
Urinary Markers of Tubular Injury and Renal Fibrosis in Patients with Type 2 Diabetes and Different Phenotypes of Chronic Kidney Disease




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Methods
2.3. Statistical Procedures
3. Results
3.1. Clinical Characteristics of Patients
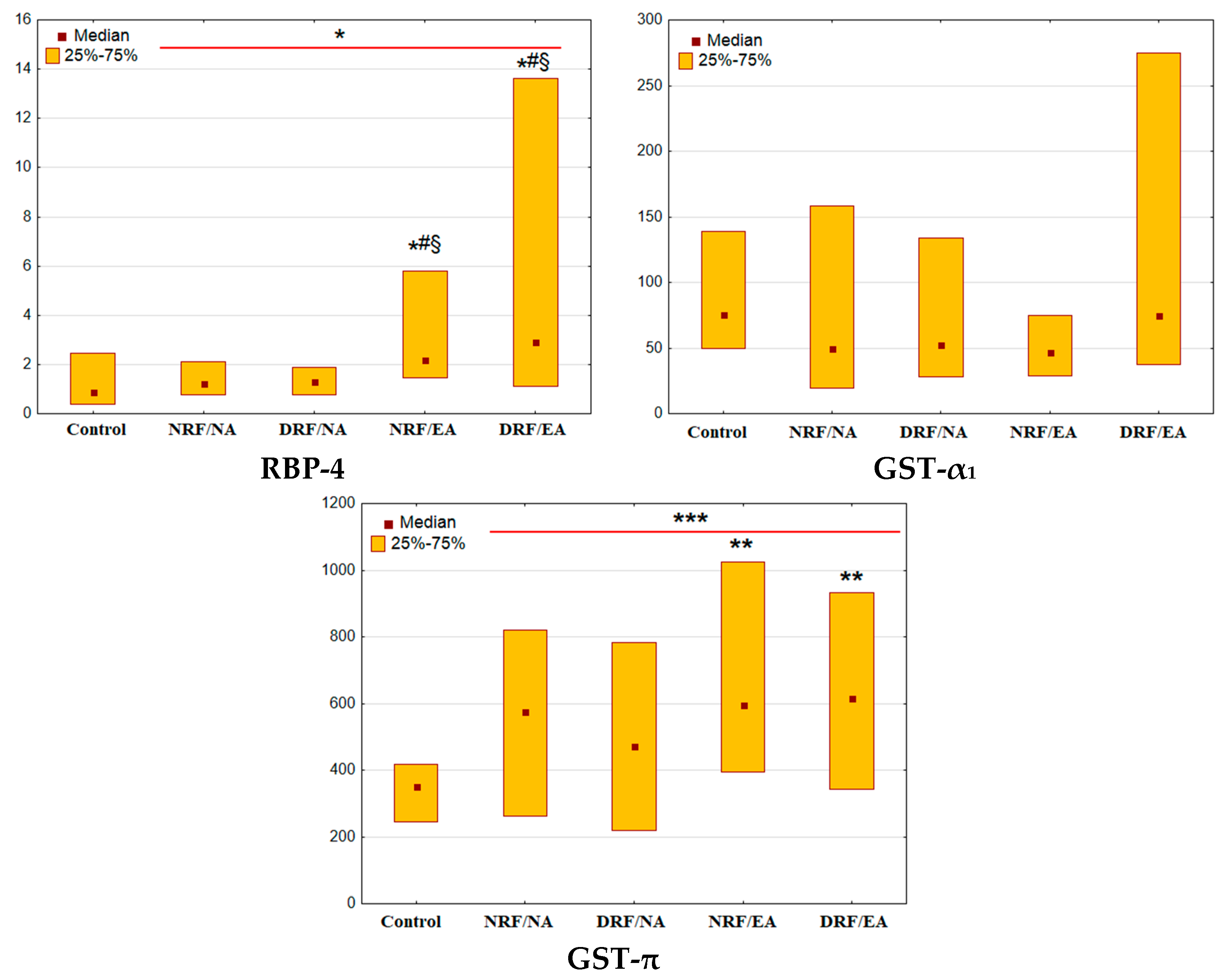
3.2. Urinary Excretion of Tubular Markers
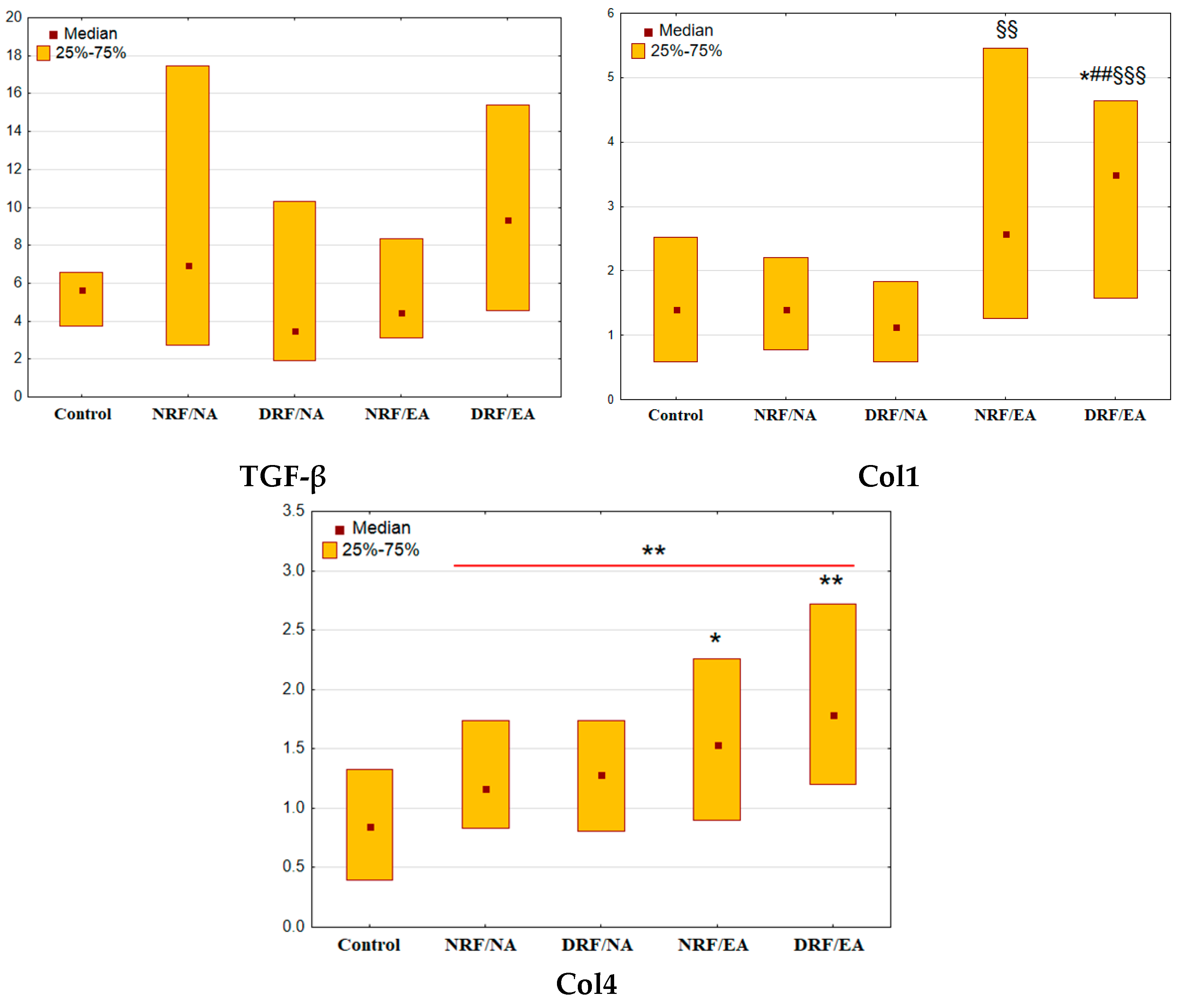
3.3. Urinary Excretion of TGF-β, Col1, and Col4
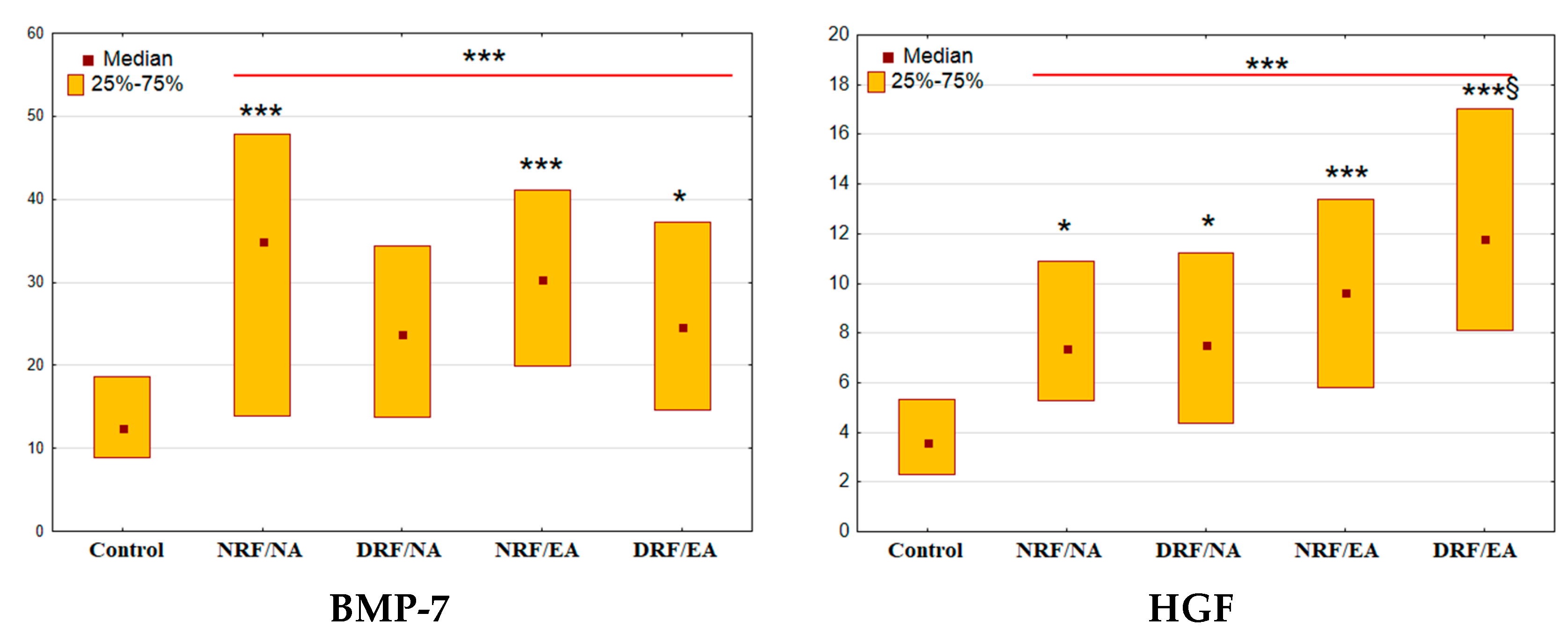
3.4. Urinary Excretion of BMP-7 and HGF
3.5. Urinary Markers in Multivariate Models
4. Discussion
4.1. Tubular Markers
4.2. TGF-β, Col1, and Col4
4.3. BMP-7 and HGF
4.4. Why do Urinary Markers Play Differently in Albuminuric and Non-Albuminuric CKD?
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viazzi, F.; Russo, G.T.; Ceriello, A.; Fioretto, P.; Giorda, C.; De Cosmo, S.; Pontremoli, R. Natural history and risk factors for diabetic kidney disease in patients with T2D: Lessons from the AMD-annals. J. Nephrol. 2019, 32, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Klimontov, V.V.; Korbut, A.I. Albuminuric and non-albuminuric patterns of chronic kidney disease in type 2 diabetes. Diabetes Metab.Syndr. 2019, 13, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G.; Solini, A.; Bonora, E.; Fondelli, C.; Orsi, E.; Nicolucci, A.; Penno, G.; RIACE Study Group. Chronic kidney disease in type 2 diabetes: Lessons from the renal insufficiency and cardiovascular events (RIACE) Italian multicentre study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Mottl, A.K.; Kwon, K.-S.; Mauer, M.; Mayer-Davis, E.J.; Hogan, S.L.; Kshirsagar, A.V. Normoalbuminuric diabetic kidney disease in the U.S. population. J. Diabetes Complicat. 2013, 27, 123–127. [Google Scholar] [CrossRef]
