
Correlation between Psychosomatic Assessment, Heart Rate Variability, and Refractory GERD: A Prospective Study in Patients with Acid Reflux Esophagitis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Ethical Requirements
2.2. Study Cohort, Inclusion and Exclusion Criteria
2.3. Acquisition and Analysis of Heart Rate Variability Data
2.4. Acid Reflux Symptoms Assessments
2.5. Psychosomatic Assessments
2.6. Characteristics of the Study Populations
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics between the GERD and Control Groups
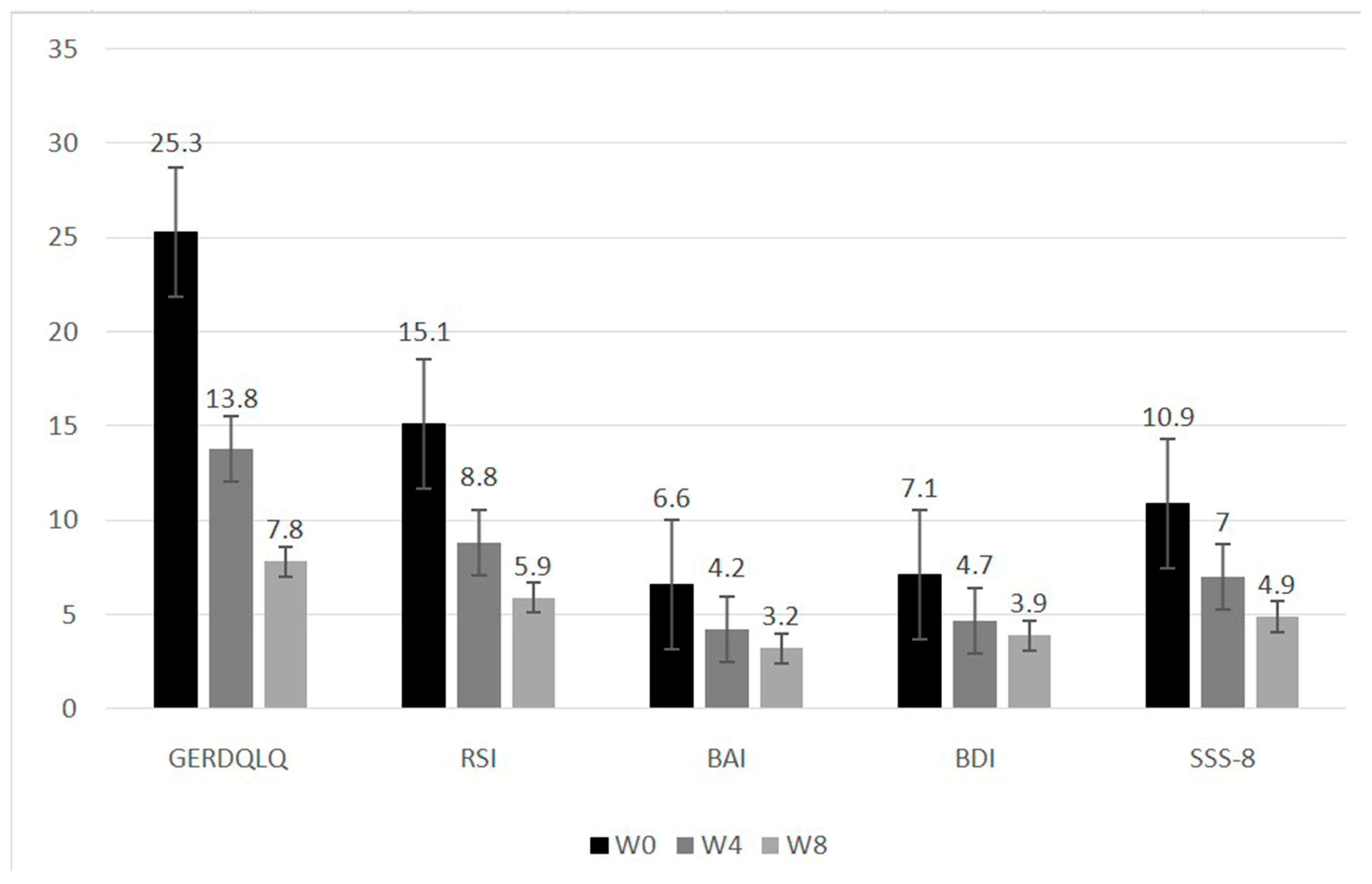
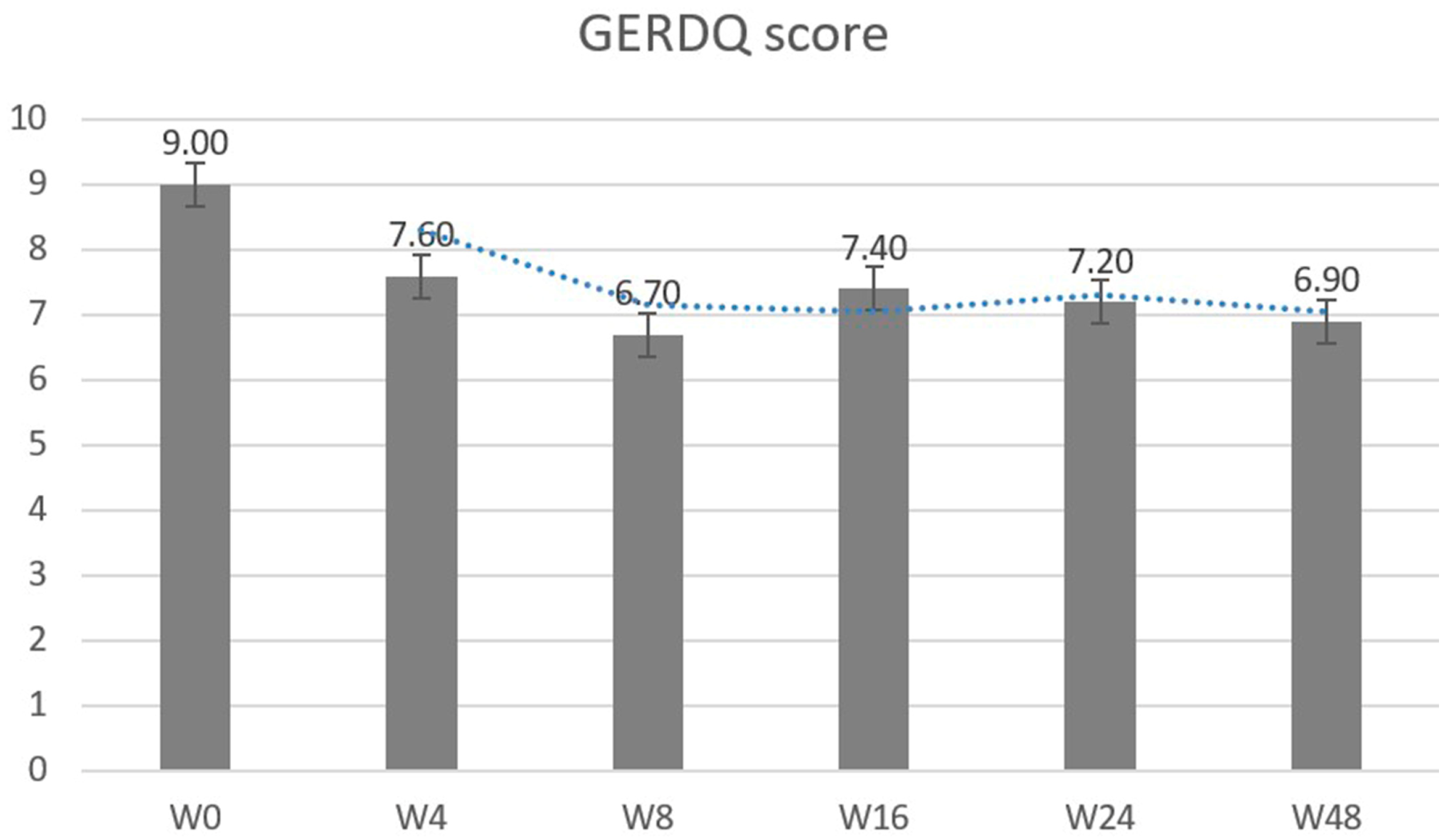
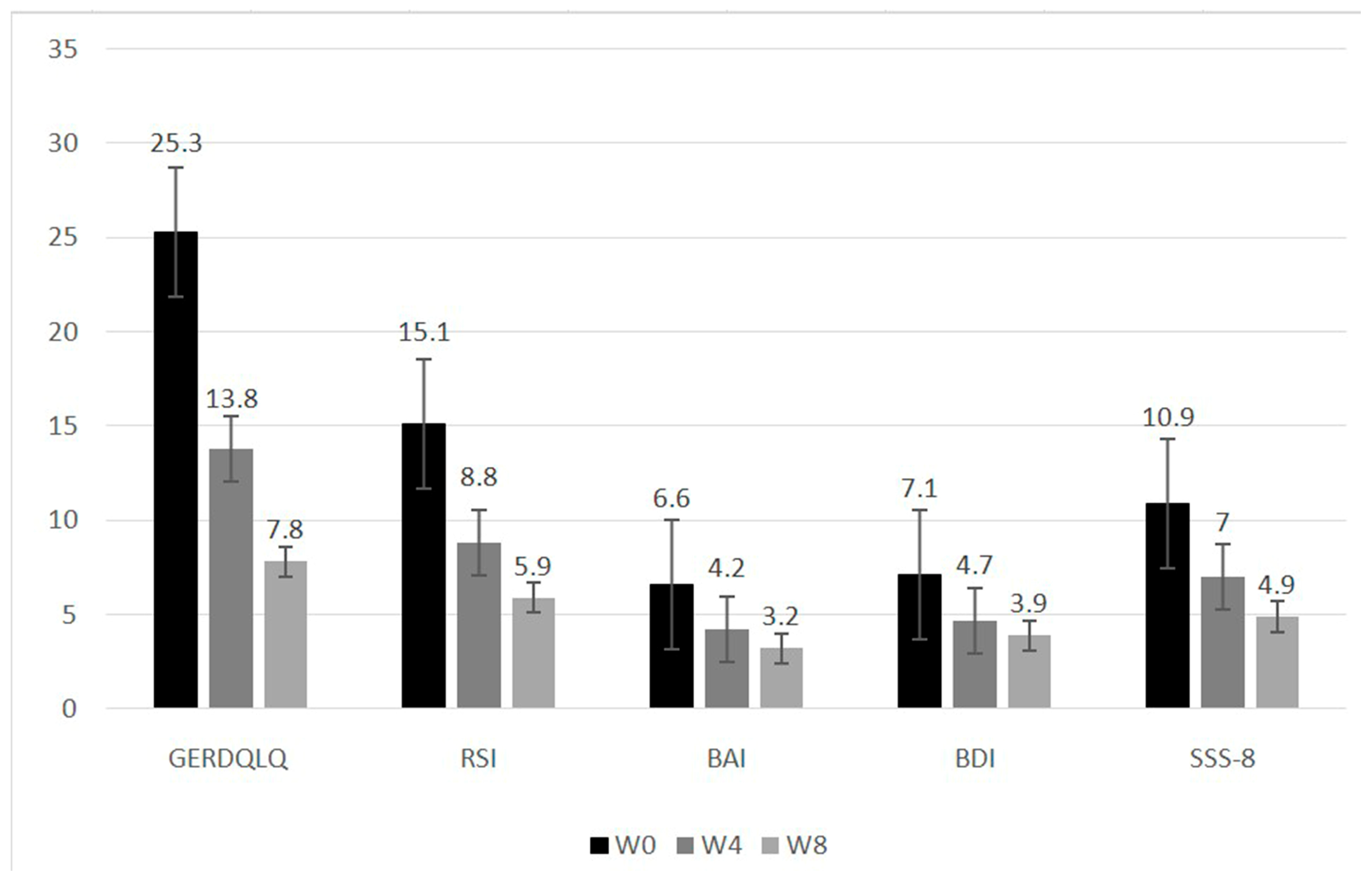
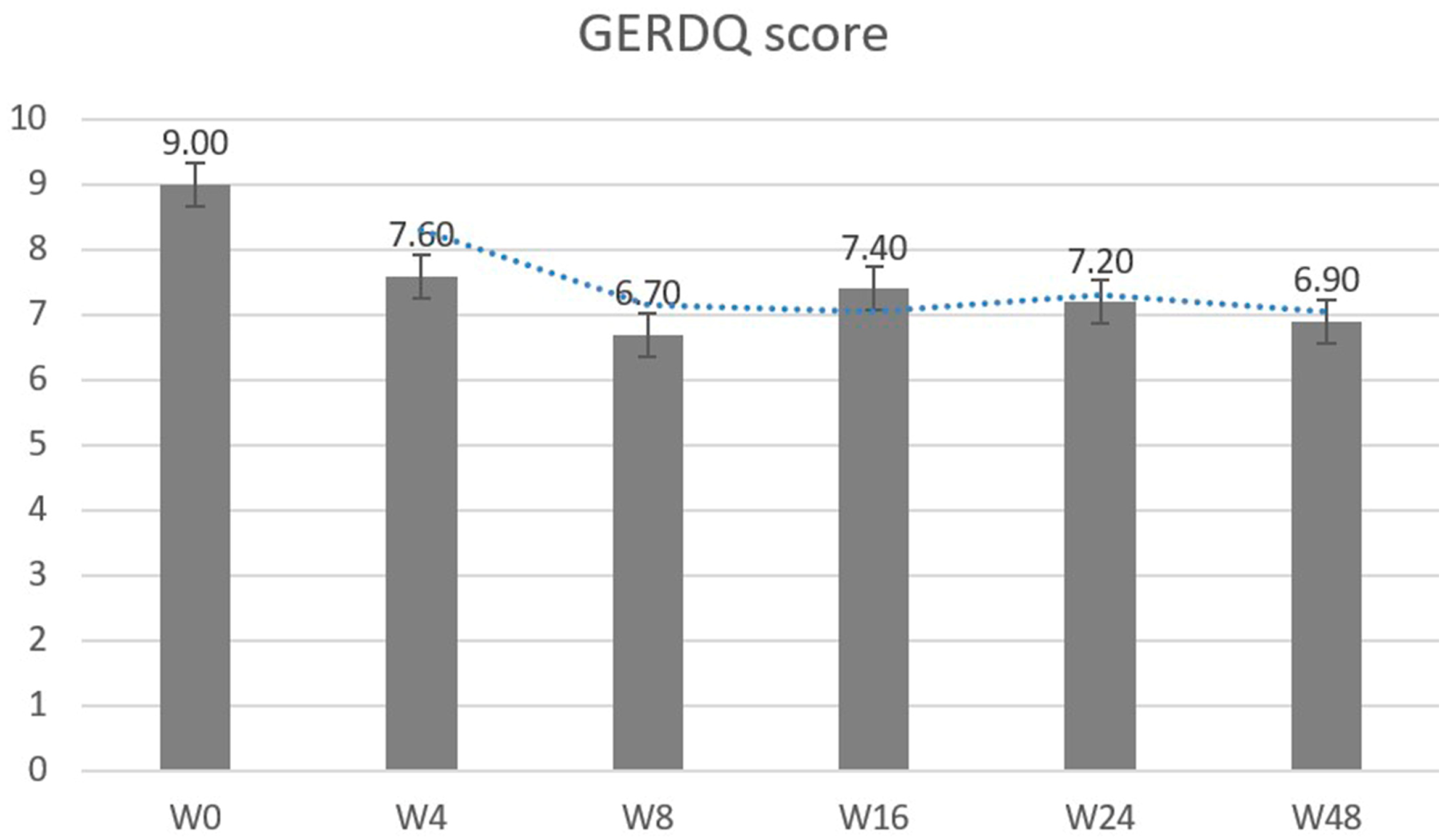
3.2. Sequential Change of Reflux Symptom Score and Psychosomatic Assessments after Treatment
3.3. Correlations between GERD Symptoms and Psychological Scores
3.4. Heart Rate Variability Parameters for the Control and the GERD Groups
3.5. Predictive Variables for Refractory GERD in Patients with Erosive Esophagitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vakil, N.; Van Zanten, S.V.; Kahrilas, P.; Dent, J.; Jones, R.; Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus. Am. J. Gastroenterol. 2006, 101, 1900–1920. [Google Scholar] [CrossRef]
- Lien, H.C.; Chang, C.S.; Yeh, H.Z.; Ko, C.W.; Chang, H.Y.; Cheng, K.F.; Sung, F.C. Increasing prevalence of erosive esophagitis among Taiwanese aged 40 years and above: A comparison between two time periods. J. Clin. Gastroenterol. 2009, 43, 926–932. [Google Scholar] [CrossRef]
- Kim, J.I.; Kim, S.G.; Kim, N.; Kim, J.G.; Shin, S.J.; Kim, H.S.; Sung, J.K.; Yang, C.H.; Shim, K.-N.; Park, S.J.; et al. Changing prevalence of upper gastrointestinal disease in 28,893 Koreans from 1995 to 2005. Eur. J. Gastroenterol. Hepatol. 2009, 21, 787–793. [Google Scholar] [CrossRef]
