Abstract
To ensure patient care in an oncological fertility preservation (FP) programme, specialists must provide technology that best suits the patients’ clinical conditions. In vitro oocyte maturation (IVM) and ovarian tissue cryopreservation (OTC) are possible fertility preservation treatments for women in need of urgent oncological treatment. IVM consists of the retrieval of immature oocytes from small antral follicles, with no or minimal ovarian stimulation by gonadotropins. Therefore, IVM has become a pertinent option for fertility preservation, especially for cases whereby ovarian stimulation is unfeasible or contra-indicated. Existing data on immature oocytes, retrieved transvaginally (OPU-IVM) or extracted from ovarian tissue ‘ex vivo’ (OTO-IVM), are still limited on technical consistency, efficacy, and safety. The present retrospective cohort study includes 89 women undergoing fertility preservation using IVM methodologies and 26 women undergoing ovarian stimulation (OS) in concomitant period. In total, 533 immature oocytes were collected from IVM patients, achieving a maturation rate of 57% and 70% in OTO-IVM and 73% and 82% in OPU-IVM at 24 h and 48 h in culture, respectively. The observed high maturation rates might be due to the use of patients’ serum in its innate status, i.e., without heat-inactivation. This permitted 7.6 ± 5.7 and 4.6 ± 4.9 oocytes to be vitrified in OTO-IVM and OPU-IVM, respectively, compared to 6.8 ± 4.6 from OS patients. Regarding OS patients, two of them underwent embryo transfer following the insemination of warmed oocytes after complete remission, resulting in a single live birth from one patient. Upon follow-up of two OTO-IVM patients after the termination of their oncological treatment, a total of 11 warmed oocytes lead to a transfer of a single embryo, but pregnancy was not achieved. From OPU-IVM, six embryos were transferred in three patients 4.25 years after oocyte vitrification, leading to the live birth of a healthy boy. The present case of live birth is among the first cases reported so far and supports the notion that IVM might be a relevant and safe FP option for cancer patients when oocyte preservation is required but ovarian stimulation is contra-indicated.
1. Introduction
In the last decade, the incidence rate of different types of cancer in young women has increased considerably, including breast cancer (SEER annual report 2020). The efficacy of early diagnosis is one of the reasons for the increased prevalence of cancer rates accompanied by other technological progresses in anticancer treatment and, consequently, enhanced long-term survival rates of women at reproductive age. Thus, it has become even more important to focus on the late side effects of cancer treatment since pregnancy rates decrease to about 38% post-cancer treatment [1]. Among young women, long-term quality of life is often diminished due to concerns about their future fertility and pregnancy. Advances in reproductive medicine and cryobiology have facilitated an increased interest in fertility preservation (FP) methods. Therefore, international guidelines underlining the significance of counselling every women about the impact of gonadotoxic treatment on future fertility and the possible effects regarding FP are important [2]. In France, the bioethics law imposes such counselling to all health professionals in cases whereby gonadotoxic treatment is required. This imposition benefits patients by smoothing the referral process to a reproductive medicine specialist before the start of oncological treatment. Established FP methods include oocyte and embryo cryopreservation following ovarian stimulation (OS). Ovarian tissue cryopreservation (OTC) is an option for patients who are at pre- or post-puberty and undergoing high-level gonadotoxic and/or urgent treatments [3,4,5,6]. Where applicable, OTC can be used in combination with OS for oocyte cryopreservation in women at a reproductive age [2]. Immature oocytes, retrieved transvaginally from small antral follicles (OPU-IVM) [7,8,9,10,11] or extracted from ovarian tissue ‘ex vivo’ (in vitro-matured ovarian tissue oocytes, i.e., OTO-IVM) [11,12,13], can undergo in vitro maturation (IVM) and be a source of oocytes for cryopreservation. This last methodology resulted in the first births reported from recovered immature oocytes from cancer patients. To date, five births have been reported following OTO-IVM—four derived from vitrified embryos [13,14,15,16] and one from vitrified oocytes [13]. Lately, a few more pregnancies (n = 6) have been also reported following OPU-IVM in cancer patients, derived from vitrified embryos [10,17,18], vitrified zygotes [19], and vitrified oocytes [17,18].
However, in view of the limited number of reported births after IVM in cancer patients, the efficacy of this technology is yet to be established [2]. Data are far from robust and are limited to rates of oocyte recovery and maturation. Reported oocyte maturation rates after 24–48 h culture vary from 23% to 62% from studies involving ‘ex vivo’ extracted oocytes from ovarian tissue [13,17,20,21,22] and between 48 and 67% from immature oocytes collected from transvaginal follicle aspiration [7,8,9,10,23,24,25]. Therefore, an improved understanding of the outcomes of using IVM in specific patients that require oncological treatment is needed.
The good clinical practice of an FP programme requires a multidisciplinary approach that considers the oncologists’ opinion when deciding on the therapeutic strategy for each oncological patient. In France, oncologists contraindicate OS to breast cancer patients in need of neoadjuvant treatment—independent of the hormonal receptivity status of tumours. In the present study, we offer OPU-IVM as an alternative to those patients and report our reproductive results along with the results of OTO-IVM applied in specific indications. We also present the results of the few patients who attempted pregnancy following post-oncological treatment.
