

Evaluation of Reporting Quality of Glaucoma Randomized Controlled Trial Abstracts: Current Status and Future Perspectives

 ,
,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
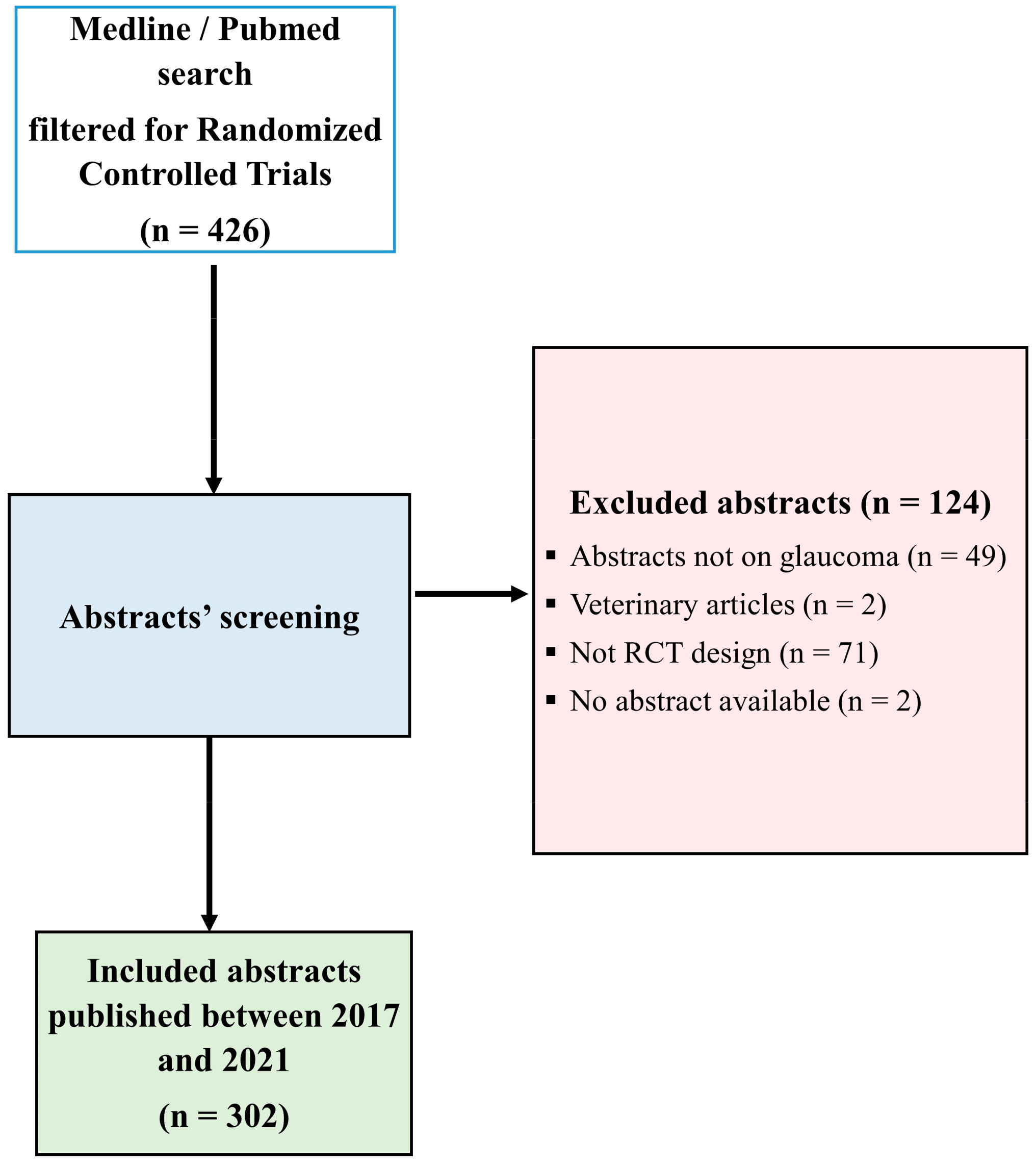
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Basavarajappa, D.; Galindo-Romero, C.; Gupta, V.; Agudo-Barriuso, M.; Gupta, V.B.; Graham, S.L.; Chitranshi, N. Signalling pathways and cell death mechanisms in glaucoma: Insights into the molecular pathophysiology. Mol. Aspects Med. 2023, 94, 101216. [Google Scholar] [CrossRef]
- Shih, V.; Parekh, M.; Multani, J.K.; McGuiness, C.B.; Chen, C.C.; Campbell, J.H.; Miller-Ellis, E.; Olivier, M.M.G. Clinical and Economic Burden of Glaucoma by Disease Severity: A United States Claims-Based Analysis. Ophthalmol. Glaucoma 2021, 4, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Mahabadi, N.; Foris, L.A.; Tripathy, K. Open Angle Glaucoma; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- De Bernardo, M.; Casaburi, C.; De Pascale, I.; Capasso, L.; Cione, F.; Rosa, N. Comparison between dynamic contour tonometry and Goldmann applanation tonometry correcting equations. Sci. Rep. 2022, 12, 20190. [Google Scholar] [CrossRef]
- Markiewitz, H.H. The so-called Imbert-Fick law. Arch. Ophthalmol. 1960, 64, 159. [Google Scholar] [CrossRef] [PubMed]
- Albis-Donado, O.; Ramirez-Neria, P.; Rios-Acosta, N.; Stalmans, I. The influence of altitude on the differences between Goldmann tonometry and Pascal dynamic contour tonometry: An ecological meta-analysis. Indian J. Ophthalmol. 2023. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, M.; Abbinante, G.; Borrelli, M.; Di Stasi, M.; Cione, F.; Rosa, N. Intraocular Pressure Measurements in Standing, Sitting, and Supine Position: Comparison between Tono-Pen Avia and Icare Pro Tonometers. J. Clin. Med. 2022, 11, 6234. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, X.X.; Hou, X.W.; Pan, C.W. Risk Factors for Primary Angle-closure Glaucoma: A Systematic Review and Meta-Analysis of 45 Studies. Optom. Vis. Sci. 2023, 100, 606–613. [Google Scholar] [CrossRef]
- Stein, J.D.; Khawaja, A.P.; Weizer, J.S. Glaucoma in Adults-Screening, Diagnosis, and Management: A Review. JAMA 2021, 325, 164–174. [Google Scholar] [CrossRef]
- Sun, J.; Li, T.; Zhao, X.; Lu, B.; Chen, J.; Liu, W.; Zhou, M.; Sun, X. Prevalence and Risk Factors of Glaucoma among Chinese People from the China Health and Retirement Longitudinal Study. J. Glaucoma 2022, 31, 789–795. [Google Scholar] [CrossRef]
- Lee, J.H.; Kwon, Y.J.; Lee, H.S.; Han, J.H.; Joung, B.; Kim, S.J. Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure. Nutrients 2022, 14, 4455. [Google Scholar] [CrossRef]
- Sun, C.; Yang, H.; Hu, Y.; Qu, Y.; Hu, Y.; Sun, Y.; Ying, Z.; Song, H. Association of sleep behaviour and pattern with the risk of glaucoma: A prospective cohort study in the UK Biobank. BMJ Open 2022, 12, e063676. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, M.; Hans, T.; Sandhu, P.S.; Midha, N. Evaluation of Vision-related Quality of Life in Patients with Glaucoma: A Hospital-based Study. J. Curr. Glaucoma Pract. 2019, 13, 9–15. [Google Scholar] [CrossRef]
