

Persistent Olfactory and Taste Dysfunction after COVID-19

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Sniffin’ Sticks Test (SST)
2.3. Taste Strips Test (TS)
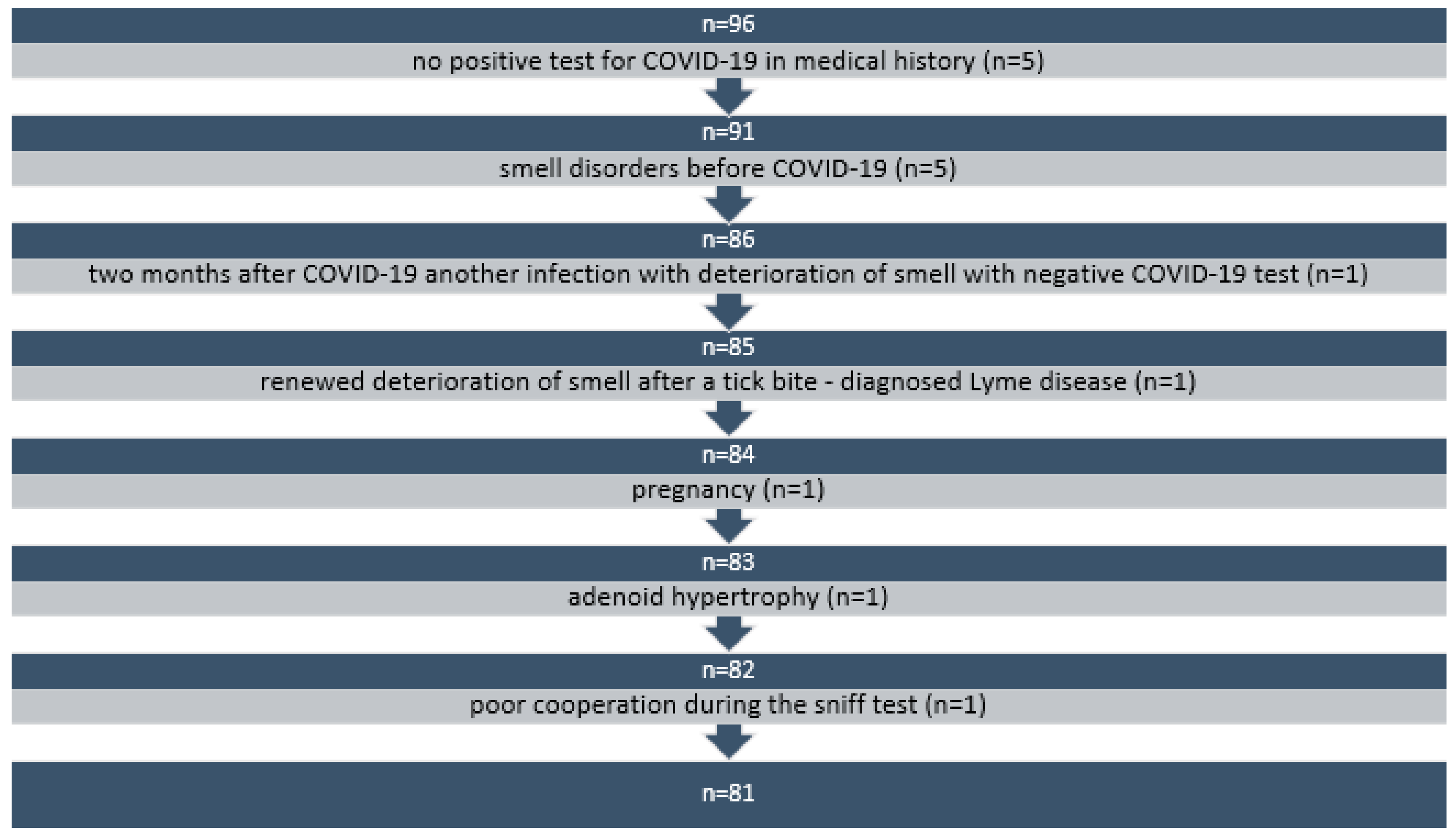
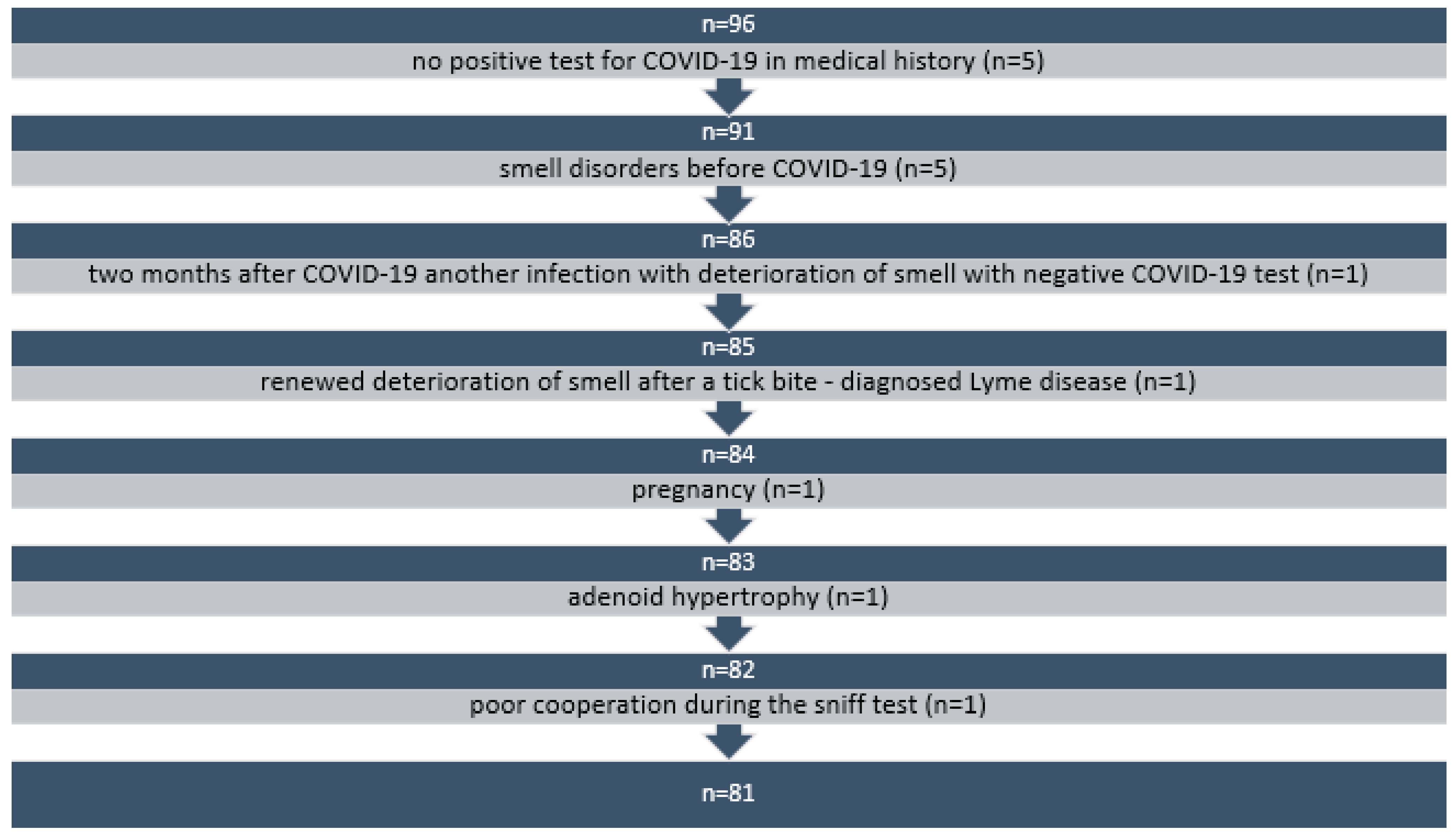
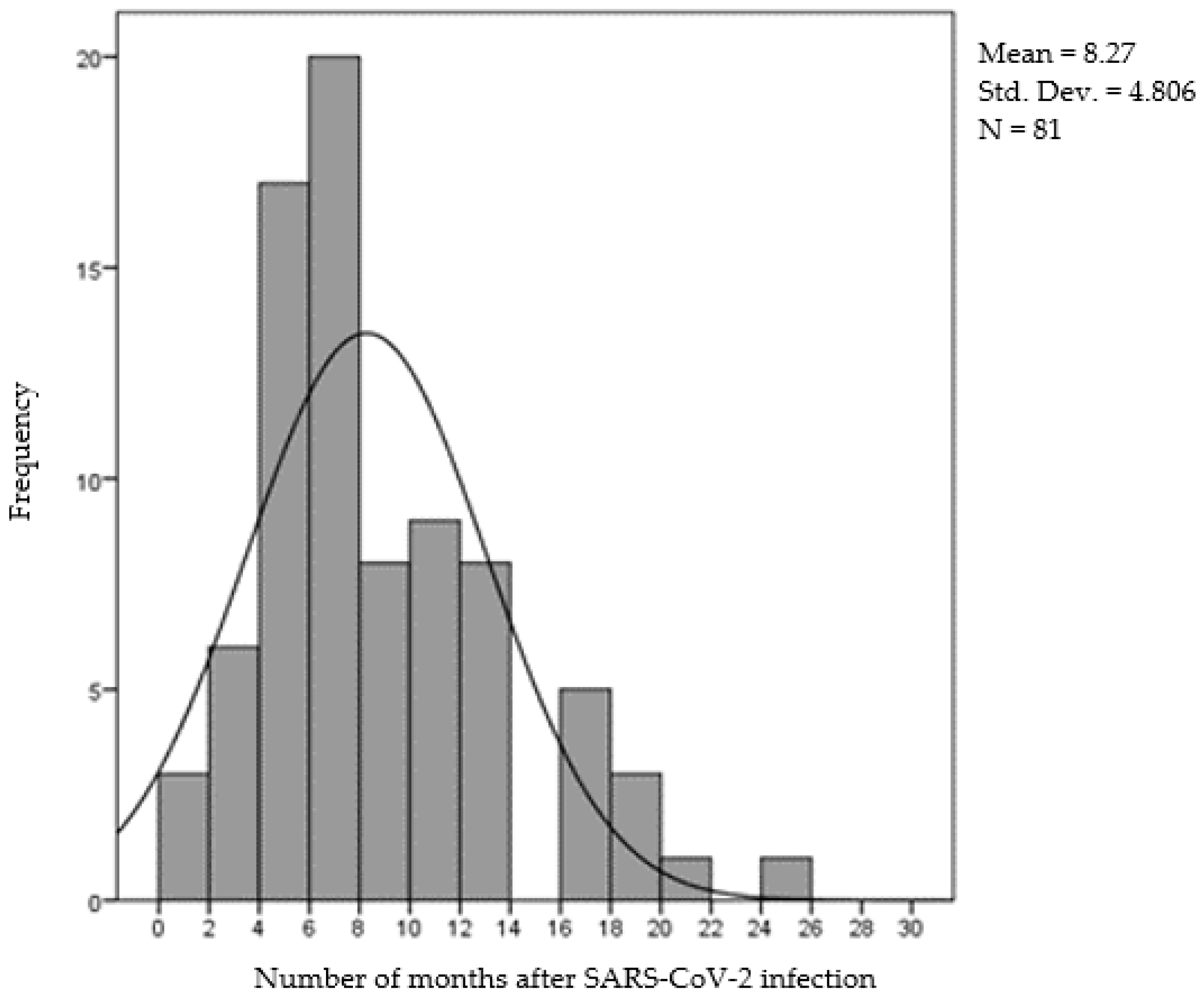
2.4. Subjects
2.5. Inclusion Criteria
2.6. Exclusion Criteria
2.7. Statistical Analysis
3. Results
3.1. Taste
3.2. Relationship between Olfactory and Gustatory Sensitivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cherry, G.; Rocke, J.; Chu, M.; Liu, J.; Lechner, M.; Lund, V.J.; Kumar, B.N. Loss of Smell and Taste: A New Marker of COVID-19? Tracking Reduced Sense of Smell during the Coronavirus Pandemic Using Search Trends. Expert Rev. Anti-Infect. Ther. 2020, 18, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Anosmia—American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS). Available online: https://www.entnet.org/covid-19/anosmia/ (accessed on 23 June 2023).