2. Materials and Methods
2.1. Patient Population
This paper presents a retrospective analysis of data from all women diagnosed with cancer who underwent oocyte preservation following OS (OS-FP) or in vitro maturation fertility preservation (IVM-FP) from the start of our FP programme at the IVF center of Inovie Fertilité—Toulouse, France, in January 2014 until December 2019. A total of 122 post-pubertal patients (16–41 years old) were offered oocyte cryopreservation according to their couple status and their personal choices. All cancer types were included. The therapeutic strategy for each patient, including the indication for OS, OTO-IVM, or OPU-IVM was discussed and approved beforehand in our multidisciplinary meeting undertaken with the oncological team from the regional cancer institute (Cancer Institute, IUC-Toulouse) and other IVF centres, with our centre being the reference centre for IVM. The process, timing, and risks associated with the different procedures were discussed among the medical staff and with the patient and her family. Eight of these patients returned to the clinic with a desire to conceive after gonadotoxic treatment, and had their oocytes warmed for ICSI treatment. Written informed consent was obtained from all the patients before each procedure. This study was approved by the local Institutional Review Board.
2.2. Ovarian Stimulation (OS)-FP Treatment
Breast cancer patients younger than 42 years old undergoing adjuvant therapy and other cancer types with the potential to achieve stimulation before starting chemotherapy were treated under two types of protocol: the fixed GnRH antagonist protocol—when FSH could start on day 2 of menstrual cycle followed by day 4 or 7 GnRH antagonist administration—or the random GnRH antagonist protocol [3]. It is important to note that none of the patients received aromatase inhibitors as a co-treatment since this medication is not allowed in France. Final oocyte maturation was achieved with 0.2 mg of GnRH agonist when at least two leading follicles reached >18 mm, and oocyte retrieval occurred 36 h later, with oocyte vitrification 2–3 h after retrieval.
3. IVM-FP Treatment
3.1. OPU-IVM
IVM-FP was indicated in patients younger than 40 years old when chemotherapy could not be delayed or if ovarian stimulation was contraindicated. In fact, most of our OPU-IVM patients were breast cancer patients who had to undergo neoadjuvant therapy for cancer treatment. OPU was performed following the monitoring of patients without any FSH stimulation until, depending on the time available prior to start of oncological treatment, follicles attained diameters between 8 and 12 mm. OPU preferably occurred at the follicular phase of the menstrual cycle or, in cases of emergency FP, in the luteal phase. IVM oocyte retrieval was performed 36–38 h after the subcutaneous or nasal administration of 2 mg GnRH-Agonist. The transvaginal ultrasound-guided retrieval of oocytes was performed using a 19-gauge single lumen needle (K-OPS-7035-RWHET, Cook, Australia) with a reduced aspiration pressure (80 mmHg) under general anaesthesia. Matured oocytes at the day of retrieval were vitrified 3 h post-retrieval.
3.2. OTO-IVM
Patients younger than 35 years old underwent unilateral oophorectomy as part of their treatment or because they were identified as patients with a ≥80% chance of being sterile after their oncological treatment and had an indication for OTC. Patients did not receive any type of gonadotropin stimulation prior to surgery. Oophorectomy was performed by laparoscopy in the local operating theatre (adjacent to our IVF laboratory) or in another hospital. In the latter case, ovaries (n = 9) were transported into Leibovitz-15 media (Life Technologies) and supplemented with penicillin/streptomycin mix (Life Technologies) within 1–2 h post-procedure. In all cases, ovaries were transported at 4 °C to minimise the deleterious effect of ischaemic tissue injury and better preserve the ovarian tissue in case reimplantation will be necessary in the future. Upon arrival in the lab, antral follicles were punctured, and the follicle wall was scratched with a scalpel to release the follicle fluid and immature oocytes in the culture dish. Ovarian tissue was trimmed to 1 mm thickness in Leibovitz L-15 medium (Life Technologies, Essonne, France) supplemented with 4 mg/mL human serum albumin (has) (Vitrolife, Goteborg, Sweden), 100 IU/mL penicillin, and 100 µg/mL streptomycin (penicillin/streptomycin mix, Life Technologies), as described elsewhere [16]. Immature oocytes, released from follicles that were ruptured during the OTC process and thus extracted in an ex vivo manner were immediately collected by a second operator under a stereomicroscope at 37 °C. Cumulus oocyte complexes (COC) were washed twice in GMOPS medium (Vitrolife) under oil (Ovoil, Vitrolife) before being placed into culture dish. Naked oocytes were discarded.
All immature COC presenting compacted cumulus cells (Figure 1A,C) from both procedures were incubated in IVM medium (IVM System, Medicult, CooperSurgical) supplemented with 75 mIU/mL recFSH (Gonal-F, Merck), 100 mIU/mL recLH (Luveris, Merck), and 10% patients’ serum for a maximum of 48 h in a four-well dish with oil overlay (Ovoil, Vitrolife) in an incubator with the following atmospheric conditions: 6.5% CO2 at 37 °C (K-system). In OPU-IVM, some oocytes had expanded cumulus cells in response to the trigger of patients with GnRH agonist. Maturation from those oocytes was observed 3–4 h after retrieval, and as soon as the first polar body extrusion was visualized under the microscope, oocytes were vitrified. If, at this time, oocytes were in the MI stage, they were cultured until mature (the following day). All oocytes underwent vitrification following denudation with or without 40 IU/mL hyaluronidase (SynVitro Hyadase, Cooper Surgical, France). All mature oocytes were cryopreserved using the vitrification method with Vitrification kit media (Kitazato, Fujifilm, Spain), as described by the authors of [26].