- Aspberg, J.; Heijl, A.; Bengtsson, B. Screening for Open-Angle Glaucoma and Its Effect on Blindness. Am. J. Ophthalmol. 2021, 228, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Rauscher, F.G.; Li, Y.; Eslami, M.; Kazeminasab, S.; Zebardast, N.; Wang, M.; Elze, T. Normative Percentiles of Retinal Nerve Fiber Layer Thickness and Glaucomatous Visual Field Loss. Transl. Vis. Sci. Technol. 2023, 12, 13. [Google Scholar] [CrossRef]
- Buonfiglio, F.; Pfeiffer, N.; Gericke, A. Immunomodulatory and Antioxidant Drugs in Glaucoma Treatment. Pharmaceuticals 2023, 16, 1193. [Google Scholar] [CrossRef]
- Kang, J.M.; Tanna, A.P. Glaucoma. Med. Clin. N. Am. 2021, 105, 493–510. [Google Scholar] [CrossRef] [PubMed]
- Wagner, I.V.; Stewart, M.W.; Dorairaj, S.K. Updates on the Diagnosis and Management of Glaucoma. Mayo Clin. Proc. Innov. Qual. Outcomes 2022, 6, 618–635. [Google Scholar] [CrossRef]
- Boudry, C.; Denion, E.; Mortemousque, B.; Mouriaux, F. Trends and topics in eye disease research in PubMed from 2010 to 2014. PeerJ 2016, 4, e1557. [Google Scholar] [CrossRef]
- Mohan, N.; Chakrabarti, A.; Nazm, N.; Mehta, R.; Edward, D.P. Newer advances in medical management of glaucoma. Indian J. Ophthalmol. 2022, 70, 1920–1930. [Google Scholar] [CrossRef]
- Speich, B.; Schroter, S.; Briel, M.; Moher, D.; Puebla, I.; Clark, A.; Schlüssel, M.M.; Ravaud, P.; Boutron, I.; Hopewell, S. Impact of a short version of the CONSORT checklist for peer reviewers to improve the reporting of randomised controlled trials published in biomedical journals: Study protocol for a randomised controlled trial. BMJ Open 2020, 10, e035114. [Google Scholar] [CrossRef]
- Imran, M.; Kwakkenbos, L.; McCall, S.J.; McCord, K.A.; Fröbert, O.; Hemkens, L.G.; Zwarenstein, M.; Relton, C.; Rice, D.B.; Langan, S.M.; et al. Methods and results used in the development of a consensus-driven extension to the Consolidated Standards of Reporting Trials (CONSORT) statement for trials conducted using cohorts and routinely collected data (CONSORT-ROUTINE). BMJ Open 2021, 11, e049093. [Google Scholar] [CrossRef]
- Hopewell, S.; Clarke, M.; Moher, D.; Wager, E.; Middleton, P.; Altman, D.G.; Schulz, K.F.; The CONSORT Group. CONSORT for reporting randomized controlled trials in journal and conference abstracts: Explanation and elaboration. PLoS Med. 2008, 5, e20. [Google Scholar] [CrossRef]
- Song, S.Y.; Kim, B.; Kim, I.; Kim, S.; Kwon, M.; Han, C.; Kim, E. Assessing reporting quality of randomized controlled trial abstracts in psychiatry: Adherence to CONSORT for abstracts: A systematic review. PLoS ONE 2017, 12, e0187807. [Google Scholar] [CrossRef] [PubMed]
- Janackovic, K.; Puljak, L. Reporting quality of randomized controlled trial abstracts in the seven highest-ranking anesthesiology journals. Trials 2018, 19, 591. [Google Scholar] [CrossRef] [PubMed]
