
Influence and Predictors of Anxiety on Health Status ≥ 5 Years Beyond Breast Cancer Diagnosis in Spain: A Cross-Sectional Study

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Measures
2.2.1. Primary Outcome
2.2.2. Secondary Outcomes
Demographic and Clinical Data Collection
Mood State
Cancer-Related Fatigue
Pain
Self-Perceived Physical Fitness
Physical Activity Level
Health-Related Quality of Life
2.3. Statistical Analysis
- Normally distributed variables (age, time since diagnosis, and time since first surgery) were analyzed using ANOVA to compare the two anxiety-level groups: low (≤3.4) vs. high (≥3.5). Results are reported as mean ± standard deviation. Post hoc comparisons were adjusted using Bonferroni correction to account for multiple testing.
- Non-normally distributed variables (mood state, non-categorized CRF, pain, self-perceived physical fitness, and HRQoL) were analyzed using the Mann–Whitney U test. Results are also reported as mean ± standard deviation. Bonferroni correction was applied where appropriate to minimize the risk of Type I error due to multiple comparisons.
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Mood State
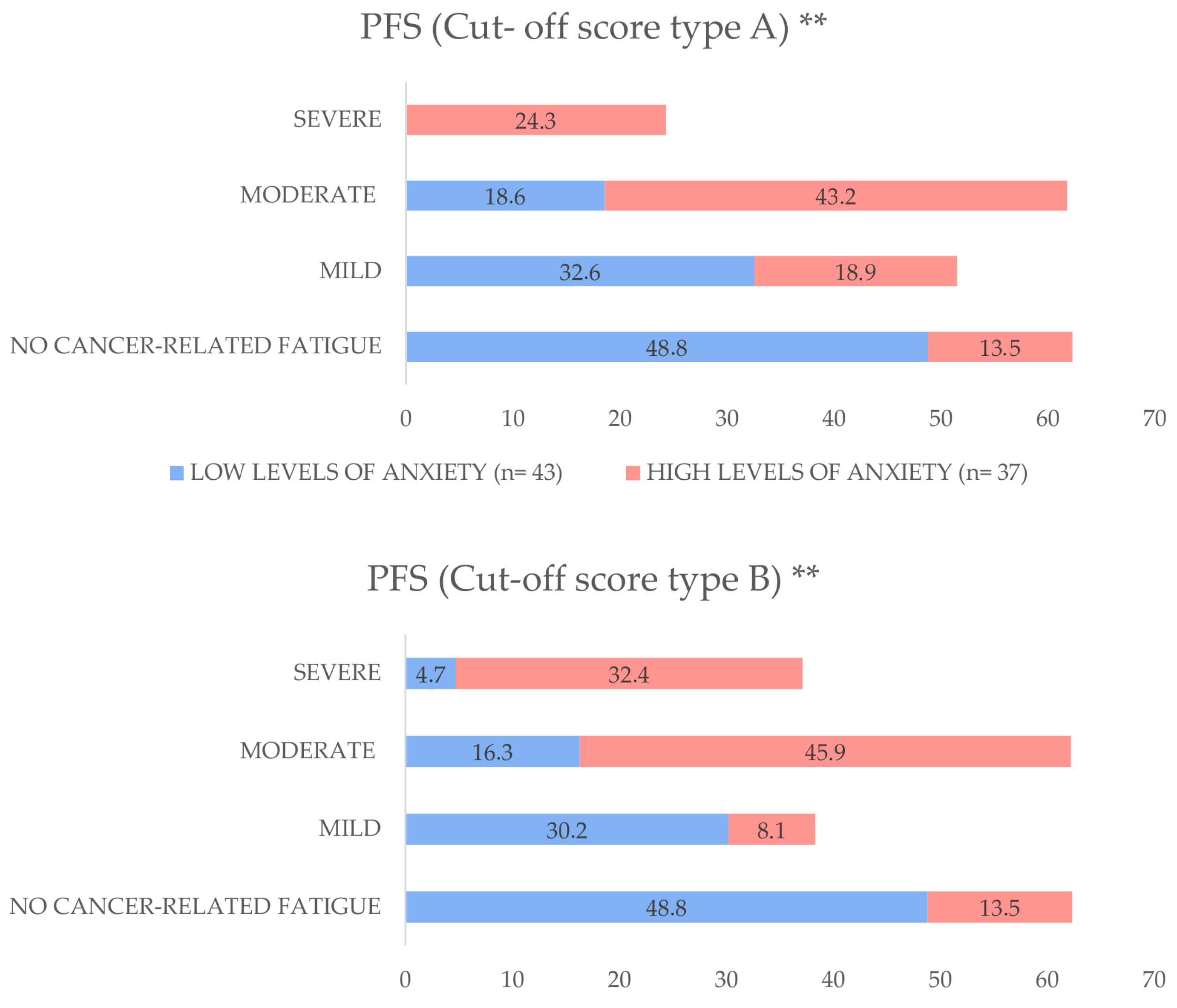
3.3. Cancer-Related Fatigue
3.4. Pain
3.5. Self-Perceived Physical Fitness
3.6. Physical Activity Level
3.7. Health-Related Quality of Life
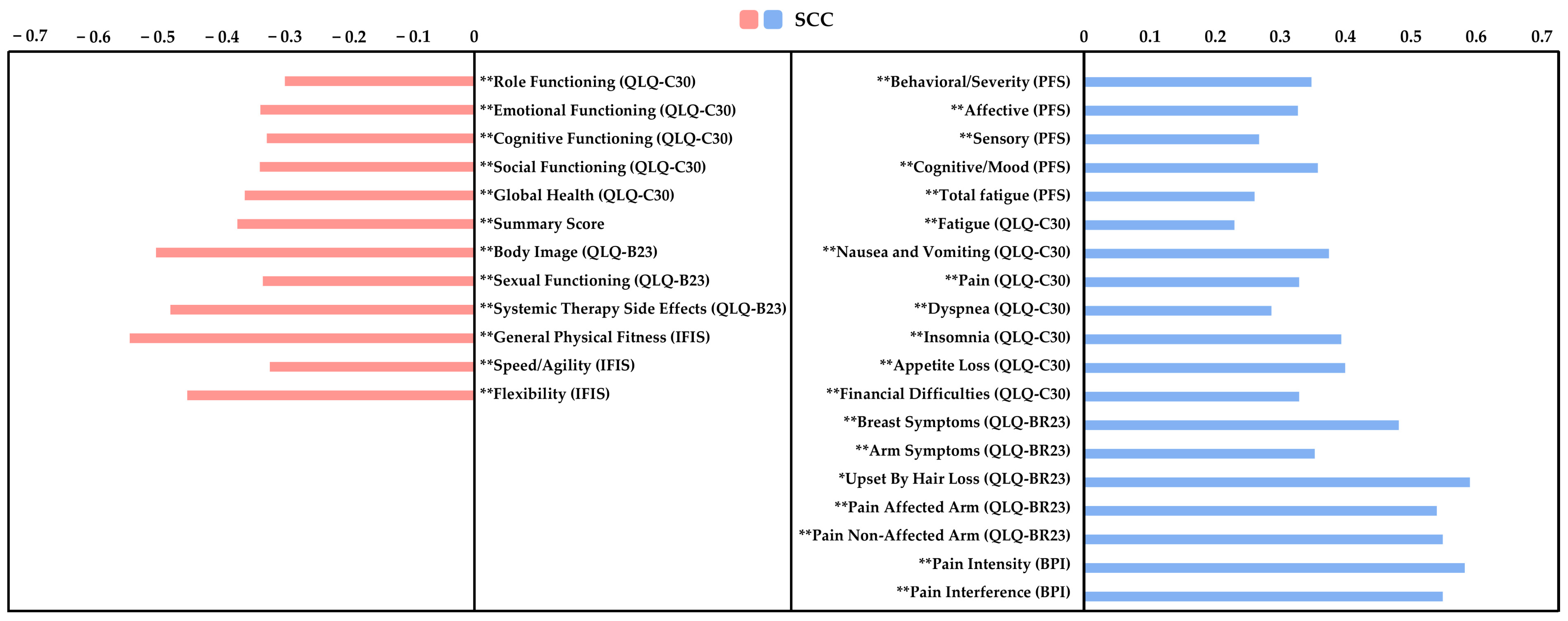
3.8. Correlation Analysis and Multiple Regression Analysis
4. Discussion
4.1. Mood State
4.2. Cancer-Related Fatigue
4.3. Pain
4.4. Self-Perceived Physical Fitness and Physical Activity Levels
4.5. Health-Related Quality of Life
4.6. Correlation Analysis and Multiple Regression Analysis
4.7. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Barrios, C.H. Global challenges in breast cancer detection and treatment. Breast 2022, 62, S3–S6. [Google Scholar] [CrossRef] [PubMed]
- Lovelace, D.L.; McDaniel, L.R.; Golden, D. Long-term effects of breast cancer surgery, treatment, and survivor care. J. Midwifery Women’s Health 2019, 64, 713–724. [Google Scholar] [CrossRef]
- Ren, Y.; Maselko, J.; Tan, X.; Olshan, A.F.; Stover, A.M.; Bennett, A.V.; Andersen, K.K.; Reeve, B.B.; Ekwueme, D.U.; Pisu, M.; et al. Emotional and functional well-being in long-term breast cancer survivorship. Cancer Causes Control. 2024, 35, 1191–1200. [Google Scholar] [CrossRef]
- Cheng, C.-T.; Ho, S.M.Y.; Lai, Y.; Zhang, Q.; Wang, G.L.; Liu, Y.; Li, J.; Chen, M.; Wu, X.; Zhao, L.; et al. Coping profiles predict long-term anxiety trajectory in breast cancer survivors. Support Care Cancer. 2021, 29, 4045–4053. [Google Scholar] [CrossRef]
- Breidenbach, C.; Heidkamp, P.; Hiltrop, K.; Müller, S.; Schneider, A.; Weber, T.; Fischer, M.; Hoffmann, R.; Klein, L.; Wolf, J.; et al. Prevalence and determinants of anxiety and depression in long-term breast cancer survivors. BMC Psychiatry 2022, 22, 101–111. [Google Scholar] [CrossRef]
- Götze, H.; Friedrich, M.; Taubenheim, S.; Müller, C.; Becker, A.; Hoffmann, B.; Lange, F.; Richter, S.; Schmitt, T.; Vogel, M.; et al. Depression and anxiety in long-term survivors 5 and 10 years after cancer diagnosis. Support Care Cancer 2020, 28, 211–220. [Google Scholar] [CrossRef]
