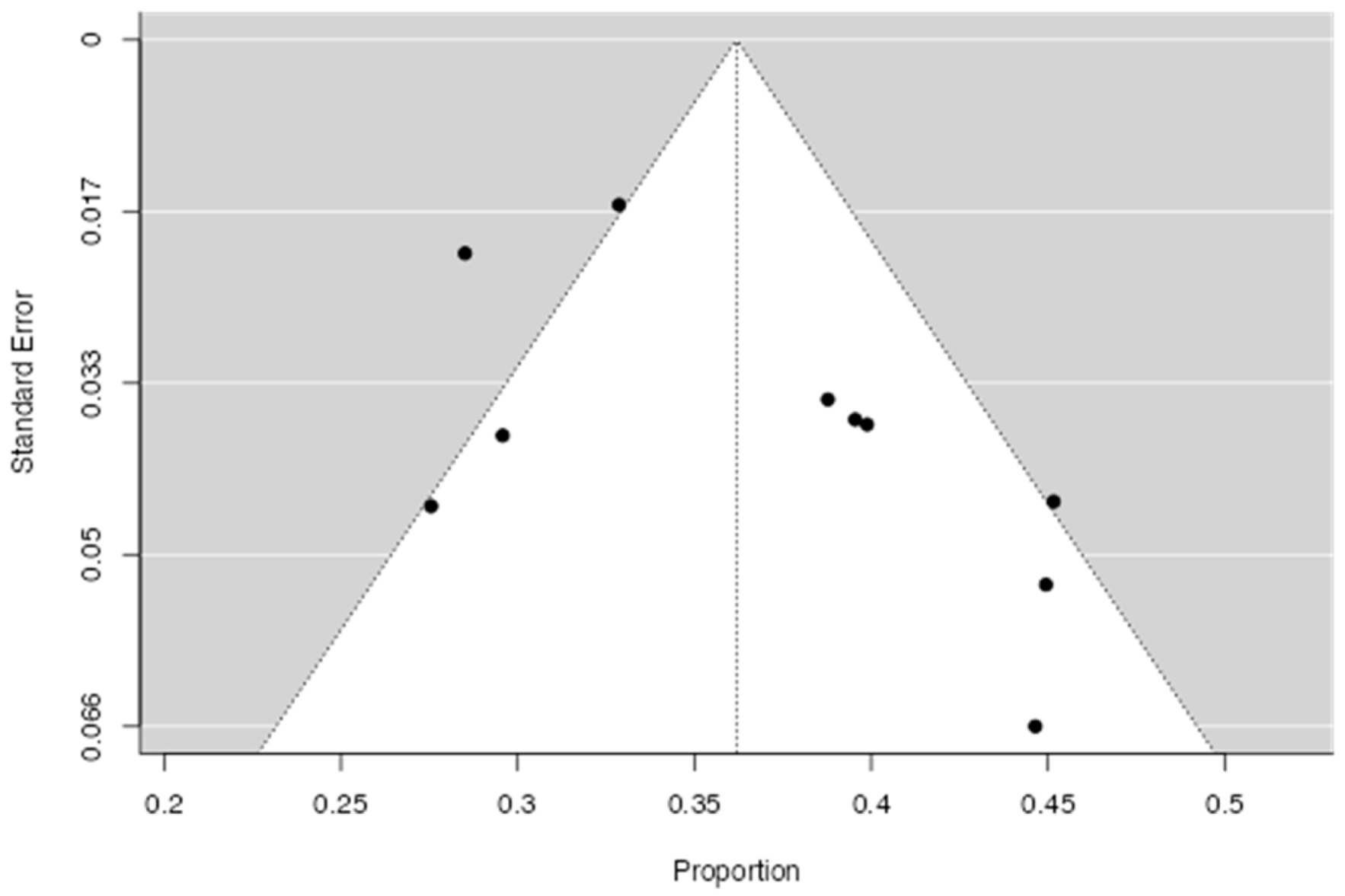
3.2.3. Prevalence of Type D Personality in CVD
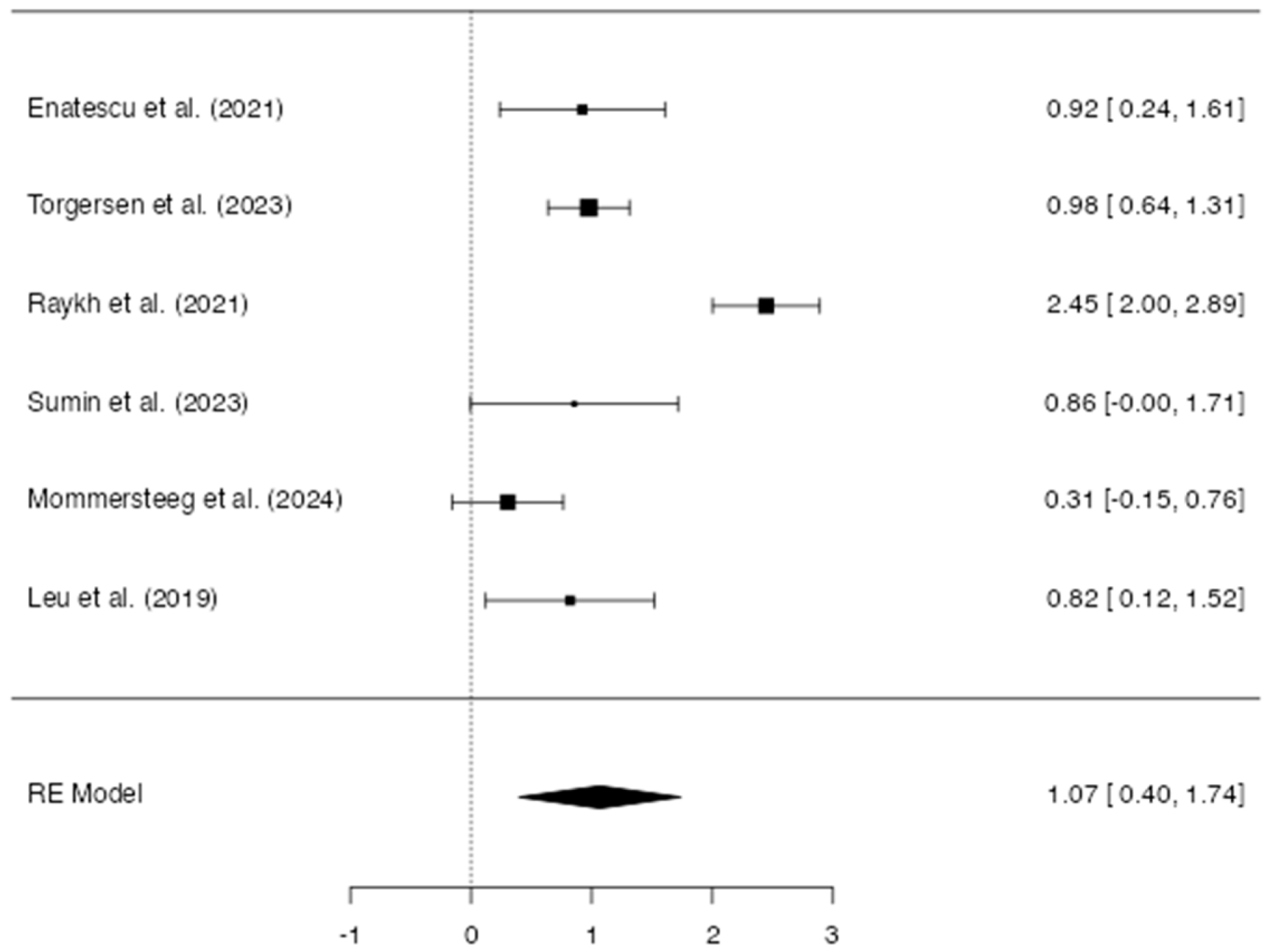
3.2.4. Difference Between Type D and Non-Type D in CVD
4. Discussion
4.1. Clinical Implications and the Role of Psychological Assessment
4.2. Possible Biological Mechanisms
4.3. Types of Markers of Type D
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saglietto, A.; Manfredi, R.; Elia, E.; D’Ascenzo, F.; De Ferrari, G.M.; Biondi-Zoccai, G.; Münzel, T. Cardiovascular disease burden: Italian and global perspectives. Minerva Cardiol. Angiol. 2021, 69, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Adhikary, D.; Barman, S.; Ranjan, R.; Stone, H. A systematic review of Major Cardiovascular Risk Factors: A Growing Global Health Concern. Cureus 2022, 14, e30119. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Levine, G.N.; Cohen, B.E.; Commodore-Mensah, Y.; Fleury, J.; Huffman, J.C.; Khalid, U.; Labarthe, D.R.; Lavretsky, H.; Michos, E.D.; Spatz, E.S.; et al. Psychological health, well-being, and the Mind-Heart-Body Connection: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e763–e783. [Google Scholar] [CrossRef] [PubMed]
- Roest, A.M.; Martens, E.J.; de Jonge, P.; Denollet, J. Anxiety and risk of incident coronary heart disease: A meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J. Personality and coronary heart disease: The type-D scale-16 (DS16). Ann. Behav. Med. 1998, 20, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Rosenman, R.H.; Friedman, M.; Straus, R.; Wurm, M.; Kositchek, R.; Hahn, W.; Werthessen, N.T. A predictive study of coronary heart disease. JAMA 1964, 189, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Mols, F.; Denollet, J. Type D personality in cardiovascular disease: A review. Stress 2010, 13, 173–182. [Google Scholar]
- Al-Qezweny, M.N.; Utens, E.M.; Dulfer, K.; Hazemeijer, B.A.; van Geuns, R.J.; Daemen, J.; van Domburg, R. The association between type D personality, depression and anxiety ten years after PCI. Neth. Heart J. 2016, 24, 538–543. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Martens, E.J.; Kupper, N.; Pedersen, S.S.; Denollet, J.; Widdershoven, J.W. Type D personality, medication adherence, and clinical outcomes in patients with heart failure. Psychosom. Med. 2010, 72, 773–780. [Google Scholar]
