

Resistance Training Before Hyperalgesia Induction Promotes Analgesic Effects Through Central and Peripheral Biomarker Modulation in an Experimental Fibromyalgia-like Model
 ,
,  ,
,  , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
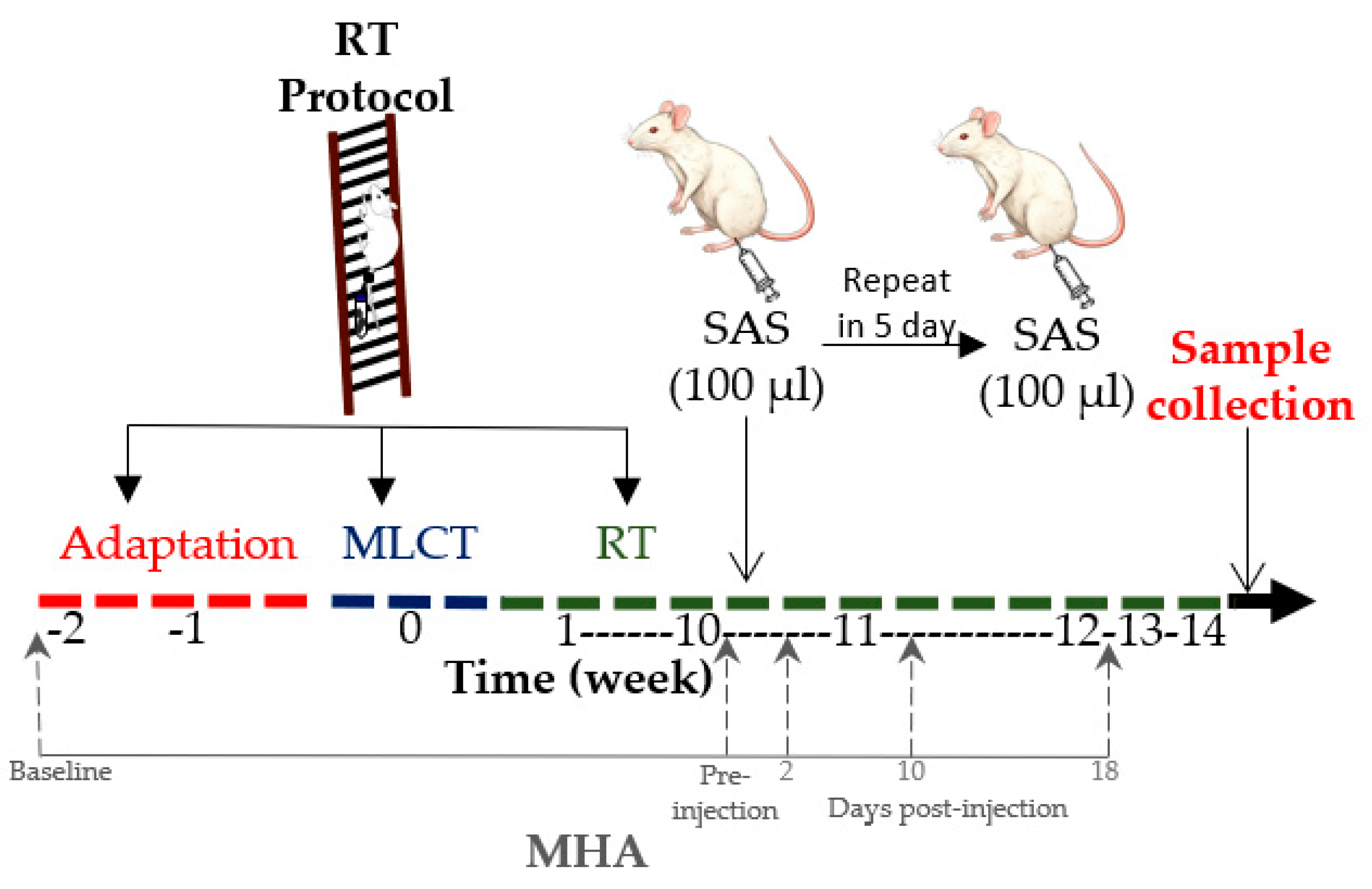
2.1. Animals and Study Design
2.2. Resistance Training
2.2.1. Adaptation Phase
2.2.2. Maximum Load Carrying Test
2.2.3. Resistance Training Protocol
2.3. Hyperalgesia Induction
2.4. Mechanical Hyperalgesia Assessment
2.5. Sample Collection
2.6. Muscle IL-6 and IL-10 Determination
2.7. Thalamic Serotonin Determination
2.8. Statistical Analysis
3. Results
3.1. Mechanical Hyperalgesia
3.2. Physical Performance
3.3. IL-6 and IL-10 in the Gastrocnemius Muscle
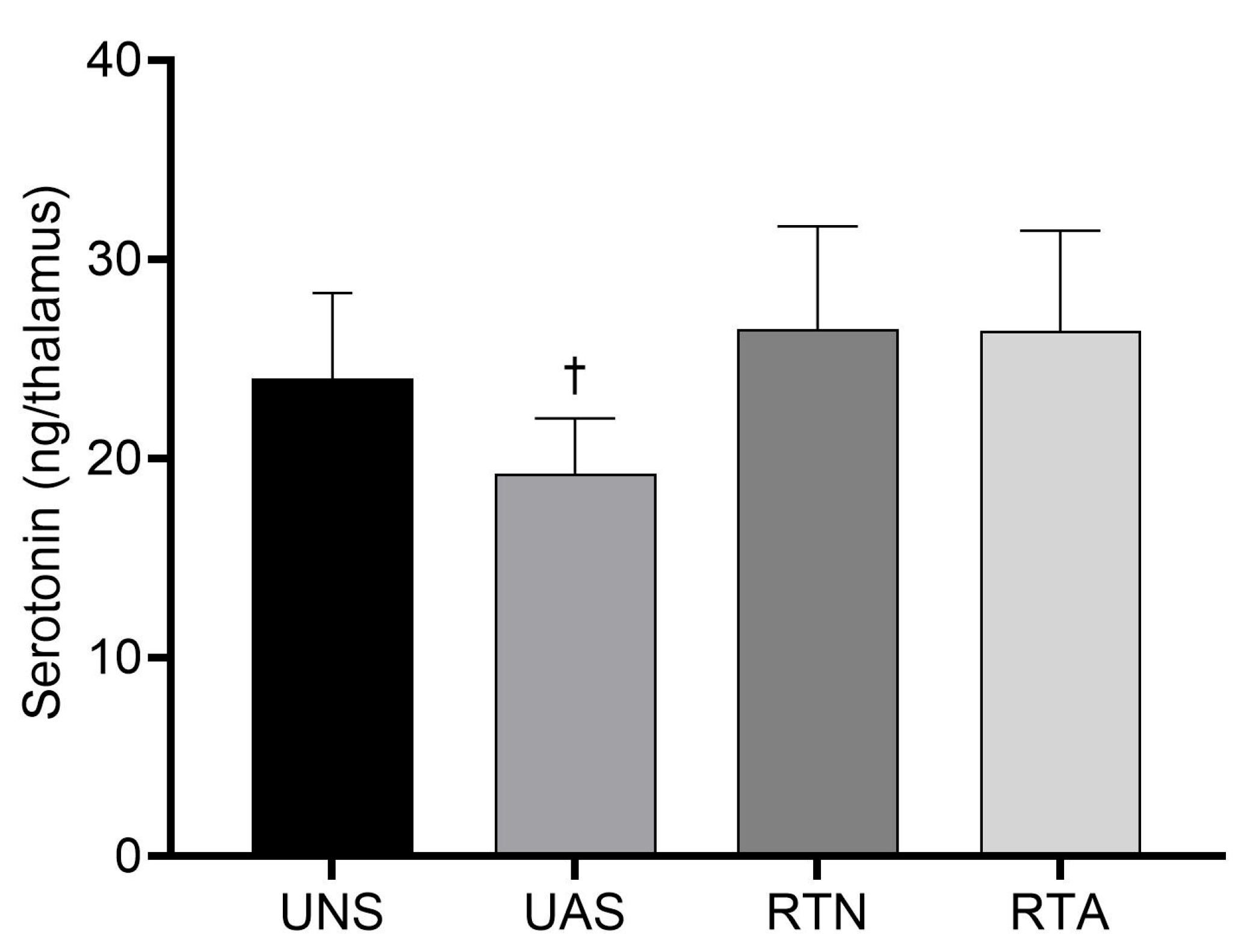
3.4. Serotonin in the Thalamus
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromialgia: Prevalencia, perfiles epidemiológicos y costes económicos. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia pathogenesis and treatment options update. Curr. Pain Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef]
- Favero, G.; Bonomini, F.; Franco, C.; Rezzani, R. Mitochondrial dysfunction in skeletal muscle of a fibromyalgia model: The potential benefits of melatonin. Int. J. Mol. Sci. 2019, 20, 765. [Google Scholar] [CrossRef]
- Heymann, R.E.; Paiva, E.S.; Martinez, J.E.; Helfenstein, M.; Rezende, M.C.; Provenza, J.R.; Souza, E.J. Novas diretrizes para o diagnóstico da fibromialgia. Rev. Bras. Reumatol. 2017, 57, S467–S476. [Google Scholar] [CrossRef]
- Marques, A.P.; Santo, A.D.S.D.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. A prevalência de fibromialgia: Atualização da revisão de literatura. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Gota, C.E. What you can do for your fibromyalgia patient. Clevel. Clin. J. Med. 2018, 85, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Pintó, I.; Agmon-Levin, N.; Howard, A.; Shoenfeld, Y. Fibromyalgia and cytokines. Immunol. Lett. 2014, 161, 200–203. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology 2021, 60, 2602–2614. [Google Scholar] [CrossRef]
- Al Sharie, S.; Varga, S.J.; Al-Husinat, L.I.; Sarzi-Puttini, P.; Araydah, M.; Bal’awi, B.R.; Varrassi, G. Unraveling the complex web of fibromyalgia: A narrative review. Medicina 2024, 60, 272. [Google Scholar] [CrossRef]