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and Taste Dysfunction in Patients with COVID-19: A Systematic Review and Meta-Analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Karamali, K.; Elliott, M.; Hopkins, C. COVID-19 Related Olfactory Dysfunction. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Speth, M.M.; Singer-Cornelius, T.; Oberle, M.; Gengler, I.; Brockmeier, S.J.; Sedaghat, A.R. Time Scale for Resolution of Olfactory Dysfunction in COVID-19. Rhinology 2020, 58, 404–405. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Borsetto, D.; Fabbris, C.; Spinato, G.; Frezza, D.; Menegaldo, A.; Mularoni, F.; Gaudioso, P.; Cazzador, D.; Marciani, S.; et al. Evolution of Altered Sense of Smell or Taste in Patients With Mildly Symptomatic COVID-19. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 729–732. [Google Scholar] [CrossRef]
- Torabi, A.; Mohammadbagheri, E.; Akbari Dilmaghani, N.; Bayat, A.-H.; Fathi, M.; Vakili, K.; Alizadeh, R.; Rezaeimirghaed, O.; Hajiesmaeili, M.; Ramezani, M.; et al. Proinflammatory Cytokines in the Olfactory Mucosa Result in COVID-19 Induced Anosmia. ACS Chem. Neurosci. 2020, 11, 1909–1913. [Google Scholar] [CrossRef]
- Fodoulian, L.; Tuberosa, J.; Rossier, D.; Boillat, M.; Kan, C.; Pauli, V.; Egervari, K.; Lobrinus, J.A.; Landis, B.N.; Carleton, A.; et al. SARS-CoV-2 Receptors and Entry Genes Are Expressed in the Human Olfactory Neuroepithelium and Brain. iScience 2020, 23, 101839. [Google Scholar] [CrossRef]
- Kanjanaumporn, J.; Aeumjaturapat, S.; Snidvongs, K.; Seresirikachorn, K.; Chusakul, S. Smell and Taste Dysfunction in Patients with SARS-CoV-2 Infection: A Review of Epidemiology, Pathogenesis, Prognosis, and Treatment Options. Asian Pac. J. Allergy Immunol. 2020, 38, 69–77. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Vaira, L.A.; Salzano, G.; Fois, A.G.; Piombino, P.; De Riu, G. Potential Pathogenesis of Ageusia and Anosmia in COVID-19 Patients. Int. Forum Allergy Rhinol. 2020, 10, 1103–1104. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position Paper on Olfactory Dysfunction. Rhinology 2016, 56, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Nettore, I.C.; Cantone, E.; Palatucci, G.; Franchini, F.; Maturi, R.; Nerilli, M.; Manzillo, E.; Foggia, M.; Maione, L.; Ungaro, P.; et al. Quantitative but Not Qualitative Flavor Recognition Impairments in COVID-19 Patients. Ir. J. Med. Sci. 2022, 191, 1759–1766. [Google Scholar] [CrossRef] [PubMed]
- Arndal, E.; Lebech, A.-M.; Podlekarava, D.; Mortensen, J.; Christensen, J.; Rönsholt, F.F.; Lund, T.K.; Katzenstein, T.L.; von Buchwald, C. Olfactory and Gustatory Outcomes Including Health-Related Quality of Life 3–6 and 12 Months after Severe-to-Critical COVID-19: A SECURe Prospective Cohort Study. J. Clin. Med. 2022, 11, 6025. [Google Scholar] [CrossRef] [PubMed]
- Bochicchio, V.; Mezzalira, S.; Maldonato, N.M.; Cantone, E.; Scandurra, C. Olfactory-Related Quality of Life Impacts Psychological Distress in People with COVID-19: The Affective Implications of Olfactory Dysfunctions. J. Affect. Disord. 2023, 323, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Sekinger, B.; Wolf, S.R.; Pauli, E.; Kobal, G. ‘Sniffin’ Sticks’: Olfactory Performance Assessed by the Combined Testing of Odor Identification, Odor Discrimination and Olfactory Threshold. Chem. Senses 1997, 22, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Sorokowska, A.; Hummel, T. [Polish version of the Sniffin’ Sticks Test—Adaptation and normalization]. Otolaryngol. Pol. 2014, 68, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Kobal, G.; Gudziol, H.; Mackay-Sim, A. Normative Data for the “Sniffin’ Sticks” Including Tests of Odor Identification, Odor Discrimination, and Olfactory Thresholds: An Upgrade Based on a Group of More than 3000 Subjects. Eur. Arch. Otorhinolaryngol. 2007, 264, 237–243. [Google Scholar] [CrossRef]