- Denollet, J.; Holmes, R.V.; Vrints, C.J.; Conraads, V.M. Unfavorable outcome of heart transplantation in recipients with type D personality. J. Heart Lung Transplant. 2007, 26, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, G.; Zhao, Z.; Li, L.; Yin, S.; Sun, X.; Yu, B.; Gao, X.; Lin, P.; Yang, Y. The relationship between Type D personality with atherosclerotic plaque and cardiovascular events: The mediation effect of inflammation and kynurenine/tryptophan metabolism. Front. Cardiovasc. Med. 2022, 9, 986712. [Google Scholar] [CrossRef] [PubMed]
- Kupper, N.; Denollet, J. Type D Personality as a Risk Factor in Coronary Heart Disease: A Review of Current Evidence. Curr. Cardiol. Rep. 2018, 20, 104. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enfermagem. 2007, 15, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research (AHFMR): Edmonton, AB, Canada, 2004; AHFMR–HTA Initiative, 13. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Springer: Cham, Switzerland, 2015. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Çoğaltay, N.; Karadağ, E. Introduction to Meta-Analysis. In Leadership and Organizational Outcomes: Meta-Analysis of Empirical Studies; Springer: Cham, Switzerland, 2015; pp. 19–40. [Google Scholar] [CrossRef]
- Edwards, P.; Clarke, M.J.; Wordsworth, S.; Yeo, S.T. A systematic review of the effectiveness of fibrin sealant in surgical procedures. Br. J. Surg. 2016, 103, 197–208. [Google Scholar] [CrossRef]
- Papadimitropoulou, K.; Vossos, V.; Kennedy, S. The role of micronutrients in cognitive function: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutr. Rev. 2019, 77, 556–570. [Google Scholar] [CrossRef]
- Thorlund, K.; Devereaux, P.J.; Wetterslev, J.; Guyatt, G. Can Trial Sequential Monitoring Boundaries Reduce Spurious Inferences from Meta-Analyses? J. Clin. Epidemiol. 2012, 65, 775–782. [Google Scholar] [CrossRef]
- Enatescu, V.R.; Cozma, D.; Țint, D.; Enătescu, I.; Șimu, M.; Giurgi-Oncu, C.; Lăzărescu, M.A.; Mornos, C. The Relationship Between Type D Personality and the Complexity of Coronary Artery Disease. Neuropsychiatr. Dis. Treat. 2021, 17, 809–820. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gecaite-Stonciene, J.; Hughes, B.M.; Burkauskas, J.; Bunevicius, A.; Kazukauskiene, N.; van Houtum, L.; Brozaitiene, J.; Neverauskas, J.; Mickuviene, N. Fatigue Is Associated with Diminished Cardiovascular Response to Anticipatory Stress in Patients with Coronary Artery Disease. Front. Physiol. 2021, 12, 692098. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gecaite-Stonciene, J.; Hughes, B.M.; Kazukauskiene, N.; Bunevicius, A.; Burkauskas, J.; Neverauskas, J.; Bellani, M.; Mickuviene, N. Cortisol response to psychosocial stress, mental distress, fatigue and quality of life in coronary artery disease patients. Sci. Rep. 2022, 12, 19373. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Izquierdo Coronel, B.; López Pais, J.; Nieto Ibáñez, D.; Olsen Rodríguez, R.; Galán Gil, D.; Perela Álvarez, C.; Abad Romero, R.; Álvarez Bello, M.; Martín Muñoz, M.; Espinosa Pascual, M.J.; et al. Prevalence and prognosis of anxiety, insomnia, and type D personality in patients with myocardial infarction: A Spanish cohort. Cardiol. J. 2024, 31, 261–270. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kazukauskiene, N.; Fineberg, N.A.; Bunevicius, A.; Narvaez Linares, N.F.; Poitras, M.; Plamondon, H.; Pranckeviciene, A.; Gecaite-Stonciene, J.; Brozaitiene, J.; Varoneckas, G.; et al. Predictive value of baseline cognitive functioning on health-related quality of life in individuals with coronary artery disease: A 5-year longitudinal study. Eur. J. Cardiovasc. Nurs. 2022, 21, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Leu, H.B.; Yin, W.H.; Tseng, W.K.; Wu, Y.W.; Lin, T.H.; Yeh, H.I.; Cheng Chang, K.; Wang, J.H.; Wu, C.C.; Chen, J.W. Impact of type D personality on clinical outcomes in Asian patients with stable coronary artery disease. J. Formos. Med. Assoc. 2019, 118, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Mommersteeg, P.M.C.; Lodder, P.; Aarnoudse, W.; Magro, M.; Widdershoven, J.W. Psychosocial distress and health status as risk factors for ten-year major adverse cardiac events and mortality in patients with non-obstructive coronary artery disease. Int. J. Cardiol. 2024, 406, 132062. [Google Scholar] [CrossRef] [PubMed]
- Raykh, O.I.; Sumin, A.N.; Korok, E.V. The Influence of Personality Type D on Cardiovascular Prognosis in Patients After Coronary Artery Bypass Grafting: Data from a 5-Year-Follow-up Study. Int. J. Behav. Med. 2022, 29, 46–56. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sumin, A.N.; Shcheglova, A.V. Pathogenetic Mechanisms Underlying Major Adverse Cardiac Events in Personality Type D Patients after Percutaneous Coronary Intervention: The Roles of Cognitive Appraisal and Coping Strategies. Diagnostics 2023, 13, 3374. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sumin, A.N.; Shcheglova, A.V.; Barbarash, O.L. New indicator of arterial stiffness START—Is there a prognostic value of its dynamics in patients with coronary artery disease? Biomedicines 2024, 12, 1638. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Timmermans, I.; Versteeg, H.; Duijndam, S.; Graafmans, C.; Polak, P.; Denollet, J. Social inhibition and emotional distress in patients with coronary artery disease: Type D personality construct. J. Health Psychol. 