- Jansson, C.; Nordenstedt, H.; Wallander, M.-A.; Johansson, S.; Johnsen, R.; Hveem, K.; Lagergren, J. Severe gastro-oesophageal reflux symptoms in relation to anxiety, depression and coping in a population-based study. Aliment. Pharmacol. Ther. 2007, 26, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.T.; Gunning, J.; A Lewis, S. Health care seeking by heartburn sufferers is associated with psychosocial factors. Am. J. Gastroenterol. 1996, 91, 2500–2504. [Google Scholar] [PubMed]
- Prasad, M.; Rentz, A.M.; Revicki, D.A. The impact of treatment for gastro-oesophageal reflux disease on health-related quality of life: A literature review. Pharmacoeconomics 2003, 21, 769–790. [Google Scholar] [CrossRef]
- McDougall, N.I.; Johnston, B.T.; Collins, J.S.; McFarland, J.R.; Love, G.A. Disease progression in gastro-oesophageal reflux disease as determined by repeat oesophageal pH monitoring and endoscopy 3 to 4.5 years after diagnosis. Eur. J. Gastroenterol. Hepatol. 1997, 9, 1161–1167. [Google Scholar] [PubMed]
- Patel, A.; Sayuk, G.S.; Gyawali, C.P. Prevalence, characteristics, and treatment outcomes of reflux hypersensitivity detected on pH-impedance monitoring. Neurogastroenterol. Motil. 2016, 28, 1382–1390. [Google Scholar] [CrossRef] [PubMed]
- Roman, S.; Keefer, L.; Imam, H.; Korrapati, P.; Mogni, B.; Eident, K.; Friesen, L.; Kahrilas, P.J.; Martinovich, Z.; Pandolfino, J. Majority of symptoms in esophageal reflux PPI non-responders are not related to reflux. Neurogastroenterol. Motil. 2015, 27, 1667–1674. [Google Scholar] [CrossRef]
- Barlow, W.J.; Orlando, R.C. The pathogenesis of heartburn in nonerosive reflux disease: A unifying hypothesis. Gastroenterology 2005, 128, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Fullard, M.; Kang, J.Y.; Neild, P.; Poullis, A.; Maxwell, J.D. Systematic review: Does gastro-oesophageal reflux disease progress? Aliment. Pharmacol. Ther. 2006, 24, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Milovanovic, B.; Filipovic, B.; Mutavdzin, S.; Zdravkovic, M.; Gligorijevic, T.; Paunovic, J.; Arsic, M. Cardiac autonomic dysfunction in patients with gastroesophageal reflux disease. World J. Gastroenterol. 2015, 21, 6982–6989. [Google Scholar] [CrossRef] [PubMed]