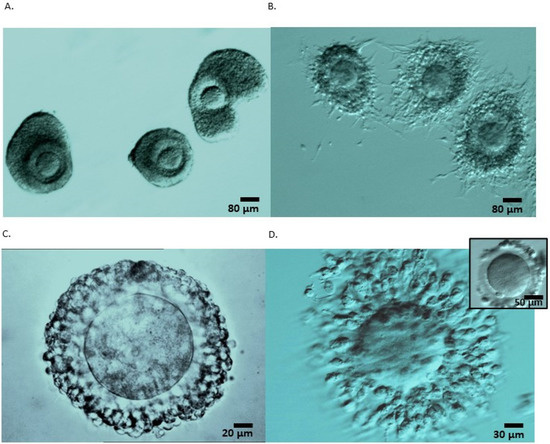
Figure 1.
Cumulus enclosed oocytes recovered from ovarian tissue ex vivo (A,B) and following follicular aspiration (C,D). (A) Cumulus-enclosed GV stage oocytes consisted of retrieved ovarian tissue following dissection and preparation for freezing. These COC constituted of healthy tightly compacted cells surrounding the oocyte despite being recovered from an ovary exposed for 2 h at 4 °C. (B) After being in IVM culture for 26 h, the cumulus cells of the matured oocytes expanded and surrounded the oocytes, forming a net of elongated cells partially attached to the dish. (C) A compacted cumulus-enclosed GV stage oocyte retrieved following follicle aspiration, and (D) after 24 h IVM culture enclosing a mature oocyte; an image of the same oocyte after denudation with the polar body visible at 7 o’clock position (right superior corner). All oocytes were cultured in IVM containing patients’ serum that were not subjected to heat-inactivation.
3.3. Oocyte Warming and Embryo Transfer Procedure
Patients who returned to the centre to attempt pregnancy did so with the approval of their oncologist, and their hormonal replacement therapy (artificial) protocol of endometrium preparation was approved in the FP multidisciplinary meeting.
The warming of oocytes was performed using the kitazato kit method [26]. All vitrified oocytes were warmed, and the surviving oocytes were inseminated using ICSI 2 h after the warming process was completed. Embryos were cultured until day 3 under 5% O2, 7% CO2 (k-system dry incubator) into G5-series (Vitrolife) and selected for transfer strictly according to their morphological appearance.
Endometrium priming cycle began on the first day of menstruation or after HRT withdrawal caused bleeding in postmenopausal patients. Briefly, the endometrium was primed with oral oestradiol valerate at a dose of 2 mg three times daily. When an endometrial thickness of more than 6 mm was reached, luteal support was provided using intravaginal micronized progesterone tablets (200 mg three times a day) on the evening of oocyte warming, and embryo transfer was scheduled for the fourth day of progesterone administration. Oestrogens and progestins were administered until a pregnancy blood test was performed and continued until 8 weeks of gestation, after which the dose was reduced, and the luteal support was discontinued 1 week later.
4. Statistical Analysis
Continuous data are presented as mean ± SD (range) and compared using Kruskal–Wallis rank test, and categorical data are expressed as numbers (percentages) and compared using the Chi-squared test (or Fisher’s exact test where appropriate).
5. Results
5.1. Patients’ Characteristics
Patients undergoing OPU-IVM (n = 73) included mostly breast cancer patients who had undergone neoadjuvant oncological treatment (80%). In total, 17% of OPU-IVM cases included breast cancer patients undergoing adjuvant oncological treatment who had been referred to our centre too close to the starting date of the chemotherapy treatment or had any other contra-indication for OS. The OTO-IVM (n = 16) cases were identified as patients with a ≥80% chance of being sterile after receiving oncological treatment. The borderline ovarian tumour patients in the OTO-IVM group (n = 6) were patients who had to undergo ovariectomy followed (or not) by chemotherapy in view of suspicious lesions. In most of these cases, OTC was also performed in case future reimplantation is needed or new developments offer the possibility to obtain mature oocytes from her tissue. Most cases of OS included patients with breast cancer receiving an adjuvant treatment (70%). The proportion and numbers of the type of disease in each FP treatment are detailed in Table 1. Side effects were minimal and restricted to one breast cancer patient. This patient was diagnosed with suspected hemoperitoneum occurrence a few days after OPU-IVM. She was discharged after being hospitalised for three days following laparoscopy surgery without the detection of active internal bleeding.

Table 1.
Proportion of the study population according to the type of cancer and the type of cryopreservation procedure for fertility preservation (FP).
5.2. Comparison of Collection Parameters among OTO-IVM, OPU-IVM and OS Procedures
As shown in Table 2, the groups were comparable in terms of FSH level, antral follicle count (AFC), and BMI index. However, given their type of cancer diagnosis, patients in the OTO-IVM group were younger compared to the age of patients undergoing OPU-IVM and OS procedures, who were mostly breast cancer patients.
Table 2.
Comparison of outcomes from OTO-IVM, OPU-IVM, and OS cryopreservation procedures in cancer patients.
Out of the 122 patients who underwent treatment for fertility preservation during the study period, 7 did not obtain oocytes after OTO-IVM (n = 2), OPU-IVM (n = 4), and OS (n = 1). In IVM procedures, oocytes were collected during the follicular phase in 62% and 78% of patients and during the luteal phase in 27% and 22% of cycles from OTO-IVM and OPU-IVM, respectively. In 11% of patients whom ovariectomy was performed in another hospital and transported to the laboratory for OTO-IVM, no information was provided regarding the day of the cycle.
5.3. Oocytes Collection and Maturation
The number of oocytes collected was higher in OTO-IVM and OS compared to OPU-IVM (p < 0.001). All oocytes collected after OTO were at the GV-stage with enclosed compacted cumulus cells (Figure 1), while in OPU, since these patients received GnRH-agonist triggering, 19% of oocytes were already at the MII-stage and 2% were at the MI-stage upon retrieval. In OS patients, 86% of oocytes were MII, 5 oocytes were at the MI stage, and 29 were at the GV stage after denudation. Further in vitro maturation of these collected immature MI/GV oocytes was not performed.