- Baulig, C.; Krummenauer, F.; Geis, B.; Tulka, S.; Knippschild, S. Reporting quality of randomised controlled trial abstracts on age-related macular degeneration health care: A cross-sectional quantification of the adherence to CONSORT abstract reporting recommendations. BMJ Open 2018, 8, e021912. [Google Scholar] [CrossRef] [PubMed]
- Vrebalov Cindro, P.; Bukic, J.; Pranic, S.; Leskur, D.; Rusic, D.; Seselja Perisin, A.; Bozic, J.; Vukovic, J.; Modun, D. Did an introduction of CONSORT for abstracts guidelines improve reporting quality of randomised controlled trials’ abstracts on Helicobacter pylori infection? Observational study. BMJ Open 2022, 12, e054978. [Google Scholar] [CrossRef]
- Xie, L.; Qin, W.; Gu, Y.; Pathak, J.; Zeng, S.; Du, M. Quality assessment of randomized controlled trial Abstracts on drug therapy of periodontal disease from the Abstracts published in dental science citation indexed journals in the last ten years. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e626–e633. [Google Scholar] [CrossRef]
- Lundh, A.; Lexchin, J.; Mintzes, B.; Schroll, J.B.; Bero, L. Industry sponsorship and research outcome. Cochrane Database Syst. Rev. 2017, 2, MR000033. [Google Scholar] [CrossRef]
- Fundytus, A.; Wells, J.C.; Sharma, S.; Hopman, W.; Del Paggio, J.; Gyawali, B.; Mukherji, D.; Hammad, N.; Pramesh, C.; Aggarwal, A.; et al. Industry Funding of Oncology Randomised Controlled Trials: Implications for Design, Results and Interpretation. Clin. Oncol. 2022, 34, 28–35. [Google Scholar] [CrossRef]
- Wiehn, J.; Nonte, J.; Prugger, C. Reporting quality for abstracts of randomised trials on child and adolescent depression prevention: A meta-epidemiological study on adherence to CONSORT for abstracts. BMJ Open 2022, 12, e061873. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, F.; Gufran, K.; Ahmed, M.M.; Alsakr, A.; Almutairi, A. Quality of Reporting Randomized Controlled Trials Published in Three of the Most Citable Periodontal Journals from 2018 to 2022. Healthcare 2023, 11, 3180. [Google Scholar] [CrossRef] [PubMed]
- Marin, A.I.; Silva, H.N.D.; Chen, H.; Mehta, N.; Nguyen, L.K.; SooHoo, J.R.; Adams, J.E.; Singh, J.K. A Third-Year Medical School Ophthalmology Curriculum for a Longitudinal Integrated Clerkship Model. J. Acad. Ophthalmol. 2022, 14, e209–e215. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.A.; Fisher, A.C.; Pershing, S. Analysis of the Readability and Accountability of Online Patient Education Materials Related to Glaucoma Diagnosis and Treatment. Clin. Ophthalmol. 2023, 17, 779–788. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | N | % |
|---|---|---|
| Type of intervention | ||
| Non-pharmacological | 170 | 56.3 |
| Pharmacological | 132 | 43.7 |
| Study centers | ||
| Single center | 243 | 80.5 |
| Multicenter | 59 | 19.5 |
| Significance of results | ||
| Non-significant | 108 | 35.8 |
| Significant | 194 | 64.2 |
| Number of participants | ||
| <100 | 170 | 56.3 |