2019, 24, 1929–1944. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Torgersen, K.S.; Sverre, E.C.B.; Weedon-Fekjær, H.; Andreassen, O.A.; Munkhaugen, J.; Dammen, T. Risk of recurrent cardiovascular events in coronary artery disease patients with Type D personality. Front. Psychol. 2023, 14, 1119146. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, D.; Izawa, A.; Matsunaga, Y. The Association of Depression with Type D Personality and Coping Strategies in Patients with Coronary Artery Disease. Intern. Med. 2020, 59, 1589–1595. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zia-Ul-Sabah, S.A.M.; Alqahtani, S.A.M.; Alghamdi, B.H.; Wani, J.I.; Aziz, S.; Durrani, H.K.; Patel, A.A.; Rangraze, I.; Wani, S.J. Association of type-D personality and left-ventricular remodelling in patients treated with primary percutaneous intervention after ST-segment elevation myocardial infarction. BMC Cardiovasc. Disord. 2024, 24, 600. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Breik, W.; Elbedour, S. The Predictive Ability of Type D Personality Pattern, Anxiety, and Depression in Cardiac Disease. Eur. J. Ment. Health 2021, 16, 196–209. [Google Scholar] [CrossRef]
- Menon, V.; Pillai, A.G.; Satheesh, S.; Kaliamoorthy, C.; Sarkar, S. Factor structure and validity of Type D personality scale among Indian (Tamil-speaking) patients with acute myocardial infarction. Indian J. Psychiatry 2019, 61, 572–577. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tenbult, N.; van Asten, I.; Traa, S.; Brouwers, R.W.M.; Spee, R.F.; Lu, Y.; Brini, A.; Kop, W.; Kemps, H. Determinants of information needs in patients with coronary artery disease receiving cardiac rehabilitation: A prospective observational study. BMJ Open 2023, 13, e068351. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Higgins, J.P.; Thompson, S.G.; Spiegelhalter, D.J. A re-evaluation of random-effects meta-analysis. J. R. Stat. Soc. Ser. A Stat. Soc. 2009, 172, 137–159. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Riley, R.D.; Higgins, J.P.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.S.; Denollet, J. Type D personality, cardiac events, and impaired quality of life: A review. Eur. J. Cardiovasc. Prev. Rehabil. 2003, 10, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Global Cardiovascular Risk Consortium; Magnussen, C.; Ojeda, F.M.; Leong, D.P.; Alegre-Díaz, J.; Amouyel, P.; Aviles-Santa, L.; De Bacquer, D.; Ballantyne, C.M.; Bernabé-Ortiz, A.; et al. Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. N. Engl. J. Med. 2023, 389, 1273–1285. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Friedman, M.; Rosenman, R.H. Association of specific overt behavior pattern with blood and cardiovascular findings; blood cholesterol level, blood clotting time, incidence of arcus senilis, and clinical coronary artery disease. J. Am. Med. Assoc. 1959, 169, 1286–1296. [Google Scholar] [CrossRef] [PubMed]
- Chida, Y.; Steptoe, A. The association of anger and hostility with future coronary heart disease: A meta-analytic review of prospective evidence. J. Am. Coll. Cardiol. 2009, 53, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J. DS14: Standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Checklist |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| S. No | First Author’s Name/Year of Publication [Reference Number] | Country | Sample Size | Male Percentage | Age (Mean; Age Range) | Study Design | MA Data | Clinical Condition | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Enatescu/2021 [23] | Romania | 221 | 59.3 | 60 ± 10.2 | Cross-sectional | Odds Ratio | CAD (coronary artery disease) | Type D is associated with higher CVD severity (IMA). |
| 2 | Gecaite-Stonciene/2021 [24] | Lithuania | 142 | 85 | 52 ± 8 | Cross-sectional | Prevalence | ACS (Acute Coronary Syndrome) | Type D is associated with higher distress and lower cardiovascular response. |
| 3 | Gecaite-Stonciene/2022 [25] | Lithuania | 98 | 87.8 | 52.92 ± 7.17 | Cross-sectional | Prevalence | CAD | Type D was associated with CAD (cortisol response). |
| 4 | Izquierdo Coronel/2024 (1) [26] | Spain | 56 | 45 | 66.8 ± 13.7 | Longitudinal study (FU: 3 years) | Prevalence | MINOCA (myocardial infarction with non-obstructive coronary arteries) | Type D is associated with a cardiovascular condition. |
| 5 | Izquierdo Coronel/2024 (2) [26] | Spain | 477 | 76 | 66.5 ± 13.7 | Longitudinal study (FU: 3 years) | Prevalence | MICAD (myocardial infarction with coronary artery disease) | Type D is associated with a cardiovascular condition. |
| 6 | Kazukauskien/2022 [27] | Lithuania | 864 | 74 | 58 ± 9 | Longitudinal study (FU: 5 years) | Prevalence | CAD | Type D personality is associated with a lower quality of life. |
| 7 | Leu/2019 [28] | Taiwan | 777 | 84.3 | 62.03 ± 10.5 | Longitudinal study (FU: 1 year) | Odds Ratio | CAD | Type D personality predicts CAD. |
| 8 | Mommersteeg/2024 [29] | The Netherlands | 517 | 55 | 63 | Longitudinal study (FU: 10 years) | Odds Ratio | MACE (major adverse cardiovascular event) | Type D does not predict negative outcomes in MACE. |