Upon culturing for 24–28 h, the rates of maturation were 16% higher for OPU than for OTO oocytes, and upon culturing for 44–48 h, 82% of GV-stage oocytes ended up maturing to MII from OPU-IVM compared to 70% of OTO-IVM patients (p < 0.0001). However, the total number of matured vitrified oocytes was higher for OTO patients (7.6 ± 5.7) compared to those who received OPU (4.6 ± 4.9; p < 0.05) and OS (6.8 ± 4.6) (NS) (Table 2).
There was no difference in maturation rates at the 48 h culture period, when oocytes were extracted “ex vivo” (OTO-IVM) from the unstimulated ovaries during the follicular phase (69%) or luteal phase (68%) in the 89% of patients from whom progesterone level could be obtained to determine the luteal phase. However, from GnRH-agonist-triggered OPU-IVM patients, maturation rates were higher when oocytes were collected during the follicular phase compared to the luteal phase, although these differences were not significant (69% versus 50% at 28 h, and 81% versus 71% at 48 h culture, respectively) (NS). The rate of oocytes that were already matured at MII in OPU-IVM when oocyte retrieval was performed during the follicular phase was 19% versus 13% for luteal phase retrieval (NS).
Concerning the effect of ovarian transportation on OTO-IVM rates, we observed a lower kinetics of maturation following 1–2 h of exposure at 4 °C compared to immature oocytes from ovaries recovered at our centre and with a shorter exposure time (15–30 min) at 4 °C, which yielded a result of 52% versus 64% at 24 h (NS). After 48 h, a similar maturation was obtained in both conditions (69% versus 66%).
5.4. Outcomes of Cryopreserved Oocytes
A total of seven (6%) out of one-hundred-and-fifteen patients with oocytes cryopreserved in our oncofertility programme were deceased one to two years after cancer diagnosis (four after OTO, two after OPU, and one after OS treatment). Until December 2019, a total of nine (8%) patients returned for oocyte warming (Table 3), and the average of years for these patients’ return following disease-free diagnosis was a mean of 1 year in OTO, 4.25 years in OPU, and 3 years in OS patients. We obtained a relatively low oocyte survival rate (<60%) but a normal proportion of fertilization, which resulted in 35% embryos acquired per total number of oocytes warmed in IVM treatment groups and 50% after OS treatment (NS). Six patients with warmed oocytes underwent the procedure of transferring cleaved embryos, resulting in two clinical pregnancies at 6 weeks, one after OPU-IVM and one after OS. The remaining four patients failed to achieve pregnancy. The OPU-IVM patient was 35 years old, and the OS patient was 38 years old at the time of oocyte vitrification, and both patients were diagnosed with breast cancer prior to FP. These two pregnancies resulted in the delivery of healthy children. The OS patient had a caesarean section at 36.3 weeks of gestation to deliver a boy presenting an Apgar score of 10 and a birth weight and height of 3880 kg and 49 cm, respectively. At one year of age, the boy presented normal developmental growth and cognitive status.
Table 3.
Outcomes of cryopreserved oocytes in each procedure type of fertility preservation (FP).
5.5. Pregnancy Case from OPU-IVM
In one pregnancy derived from a 35-year-old patient at the time of OPU-IVM treatment from whom eight immature oocytes were retrieved, five oocytes matured 24 h after IVM and were vitrified. The patient returned four years later presenting an ovarian insufficiency with 0.23 ng/mL AMH levels and 21 IU/l FSH after the cessation of her oncological treatment and disease-free diagnosis. Four oocytes survived the warming procedure, and one five-cell embryo was transferred on day 2 of a hormonal replacement therapy (HRT) cycle. After 37.6 weeks of gestation, this resulted in the birth of a healthy boy with an Apgar score 10 and a birth weight and height of 3880 kg and 49 cm, respectively. At one year of age, the developmental growth and cognitive status of the child was reportedly within a normal range.
6. Discussion
The presented case of live birth indicates that IVM followed by oocyte vitrification can be applied as a strategy for FP for women in need of oncological treatment. To our knowledge, very few births have been reported in the literature from IVM cases regarding FP in cancer patients. The first live births from OPU-IVM in cancer patients were from vitrified embryos, which were transferred a few years later when patients were in remission [10,17]. The type of oncological condition for each of the patients has not been specified by the authors. The first live birth reported from vitrified IVM oocytes was from a patient diagnosed with invasive breast cancer at the age of 29 [27]. Ovarian stimulation was contra-indicated in view of the cancer type (oestrogen-receptor positive), and the patient decided to undergo IVM only, instead of OTC. Seven immature oocytes were retrieved at OPU, and six oocytes were vitrified 48 h after IVM. The patient returned five years later once deemed cured, became pregnant after the transfer of one cleavage-stage embryo upon endometrial preparation with HRT, and delivered a healthy boy at term. More recently, a live birth following the cryopreservation of zygotes after IVM was reported in a breast cancer patient [19]. A total of two out of four immature oocytes reached maturation, with two zygotes being cryopreserved, the latter of which were thawed 9 years later and cultured until day 3, resulting in a healthy baby at term. The patient was 42 years old by then and had been attempting to conceive naturally without success for 5 years. Subsequently, the single IVM birth described here is thus, to our knowledge, a third reported healthy child from vitrified oocytes after IVM in a cancer patient. The patient was diagnosed with breast cancer, and IVM was performed prior to her receiving neoadjuvant oncology treatment at the age of 35. At the time, ovarian stimulation was contra-indicated by the oncologists. Eight immature oocytes were retrieved, with five becoming mature 24 h after IVM. Four years later, when the patient was considered disease-free, she returned with ovarian insufficiency and, following the survival of four oocytes, one five-cell embryo was transferred into an HRT cycle, and the patient delivered a healthy boy. Overall, cases of pregnancy after IVM in cancer patients are recent and data remain limited. The reasons for a lack of data on IVM in cancer patients include the fact that IVM is restricted to certain patient conditions, mainly those that have contra-indication(s) for hormonal stimulation. Another reason for the lack of data on IVM outcomes is because few IVF centres apply IVM routinely and, when considering the risk-benefit balance of the intervention, are often not sufficiently prepared to provide IVM treatment to their FP patients due to a lack of know-how. Additionally, there is the fact that, since the application of IVM together with oocyte vitrification techniques on cancer patients, the return rate of cancer-survivals to recuperate their oocytes is rather low (6–15%) [10,11].