| ≥100 | 132 | 43.7 |
| Funding | ||
| Non-industry | 292 | 96.7 |
| Industry | 10 | 3.3 |
| Setting | ||
| Non-hospital | 159 | 52.6 |
| Hospital | 143 | 47.4 |
| Abstract structure | ||
| Unstructured abstract | 15 | 5.0 |
| Structured abstract | 287 | 95.0 |
| Quartiles | ||
| Non-ranked | 38 | 12.6 |
| 1st | 91 | 30.1 |
| 2nd | 72 | 23.8 |
| 3rd | 79 | 26.2 |
| 4th | 22 | 7.3 |
| Mean (SD) | Median (IQR) | |
| Number of authors | 6.54 (3.41) | 6.00 (4.00–8.00) |
| Impact factor | 5.73 (17.42) | 2.97 (2.02–5.49) |
| Item | Kappa Point | Kappa > 0.60 |
|---|---|---|
| Title | 0.888 | * |
| Authors | 0.953 | * |
| Trial design | 0.791 | * |
| Methods | ||
| Participants | 0.958 | * |
| Interventions | 0.607 | * |
| Objective | 0.722 | * |
| Outcome | 0.864 | * |
| Randomization | 0.607 | * |
| Blinding | 0.684 | * |
| Results | ||
| Numbers randomized | 0.637 | * |
| Recruitment | 0.954 | * |
| Numbers analyzed | 0.969 | * |
| Outcome | 0.737 | * |
| Harms | 0.639 | * |
| Conclusions | 0.607 | * |
| Trial registration | 0.895 | * |
| Funding | 0.830 | * |
| Items | N | % |
|---|---|---|
| Title | 118 | 39.1 |
| Authors | 136 | 45.0 |
| Trial design | 62 | 20.5 |
| Methods | ||
| Participants | 186 | 61.6 |
| Interventions | 294 | 97.4 |
| Objective | 296 | 98.0 |
| Outcome | 222 | 73.5 |
| Randomization | 18 | 6.0 |
| Blinding | 56 | 18.5 |
| Results | ||
| Numbers randomized | 224 | 74.2 |
| Recruitment | 143 | 47.4 |
| Numbers analyzed | 61 | 20.2 |
| Outcome | 236 | 78.1 |
| Harms | 87 | 28.8 |
| Conclusions | 295 | 97.7 |
| Trial registration | 50 | 16.6 |
| Funding | 18 | 6.0 |
| Score | Score (%) | |
|---|---|---|
| Mean | 8.28 | 48.32 |
| SD | 2.34 | 13.61 |
| 95% CI | 8.02–8.55 | 46.77–49.86 |
| Median | 8.00 | 47.00 |
| IQR | 7.00–10.00 | 41.00–58.00 |
| Characteristics | Mean Score (%) | 95% CI |
|---|---|---|
| Type of intervention | ||
| Non-pharmacological | 46.45 | 44.44–48.45 |
| Pharmacological | 50.72 | 48.35–53.09 |
| Study centers | ||
| Single center | 46.12 | 44.59–47.66 |
| Multicenter | 57.34 | 53.29–61.39 |
| Significance of results | ||
| Non-significant | 44.60 | 42.00–47.20 |
| Significant | 50.38 | 48.51–52.25 |
| Number of participants | ||
| <100 | 45.12 | 43.29–46.95 |
| ≥100 | 52.42 | 49.95–54.90 |
| Funding | ||
| Non-industry | 47.59 | 46.10–49.07 |
| Industry | 69.60 | 56.94–82.26 |
| Number of authors | ||
| <5 | 44.63 | 41.90–47.36 |
| 5–7 | 45.10 | 42.85–47.35 |
| >7 | 51.40 | 48.21–54.59 |
| Collaboration | 57.38 | 52.82–61.93 |
| Setting | ||
| Non-hospital | 47.79 | 45.56–50.01 |
| Hospital | 48.90 | 46.77–51.04 |
| Abstract structure | ||
| Unstructured abstract | 34.53 | 22.54–46.53 |
| Structured abstract | 49.04 | 47.56–50.52 |
| Impact factor | ||
| <2.200 | 42.69 | 40.13–45.24 |
| 2.201–4 | 44.51 | 42.60–46.41 |
| >4 | 56.60 | 53.96–59.23 |
| Quartiles | ||
| Non-ranked | 39.00 | 35.21–42.79 |
| 1st | 55.28 | 52.60–57.95 |
| 2nd | 50.06 | 46.33–53.74 |
| 3rd | 44.46 | 42.29–46.62 |
