1. Introduction
Aortic stenosis (AS) is one of the most common and severe valvular heart diseases affecting older adults [
1,
2]. It is characterized by the narrowing of the aortic valve, which impedes blood flow from the left ventricle to the aorta, leading to increased cardiac workload, left ventricular hypertrophy, and, eventually, heart failure, if left untreated. Majority of morbidity and mortality attributable to valvular heart disease worldwide, including AS, is due to rheumatic heart disease, which is commonly seen as a cause of AS in low-income countries. In high-income countries, calcific aortic valve disease (CAVD) is the prevalent cause of AS [
2,
3]. The disease primarily stems from progressive calcification of the valve, often exacerbated by age-related factors, metabolic conditions, and congenital anomalies such as bicuspid aortic valves [
2,
3]. Globally, the prevalence of AS increases significantly with age. In individuals aged 75 years and older, the prevalence ranges between 9% and 13%, making it a leading cause of morbidity in elderly populations [
2,
4]. The Global Burden of Disease study highlights that in 2021, calcific aortic valve disease (CAVD) contributed to 2.24 million disability-adjusted life years (DALYs), marking a 30.5% increase since 1990 due to aging populations [
3]. Rising prevalence of valvular heart disease associated with advancing age combined with rapid aging of populations worldwide has labeled valvular heart diseases as the “next cardiac epidemic” [
5,
6]. Additionally, individuals with congenital anomalies, such as bicuspid aortic valves, are predisposed to earlier onset of AS [
2,
7]. The number of aortic valve procedures performed over the past decades has been constantly increasing, while at the same time, the number of mitral valve surgeries remains constant.
Cardiopulmonary bypass (CPB) is an essential technique in cardiac surgery that temporarily takes over the functions of the heart and lungs, enabling surgeons to perform complex procedures under controlled conditions. However, the benefits of CPB come at the cost of a significant systemic inflammatory response syndrome (SIRS), which can lead to multi-organ dysfunction, postoperative complications, and prolonged recovery. This inflammatory response arises from blood contact with non-endothelial surfaces, ischemia–reperfusion injury, and activation of various immune and coagulation pathways [
8,
9,
10,
11,
12]. Monocytes and endothelial cells produce pro-inflammatory cytokines, including interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), IL-8, and IL-1β, which amplify the inflammatory cascade [
8,
9,
10]. Neutrophils adhere to the endothelium, release reactive oxygen species (ROS) and proteolytic enzymes, and contribute to microvascular injury and capillary leak syndrome. The second phase involves ischemia–reperfusion injury, which occurs when blood flow is restored after a period of ischemia, particularly to the myocardium, lungs, kidneys, and intestines [
8,
12]. This phase triggers oxidative stress, increased cytokine production, and further endothelial injury, perpetuating the inflammatory response. Reactive oxygen species exacerbate endothelial dysfunction, increase vascular permeability, and damage cellular structures [
8,
9,
12]. CPB also results in the shedding of the glycocalyx layer, impairing vascular integrity and promoting edema and inflammation. IL-6 is a central pro-inflammatory cytokine and a key marker of the inflammatory response during CPB. Elevated IL-6 levels correlate with postoperative complications, including impaired lung function, circulatory instability, and organ dysfunction [
8,
9]. TNF-α is an early pro-inflammatory cytokine that promotes leukocyte recruitment, vascular permeability, and tissue injury. Although TNF-α levels during CPB are generally lower than IL-6, elevations are associated with poor outcomes [
8,
9,
10,
12]. The cytokine surge and endothelial activation contribute to the development of SIRS, characterized by vasoplegia, often requiring vasopressors, pulmonary dysfunction due to increased alveolar-capillary permeability resulting in acute lung injury or ARDS, acute kidney injury (AKI) caused by ischemia, oxidative stress, and inflammation, and coagulopathy and bleeding due to platelet dysfunction, fibrinolysis, and disruption of the coagulation cascade [
8,
9,
12,
13]. It is estimated that approximately 1.5 to 2 million CPB procedures are performed each year as part of open-heart surgeries [
14]. Despite advances in biocompatible CPB circuits and minimally invasive techniques, inflammation remains a challenge.