Cryopreservation of the ovarian cortex was made available to cancer patients long before IVM treatment [28,29]. Nowadays, data published by expert centres on ovarian tissue cryopreservation (OTC) and transplantation (OTT) demonstrate that ovarian function after grafting is restored in more than 90% of patients, and approximately half of the >100 reported births have derived from spontaneous conceptions [6,30,31,32]. OTC and OTT are now established and valid options that can be considered in all ages when there is potential for ovarian insufficiency later in a woman’s life, with the most evidence-based utility being in cases of high gonadotoxic treatment [3,4,5]. In this case, OTC can be used as an alternative when oocyte/embryo cryopreservation is not feasible because it has the advantages of being practicable in urgent situations and allows one to forego hormonal treatment. Clinical applications of the procedure to restore ovarian function and fertility were supported by experiments using animal models about thirty years ago, with the first reported success in humans being achieved 15 years later. To increase the chances of future pregnancy, OTC can be combined with other FP strategies, including the following: ovarian stimulation at posteriori to OTC; immature oocyte aspiration at same or collateral ovary followed by OTC [11]. The combination of OTC with oocyte aspiration and cryopreservation seems feasible and effective [12], but the efficacy-related data required to support this conclusion are very limited [2].
In addition, OTC can be combined with the extraction of immature oocytes from the medullar tissue for IVM in a laboratory setting from the surgically removed ovarian biopsies or whole ovaries [11,22]. OTO-IVM is a promising technique for fertility preservation in women who face the risk of losing their fertility potentiality due to cancer treatment, premature ovarian failure, or other medical conditions. Adding OTO-IVM to OTC will not delay cancer treatment and offers a surplus source of oocytes for cryopreservation. For patients with an ovary-related malignancy, experts do not recommend OTT since the putative risk of reintroducing cancer cells seems to outweigh the benefits of the OTT procedure [2]. Alternatively, OTO-IVM is a valuable option to be considered. Five live births have been reported from this methodology, without any reported congenital malformations in the new-born [13,14,15]. In our study, OTO-IVM derived from total oophorectomy resulted in an increase in the number of oocytes retrieved and vitrified when compared to OPU-IVM. It is clear from the literature that the live birth potential of these OTO-IVM oocytes may be significantly lower compared to the live birth potential of mature oocytes retrieved after ovarian stimulation [33]; however, they have, to date, resulted in more live births than oocytes retrieved and vitrified via OPU-IVM.
One of the advantages of IVM, whether by OPU or OTO, is that it can be performed at any stage of the menstrual cycle, which is particularly appropriate when urgent fertility preservation is required prior to oncological treatments [8,9]. Indeed, the retrospective analysis of 192 IVM cycles performed in 164 cancer patients showed no difference between IVM performed during the early follicular, late follicular, and luteal phases in terms of number of oocytes collected, maturation rates, number of cryopreserved oocytes and embryos, and fertilization rates [9]. Furthermore, the prospective analysis of 248 breast cancer patients who underwent fertility preservation prior to neoadjuvant chemotherapy showed similar rates for the retrieval of oocytes, regardless of whether the procedure had been performed in the follicular or luteal phase of the cycle [8]. In our dataset, we did not observe any differences in maturation rates during the follicular phase compared to oocytes extracted ex vivo in the luteal phase (OTO-IVM). However, we could observe higher in vitro maturation rates for oocytes collected from OPU-IVM during the follicular phase compared to the luteal phase (69% vs. 50% at 28 h; 81% vs. 71% at 48 h culture, respectively). Though, given the limited sample size, this difference did not reach statistical significance. It is important to note that, when oocyte retrieval was performed during the follicular phase, the proportion of oocytes that were already matured at MII in OPU-IVM was slightly higher (19% vs. 13% when retrieved at luteal). In view of these preliminary results, when possible, we recommended performing OPU-IVM in the follicular phase rather than in the luteal phase of the cycle in cancer patients.
The success rate of in vitro oocyte maturation for FP can vary depending on several factors, including the age and ovarian reserve of the patient, the protocol used for IVM, and the number and quality of mature oocytes retrieved. Although it has been reported that AFC and serum AMH values >20 follicles and 3.7 ng/mL, respectively, are required to obtain at least 10 IVM oocytes for cryopreservation [25], one must not be discouraged if less oocytes are retrieved. Interestingly, the previously mentioned cases of live births from IVM derived from only a few recovered oocytes. Anyhow, the mean number of oocytes retrieved from IVM is generally less than would be expected after ovarian stimulation, and has been reported to be between five and seventeen in cancer patients [2].