- Kircanski, K.; Williams, L.M.; Gotlib, I.H. Heart rate variability as a biomarker of anxious depression response to antidepressant medication. Depress. Anxiety 2019, 36, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Sifrim, D.; Zerbib, F. Diagnosis and management of patients with reflux symptoms refractory to proton pump inhibitors. Gut 2012, 61, 1340–1354. [Google Scholar] [CrossRef] [PubMed]
- Hershcovici, T.; Jha, L.K.; Cui, H.; Powers, J.; Fass, R. Night-time intra-oesophageal bile and acid: A comparison between gastro-oesophageal reflux disease patients who failed and those who were treated successfully with a proton pump inhibitor. Aliment. Pharmacol. Ther. 2011, 33, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Kahrilas, P.J.; Shaheen, N.J.; Vaezi, M.F. American Gastroenterological Association Medical Position Statement on the management of gastroesophageal reflux disease. Gastroenterology 2008, 135, 1383–1391. [Google Scholar] [CrossRef]
- Wong, W.M.; Lai, K.C.; Lam, K.F.; Hui, W.M.; Hu, W.H.C.; Lam, C.L.K.; Wong, B.C.Y. Prevalence, clinical spectrum and health care utilization of gastro-oesophageal reflux disease in a Chinese population: A population-based study. Aliment. Pharmacol. Ther. 2003, 18, 595–604. [Google Scholar] [CrossRef]
- Chiang, H.H.; Wu, D.C.; Hsu, P.I.; Kuo, C.H.; Tai, W.C.; Yang, S.C. Taiwan Acid-Related Disease Study Group. Clinical efficacy of 60-mg dexlansoprazole and 40-mg esomeprazole after 24 weeks for the on-demand treatment of gastroesophageal reflux disease grades A and B: A prospective randomized trial. Drug Des. Dev. Ther. 2019, 13, 1347–1356. [Google Scholar] [CrossRef]
- Martinez, S.D.; Malagon, I.B.; Garewal, H.S.; Cui, H.; Fass, R. Non-erosive reflux disease (NERD)—Acid reflux and symptom patterns. Aliment. Pharmacol. Ther. 2003, 17, 537–545. [Google Scholar] [CrossRef]