- Landis, B.N.; Welge-Luessen, A.; Brämerson, A.; Bende, M.; Mueller, C.A.; Nordin, S.; Hummel, T. “Taste Strips”—A Rapid, Lateralized, Gustatory Bedside Identification Test Based on Impregnated Filter Papers. J. Neurol. 2009, 256, 242–248. [Google Scholar] [CrossRef]
- Ciofalo, A.; Filiaci, F.; Romeo, R.; Zambetti, G.; Vestri, A.R. Epidemiological Aspects of Olfactory Dysfunction. Rhinology 2006, 44, 78–82. [Google Scholar]
- Seiden, A.M. Postviral Olfactory Loss. Otolaryngol. Clin. N. Am. 2004, 37, 1159–1166. [Google Scholar] [CrossRef]
- Bordin, A.; Mucignat-Caretta, C.; Gaudioso, P.; Pendolino, A.L.; Leoni, D.; Scarpa, B.; Andrews, P.J.; Cattelan, A.M.; Antonini, A.; Nicolai, P.; et al. Comparison of Self-Reported Symptoms and Psychophysical Tests in Coronavirus Disease 2019 (COVID-19) Subjects Experiencing Long-Term Olfactory Dysfunction: A 6-Month Follow-up Study. Int. Forum Allergy Rhinol. 2021, 11, 1592–1595. [Google Scholar] [CrossRef]
- Iannuzzi, L.; Salzo, A.E.; Angarano, G.; Palmieri, V.O.; Portincasa, P.; Saracino, A.; Gelardi, M.; Dibattista, M.; Quaranta, N. Gaining Back What Is Lost: Recovering the Sense of Smell in Mild to Moderate Patients After COVID-19. Chem. Senses 2020, 45, 875–881. [Google Scholar] [CrossRef]
- Le Bon, S.-D.; Pisarski, N.; Verbeke, J.; Prunier, L.; Cavelier, G.; Thill, M.-P.; Rodriguez, A.; Dequanter, D.; Lechien, J.R.; Le Bon, O.; et al. Psychophysical Evaluation of Chemosensory Functions 5 Weeks after Olfactory Loss Due to COVID-19: A Prospective Cohort Study on 72 Patients. Eur. Arch. Otorhinolaryngol. 2021, 278, 101–108. [Google Scholar] [CrossRef]
- Niklassen, A.S.; Draf, J.; Huart, C.; Hintschich, C.; Bocksberger, S.; Trecca, E.M.C.; Klimek, L.; Le Bon, S.D.; Altundag, A.; Hummel, T. COVID-19: Recovery from Chemosensory Dysfunction. A Multicentre Study on Smell and Taste. Laryngoscope 2021, 131, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Prem, B.; Liu, D.T.; Besser, G.; Sharma, G.; Dultinger, L.E.; Hofer, S.V.; Matiasczyk, M.M.; Renner, B.; Mueller, C.A. Long-Lasting Olfactory Dysfunction in COVID-19 Patients. Eur. Arch. Otorhinolaryngol. 2022, 279, 3485–3492. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and Gustatory Dysfunctions as a Clinical Presentation of Mild-to-Moderate Forms of the Coronavirus Disease (COVID-19): A Multicenter European Study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- Prem, B.; Liu, D.T.; Besser, G.; Renner, B.; Mueller, C.A. Retronasal Olfactory Testing in Early Diagnosed and Suspected COVID-19 Patients: A 7-Week Follow-up Study. Eur. Arch. Otorhinolaryngol. 2022, 279, 257–265. [Google Scholar] [CrossRef]