- Korbut, A.I.; Klimontov, V.V.; Vinogradov, I.V.; Romanov, V.V. Risk factors and urinary biomarkers of non-albuminuric and albuminuric chronic kidney disease in patients with type 2 diabetes. World J. Diabetes 2019, 10, 517–533. [Google Scholar] [CrossRef]
- Buyadaa, O.; Salim, A.; Morton, J.I.; Jandeleit-Dahm, K.; Magliano, D.J.; Shaw, J.E. Examining the factors contributing to the association between non-albuminuric CKD and a low rate of kidney function decline in diabetes. Ther. Adv. Endocrinol. Metab. 2022, 13, 20420188221083518. [Google Scholar] [CrossRef]
- Ekinci, E.I.; Jerums, G.; Skene, A.; Crammer, P.; Power, D.; Cheong, K.Y.; Panagiotopoulos, S.; McNeil, K.; Baker, S.T.; Fioretto, P.; et al. Renal structure in normoalbuminuric and albuminuric patients with type 2 diabetes and impaired renal function. Diabetes Care 2013, 36, 3620–3626. [Google Scholar] [CrossRef]
- Barutta, F.; Bellini, S.; Canepa, S.; Durazzo, M.; Gruden, G. Novel biomarkers of diabetic kidney disease: Current status and potential clinical application. Acta Diabetol. 2021, 58, 819–830. [Google Scholar] [CrossRef]
- Lin, Y.-C.; Chang, Y.-H.; Yang, S.-Y.; Wu, K.-D.; Chu, T.-S. Update of pathophysiology and management of diabetic kidney disease. J. Formos. Med. Assoc. 2018, 117, 662–675. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Chattopadhyay, M. Early urinary markers for diabetic and other kidney diseases. Curr. Drug Targets 2018, 19, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Klimontov, V.V.; Korbut, A.I.; Orlov, N.B.; Dashkin, M.V.; Konenkov, V.I. Multiplex bead array assay of a panel of circulating cytokines and growth factors in patients with albuminuric and non-albuminuric diabetic kidney disease. J. Clin. Med. 2020, 9, 3006. [Google Scholar] [CrossRef] [PubMed]
- Norden, A.G.; Lapsley, M.; Unwin, R.J. Urine retinol-binding protein 4: A functional biomarker of the proximal renal tubule. Adv. Clin. Chem. 2014, 63, 85–122. [Google Scholar] [CrossRef] [PubMed]
- Von Scholten, B.J.; Theilade, S.; Lajer, M.; Rossing, P. Urinary alpha- and Pi-glutathione s-transferases in adult patients with type 1 diabetes. Nephron Extra 2014, 4, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Branten, A.J.; Mulder, T.P.; Peters, W.H.; Assmann, K.J.; Wetzels, J.F. Urinary excretion of glutathione S transferases alpha and Pi in patients with proteinuria: Reflection of the site of tubular injury. Nephron 2000, 85, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Faustino, L.C.; Almeida, N.A.S.; Pereira, G.F.; Ramos, R.G.; Soares, R.M.; Morales, M.M.; Pazos-Moura, C.C.; Ortiga-Carvalho, T.M. Thyroid hormone and estradiol have overlapping effects on kidney glutathione S-transferase-α gene expression. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E787–E797. [Google Scholar] [CrossRef] [PubMed]
- Cawood, T.J.; Bashir, M.; Brady, J.; Murray, B.; Murray, P.T.; O’Shea, D. Urinary collagen IV and πGST: Potential biomarkers for detecting localized kidney injury in diabetes—A pilot study. Am. J. Nephrol. 2010, 32, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.-M.; Nikolic-Paterson, D.J.; Lan, H.Y. TGF-β: The master regulator of fibrosis. Nat. Rev. Nephrol. 2016, 12, 325–338. [Google Scholar] [CrossRef]