- Hunt, R.; Armstrong, D.; Katelaris, P.; Afihene, M.; Bane, A.; Bhatia, S.; LeMair, A. Review Team: World gastroenterology organisation global guidelines: GERD global perspective on gastroesophageal reflux disease. J. Clin. Gastroenterol. 2017, 51, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Liao, K.-H.; Sung, C.-W.; Chu, S.-F.; Chiu, W.-T.; Chiang, Y.-H.; Hoffer, B.; Ou, J.-C.; Chen, K.-Y.; Tsai, S.-H.; Lin, C.-M.; et al. Reduced power spectra of heart rate variability are correlated with anxiety in patients with mild traumatic brain injury. Psychiatry Res. 2016, 243, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Singer, D.H. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Nunan, D.; Sandercock, G.R.H.; Brodie, D.A. A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research–Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef]
- Jones, R.; Junghard, O.; Dent, J.; Vakil, N.; Halling, K.; Wernersson, B.; Lind, T. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment. Pharmacol. Ther. 2009, 30, 1030–1038. [Google Scholar] [CrossRef]
- Lechien, J.R.; Bobin, F.; Muls, V.; Thill, M.P.; Horoi, M.; Ostermann, K.; Saussez, S. Validity and reliability of the reflux symptom score. Laryngoscope 2020, 130, E98–E107. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Wang, L.; Zhu, J. Factor structure and psychometric properties of Chinese version of Beck Anxiety Inventory in Chinese doctors. J. Health Psychol. 2018, 23, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yuan, C.M.; Huang, J.; Li, Z.Z.; Chen, J.; Zhang, H.Y.; Xiao, Z.P. Reliability and validity of the Chinese version of Beck Depression Inventory-II among depression patients. Chin. Ment. Health J. 2011, 25, 476–480. [Google Scholar]
- Gierk, B.; Kohlmann, S.; Kroenke, K.; Spangenberg, L.; Zenger, M.; Brähler, E.; Löwe, B. The somatic symptom scale–8 (SSS-8): A brief measure of somatic symptom burden. JAMA Intern. Med. 2014, 174, 399–407. [Google Scholar] [CrossRef]