- Sluka, K.A.; Kalra, A.; Moore, S.A. Unilateral intramuscular injections of acidic saline produce a bilateral, long-lasting hyperalgesia. Muscle Nerve 2001, 24, 37–46. [Google Scholar] [CrossRef]
- Brito, R.G.; Rasmussen, L.A.; Sluka, K.A. Regular physical activity prevents development of chronic muscle pain through modulation of supraspinal opioid and serotonergic mechanisms. Pain Rep. 2017, 2, e618. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, R.; Rasmussen, L.; Sluka, K.A.; Chapleau, M.W. Exercise prevents development of autonomic dysregulation and hyperalgesia in a mouse model of chronic muscle pain. Pain 2016, 157, 387–398. [Google Scholar] [CrossRef]
- Larsson, A.; Palstam, A.; Löfgren, M.; Ernberg, M.; Bjersing, J.; Bileviciute-Ljungar, I.; Mannerkorpi, K. Resistance exercise improves muscle strength, health status and pain intensity in fibromyalgia—A randomized controlled trial. Arthritis Res. Ther. 2015, 17, 161. [Google Scholar] [CrossRef] [PubMed]
- Maestre Cascales, C.; Peinado Lozano, A.B.; Rojo González, J.J. Effects of a strength training program on daily living in women with fibromyalgia. J. Hum. Sport Exerc. 2019, 14, 736–747. [Google Scholar] [CrossRef]
- García-Martínez, A.M.; De Paz, J.A.; Márquez, S. Effects of an exercise programme on self-esteem, self-concept and quality of life in women with fibromyalgia: A randomized controlled trial. Rheumatol. Int. 2012, 32, 1869–1876. [Google Scholar] [CrossRef]
- Sener, U.; Ucok, K.; Ulasli, A.M.; Genc, A.; Karabacak, H.; Coban, N.F.; Cevik, H. Evaluation of health-related physical fitness parameters and association analysis with depression, anxiety, and quality of life in patients with fibromyalgia. Int. J. Rheum. Dis. 2016, 19, 763–772. [Google Scholar] [CrossRef]
- Chen, J.; Han, B.; Wu, C. On the superiority of a combination of aerobic and resistance exercise for fibromyalgia syndrome: A network meta-analysis. Front. Psychol. 2022, 13, 949256. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.; Spencer, H.; Kortebein, P. Exercise recommendations in patients with newly diagnosed fibromyalgia. PM&R 2012, 4, 252–255. [Google Scholar]
- Hornberger, T.A., Jr.; Farrar, R.P. Physiological hypertrophy of the FHL muscle following 8 weeks of progressive resistance exercise in the rat. Can. J. Appl. Physiol. 2004, 29, 16–31. [Google Scholar] [CrossRef]