- Maass, S.W.M.C.; Boerman, L.M.; Verhaak, P.F.M.; van der Linden, M.; de Vries, J.; Smits, A.; Janssen, M.; Peters, R.; Bakker, T.; Willems, R.; et al. Long-term psychological distress in breast cancer survivors and their matched controls: A cross-sectional study. Maturitas 2019, 130, 6–12. [Google Scholar] [CrossRef]
- De La Torre-Luque, A.; Victoria Cerezo, M.; López, E.; Sibole, J.V. Emotional distress among long-term breast cancer survivors: The role of insomnia and worry. Behav. Psychol. 2020, 28, 533–549. [Google Scholar]
- Ribeiro, F.E.; Palma, M.R.; Silva, D.T.C.; Costa, L.P.; Almeida, V.C.; Santos, R.M.; Oliveira, M.F.; Lima, A.S.; Ferreira, T.J.; Gomes, L.C.; et al. Relationship of anxiety and depression symptoms with the different domains of physical activity in breast cancer survivors. J. Affect. Disord. 2020, 273, 210–214. [Google Scholar] [CrossRef]
- Eysenck, M.W.; Fajkowska, M. Anxiety and depression: Toward overlapping and distinctive features. Cogn. Emot. 2018, 32, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.; Buckman, J.E.J.; Cape, J.; Agnew-Davies, R.; Barkham, M.; Reynolds, S.; Szmukler, G.; Kellett, S.; Kuyken, W.; Byford, S.; et al. Trajectories of depression and anxiety symptom change during psychological therapy. J. Affect. Disord. 2019, 249, 327–335. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Nolen, W.A.; Lamers, F.; Zitman, F.G.; Beekman, A.T.F.; Smit, J.H.; Cuijpers, P.; de Graaf, R.; van Dyck, R.; Spinhoven, P.; et al. Two-year course of depressive and anxiety disorders: Results from the Netherlands Study of Depression and Anxiety (NESDA). J. Affect. Disord. 2011, 133, 76–85. [Google Scholar] [CrossRef]
- Li, J.; Cai, Z.; Li, X.; Wang, Y.; Zhang, L.; Chen, H.; Liu, Q.; Zhao, T.; Sun, W.; Huang, F.; et al. Mindfulness-based therapy versus cognitive behavioral therapy for people with anxiety symptoms: A systematic review and meta-analysis of random controlled trials. Ann. Palliat. Med. 2021, 10, 7596–7612. [Google Scholar] [CrossRef] [PubMed]
- McGregor, B.A.; Antoni, M.H. Psychological intervention and health outcomes among women treated for breast cancer: A review of stress pathways and biological mediators. Brain Behav. Immun. 2009, 23, 159–166. [Google Scholar] [CrossRef]
- Williams, A.M.; Khan, C.P.; Heckler, C.E.; Mustian, K.M.; Peppone, L.J.; Janelsins, M.C.; Morrow, G.R.; Palesh, O.G.; Sprod, L.K.; Mohile, S.G.; et al. Fatigue, anxiety, and quality of life in breast cancer patients compared to non-cancer controls: A nationwide longitudinal analysis. Breast Cancer Res. Treat. 2021, 187, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Cornelius, V.; Ream, E.; Watson, E.; Smith, J.; Jones, K.; Patel, R.; Green, A.; Clarke, S.; Wright, D.; et al. Anxiety after completion of treatment for early-stage breast cancer: A systematic review to identify candidate predictors and evaluate multivariable model development. Support. Care Cancer 2017, 25, 2321–2333. [Google Scholar] [CrossRef]
- Greer, J.A.; Solis, J.M.; Temel, J.S.; Lennes, I.T.; Pirl, W.F.; Park, E.R.; Lynch, T.J.; Gallagher, E.R.; Maguire, R.; Liao, Z.; et al. Anxiety disorders in long-term survivors of adult cancers. Psychosomatics 2011, 52, 417–423. [Google Scholar] [CrossRef]