Concerning maturation rates achieved after IVM, reports from the literature describe up to 67% of maturation at 48 h culture when OPU-IVM is performed and ranges from 24 to 57% maturation from oocytes deriving from OTO-IVM [2]. Our overall high rates of maturation of 70% at 48 h of culture in OTO-IVM, and a much higher maturation rate of 82% in OPU-IVM compared to the literature cases might be explained by the type of culture conditions applied. IVM culture involves additives such as hormones, growth factors, and protein sources such as HSA, SSS or patients’ serum. It is common practice to render patients’ serum heat-inactive to avoid concerns over possible contaminants being present in serum and to inactivate the complement binding capacity to avoid cell lysis by antibody binding. This was in fact necessary in routine cell culture, which often involved the use of heterologous serum and serum from animal source. Logically, when using autologous serum, the process of inactivation is obsolete because, firstly, serum is ‘per se’ sterile, and secondly, an immunological reaction will logically not take place. We are the first to report the use of patients’ serum in its innate state, i.e. without heat-inactivation in an IVM culture system. This implies that components such as growth factors, hormones, and other proteins remain intact, favoring the cumulus-cells support to oocyte maturation. However, in the present study, we did not perform a comparison between the two groups (inactivating the serum or not) to effectively demonstrate the differences in maturation rates between the conditions.
It is unclear if our enriched culture system could be the cause for the relatively low survival rates following vitrification. It has been postulated that IVM oocytes are more susceptible to vitrification, and several reports have described the negative effects of vitrification on oocyte survival when IVM is involved [33,34]. However, as data on survival rates after vitrification and warming from oocytes and embryos after IVM in oncological patients are scarce, evaluation on its efficacity is currently unfeasible. The two cases of OS also presented a limited survival rate when compared to our donor oocyte population (56% versus 86%). The low number of patients do not allow us to conclude whether the pathology of the patient influences oocyte quality to vitrification procedure.
It is important to note some other limitations of the present study. Firstly, the study is of a retrospective nature, and data regarding oocyte preservation have been collected throughout a six-year period. This meant that there was a higher chance that any changes related to products other than the IVM medium and culture, or even environmental changes, could have affected the results. Secondly, is the limited sample size, mainly regarding patient return rates, which were fairly low for reasons previously mentioned. Therefore, data on the impact of specific methodologies on oocyte maturation rates presented in this study may not be conclusive. These data are related to the phase of the cycle whereby oocytes are retrieved, whether at the luteal or follicular phase, as well as the influence of the timings of immature oocyte exposure to different temperatures. These aspects should be further analysed with a more robust set of data.
A very important factor to consider is the benefit–risk balance of the OPU-IVM procedure. The methodology of IVM oocyte retrieval is more abrupt than that of conventional OS retrieval. It involves concomitant aspiration and the needle-forced detachment of granulosa cells from the wall of small antral follicles. This increases the risk of blood contamination with respect to follicular fluid and might increase the risk of complications such as internal bleeding post-retrieval. Therefore, IVM requires specific expertise to optimize oocyte retrieval to avoid complications. This might be even more drastic in cancer patients because, if extra eventual intervention or hospitalisation is necessary, their chemotherapy treatment may experience delays. Therefore, it is strongly recommended to perform OPU-IVM only when oocyte cryopreservation is required but ovarian stimulation is not feasible [2], and when patients medical conditions allow.
In summary, with the increase in the life expectancy of patients diagnosed with most types of cancer due to advances in therapeutics and early diagnoses, opening possibilities for different strategies of fertility preservation has become crucial for the improvement of patient quality of life after oncological treatment. IVM technology offers an alternative for FP that otherwise would be not accessible to patients in certain situations. While IVM has shown promising results, it is important to discuss the potential risks and benefits of this technique with a healthcare provider before proceeding. Overall, data on IVM and OTC are still limited with respect to technical consistency, and their efficacy and safety are still to be proven. Prospective studies involving experts in the field could provide additional data to fulfil this aim.