- Li, T.; Wei, J.; Fritzsche, K.; Toussaint, A.C.; Zhang, L.; Zhang, Y.; Leonhart, R. Validation of the Chinese version of the Somatic Symptom Scale-8 in patients from tertiary hospitals in China. Front. Psychiatry 2022, 13, 940206. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.-M.; Kuo, M.-T.; Hsu, P.-I.; Kuo, C.-H.; Tai, W.-C.; Yang, S.-C.; Wu, K.-L.; Wang, H.-M.; Yao, C.-C.; Tsai, C.-E.; et al. Taiwan Acid-Related Disease Study Group. First-week clinical responses to dexlansoprazole 60 mg and esomeprazole 40 mg for the treatment of grades A and B gastroesophageal reflux disease. World J. Gastroenterol. 2017, 23, 8395–8404. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Wang, H.P.; Lin, L.Y.; Lee, B.C.; Chiu, H.M.; Wu, M.S.; Lin, J.T. Heart rate variability in patients with different manifestations of gastroesophageal reflux disease. Auton. Neurosci. 2004, 116, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-L.; Orr, W.C.; Yang, C.C.; Kuo, T.B. Cardiac autonomic regulation differentiates reflux disease with and without erosive esophagitis. Scand. J. Gastroenterol. 2006, 41, 1001–1006. [Google Scholar] [CrossRef]
- Jung, H.K.; Choi, M.G.; Baek, M.K.; Wu, J.C. Development and psychometric assessment of a self-evaluation questionnaire for gastroesophageal reflux disease. J. Neurogastroenterol. Motil. 2018, 24, 584. [Google Scholar] [CrossRef]
- Mayer, E.A. The neurobiology of stress and gastrointestinal disease. Gut 2000, 47, 861–869. [Google Scholar] [CrossRef]
- Song, E.M.; Jung, H.-K.; Jung, J.M. The Association Between Reflux Esophagitis and Psychosocial Stress. Dig. Dis. Sci. 2013, 58, 471–477. [Google Scholar] [CrossRef]
- Scarpellini, E.; Ang, D.; Pauwels, A.; De Santis, A.; Vanuytsel, T.; Tack, J. Management of refractory typical GERD symptoms. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Keefer, L.; Craft, J.; Dowjotas, K.; Kahrilas, I.J.; Roman, S.; Pandolfino, J.E. 765 Symptom reporting among PPI non responders may be driven by esophageal hypervigilance and not reflux phenotype. Gastroenterology 2015, 148, S-147. [Google Scholar] [CrossRef]
- Taft, T.H.; Guadagnoli, L.; Carlson, D.A.; Kou, W.; Keefer, L.; Pandolfino, J. Validation of the Short-Form Esophageal Hypervigilance and Anxiety Scale. Clin. Gastroenterol. Hepatol. 2022, 20, e64–e73. [Google Scholar] [CrossRef] [PubMed]