- Shrestha, B.; Dunn, L. The Declaration of Helsinki on medical research involving human subjects: A review of seventh revision. J. Nepal Health Res. Counc. 2020, 17, 548–552. [Google Scholar] [CrossRef]
- Sarac, F.S.; Erkal Ilhan, S.; Kutun, S.; Kutluturkan, S. The effect of informative mobile app use on anxiety, distress, and quality of life of women with breast cancer. Eur. J. Breast Health 2024, 20, 207–214. [Google Scholar] [CrossRef]
- Mittal, N.; Tyagi, N.; Parvaiz, N.; Dhalla, N.; Asthana, G. Comparative assessment of stress and anxiety among medical and nonmedical undergraduate students: A cross-sectional study. Indian J. Med. Spec. 2025, 16, 60–64. [Google Scholar] [CrossRef]
- Cantarero-Villanueva, I.; Sanchez-Jimenez, A.; Galiano-Castillo, N.; Diaz-Rodriguez, L.; Martin-Martin, L.; Arroyo-Morales, M. Effectiveness of lumbopelvic exercise in colon cancer survivors: A randomized controlled clinical trial. Med. Sci. Sports Exerc. 2016, 48, 1438–1446. [Google Scholar] [CrossRef] [PubMed]
- Luyk, N.H.; Beck, F.M.; Weaver, J.M. A visual analogue scale in the assessment of dental anxiety. Anesth. Prog. 1988, 35, 121–123. [Google Scholar]
- Aviado-Langer, J. Measuring preoperative anxiety in patients with breast cancer using the visual analog scale. Clin. J. Oncol. Nurs. 2014, 18, 489–491. [Google Scholar] [CrossRef]
- Labaste, F.; Ferré, F.; Combelles, H.; Dupont, C.; Martin, P.; Leroy, A.; Moreau, J.; Bernard, S.; Petit, L.; Dubois, M.; et al. Validation of a visual analogue scale for the evaluation of the postoperative anxiety: A prospective observational study. Nurs. Open 2019, 6, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Widyastuty, A.; Effendy, E.; Amin, M.M. Correlation between visual analogue scale score and Hospital Anxiety Depression Scale-depression score in patients with cervical cancer in the Hospital Vina Cancer, Medan. Open Access Maced. J. Med. Sci. 2019, 7, 2634–2637. [Google Scholar] [CrossRef]
- Sanz, J.; Gutiérrez, S.; García-Vera, M.P. Psychometric properties of the Scale for Mood Assessment (EVEA): A review. Ansiedad Estrés 2014, 20, 27–49. [Google Scholar]
- Piper, B.F.; Dibble, S.L.; Dodd, M.J.; Weiss, M.; Slaughter, R.; Paul, S.M.; Henrichs, M.; McCallum, C.; Fischer, P.; Johnson, M.; et al. The revised Piper Fatigue Scale: Psychometric evaluation in women with breast cancer. Oncol. Nurs. Forum 1998, 25, 677–684. [Google Scholar]
- Stover, A.M.; Reeve, B.B.; Piper, B.F.; Oberst, M.T.; Jacobsen, P.B.; Cella, D.; Wenzel, L.; Snyder, C.; Schipper, H.; Kornblith, A.B.; et al. Deriving clinically meaningful cut-scores for fatigue in a cohort of breast cancer survivors: A Health, Eating, Activity, and Lifestyle (HEAL) Study. Qual. Life Res. 2013, 22, 2279–2292. [Google Scholar] [CrossRef]
- Cantarero-Villanueva, I.; Fernández-Lao, C.; Díaz-Rodríguez, L.; Galiano-Castillo, N.; Arroyo-Morales, M.; Martín-Martín, L.; Pecos-Martín, D. The Piper Fatigue Scale-Revised: Translation and psychometric evaluation in Spanish-speaking breast cancer survivors. Qual. Life Res. 2014, 23, 271–276. [Google Scholar] [CrossRef]