| 4th | 43.77 | 39.76–47.79 |
| Characteristics | Univariate Analysis, Estimate 95% CI | Multivariate Analysis, Estimate 95% CI |
|---|---|---|
| Type of intervention | ||
| Non-pharmacological | Reference | Reference |
| Pharmacological | 4.273 (1.198–7.347) ** | 2.406 (−0.170–4.982) |
| Study centers | ||
| Single center | Reference | Reference |
| Multicenter | 11.216 (7.536–14.895) *** | 4.367 (0.822–7.911) * |
| Significance of results | ||
| Non-significant | Reference | Reference |
| Significant | 5.780 (2.626–8.933) *** | 2.946 (0.335–5.557) * |
| Number of participants | ||
| <100 | Reference | Reference |
| ≥100 | 7.301 (4.300–10.301) *** | 2.424 (−0.304–5.152) |
| Funding | ||
| Non-industry | Reference | Reference |
| Industry | 22.014 (13.756–30.273) *** | 12.341 (4.775–19.907) ** |
| Number of authors | ||
| <5 | Reference | Reference |
| 5–7 | 0.466 (−3.347–4.279) | 0.686 (−2.597–3.968) |
| >7 | 6.770 (2.767–10.772) ** | 2.358 (−1.152–5.869) |
| Collaboration | 12.742 (7.816–17.669) *** | 3.339 (−1.570–8.248) |
| Setting | ||
| Non-hospital | Reference | |
| Hospital | 1.116 (−1.974–4.206) | |
| Abstract structure | ||
| Unstructured abstract | Reference | Reference |
| Structured abstract | 14.502 (7.588–21.415) *** | 14.784 (8.867–20.700) *** |
| Impact factor | ||
| <2.200 | Reference | Reference |
| 2.201–4 | 1.820 (−1.617–5.257) | −4.277 (−8.521- (−0.032)) * |
| >4 | 13.912 (10.535–17.288) *** | 11.327 (4.396–18.259) ** |
| Quartiles | ||
| Non-ranked | Reference | Reference |
| 1st | 16.275 (11.533–21.016) *** | −0.701 (−8.894–7.491) |
| 2nd | 11.056 (6.133–15.978) *** | 8.299 (2.820–13.778) ** |
| 3rd | 5.456 (0.609–10.302) * | 6.943 (1.464–12.423) * |
| 4th | 4.773 (−1.804–11.350) | 2.820 (−2.933–8.572) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vucinovic, A.; Bukic, J.; Rusic, D.; Leskur, D.; Seselja Perisin, A.; Radic, M.; Grahovac, M.; Modun, D. Evaluation of Reporting Quality of Glaucoma Randomized Controlled Trial Abstracts: Current Status and Future Perspectives. Life 2024, 14, 117. https://doi.org/10.3390/life14010117
Vucinovic A, Bukic J, Rusic D, Leskur D, Seselja Perisin A, Radic M, Grahovac M, Modun D. Evaluation of Reporting Quality of Glaucoma Randomized Controlled Trial Abstracts: Current Status and Future Perspectives. Life. 2024; 14(1):117. https://doi.org/10.3390/life14010117
Chicago/Turabian StyleVucinovic, Ana, Josipa Bukic, Doris Rusic, Dario Leskur, Ana Seselja Perisin, Marijana Radic, Marko Grahovac, and Darko Modun. 2024. "Evaluation of Reporting Quality of Glaucoma Randomized Controlled Trial Abstracts: Current Status and Future Perspectives" Life 14, no. 1: 117. https://doi.org/10.3390/life14010117
APA StyleVucinovic, A., Bukic, J., Rusic, D., Leskur, D., Seselja Perisin, A., Radic, M., Grahovac, M., & Modun, D. (2024). Evaluation of Reporting Quality of Glaucoma Randomized Controlled Trial Abstracts: Current Status and Future Perspectives. Life, 14(1), 117. https://doi.org/10.3390/life14010117