- Gyawali, C.P.; Kahrilas, P.J.; Savarino, E.; Zerbib, F.; Mion, F.; Smout, A.J.P.M.; Vaezi, M.; Sifrim, D.; Fox, M.R.; Vela, M.F.; et al. Modern diagnosis of GERD: The Lyon Consensus. Gut 2018, 67, 1351–1362. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variate | GERD Group (n = 98, %) | Control Group (n = 50, %) | p-Value |
|---|---|---|---|
| Age | 50.6 ± 15.1 | 50.2 ± 13.1 | 0.854 |
| Sex (M/F) | 33/65 (33.7/66.3) | 20/30 (40.0/60.0) | 0.448 |
| BMI | 24.6 ± 4.1 | 24.5 ± 4.5 | 0.987 |
| Smoking | 9 (9.2) | 5 (10.0) | 0.872 |
| Alcohol | 13 (13.3) | 2 (4.0) | 0.090 |
| Coffee | 57 (58.2) | 32 (64.0) | 0.493 |
| Tea | 61 (62.2) | 39 (78.0) | 0.023 |
| Betel nut | 2 (2.0) | 0 (0) | 0.309 |
| Spicy food | 59 (60.2) | 34 (68) | 0.353 |
| Sweaty food | 67 (68.4) | 40 (80) | 0.135 |
| Comorbidities | |||
| Diabetes | 15 (7.3) | 4 (8) | 0.209 |
| Hypertension | 25 (25.5) | 5 (10) | 0.080 |
| Coronary artery disease | 7 (7.1) | 1 (2) | 0.191 |
| Cerebral vascular disease | 0 (0) | 0 (0) | - |
| Chronic kidney disease | 1 (1.0) | 0 (0) | 0.474 |
| Insomnia | 55 (56.1) | 14 (28.0) | 0.001 |
| GERD history | 73 (74.5) | 0 (0) | <0.001 |
| Symptom score | |||
| GERDQ | 9.0 ± 2.4 | 5.9 ± 0.4 | <0.001 |
| GERDQLQ | 25.3 ± 17.2 | 0 | <0.001 |
| RSI | 15.1 ± 8.5 | 0.4 ± 0.2 | <0.001 |
| BAI | 6.6 ± 6.6 | 0 | <0.001 |
| BDI | 7.1 ± 6.7 | 0 | <0.001 |
| SSD-8 | 10.9 ± 6.8 | 0 | <0.001 |
| GERDQ (r and p Value) | GERDQLQ (r and p Value) | RSI (r and p Value) | |
|---|---|---|---|
| W0 | |||
| BAI | r = 0.452, p < 0.001 | r = 0.705, p < 0.001 | r = 0.656, p < 0.001 |
| BDI | r = 0.438, p < 0.001 | r = 0.698, p < 0.001 | r = 0.641, p < 0.001 |
| SSS-8 | r = 0.595, p < 0.001 | r = 0.810, p < 0.001 | r = 0.798, p < 0.001 |
| W4 | |||
| BAI | r = 0.406, p < 0.001 | r = 0.634, p < 0.001 | r = 0.547, p < 0.001 |
| BDI | r = 0.329, p = 0.001 | r = 0.584, p < 0.001 | r = 0.506, p < 0.001 |
| SSS-8 | r = 0.476, p < 0.001 | r = 0.675, p < 0.001 | r = 0.629, p < 0.001 |
| W8 | |||
| BAI | r = 0.391, p < 0.001 | r = 0.711, p < 0.001 | r = 0.616, p < 0.001 |