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Escalante, C.P.; et al. Cancer-Related Fatigue, version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 1012–1039. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Bhargava, R.; Fatigoni, S.; Mazzotta, M.; Schiavon, G.; Zamagni, C.; Montanari, M.; Pinto, C.; Di Maio, M.; Grassi, L.; et al. Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann. Oncol. 2020, 31, 713–723. [Google Scholar] [CrossRef]
- Boonstra, A.M.; Schiphorst Preuper, H.R.; Reneman, M.F.; Post, M.W.; Stewart, R.E. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int. J. Rehabil. Res. 2008, 31, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Badia, X.; Muriel, C.; Gracia, A.; Herdman, M.; Casado, A. Validación española del cuestionario Brief Pain Inventory en pacientes con dolor de causa neoplásica. Med. Clin. 2003, 120, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Segura-Jiménez, V.; Estévez-López, F.; García-Gómez, A. International Fitness scale (IFIS): Construct validity and reliability in women with fibromyalgia: The al-Ándalus project. Arch. Phys. Med. Rehabil. 2016, 97, 395–404. [Google Scholar] [CrossRef]
- Ruiz Comellas, A.; Pera, G.; Baena Díez, J.M.; González López-Valcárcel, B.; Rodríguez Artalejo, F. Validation of a Spanish short version of the Minnesota leisure time Physical Activity Questionnaire (VREM). Rev. Española Salud Pública 2012, 86, 495–508. [Google Scholar] [CrossRef]
- Herrmann, S.D.; Willis, E.A.; Ainsworth, B.E.; Hartman, T.J.; Lofgren, I.E. 2024 Adult Compendium of Physical Activities: A third update of the energy costs of human activities. J. Sport Health Sci. 2024, 13, 6–12. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; Dempsey, P.C.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Mendes, M.d.A.; da Silva, I.; Ramires, V.; de Souza, B.L.; da Silva, L.L. Metabolic equivalent of task (METs) thresholds as an indicator of physical activity intensity. PLoS ONE 2018, 13, e0200701. [Google Scholar] [CrossRef]
- Matthews, C.E.; Moore, S.C.; Arem, H.; Freedman, N.D.; Berrington de González, A.; Hollenbeck, A.R.; Leitzmann, M.F. Amount and intensity of leisure-time physical activity and lower cancer risk. J. Clin. Oncol. 2020, 38, 686–697. [Google Scholar] [CrossRef]
- Cerezo, O.; Oñate-Ocaña, L.F.; Arrieta-Joffe, P.; García-Pérez, A.; Cruz-Ramos, J.A.; López-Macías, D. Validation of the Mexican-Spanish version of the EORTC QLQ-C30 and BR23 questionnaires to assess health-related quality of life in Mexican women with breast cancer: Quality of life in patients with breast cancer. Eur. J. Cancer Care 2012, 21, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Husson, O.; de Rooij, B.H.; Kieffer, J.; van Leeuwen, M.C.; Mols, F.; van de Poll-Franse, L.V. The EORTC QLQ-C30 summary score as prognostic factor for survival of patients with cancer in the “real-world”: Results from the population-based PROFILES registry. Oncologist 2019, 25, e722–e732. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Rahbar, M.H. Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiology 2016, 6, 227–247. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 721–732. [Google Scholar] [CrossRef]