- Singer-Cornelius, T.; Cornelius, J.; Oberle, M.; Metternich, F.U.; Brockmeier, S.J. Objective Gustatory and Olfactory Dysfunction in COVID-19 Patients: A Prospective Cross-Sectional Study. Eur. Arch. Otorhinolaryngol. 2021, 278, 3325–3332. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Hummel, T.; Hopkins, C.; Dibattista, M.; Menini, A.; Spinato, G.; Fabbris, C.; Emanuelli, E.; D’Alessandro, A.; Marzolino, R.; et al. High Prevalence of Long-Term Olfactory, Gustatory, and Chemesthesis Dysfunction in Post-COVID-19 Patients: A Matched Case-Control Study with One-Year Follow-up Using a Comprehensive Psychophysical Evaluation. Rhinology 2021, 59, 517–527. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Odor Threshold | Odor Discrimination | Odor Identification | Total Score | |
|---|---|---|---|---|
| N | 81 | 81 | 81 | 81 |
| M ± SD | 3.34 ± 4.72 | 9.89 ± 3.10 | 9.12 ± 3.00 | 22.35 ± 7.78 |
| Min | 0.00 | 0.00 | 2.00 | 3.00 |
| Max | 16.00 | 16.00 | 15.00 | 40.00 |
| P10 | 0.00 | 6.00 | 5.00 | 11.20 |
| P25 | 0.00 | 8.00 | 7.00 | 18.00 |
| P50 | 1.00 | 10.00 | 9.00 | 23.00 |
| P75 | 4.00 | 12.00 | 11.00 | 27.00 |
| P90 | 14.50 | 13.00 | 13.00 | 32.00 |
| Task | Correct Answer | Incorrect Answers | No Answer | ||
|---|---|---|---|---|---|
| 1 | Orange, 88.9% | Blackberry, 3.7% | Strawberry, 2.5% | Pineapple, 4.9% | - |
| 2 | Leather, 33.3% | Smoke, 24.7% | Glue, 23.5% | Grass, 13.6% | 4.9% |
| 3 | Cinnamon, 53.1% | Honey, 12.3% | Vanilla. 21% | Chocolate, 7.4% | 6.2% |
| 4 | Mint, 65.4% | Chives, 4.9% | Fir, 23.5% | Onion, 4.9% | 1.2% |
| 5 | Banana, 59.3% | Cocoa, 13.6% | Walnut, 9.9% | Cherry, 13.6% | 3.7% |
| 6 | Lemon, 43.2 | Peach, 3.7% | Apple, 3.7% | Grapefruit, 43.2% | 3.7% |
| 7 | Licorice, 42% | Cherry, 12.3% | Mint, 9.9% | Cookies, 32.1% | 3.7% |
| 8 | Turpentine, 38.3% | Mustard, 4.9% | Gum, 9.9% | Menthol, 44.4% | 2.5% |
| 9 | Garlic, 49.4% | Onion, 28.4% | Sauerkraut, 19.8% | Carrot, 2.5% | - |
| 10 | Coffee, 80.2% | Cigarettes, 8.6% | Wine, 2.5% | Smoke, 6.2% | 2.5% |
| 11 | Apple, 13.6% | Melon, 53.1% | Peach, 21% | Orange, 9.9% | 2.5% |
| 12 | Cloves, 76.5% | Pepper, 4.9% | Cinnamon, 17.3% | Mustard, 1.2% | - |
| 13 | Pineapple, 51.9% | Pear, 21% | Plum, 6.2% | Peach, 17.3% | 3.7% |
| 14 | Rose, 70.4% | Chamomile, 14.8% | Raspberry, 3.7% | Cherry, 6.2% | 4.9% |
| 15 | Aniseed, 56.8% | Rum, 9.9% | Honey, 9.9% | Fir, 18.5% | 4.9% |
| 16 | Fish, 86.4% | Bread, 6.2% | Cheese, 2.5% | Ham, 3.7% | 1.2% |
| Correct | Incorrect | |
|---|---|---|
| Sweet | 78 (96.3%) | 3 (3.7%) |
| Salty | 68 (84%) | 13 (16%) |
| Sour | 72 (88.9%) | 9 (11.1%) |
| Bitter | 70 (86.4%) | 11 (13.6%) |
| Sweet | Salty | Sour | Bitter | |
|---|---|---|---|---|
| Anosmia (n = 18) | 100% | 83.3% | 88.9% | 77.8% |
| Hyposmia (n = 52) | 94.2% | 80.8% | 88.5% | 86.5% |
| Normosmia (n = 11) | 100% | 84.0% | 90.9% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buksinska, M.; Skarzynski, P.H.; Raj-Koziak, D.; Gos, E.; Talarek, M. Persistent Olfactory and Taste Dysfunction after COVID-19. Life 2024, 14, 317. https://doi.org/10.3390/life14030317
Buksinska M, Skarzynski PH, Raj-Koziak D, Gos E, Talarek M. Persistent Olfactory and Taste Dysfunction after COVID-19. Life. 2024; 14(3):317. https://doi.org/10.3390/life14030317
Chicago/Turabian StyleBuksinska, Malgorzata, Piotr Henryk Skarzynski, Danuta Raj-Koziak, Elzbieta Gos, and Malgorzata Talarek. 2024. "Persistent Olfactory and Taste Dysfunction after COVID-19" Life 14, no. 3: 317. https://doi.org/10.3390/life14030317
APA StyleBuksinska, M., Skarzynski, P. H., Raj-Koziak, D., Gos, E., & Talarek, M. (2024). Persistent Olfactory and Taste Dysfunction after COVID-19. Life, 14(3), 317. https://doi.org/10.3390/life14030317