Author Contributions
Conceptualization, D.N.; methodology, D.N., C.F.-P., M.C., P.A., M.D. and M.M.; validation, D.N., C.F.-P., M.C., P.A., M.D. and M.M.; formal analysis, D.N.; investigation, D.N.; data curation, D.N.; writing—original draft, D.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Ramsay Santé (COS-RGDS-2021-09-007) approved on 19 October 2021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is unavailable due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Anderson, R.A.; Brewster, D.H.; Wood, R.; Nowell, S.; Fischbacher, C.; Kelsey, T.W.; Wallace, W.H.B. The Impact of Cancer on Subsequent Chance of Pregnancy: A Population-Based Analysis. Hum. Reprod. 2018, 33, 1281–1290. [Google Scholar] [CrossRef]
- ESHRE Guideline Group on Female Fertility Preservation; Anderson, R.A.; Amant, F.; Braat, D.; D’Angelo, A.; Chuva de Sousa Lopes, S.M.; Demeestere, I.; Dwek, S.; Frith, L.; Lambertini, M.; et al. ESHRE Guideline: Female Fertility Preservation. Hum. Reprod. Open 2020, 2020, hoaa052. [Google Scholar] [CrossRef]
- Cakmak, H.; Katz, A.; Cedars, M.I.; Rosen, M.P. Effective Method for Emergency Fertility Preservation: Random-Start Controlled Ovarian Stimulation. Fertil. Steril. 2013, 100, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- De Vos, M.; Smitz, J.; Woodruff, T.K. Fertility Preservation in Women with Cancer. Lancet 2014, 384, 1302–1310. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F. International Society for Fertility Preservation–ESHRE–ASRM Expert Working Group Update on Fertility Preservation from the Barcelona International Society for Fertility Preservation-ESHRE-ASRM 2015 Expert Meeting: Indications, Results and Future Perspectives. Fertil. Steril. 2017, 108, 407–415.e11. [Google Scholar] [CrossRef]
- Silber, S.J.; DeRosa, M.; Goldsmith, S.; Fan, Y.; Castleman, L.; Melnick, J. Cryopreservation and Transplantation of Ovarian Tissue: Results from One Center in the USA. J. Assist. Reprod. Genet. 2018, 35, 2205–2213. [Google Scholar] [CrossRef]
- Hourvitz, A.; Yerushalmi, G.M.; Maman, E.; Raanani, H.; Elizur, S.; Brengauz, M.; Orvieto, R.; Dor, J.; Meirow, D. Combination of ovarian tissue harvesting and immature oocyte collection for fertility preservation increases preservation yield. Reprod. Biomed. Online 2015, 31, 497–505. [Google Scholar] [CrossRef]
- Grynberg, M.; Poulain, M.; le Parco, S.; Sifer, C.; Fanchin, R.; Frydman, N. Similar in Vitro Maturation Rates of Oocytes Retrieved during the Follicular or Luteal Phase Offer Flexible Options for Urgent Fertility Preservation in Breast Cancer Patients. Hum. Reprod. 2016, 31, 623–629. [Google Scholar] [CrossRef]
- Creux, H.; Monnier, P.; Son, W.-Y.; Tulandi, T.; Buckett, W. Immature Oocyte Retrieval and in Vitro Oocyte Maturation at Different Phases of the Menstrual Cycle in Women with Cancer Who Require Urgent Gonadotoxic Treatment. Fertil. Steril. 2017, 107, 198–204. [Google Scholar] [CrossRef]
- Creux, H.; Monnier, P.; Son, W.-Y.; Buckett, W. Thirteen Years’ Experience in Fertility Preservation for Cancer Patients after in Vitro Fertilization and in Vitro Maturation Treatments. J. Assist. Reprod. Genet. 2018, 35, 583–592. [Google Scholar] [CrossRef]
- Delattre, S.; Segers, I.; Van Moer, E.; Drakopoulos, P.; Mateizel, I.; Enghels, L.; Tournaye, H.; De Vos, M. Combining Fertility Preservation Procedures to Spread the Eggs across Different Baskets: A Feasibility Study. Hum. Reprod. 2020, 35, 2524–2536. [Google Scholar] [CrossRef] [PubMed]
- Fasano, G.; Dechène, J.; Antonacci, R.; Biramane, J.; Vannin, A.S.; Van Langendonckt, A.; Devreker, F.; Demeestere, I. Outcomes of immature oocytes collected from ovarian tissue for cryopreservation in adult and prepubertal patients. Reprod. Biomed. Online 2017, 34, 575–582. [Google Scholar] [CrossRef]
- Segers, I.; Bardhi, E.; Mateizel, I.; Van Moer, E.; Schots, R.; Verheyen, G.; Tournaye, H.; De Vos, M. Live Births Following Fertility Preservation Using In-Vitro Maturation of Ovarian Tissue Oocytes. Hum. Reprod. 2020, 35, 2026–2036. [Google Scholar] [CrossRef]
- Prasath, E.B.; Chan, M.L.H.; Wong, W.H.W.; Lim, C.J.W.; Tharmalingam, M.D.; Hendricks, M.; Loh, S.F.; Chia, Y.N. First Pregnancy and Live Birth Resulting from Cryopreserved Embryos Obtained from in Vitro Matured Oocytes after Oophorectomy in an Ovarian Cancer Patient. Hum. Reprod. 2014, 29, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Uzelac, P.S.; Nakajima, S.T. Live Birth Following in Vitro Maturation of Oocytes Retrieved from Extracorporeal Ovarian Tissue Aspiration and Embryo Cryopreservation for 5 Years. Fertil. Steril. 2015, 104, 3. [Google Scholar] [CrossRef] [PubMed]
- Segers, I.; Mateizel, I.; Van Moer, E.; Smitz, J.; Tournaye, H.; Verheyen, G.; De Vos, M. In Vitro Maturation (IVM) of Oocytes Recovered from Ovariectomy Specimens in the Laboratory: A Promising “Ex Vivo” Method of Oocyte Cryopreservation Resulting in the First Report of an Ongoing Pregnancy in Europe. J. Assist. Reprod. Genet. 2015, 32, 1221–1231. [Google Scholar] [CrossRef]