Dexmedetomidine is an α2-adrenergic agonist commonly used in anesthesia and intensive care settings. It is potent and highly selective for α2 adrenergic receptors with α2: α1 ratio of 1620:1 [
15]. Dexmedetomidine acts on α2-adrenergic receptors in the central nervous system, particularly in the locus coeruleus, resulting in sedation that resembles natural sleep. Its sympatholytic effects reduce heart rate and blood pressure, while its analgesic action is mediated through both spinal and supraspinal mechanisms. Dexmedetomidine also influences the cholinergic anti-inflammatory pathway, which may play a role in mitigating the systemic inflammatory response to surgical trauma and ischemia–reperfusion injury [
16]. Even though it has been approved for sedation of adult intensive care unit patients [
17], dexmedetomidine is widely used as an adjunct to general anesthesia and as a sedative agent in patients undergoing procedures under regional anesthesia. Its opioid-sparing effect is particularly valuable in multimodal analgesia protocols aimed at reducing opioid consumption and minimizing opioid-related side effects, such as respiratory depression, nausea, and postoperative delirium [
18]. Dexmedetomidine has demonstrated cardioprotective properties in ischemia–reperfusion models, reducing myocardial injury and improving cardiac function [
19]. Preclinical studies suggest that dexmedetomidine protects renal function by activating the cholinergic anti-inflammatory pathway and reducing oxidative stress [
16,
20,
21,
22]. Dexmedetomidine’s neuroprotective effects are particularly useful, especially in elderly patients undergoing cardiac and non-cardiac surgery. It attenuates neuroinflammation, reduces apoptosis, and promotes anti-oxidative responses, thereby protecting against ischemic brain injury [
23].
Although substantial evidence supports the beneficial effects of dexmedetomidine in the cardiac surgery setting [
12,
19,
23,
24,
25,
26,
27], definitive recommendations regarding the optimal timing, dosage, or specific patient cohort that would benefit most from its effects are still lacking. Our study aimed to evaluate whether dexmedetomidine exerts a clinically relevant anti-inflammatory effect in patients undergoing open-heart surgery and to determine the optimal dose.
4. Discussion
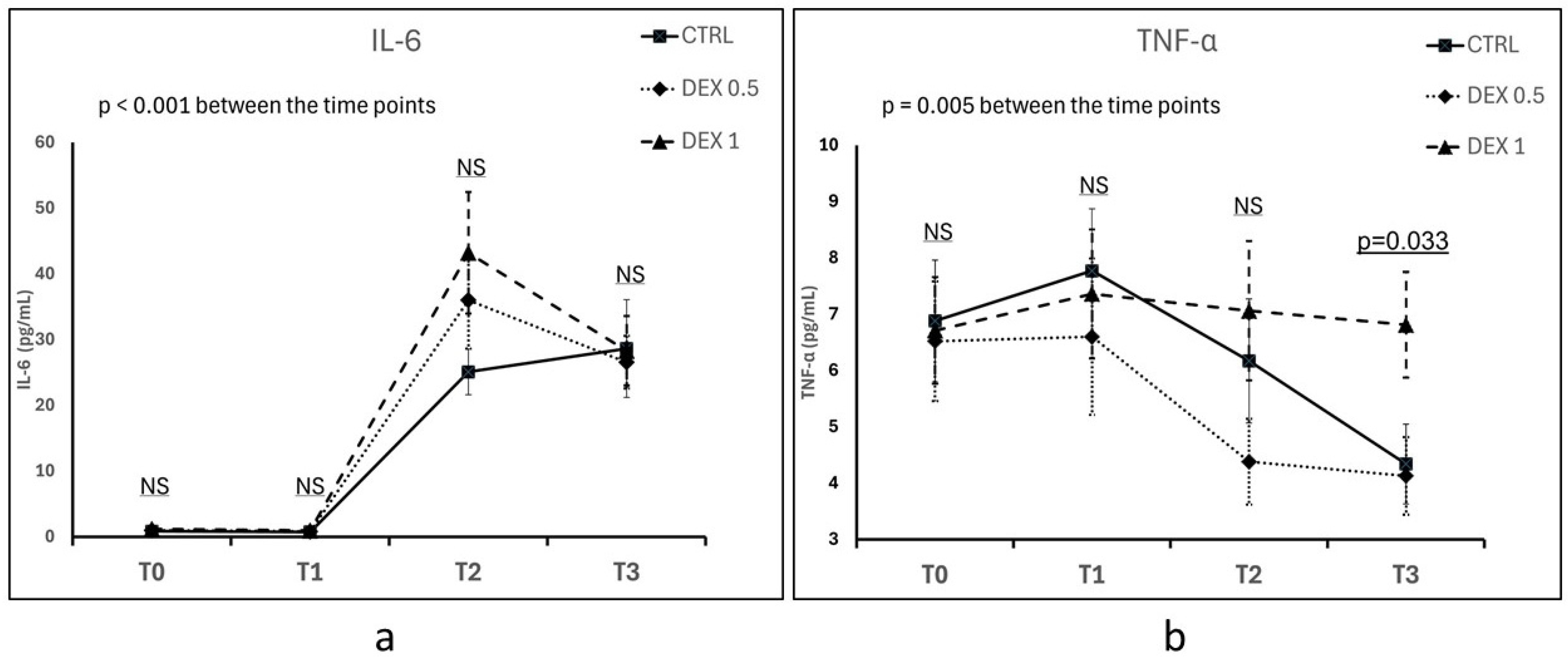
The inflammatory response following CPB is characterized by the release of pro-inflammatory cytokines, particularly IL-6 and TNF-α. The aim of this study was to investigate the effects of dexmedetomidine on inflammatory markers, clinical outcomes, and postoperative recovery in patients undergoing SAVR requiring CPB. Our results highlight the potential immunomodulatory and clinical benefits of dexmedetomidine but also demonstrate that some previously reported effects could not be readily reproduced in our cohort.