- Chang, C.T.; Fong, S.W.; Lee, C.H.; Chuang, Y.C.; Lin, S.H.; Chen, C.C. Involvement of acid-sensing ion channel 1b in the development of acid-induced chronic muscle pain. Front. Neurosci. 2019, 13, 1247. [Google Scholar] [CrossRef]
- Yamashita, S.; Dozono, N.; Tobori, S.; Nagayasu, K.; Kaneko, S.; Shirakawa, H.; Ueda, H. Peripheral Beta-2 adrenergic receptors mediate the sympathetic efferent activation from central nervous system to splenocytes in a mouse model of fibromyalgia. Int. J. Mol. Sci. 2023, 24, 3465. [Google Scholar] [CrossRef] [PubMed]
- Jibira, Y.; Boakye-Gyasi, E.; Abotsi, W.K.M.; Amponsah, I.K.; Duah, P.; Baah, F.K.; Woode, E. Antinociceptive effects of a hydroethanolic stem bark extract of Burkea africana. Heliyon 2022, 8, e08852. [Google Scholar] [CrossRef] [PubMed]
- Staud, R.; Weyl, E.E.; Bartley, E.; Price, D.D.; Robinson, M.E. Analgesic and anti-hyperalgesic effects of muscle injections with lidocaine or saline in patients with fibromyalgia syndrome. Eur. J. Pain 2014, 18, 803–812. [Google Scholar] [CrossRef]
- Whitehead, R.A.; Lam, N.L.; Sun, M.S.; Sanchez, J.; Noor, S.; Vanderwall, A.G.; Milligan, E.D. Chronic sciatic neuropathy in rat reduces voluntary wheel-running activity with concurrent chronic mechanical allodynia. Anesth. Analg. 2017, 124, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Park, M.Y.; Han, D.; Lim, J.H.; Shin, M.K.; Han, Y.R.; Kim, D.H.; Kim, K.S. Assessment of pressure pain thresholds in collisions with collaborative robots. PLoS ONE 2019, 14, e0215890. [Google Scholar] [CrossRef]
- Madden, V.; Bellan, V.; Russek, L.; Camfferman, D.; Vlaeyen, J.; Moseley, G. Pain by association? Experimental modulation of human pain thresholds using classical conditioning. J. Pain 2016, 17, 1105–1115. [Google Scholar] [CrossRef]
- Alvarez, P.; Gear, R.W.; Green, P.G.; Levine, J.D. IB4-saporin attenuates acute and eliminates chronic muscle pain in the rat. Exp. Neurol. 2012, 233, 859–865. [Google Scholar] [CrossRef]
- Chen, L.; Chen, W.; Qian, X.; Fang, Y.; Zhu, N. Liquiritigenin alleviates mechanical and cold hyperalgesia in a rat neuropathic pain model. Sci. Rep. 2014, 4, 5676. [Google Scholar] [CrossRef]