- Isaka, Y. Targeting TGF-β signaling in kidney fibrosis. Int. J. Mol. Sci. 2018, 19, 2532. [Google Scholar] [CrossRef] [PubMed]
- Bülow, R.D.; Boor, P. Extracellular matrix in kidney fibrosis: More than just a scaffold. J. Histochem. Cytochem. 2019, 67, 643–661. [Google Scholar] [CrossRef]
- Schanstra, J.P.; Zürbig, P.; Alkhalaf, A.; Argiles, A.; Bakker, S.J.L.; Beige, J.; Bilo, H.J.G.; Chatzikyrkou, C.; Dakna, M.; Dawson, J.; et al. Diagnosis and prediction of CKD progression by assessment of urinary peptides. J. Am. Soc. Nephrol. 2015, 26, 1999–2010. [Google Scholar] [CrossRef]
- Manson, S.R.; Austin, P.F.; Guo, Q.; Moore, K.H. BMP-7 signaling and its critical roles in kidney development, the responses to renal injury, and chronic kidney disease. Vitam. Horm. 2015, 99, 91–144. [Google Scholar] [CrossRef] [PubMed]
- Tsujimura, T.; Idei, M.; Yoshikawa, M.; Takase, O.; Hishikawa, K. Roles and regulation of bone morphogenetic protein-7 in kidney development and diseases. World J. Stem Cells 2016, 8, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Matsumoto, K.; Nakamura, T. HGF as a renotrophic and anti-fibrotic regulator in chronic renal disease. Front. Biosci. 2008, 13, 7072–7086. [Google Scholar] [CrossRef] [PubMed]
- Gaião, S.M.; de Carvalho Paiva, J.A.O. Biomarkers of renal recovery after acute kidney injury. Rev. Bras. Ter. Intensiv. 2017, 29, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Noordzij, M.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Sample size calculations. Nephron Clin. Pract. 2011, 118, c319–c323. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 27–53. [Google Scholar] [CrossRef]