| BDI | r = 0.348, p < 0.001 | r = 0.668, p < 0.001 | r = 0.560, p < 0.001 |
| SSS-8 | r = 0.518, p < 0.001 | r = 0.808, p < 0.001 | r = 0.712, p < 0.001 |
| Variate/Time | Control Group | GERD Group W0 | GERD Group W8 | p-Value a |
|---|---|---|---|---|
| HR | 75.6 ± 10.1 | 73.3 ± 14.7 | 74.5 ± 12.2 | 0.394 |
| SD | 28.7 ± 12.6 * | 39.8 ± 46.3 | 34.4 ± 31.0 | 0.319 |
| RRIV (ms) | 59.1 ± 100.1 | 58.1 ± 73.7 | 56.1 ± 79.4 | 0.857 |
| TP (ms2) | 784.0 ± 699.3 * | 1556.2 ± 3324.4 | 1853.1 ± 5136.1 | 0.666 |
| VLF (Hz) | 331.7 ± 263.3 * | 561.1 ± 954.5 | 468.5 ± 680.5 | 0.487 |
| LF (Hz) | 182.5 ± 201.4 | 396.0 ± 1121.8 | 349.3 ± 896.5 | 0.654 |
| HF (Hz) | 208.9 ± 318.2 * | 618.5 ± 1644.6 | 443.4 ± 1209.6 | 0.319 |
| NN | 803.7 ± 113.1 | 840.2 ± 149.7 | 819.5 ± 130.0 | 0.122 |
| ANSage (y/o) | 55.3 ± 18.4 | 51.9 ± 21.5 | 53.0 ± 20.1 | 0.527 |
| Bal | −0.43 ± 1.94 | −0.75 ± 2.65 | −0.44 ± 2.50 | 0.257 |
| SDNN (ms) | 28.3 ± 12.5 * | 39.8 ± 46.3 | 34.2 ± 31.0 | 0.301 |
| In (LF/HF) | 0.077 ± 0.921 | 0.003 ± 1.106 | 0.126 ± 1.057 | 0.055 |
| LF (%) | 44.7 ± 18.6 | 40.8 ± 21.8 | 44.2 ± 21.6 | 0.155 |
| Refractory GERD (n = 15) | Non-Refractory GERD (n = 83) | p-Value | |
|---|---|---|---|
| Age | 52.8 ± 15.0 | 50.2 ± 15.2 | 0.547 |
| Sex(M/F) (n/%) | 3/12 (20.0/80.0) | 30/53 (31.6/63.9) | 0.223 |
| GERDQ | 10.7 ± 1.8 | 8.7 ± 2.3 | 0.002 |
| GERDQLQ | 38.5 ± 12.5 | 22.9 ± 16.9 | 0.001 |
| RSI | 20.9 ± 7.8 | 14.1 ± 8.2 | 0.004 |
| BAI | 9.5 ± 6.5 | 6.1 ± 6.6 | 0.069 |
| BDI | 10.4 ± 5.3 | 6.5 ± 6.7 | 0.037 |
| SSS-8 | 16.7 ± 7.2 | 9.8 ± 6.2 | <0.001 |
| HR | 70.7 ± 13.5 | 74.5 ± 14.4 | 0.354 |
| SD | 30.5 ± 25.9 | 40.2 ± 45.4 | 0.426 |
| RRIV (ms) | 38.3 ± 35.2 | 64.2 ± 75.5 | 0.197 |
| TP (ms2) | 1194.6 ± 2239.4 | 1622.3 ± 3493.3 | 0.649 |
| VLF (ms2) | 500.6 ± 859.6 | 572.1 ± 975.3 | 0.791 |
| LF (ms2) | 224.3 ± 420.4 | 427.0 ± 1205.0 | 0.522 |
| HF (ms2) | 382.9 ± 956.9 | 591.0 ± 1595.6 | 0.626 |
| NN | 870.9 ± 159.3 | 826.0 ± 143.6 | 0.276 |
| ANSage (y/o) | 56.4 ± 21.0 | 51.1 ± 21.6 | 0.377 |