The inflammatory response to CPB was confirmed by a significant increase in IL-6 and TNF-α levels in all patient groups postoperatively. Although dexmedetomidine was expected to attenuate this inflammatory surge, our results were mixed. Group 2 (high-dose dexmedetomidine) exhibited the highest postoperative IL-6 levels, though the differences between groups were not statistically significant. However, TNF-α levels were significantly higher in Group 2 at 12 h post-CPB. A notable finding was the correlation between the prolonged CPB duration in Group 2 and the elevated TNF-α levels 12 h post-CPB. This suggests that prolonged extracorporeal circulation may attenuate the expected immunomodulatory effects of dexmedetomidine, despite the administration of a high dose of the studied drug in this group. These findings support the notion that the magnitude of systemic inflammation is multifactorial, influenced not only by pharmacological interventions but also by surgical complexity and perfusion-related factors.
The significantly longer CPB duration in Group 2 warrants discussion, as CPB time varies even within the same surgical procedure. In SAVR, multiple factors influence CPB duration, including surgical complexity and the degree of valve calcification. Extensive calcification necessitates more thorough decalcification, prolonging both operative and CPB times. Despite a standardized surgical protocol, surgeon experience, intraoperative decisions, and technical variability (e.g., speed of aortic cross-clamping, cardioplegia administration, and suture placement) can introduce differences in CPB duration. Additionally, despite randomization, the small sample size may have led to an uneven distribution of surgical complexity across groups. While CPB time differences were observed, they are likely multifactorial, influenced by patient-specific factors, intraoperative variability, and perfusion-related decisions rather than dexmedetomidine administration.
In our study, the neutrophil-to-lymphocyte ratio (NLR) was analyzed as part of the baseline characteristics, as peripheral blood differential counts were only available upon hospital admission. NLR reflects the balance between innate immune activation (neutrophils) and adaptive immune suppression (lymphocytes). No statistically significant differences in NLR were observed between groups at baseline, suggesting that preoperative systemic inflammatory status was comparable across all groups. While IL-6 and TNF-α were the primary cytokines analyzed in this study, NLR could serve as a valuable inflammatory marker in the context of CPB, reflecting perioperative stress, immune suppression, and postoperative outcomes. Given its cost-effectiveness and widespread clinical availability, NLR may be a useful complementary biomarker for assessing systemic inflammation in future trials.