- Tran, T.X.M.; Jung, S.-Y.; Lee, E.-G.; Kim, H.-J.; Kim, H. Fear of cancer recurrence and its negative impact on health-related quality of life in long-term breast cancer survivors. Cancer Res. Treat. 2022, 54, 1065–1073. [Google Scholar] [CrossRef]
- Keesing, S.; Rosenwax, L.; McNamara, B. The implications of women’s activity limitations and role disruptions during breast cancer survivorship. Women’s Health 2018, 14, 1745505718756381. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Maurer, T.; Behrens, S.; Kneis, S.; Wiskemann, J. Cancer-related fatigue: Towards a more targeted approach based on classification by biomarkers and psychological factors. Int. J. Cancer 2024, 154, 1011–1018. [Google Scholar] [CrossRef]
- Lobefaro, R.; Rota, S.; Porcu, L.; Gatto, M.; Ricciardi, C. Cancer-related fatigue and depression: A monocentric, prospective, cross-sectional study in advanced solid tumors. ESMO Open 2022, 7, 100457. [Google Scholar] [CrossRef]
- Yin, M.; Wang, C.; Gu, K.; Xu, X.; Zheng, Y. Chronic pain and its correlates among long-term breast cancer survivors. J. Cancer Surviv. 2023, 17, 460–467. [Google Scholar] [CrossRef]
- Pérez, C.; Ochoa, D.; Sánchez, N.; García, L.; Martínez, R. Pain in long-term cancer survivors: Prevalence and impact in a cohort composed mostly of breast cancer survivors. Cancers 2024, 16, 1581. [Google Scholar] [CrossRef]
- Aboushaar, N.; Serrano, N. The mutually reinforcing dynamics between pain and stress: Mechanisms, impacts and management strategies. Front. Pain Res. 2024, 5, 1445280. [Google Scholar] [CrossRef] [PubMed]
- Lingens, S.P.; Schulz, F.; Müller, I.; Nissen, C.; Hinz, A. Associations between self-efficacy, distress and anxiety in cancer patient-relative dyads visiting psychosocial cancer support services: Using actor-partner interdependence modelling. PLoS ONE 2021, 16, e0255318. [Google Scholar] [CrossRef]
- Rodrigues, B.; Encantado, J.; Franco, S.; Silva, M.; Santos, L. Psychosocial correlates of physical activity in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2024. ahead of print. [Google Scholar] [CrossRef]
- Kochman, M.; Kielar, A.; Kasprzak, M.; Nowak, P.; Zielińska, A. The relationship between self-rated health and physical fitness in Polish youth. Healthcare 2023, 12, 24. [Google Scholar] [CrossRef] [PubMed]
- Aandstad, A. Self-perceived and self-tested endurance: Associations with objective measures. Percept. Mot. Ski. 2022, 129, 1492–1503. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Campbell, A.M.; Stuiver, M.M.; Pinto, B.M.; Schwartz, A.L. Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA Cancer J. Clin. 2019, 69, 468–484. [Google Scholar] [CrossRef]
- Voskanyan, V.; Marzorati, C.; Sala, D.; Grasso, R.; Pietrobon, R.; van der Heide, I. Correction to: Psychosocial factors associated with quality of life in cancer survivors: Umbrella review. J. Cancer Res. Clin. Oncol. 2024, 150, 408. [Google Scholar] [CrossRef]
- Franzoi, M.A.; Aupomerol, M.; Havas, J.; Pérez, N.; González, M. Investigating sexual health after breast cancer by longitudinal assessment of patient-reported outcomes. ESMO Open 2024, 9, 102236. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Knifton, L.; Robb, K.A.; Stahl, D.; Hann, M. Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 2019, 19, 943–951. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | LTBCSs’ Anxiety Levels | p/χ2 | |