- Kedem, A. Outcome of Immature Oocytes Collection of 119 Cancer Patients during Ovarian Tissue Harvesting for Fertility Preservation. J. Assist. Reprod. Genet. 2018, 6, 851–856. [Google Scholar] [CrossRef]
- Mayeur, A.; Puy, V.; Windal, V.; Hesters, L.; Gallot, V.; Benoit, A.; Grynberg, M.; Sonigo, C.; Frydman, N. Live Birth Rate after Use of Cryopreserved Oocytes or Embryos at the Time of Cancer Diagnosis in Female Survivors: A Retrospective Study of Ten Years of Experience. J. Assist. Reprod. Genet 2021, 38, 1767–1775. [Google Scholar] [CrossRef]
- Rodrigues, P. Oncofertility Case Report: Live Birth 10 Years after Oocyte in Vitro Maturation and Zygote Cryopreservation. J. Assist. Reprod. Genet. 2020, 6, 1767–1775. [Google Scholar] [CrossRef]
- Takae, S.; Sugishita, Y.; Yoshioka, N.; Hoshina, M.; Horage, Y.; Sato, Y.; Nishijima, C.; Kawamura, K.; Suzuki, N. The Role of Menstrual Cycle Phase and AMH Levels in Breast Cancer Patients Whose Ovarian Tissue Was Cryopreserved for Oncofertility Treatment. J. Assist. Reprod. Genet. 2015, 32, 305–312. [Google Scholar] [CrossRef]
- Yin, H.; Jiang, H.; Kristensen, S.G.; Andersen, C.Y. Vitrification of in Vitro Matured Oocytes Collected from Surplus Ovarian Medulla Tissue Resulting from Fertility Preservation of Ovarian Cortex Tissue. J. Assist. Reprod. Genet. 2016, 33, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Silber, S.J.; Goldsmith, S.; Castleman, L.; Hurlbut, K.; Fan, Y.; Melnick, J.; Hayashi, K. In-Vitro Maturation and Transplantation of Cryopreserved Ovary Tissue: Understanding Ovarian Longevity. Reprod. BioMed. Online 2022, 44, 504–514. [Google Scholar] [CrossRef] [PubMed]
- El Hachem, H.; Sonigo, C.; Benard, J.; Presse, M.; Sifer, C.; Sermondade, N.; Grynberg, M. Comparison of GnRH Agonist and HCG for Priming in Vitro Maturation Cycles in Cancer Patients Undergoing Urgent Fertility Preservation. PLoS ONE 2018, 13, e0208576. [Google Scholar] [CrossRef] [PubMed]
- Sermondade, N.; Sonigo, C.; Sifer, C.; Valtat, S.; Ziol, M.; Eustache, F.; Grynberg, M. Serum Antimüllerian Hormone Is Associated with the Number of Oocytes Matured in Vitro and with Primordial Follicle Density in Candidates for Fertility Preservation. Fertil. Steril. 2019, 111, 357–362. [Google Scholar] [CrossRef]
- Sonigo, C.; Simon, C.; Boubaya, M.; Benoit, A.; Sifer, C.; Sermondade, N.; Grynberg, M. What Threshold Values of Antral Follicle Count and Serum AMH Levels Should Be Considered for Oocyte Cryopreservation after in Vitro Maturation? Hum. Reprod. 2016, 31, 1493–1500. [Google Scholar] [CrossRef]
- Rienzi, L.; Cobo, A.; Paffoni, A.; Scarduelli, C.; Capalbo, A.; Vajta, G.; Remohí, J.; Ragni, G.; Ubaldi, F.M. Consistent and Predictable Delivery Rates after Oocyte Vitrification: An Observational Longitudinal Cohort Multicentric Study. Hum. Reprod. 2012, 27, 1606–1612. [Google Scholar] [CrossRef]
- Grynberg, M.; Mayeur Le Bras, A.; Hesters, L.; Gallot, V.; Frydman, N. First Birth Achieved after Fertility Preservation Using Vitrification of in Vitro Matured Oocytes in a Woman with Breast Cancer. Ann. Oncol. 2020, 31, 541–542. [Google Scholar] [CrossRef]
- Gellert, S.E.; Pors, S.E.; Kristensen, S.G.; Bay-Bjørn, A.M.; Ernst, E.; Yding Andersen, C. Transplantation of frozen-thawed ovarian tissue: An update on worldwide activity published in peer-reviewed papers and on the Danish cohort. J. Assist. Reprod. Genet. 2018, 35, 561–570. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.M.; Demylle, D.; Jadoul, P.; Pirard, C.; Squifflet, J.; Martinez-Madrid, B.; Langendonckt, A.V. Livebirth after Orthotopic Transplantation of Cryopreserved Ovarian Tissue. Lancet 2004, 364, 1405–1410. [Google Scholar] [CrossRef]
- Donnez, J.; Dolmans, M.-M. Fertility Preservation in Women. Available online: https://www.nejm.org/doi/10.1056/NEJMra1614676 (accessed on 28 May 2021).
- Diaz-Garcia, C.; Domingo, J.; Garcia-Velasco, J.A.; Herraiz, S.; Mirabet, V.; Iniesta, I.; Cobo, A.; Remohí, J.; Pellicer, A. Oocyte Vitrification versus Ovarian Cortex Transplantation in Fertility Preservation for Adult Women Undergoing Gonadotoxic Treatments: A Prospective Cohort Study. Fertil. Steril. 2018, 109, 478–485.e2. [Google Scholar] [CrossRef]
- Silber, S.; Kagawa, N.; Kuwayama, M.; Gosden, R. Duration of Fertility after Fresh and Frozen Ovary Transplantation. Fertil. Steril. 2010, 94, 2191–2196. [Google Scholar] [CrossRef] [PubMed]
- Son, W.-Y.; Henderson, S.; Cohen, Y.; Dahan, M.; Buckett, W. Immature Oocyte for Fertility Preservation. Front. Endocrinol. 2019, 10, 464. [Google Scholar] [CrossRef] [PubMed]
- Mohsenzadeh, M.; Tabibnejad, N.; Vatanparast, M.; Anbari, F.; Ali Khalili, M.; Karimi-Zarchi, M. Vitrification Has Detrimental Effects on Maturation, Viability, and Subcellular Quality of Oocytes Post IVM in Cancerous Women: An Experimental Study. Int. J. Reprod. Biomed. 2019, 17, 175–184. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).