The incidence of postoperative delirium (CAM-positive cases) was highest in the control group and lowest in Group 2 on POD1. Although the overall incidence of delirium did not reach statistical significance, a trend was observed, aligning with previous reports on the neuroprotective role of dexmedetomidine. The reduction in delirium may be attributed to the sedative effect of dexmedetomidine, which preserves sleep architecture and reduces opioid consumption.
In contrast, the incidence of AF was numerically lower in Group 2, but this difference did not reach statistical significance. Considering the established role of systemic inflammation in AF development, the observed trend may reflect the sympatholytic effects of dexmedetomidine. However, the lack of correlation between TNF-α reduction and AF incidence suggests that other inflammatory mediators or hemodynamic factors may be involved. Future research should clarify whether dexmedetomidine reduces AF risk primarily through autonomic modulation rather than anti-inflammatory mechanisms.
Despite the opioid-sparing effect observed in Group 2, the time to extubation was longest in this group. One potential explanation is that higher doses of dexmedetomidine led to dose-dependent bradycardia and hemodynamic depression, necessitating prolonged postoperative monitoring before extubation. This aligns with prior studies indicating that higher dexmedetomidine doses may prolong sedation in cardiac surgery patients. Additionally, most extubation procedures were delayed due to nursing staff shift changes. As a result, the recorded extubation times may not accurately reflect the patients’ actual clinical readiness for extubation. This procedural factor may have masked any potential dexmedetomidine-related effect on early extubation.
Bradycardia incidence was low across all groups, with no significant differences. TCP was required in only one patient in Group 2, while pacing was more frequent in Groups 0 and 1. These findings suggest that dexmedetomidine did not increase the risk of clinically significant bradycardia within the studied dose range. Alternatively, the need for pacing in Groups 0 and 1 may have been influenced by factors unrelated to dexmedetomidine. While our results do not establish a causal relationship between dexmedetomidine and bradycardia, they underscore the need for careful dose titration in hemodynamically vulnerable patients.