|---|---|---|---|
| Low Levels of Anxiety | High Levels of Anxiety | ||
| ≤3.4 (VAS-A) (n = 43) | ≥3.5 (VAS-A) (n = 37) | ||
| Mean age ± SD, years | 48.41 ± 8.05 | 50.51 ± 8.02 | 0.63 a |
| Mean time since diagnosis ± SD, months | 91.52 ± 27.94 | 89.24 ± 30.99 | 0.49 a |
| Mean time since the first surgery ± SD, months | 88.43 ± 28.58 | 86.64 ± 31.23 | 0.50 a |
| Marital status, n (%) | |||
| Unmarried | 6 (14) | 7 (18.9) | |
| Married | 33 (76.7) | 22 (59.5) | |
| Divorced or separated | 2 (4.7) | 6 (16.2) | |
| Widowed | 2 (4.7) | 2 (5.4) | 0.27 b |
| Educational level, n (%) | |||
| Primary school | 15 (34.9) | 19 (51.4) | |
| Secondary school | 9 (20.9) | 9 (24.3) | |
| University | 19 (44.2) | 9 (24.3) | 0.16 b |
| Employment status, n (%) | |||
| Housewife | 15 (34.9) | 12 (27) | |
| Currently working | 13 (30.2) | 4 (10.8) | |
| Sick leave | 11 (25.6) | 15 (51.4) | |
| Retired | 4 (9.3) | 5 (10.8) | 0.06 b |
| Tobacco consumption, n (%) | |||
| Non-consumption | 24 (55.8) | 16 (43.2) | |
| Smoker | 9 (20.9) | 10 (27) | |
| Ex-smoker | 10 (23.3) | 11 (29.7) | 0.53 b |
| Alcohol consumption, n (%) | |||
| Non-consumption | 13 (30.2) | 17 (45.9) | |
| Monthly | 7 (16.3) | 12 (32.4) | |
| Weekly | 20 (46.5) | 7 (18.9) | |
| Daily | 3 (7) | 1 (2.7) | 0.06 b |
| Menopause, n (%) | |||
| No | 6 (14) | 5 (13.5) | |
| Yes | 37 (86) | 32 (86.5) | 0.95 b |
| Family history of breast cancer, n (%) | |||
| No | 25 (58.1) | 14 (37.8) | |
| Yes | 18 (41.9) | 23 (62.2) | 0.07 b |
| Tumor stage, n (%) | |||
| I | 14 (32.6) | 9 (24.3) | |
| II | 23 (53.5) | 23 (62.2) | |
| IIIa | 6 (14.0) | 5 (13.5) | 0.69 b |
| Type of treatment, n (%) | |||
| None | 0 (0) | 0 (0) | |
| Radiotherapy | 0 (0) | 3 (8.1) | |
| Chemotherapy | 2 (4.7) | 4 (10.8) | |
| Radiotherapy and chemotherapy | 41 (95.3) | 30 (81.1) | 0.08 b |
| Surgery, n (%) | |||
| Lumpectomy | 8 (18.6) | 8 (21.6) | |
| Quadrantectomy | 26 (60.5) | 13 (35.1) | |
| Unilateral mastectomy | 9 (20.9) | 12 (32.4) | |
| Bilateral mastectomy | 0 (0) | 4 (10.8) | 0.06 b |
| Type of medication, n (%) | |||
| None | 11 (25.6) | 8 (21.6) | |
| Tamoxifen | 17 (39.5) | 14 (37.8) | |
| Other types | 15 (34.9) | 15 (40.5) | 0.85 b |
| Metastasis, n (%) | |||
| No | 36 (83.7) | 30 (81.1) | |
| Yes | 7 (16.3) | 7 (18.9) | 0.75 b |
| Recurrence, n (%) | |||
| No | 36 (83.7) | 31 (83.8) | |
| Yes | 7 (16.3) | 6 (16.2) | 0.99 b |
| Currently seeing a psychologist or in the last three months, n (%) | |||
| No | 16 (37.2) | 17 (45.9) | |
| Yes | 27 (62.8) | 20 (54.1) | 0.42 b |
| Currently seeing a physiotherapist or in the last three months, n (%) | |||
| No | 17 (39.5) | 12 (32.4) | |
| Yes | 26 (60.5) | 25 (67.6) | 0.51 b |
| Variables | LTBCSs’ Anxiety Levels | p/χ2 | Cohen’s d | |
|---|---|---|---|---|
| Low Levels of Anxiety | High Levels of Anxiety | |||
| ≤3.4 (VAS-A) (n = 43) | ≥3.5 (VAS-A) (n = 37) | |||
| EVEA, mean ± SD (95% CI) a | ||||
| Sadness–Depression | 1.10 ± 1.38 (0.67–1.53) | 5.02 ± 2.30 (4.25–5.79) | <0.01 ** | >1.20 |
| Anger–Hostility | 0.64 ± 0.88 (0.37–0.91) | 4.11 ± 2.46 (3.29–4.93) | <0.01 ** | >1.20 |