| Bal | 0.6 ± 3.4 | −0.8 ± 2.4 | 0.054 |
| SDNN (ms) | 30.5 ± 25.9 | 40.1 ± 45.4 | 0.430 |
| In (LF/HF) | 0.3 ± 1.2 | −0.1 ± 1.1 | 0.209 |
| LF (%) | 48.9 ± 23.3 | 41.2 ± 21.3 | 0.209 |
| Variants | Refractory GERD n = 15 (%) | Non-Refractory GERD n = 83 (%) | Multivariate OR (95% C.I.) | p-Value |
|---|---|---|---|---|
| GERDQ (≥10) | 12 (80.0) | 32 (38.6) | 11.028 (2.147–56.654) | 0.004 |
| RSI (≥13) | 12 (80.0) | 46 (55.4) | 1.350 (0.279–6.542) | 0.709 |
| BDI (≥17) | 3 (20.0) | 2 (2.4) | 7.994 (0.736–86.879) | 0.088 |
| SSS-8 (≥12) | 12 (80.0) | 28 (33.7) | 7.377 (1.636–33.256) | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-M.; Huang, P.-Y.; Yang, S.-C.; Wu, M.-K.; Tai, W.-C.; Chen, C.-H.; Yao, C.-C.; Lu, L.-S.; Chuah, S.-K.; Lee, Y.-C.; et al. Correlation between Psychosomatic Assessment, Heart Rate Variability, and Refractory GERD: A Prospective Study in Patients with Acid Reflux Esophagitis. Life 2023, 13, 1862. https://doi.org/10.3390/life13091862
Wang H-M, Huang P-Y, Yang S-C, Wu M-K, Tai W-C, Chen C-H, Yao C-C, Lu L-S, Chuah S-K, Lee Y-C, et al. Correlation between Psychosomatic Assessment, Heart Rate Variability, and Refractory GERD: A Prospective Study in Patients with Acid Reflux Esophagitis. Life. 2023; 13(9):1862. https://doi.org/10.3390/life13091862
Chicago/Turabian StyleWang, Hsin-Ming, Pao-Yuan Huang, Shih-Cheng Yang, Ming-Kung Wu, Wei-Chen Tai, Chih-Hung Chen, Chih-Chien Yao, Lung-Sheng Lu, Seng-Kee Chuah, Yu-Chi Lee, and et al. 2023. "Correlation between Psychosomatic Assessment, Heart Rate Variability, and Refractory GERD: A Prospective Study in Patients with Acid Reflux Esophagitis" Life 13, no. 9: 1862. https://doi.org/10.3390/life13091862
APA StyleWang, H.-M., Huang, P.-Y., Yang, S.-C., Wu, M.-K., Tai, W.-C., Chen, C.-H., Yao, C.-C., Lu, L.-S., Chuah, S.-K., Lee, Y.-C., & Liang, C.-M. (2023). Correlation between Psychosomatic Assessment, Heart Rate Variability, and Refractory GERD: A Prospective Study in Patients with Acid Reflux Esophagitis. Life, 13(9), 1862. https://doi.org/10.3390/life13091862