- Joseph, E.; Levine, J. Multiple PKCε-dependent mechanisms mediating mechanical hyperalgesia. Pain 2010, 150, 17–21. [Google Scholar] [CrossRef]
- Prado, F.; Vieira, W.; Magalhães, S.; Bonet, I.; Tambeli, C. The onset speed of hyperglycemia is important to the development of neuropathic hyperalgesia in streptozotocin-induced diabetic rats. Eur. J. Neurosci. 2020, 52, 3642–3651. [Google Scholar] [CrossRef]
- Li, J.; Thorn, D.; Qiu, Y.; Peng, B.; Zhang, Y. Antihyperalgesic effects of imidazoline I2 receptor ligands in rat models of inflammatory and neuropathic pain. Br. J. Pharmacol. 2014, 171, 1580–1590. [Google Scholar] [CrossRef] [PubMed]
- Snow, N.J.; Kirkland, M.C.; Downer, M.B.; Murphy, H.M.; Ploughman, M. Transcranial magnetic stimulation maps the neurophysiology of chronic noncancer pain: A scoping review. Medicine 2022, 101, e31774. [Google Scholar] [CrossRef] [PubMed]
- Paxinos, G.; Watson, C. The Rat Brain in Stereotaxic Coordinates; Academic Press: San Diego, CA, USA, 2006. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Dina, O.A.; Levine, J.D.; Green, P.G. Enhanced cytokine-induced mechanical hyperalgesia in skeletal muscle produced by a novel mechanism in rats exposed to unpredictable sound stress. Eur. J. Pain 2011, 15, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.M.; An, J. Cytokines, inflammation, and pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef]
- Kayabaş, M.; Şahin, L.; Makav, M.; Alwazeer, D.; Aras, L.; Yiğit, S.; LeBaron, T.W. Protective Effect of Hydrogen-Rich Saline on Spinal Cord Damage in Rats. Pharmaceuticals 2023, 16, 527. [Google Scholar] [CrossRef] [PubMed]
- Russell, I.J. Neurochemische Pathogenese der Fibromyalgie. Z. Rheumatol. 1998, 57, S63–S66. [Google Scholar] [CrossRef]
- Rezende, R.M.; Coimbra, R.S.; Kohlhoff, M.; Favarato, L.S.C.; Martino, H.S.D.; Leite, L.B.; Natali, A.J. Effects of tryptophan and physical exercise on the modulation of mechanical hypersensitivity in a fibromyalgia-like model in female rats. Cells 2024, 13, 1647. [Google Scholar] [CrossRef]
- Lima, L.V.; Abner, T.S.S.; Sluka, K.A. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. J. Physiol. 2017, 595, 4141–4150. [Google Scholar] [CrossRef]