| Happiness | 6.19 ± 2.41 (5.44–6.93) | 5.76 ± 8.55 (2.91–8.61) | <0.01 ** | 0.06 |
| PFS (domains), mean ± SD (95% CI) a | ||||
| Behavioral/Severity | 1.63 ± 2.07 (0.99–2.26) | 4.57 ± 2.86 (3.62–5.53) | <0.01 ** | 1.18 |
| Affective | 1.77 ± 2.35 (1.05–2.50) | 5.11 ± 3.07 (4.08–6.13) | <0.01 ** | >1.20 |
| Sensory | 2.08 ± 2.50 (1.31–2.85) | 5.09 ± 2.91 (4.12–6.06) | <0.01 ** | 1.11 |
| Cognitive/Mood | 1.72 ± 2.02 (1.09–2.34) | 4.92 ± 2.93 (3.94–5.90) | <0.01 ** | >1.20 |
| Total | 1.79 ± 2.03 (1.16–2.41) | 4.94 ± 2.68 (4.04–5.83) | <0.01 ** | >1.20 |
| VAS (cm), mean ± SD (95% CI) a | ||||
| Dominant arm | 1.23 ± 1.64 (0.72–1.73) | 3.56 ± 2.92 (2.59–4.54) | <0.01 ** | 0.98 |
| Non-dominant arm | 0.32 ± 0.89 (0.05–0.60) | 2.78 ± 3.39 (1.65–3.91) | <0.01 ** | 0.99 |
| BPI, mean ± SD (95% CI) a | ||||
| Intensity | 1.48 ± 1.66 (0.97–1.99) | 3.19 ± 2.97 (2.20–4.19) | 0.01 * | 0.71 |
| Interference | 1.01 ± 1.66 (0.50–1.52) | 3.20 ± 3.10 (2.17– 4.24) | 0.01 * | 0.88 |
| IFIS, mean ± SD (95% CI) | ||||
| General physical fitness | 3.55 ± 0.98 (3.25–3.86) | 2.97 ± 0.92 (2.66–3.28) | <0.01 ** | 0.61 |
| Cardiorespiratory fitness | 2.95 ± 1.23 (2.57–3.33) | 2.81 ± 0.93 (2.49–3.12) | 0.05 * | 0.13 |
| Muscular strength | 3.13 ± 1.05 (2.81–3.46) | 2.56 ± 0.89 (2.26–2.86) | 0.01 * | 0.59 |
| Speed/Agility | 3.25 ± 0.95 (2.96–3.54) | 2.59 ± 0.86 (2.30–2.88) | <0.01 ** | 0.73 |
| Flexibility | 3.09 ± 0.94 (2.80–3.38) | 2.62 ± 1.08 (2.25–2.98) | 0.03 * | 0.46 |
| MLTPA, n (%) b | ||||
| Inactive: ≤3 (MET—hour/week) | 8 (18.6) | 13 (35.1) | 0.24 | |
| Low active: 3.1–7.4 (MET—hour/week) | 19 (44.2) | 13 (35.1) | ||
| Active: ≥7.5 (MET—hour/week) | 16 (37.2) | 11 (29.7) | - | |
| Variables | LTBCSs’ Anxiety Levels | p Values | Cohen’s d | |
|---|---|---|---|---|
| Low Levels of Anxiety | High Levels of Anxiety | |||
| ≤3.4 (VAS-A) (n = 43) | ≥3.5 (VAS-A) (n = 37) | |||
| Functioning Scales QLQ-C30, mean ± SD (95% CI) | ||||
| Physical Functioning | 29.06 ± 16.70 (23.92–34.20) | 36.02 ± 21.34 (28.90–43.14) | 0.20 | 0.36 |
| Role Functioning | 90.10 ± 14.78 (85.55–94.65) | 71.72 ± 21.68 (64.49–78.95) | <0.01 ** | 0.99 |
| Emotional Functioning | 88.37 ± 23.43 (81.15–95.58) | 68.91 ± 32.19 (58.18–79.65) | <0.01 ** | 0.69 |
| Cognitive Functioning | 79.06 ± 21.15 (72.55–85.58) | 48.64 ± 32.30 (37.87–59.41) | <0.01 ** | 1.11 |
| Social Functioning | 74.41 ± 24.21 (66.96–81.87) | 47.29 ± 31.79 (36.69–57.89) | <0.01 ** | 0.96 |
| Symptom Scales QLQ-C30, mean ± SD (95% CI) | ||||
| Fatigue | 60.36 ± 36.50 (48.18–72.53) | 82.94 ± 23.14 (75.82–90.06) | <0.01 ** | 0.74 |
| Nausea and Vomiting | 22.99 ± 24.41 (15.48–30.51) | 52.25 ± 31.30 (41.81–62.69) | <0.01 ** | 1.04 |
| Pain | 3.48 ± 11.81 (−0.14–7.12) | 12.16 ± 22.78 (4.56–19.75) | 0.02 * | 0.48 |
| Single Items QLQ-C30, mean ± SD (95% CI) | ||||
| Dyspnea | 25.58 ± 23.94 (18.21–32.95) | 54.05 ± 34.11 (42.68–65.42) | <0.01 ** | 0.97 |
| Insomnia | 13.95 ± 25.44 (6.12–21.78) | 34.23 ± 33.78 (22.97–45.49) | <0.01 ** | 0.68 |
| Appetite Loss | 42.24 ± 32.19 (32.34–52.15) | 59.45 ± 34.36 (48.00–70.91) | 0.02 * | 0.52 |
| Constipation | 9.30 ± 23.37 (2.10–16.49) | 14.41 ± 27.82 (5.13–23.69) | 0.34 | 0.20 |