| 9 | Raykh/2021 [30] | Russia | 602 | 81.4 | 57.7 ± 7.3 | Longitudinal study (FU: 10 years) | Odds Ratio | Post-coronary artery bypass grafting | Negative outcomes of CAD at 5 years post intervention are highly associated with Type D. |
| 10 | Sumin/2023 [31] | Russia | 91 | - | 64.7 | Longitudinal study (FU: 1 year) | Odds Ratio | MACE | Type D personality predicts MACE events and hospitalization. |
| 11 | Sumin/2024 [32] | Russia | 196 | 73 | 62 ± 1 | Longitudinal study (FU: 10 years) | Prevalence | CAD | Type D is predictive of the prognosis of CAD. |
| 12 | Timmermans/2019 [33] | The Netherlands | 173 | 77 | 69.1 ± 9.6 | Cross-sectional | Prevalence | CAD | Type D personality is associated with a low quality of life (physical health status) and social anxiety. |
| 13 | Torgersen/2023 [34] | Norway | 1083 | 79 | 61.5 ± 9.6 | Cohort study; FU: 4.2 years | Odds Ratio | CAD | Type D personality is associated with recurrent CAD. |
| 14 | Wang/2022 [11] | China | 177 | 58.8 | 55.79 ± 10.70 | Cross-sectional | Prevalence | CAD | Type D is associated with poor cardiovascular outcomes in CAD, mediated by a pro-inflammatory biomarker. |
| 15 | Yamaguchi/2020 [35] | Japan | 89 | 88.8 | 66 (58–74) | Cross-sectional | Prevalence | CAD | Type D personality in CAD is associated with depression and negative coping. |
| 16 | Zia-ul-Sabah/2024 [36] | Saudi Arabia | 124 | 55 | 67 ± 10 | Longitudinal (FU: 1 year) | Prevalence | Post-STEMI | Type D is predictive of the severity of left ventricular adverse remodeling. |
| S. No | First Author’s Name/Year of Publication [Reference Number] | Item_1 | Item_2 | Item_3 | Item_4 | Item_5 | Item_6 | Item_7 | Item_8 | Item_9 | Item_10 | Item_11 | Item_12 | Item_13 | Item_14 | Total Score | Index of Quality | Risk of Bias | Index of Quality | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Enatescu/2021 [23] | 2 | 2 | 2 | 2 | 0 | 1 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 2 | Gecaite-Stonciene/2021 [24] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 3 | Gecaite-Stonciene/2022 [25] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 21 | 0.88 | G | 88 | 13 |
| 4 | Izquierdo Coronel/2024 [26] | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 19 | 0.79 | A | 79 | 21 |
| 5 | Kazukauskien/2022 [27] | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 | 0.83 | G | 83 | 17 |
| 6 | Leu/2019 [28] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 7 | Mommersteeg/2024 [29] | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 19 | 0.79 | A | 79 | 21 |