- Rabelo, P.C.; Almeida, T.F.; Guimarães, J.B.; Barcellos, L.A.; Cordeiro, L.M.; Moraes, M.M.; Coimbra, C.C.; Szawka, R.E.; Soares, D.D. Intrinsic exercise capacity is related to differential monoaminergic activity in the rat forebrain. Brain Res. Bull. 2015, 112, 7–13. [Google Scholar] [CrossRef]
- Aguiar, G.C.; Do Nascimento, M.R.; De Miranda, A.S.; Rocha, N.P.; Teixeira, A.L.; Scalzo, P.L. Effects of an exercise therapy protocol on inflammatory markers, perception of pain, and physical performance in individuals with knee osteoarthritis. Rheumatol. Int. 2015, 35, 525–531. [Google Scholar] [CrossRef]
- Forti, L.N.; Njemini, R.; Beyer, I.; Eelbode, E.; Meeusen, R.; Mets, T.; Bautmans, I. Strength training reduces circulating interleukin-6 but not brain-derived neurotrophic factor in community-dwelling elderly individuals. Age 2014, 36, 9704. [Google Scholar] [CrossRef] [PubMed]
- Padilha, C.S.; Borges, F.H.; Costa Mendes da Silva, L.E.; Frajacomo, F.T.T.; Jordao, A.A.; Duarte, J.A.; Cecchini, R.; Guarnier, F.A.; Deminice, R. Resistance exercise attenuates skeletal muscle oxidative stress, systemic pro-inflammatory state, and cachexia in Walker-256 tumor-bearing rats. Appl. Physiol. Nutr. Metab. 2017, 42, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Burghardt, R.D.; Kazim, M.A.; Rüther, W.; Niemeier, A.; Strahl, A. The impact of physical activity on serum levels of inflammatory markers in rheumatoid arthritis: A systematic literature review. Rheumatol. Int. 2019, 39, 793–804. [Google Scholar] [CrossRef]
- Conroy, S.M.; Courneya, K.S.; Brenner, D.R.; Shaw, E.; O’Reilly, R.; Yasui, Y.; Woolcott, C.G.; Friedenreich, C.M. Impact of aerobic exercise on levels of IL-4 and IL-10: Results from two randomized intervention trials. Cancer Med. 2016, 5, 2385–2397. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Saeed, N.B.; Melhem, M.B.; Al-Ababneh, H. The impact of some types of physical activity on the level of releasing serotonin hormone (a comparative study). Educ. Psychol. Sci. Ser. 2023, 2, 119–134. [Google Scholar]
- Sousa, M.; Oliveira, R.; Brito, J.P.; Martins, A.D.; Moutão, J.; Alves, S. Effects of combined training programs in individuals with fibromyalgia: A systematic review. Healthcare 2023, 11, 1708. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Time | UNS | UAS | RTN | RTA | η2 |
|---|---|---|---|---|---|
| 0 | 37.25 ± 4.63 | 37.43 ± 4.54 | 39.47 ± 3.46 | 40.81 ± 4.69 | 0.09 |