| Diarrhea | 18.21 ± 27.41 (9.77–26.65) | 33.33 ± 35.13 (21.61–45.04) | 0.04 * | 0.48 |
| Financial Difficulties | 4.65 ± 11.68 (1.05–8.24) | 20.72 ± 29.76 (10.79–30.64) | 0.04 * | 0.71 |
| Global Health Status QLQ-C30, mean ± SD (95% CI) | ||||
| Global Health Status | 35.22 ± 39.16 (22.16–48.28) | 12.40 ± 24.15 (4.97–19.83) | <0.01 ** | 0.70 |
| Summary Score QLQ-C30, mean ± SD (95% CI) | ||||
| Summary Score | 72.48 ± 11.22 (69.02–75.93) | 57.87 ± 16.25 (52.45–63.29) | <0.01 ** | 1.05 |
| Functional Scales QLQ-BR23, mean ± SD (95% CI) | ||||
| Body Image | 70.93 ± 19.36 (64.97–76.88) | 55.18 ± 23.27 (47.42–62.93) | <0.01 ** | 0.74 |
| Sexual Functioning | 85.27 ± 19.65 (79.22–91.32) | 67.79 ± 33.22 (56.71–78.87) | 0.01 * | 0.64 |
| Sexual Enjoyment | 23.64 ± 19.66 (17.59–29.69) | 19.82 ± 22.85 (12.20–27.43) | 0.23 | 0.18 |
| Future Perspective | 26.12 ± 16.21 (17.38–34.86) | 37.20 ± 23.24 (30.05–44.36) | 0.01 * | 0.55 |
| Symptom Scales QLQ-BR23, mean ± SD (95% CI) | ||||
| Systemic Therapy Side Effects | 42.34 ± 37.39 (29.87–54.80) | 65.11 ± 36.33 (53.93–76.29) | <0.01 ** | 0.62 |
| Breast Symptoms | 20.01 ± 18.33 (14.37–25.65) | 38.60 ± 22.88 (30.97–46.24) | <0.01 ** | 0.90 |
| Arm Symptoms | 18.02 ± 20.32 (11.76–24.27) | 35.58 ± 31.52 (25.07–46.09) | 0.01 * | 0.66 |
| Upset By Hair Loss | 22.47 ± 23.44 (15.26–29.69) | 42.64 ± 34.99 (30.97–54.30) | 0.01 * | 0.68 |
| Model | Variables/Predictors | β | 95% CI | t | p Values | Linear Regression Equation Y = a + bX |
|---|---|---|---|---|---|---|
| Model 1 (r2 = 0.432) | Total CRF (PFS) | 0.65 | 0.45 ± 0.76 | 7.69 | <0.01 ** | Anxiety = 1.08 + (0.60 Total CRF) |
| Model 2 (r2 = 0.470) | Total CRF (PFS) | 0.51 | 0.28 ± 0.66 | 4.97 | <0.01 ** | Anxiety = 2.86 + (0.47 Total CRF) + (−0.02 Cognitive Functioning) |
| Cognitive Functioning (QLQ-C30) | −0.24 | −0.03 ± −0.00 | −2.37 | 0.02 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez-Salvago, F.; Pujol-Fuentes, C.; Medina-Luque, J.; Figueroa-Mayordomo, M.; Boquete-Pumar, C.; Atienzar-Aroca, S. Influence and Predictors of Anxiety on Health Status ≥ 5 Years Beyond Breast Cancer Diagnosis in Spain: A Cross-Sectional Study. Life 2025, 15, 932. https://doi.org/10.3390/life15060932
Álvarez-Salvago F, Pujol-Fuentes C, Medina-Luque J, Figueroa-Mayordomo M, Boquete-Pumar C, Atienzar-Aroca S. Influence and Predictors of Anxiety on Health Status ≥ 5 Years Beyond Breast Cancer Diagnosis in Spain: A Cross-Sectional Study. Life. 2025; 15(6):932. https://doi.org/10.3390/life15060932
Chicago/Turabian StyleÁlvarez-Salvago, Francisco, Clara Pujol-Fuentes, Jose Medina-Luque, Maria Figueroa-Mayordomo, Carmen Boquete-Pumar, and Sandra Atienzar-Aroca. 2025. "Influence and Predictors of Anxiety on Health Status ≥ 5 Years Beyond Breast Cancer Diagnosis in Spain: A Cross-Sectional Study" Life 15, no. 6: 932. https://doi.org/10.3390/life15060932
APA StyleÁlvarez-Salvago, F., Pujol-Fuentes, C., Medina-Luque, J., Figueroa-Mayordomo, M., Boquete-Pumar, C., & Atienzar-Aroca, S. (2025). Influence and Predictors of Anxiety on Health Status ≥ 5 Years Beyond Breast Cancer Diagnosis in Spain: A Cross-Sectional Study. Life, 15(6), 932. https://doi.org/10.3390/life15060932