Interestingly, the infection rate was higher in the dexmedetomidine-treated groups, although this difference was not statistically significant. This finding contrasts with prior studies suggesting that dexmedetomidine may enhance immune function. A plausible explanation is that the prolonged CPB duration in Group 2 led to greater endothelial dysfunction and immunosuppression, overshadowing any potential protective effect of dexmedetomidine. Antibiotic use did not correlate with infection rates, as antibiotic administration was often based on the operating surgeon’s clinical judgment rather than microbiological confirmation.
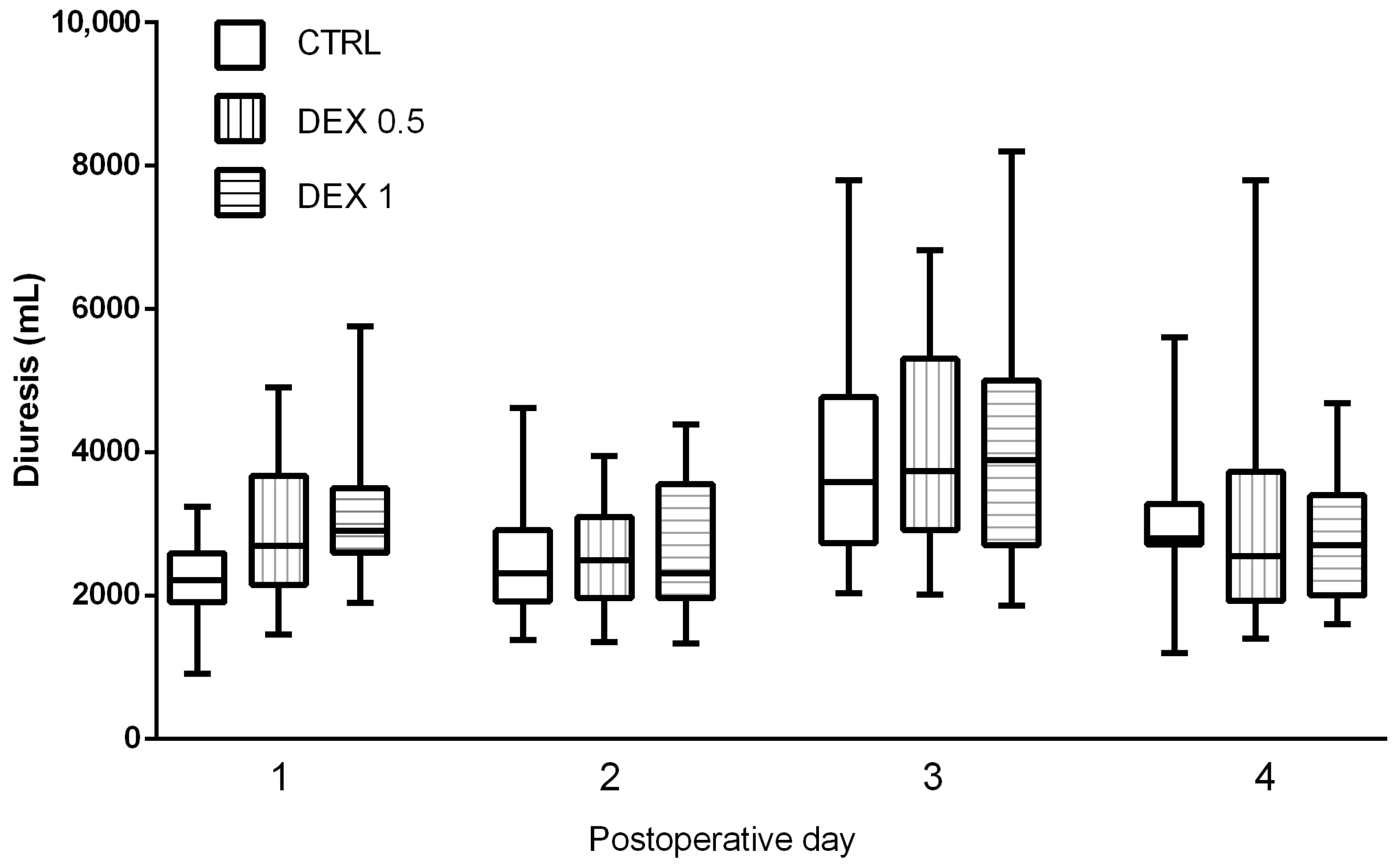
Postoperative renal function assessment indicated that dexmedetomidine had no adverse impact on renal function, as GFR and creatinine levels remained stable across all groups. Notably, diuresis was significantly increased in Groups 1 and 2, particularly on POD1, suggesting that dexmedetomidine may enhance fluid excretion and natriuresis. This observation is consistent with prior research suggesting that dexmedetomidine modulates renal perfusion and sympathetic tone, facilitating urinary excretion without impairing renal function. Despite this increased diuresis, other renal markers, including urea and creatinine, did not differ significantly between groups. This supports the assumption that dexmedetomidine does not contribute to renal dysfunction. Concerns regarding dexmedetomidine-induced hemodynamic instability or reduced renal perfusion due to bradycardia were not substantiated, as no evidence of renal impairment was observed. Future investigations involving larger cohorts and additional renal biomarkers (e.g., neutrophil gelatinase-associated lipocalin [NGAL] or cystatin C) may provide a more comprehensive assessment of dexmedetomidine’s potential nephroprotective effects in CPB patients.
This study has several limitations. The relatively small sample size limited statistical power, particularly for detecting differences in AF incidence and infection rates. Additionally, while dexmedetomidine’s anti-inflammatory effects were partially demonstrated, the results may have been confounded by surgical complexity and perfusion times. Future research should involve larger patient populations and expanded inflammatory marker panels, including IL-10, CRP, and nuclear factor kappa B (NF-κB) pathway analysis, to better elucidate dexmedetomidine’s immunomodulatory properties in cardiac surgery patients.

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}