| 70 | 40.75 ± 3.20 | 41.99 ± 1.63 | 41.75 ± 3.51 | 40.55 ± 2.57 | 0.00 |
| 73 | 44.66 ± 3.24 | 24.63 ± 4.33 *#✝ | 41.27 ± 2.34 | 32.58 ± 4.87 *# | 0.80 |
| 81 | 43.03 ± 3.38 | 30.28 ± 3.46 *#✝ | 39.32 ± 2.10 | 39.28 ± 1.78 | 0.60 |
| 89 | 42.04 ± 2.58 | 37.81 ± 3.21 *✝ | 39.12 ± 1.97 | 41.15 ± 3.57 | 0.03 |
| Time | UNS | UAS | RTN | RTA | η2 |
|---|---|---|---|---|---|
| 0 | 308.1 ± 27.5 | 325.3 ± 61.7 | 327.4 ± 45.0 | 338.0 ± 54.0 | 0.03 |
| 70 | 336.3 ± 46.3 | 331.8 ± 22.5 | 421.3 ± 40.9 *& | 462.0 ± 42.0 *&# | 0.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiapeta, A.V.; de Oliveira, L.L.; Leite, L.B.; da Silva, B.A.F.; Costa, S.F.F.; Soares, L.L.; Moraes, A.A.d.; Drummond, L.R.; Forte, P.; José Natali, A.; et al. Resistance Training Before Hyperalgesia Induction Promotes Analgesic Effects Through Central and Peripheral Biomarker Modulation in an Experimental Fibromyalgia-like Model. Life 2025, 15, 849. https://doi.org/10.3390/life15060849
Chiapeta AV, de Oliveira LL, Leite LB, da Silva BAF, Costa SFF, Soares LL, Moraes AAd, Drummond LR, Forte P, José Natali A, et al. Resistance Training Before Hyperalgesia Induction Promotes Analgesic Effects Through Central and Peripheral Biomarker Modulation in an Experimental Fibromyalgia-like Model. Life. 2025; 15(6):849. https://doi.org/10.3390/life15060849
Chicago/Turabian StyleChiapeta, Andrês Valente, Leandro Licursi de Oliveira, Luciano Bernardes Leite, Bruna Aparecida Fonseca da Silva, Sebastião Felipe Ferreira Costa, Leôncio Lopes Soares, Alexa Alves de Moraes, Lucas Rios Drummond, Pedro Forte, Antônio José Natali, and et al. 2025. "Resistance Training Before Hyperalgesia Induction Promotes Analgesic Effects Through Central and Peripheral Biomarker Modulation in an Experimental Fibromyalgia-like Model" Life 15, no. 6: 849. https://doi.org/10.3390/life15060849
APA StyleChiapeta, A. V., de Oliveira, L. L., Leite, L. B., da Silva, B. A. F., Costa, S. F. F., Soares, L. L., Moraes, A. A. d., Drummond, L. R., Forte, P., José Natali, A., & Carneiro-Júnior, M. A. (2025). Resistance Training Before Hyperalgesia Induction Promotes Analgesic Effects Through Central and Peripheral Biomarker Modulation in an Experimental Fibromyalgia-like Model. Life, 15(6), 849. https://doi.org/10.3390/life15060849