| 8 | Raykh/2021 [30] | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 19 | 0.79 | A | 79 | 21 |
| 9 | Sumin/2023 [31] | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 18 | 0.75 | A | 75 | 25 |
| 10 | Sumin/2024 [32] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 11 | Timmermans/2019 [33] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 12 | Torgersen/2023 [34] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 13 | Wang/2022 [11] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 14 | Yamaguchi/2020 [35] | 2 | 2 | 2 | 2 | 1 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 23 | 0.96 | H | 96 | 4 |
| 15 | Zia-ul-Sabah/2024 [36] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 | 0.92 | G | 92 | 8 |
| 16 | Breik/2021 [37] | 2 | 2 | 2 | 1 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 21 | 0.88 | G | 88 | 13 |
| 17 | Menon/2019 [38] | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 19 | 0.79 | A | 79 | 21 |
| 18 | Tenbult/2023 [39] | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 19 | 0.79 | A | 79 | 21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Nakhebi, O.A.S.; Albu-Kalinovic, R.; Bosun, A.; Neda-Stepan, O.; Gliga, M.; Crișan, C.-A.; Marinescu, I.; Mornoș, C.; Enatescu, V.-R. Cardiovascular Diseases and Type D Personality: Systematic Review and Meta-Analysis of the Literature of the Last 10 Years. Life 2025, 15, 1061. https://doi.org/10.3390/life15071061
Al Nakhebi OAS, Albu-Kalinovic R, Bosun A, Neda-Stepan O, Gliga M, Crișan C-A, Marinescu I, Mornoș C, Enatescu V-R. Cardiovascular Diseases and Type D Personality: Systematic Review and Meta-Analysis of the Literature of the Last 10 Years. Life. 2025; 15(7):1061. https://doi.org/10.3390/life15071061
Chicago/Turabian StyleAl Nakhebi, Omar Anwar Saleh, Raluka Albu-Kalinovic, Adela Bosun, Oana Neda-Stepan, Marius Gliga, Cătălina-Angela Crișan, Ileana Marinescu, Cristian Mornoș, and Virgil-Radu Enatescu. 2025. "Cardiovascular Diseases and Type D Personality: Systematic Review and Meta-Analysis of the Literature of the Last 10 Years" Life 15, no. 7: 1061. https://doi.org/10.3390/life15071061
APA StyleAl Nakhebi, O. A. S., Albu-Kalinovic, R., Bosun, A., Neda-Stepan, O., Gliga, M., Crișan, C.-A., Marinescu, I., Mornoș, C., & Enatescu, V.-R. (2025). Cardiovascular Diseases and Type D Personality: Systematic Review and Meta-Analysis of the Literature of the Last 10 Years. Life, 15(7), 1061. https://doi.org/10.3390/life15071061