- Steinhoff, J.S.; Lass, A.; Schupp, M. Biological functions of RBP4 and its relevance for human diseases. Front. Physiol. 2021, 12, 659977. [Google Scholar] [CrossRef]
- Xun, C.; Zhao, Y.; Wang, W.; Chen, C. Circulating RBP4 increase and its diagnosis of chronic kidney disease. Ann. Clin. Lab. Sci. 2018, 48, 205–207. [Google Scholar]
- Domingos, M.A.M.; Queiroz, M.; Lotufo, P.A.; Benseñor, I.J.; de Oliveira Titan, S.M. Serum RBP4 and CKD: Association with Insulin Resistance and Lipids. J. Diabetes Complicat. 2017, 31, 1132–1138. [Google Scholar] [CrossRef]
- Park, S.E.; Lee, N.S.; Park, J.W.; Rhee, E.-J.; Lee, W.-Y.; Oh, K.-W.; Park, S.-W.; Park, C.-Y.; Youn, B.-S. Association of urinary RBP4 with insulin resistance, inflammation, and microalbuminuria. Eur. J. Endocrinol. 2014, 171, 443–449. [Google Scholar] [CrossRef]
- Nielsen, R.; Christensen, E.I.; Birn, H. Megalin and cubilin in proximal tubule protein reabsorption: From experimental models to human disease. Kidney Int. 2016, 89, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.P.; Yokoi, H.; Kasahara, M.; Imamaki, H.; Ishii, A.; Kuwabara, T.; Koga, K.; Kato, Y.; Toda, N.; Ohno, S.; et al. Increase of total nephron albumin filtration and reabsorption in diabetic nephropathy. J. Am. Soc. Nephrol. 2017, 28, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Kurosaki, Y.; Imoto, A.; Kawakami, F.; Yokoba, M.; Takenaka, T.; Ichikawa, T.; Katagiri, M.; Ishii, N. Oxidative stress increases megalin expression in the renal proximal tubules during the normoalbuminuric stage of diabetes mellitus. Am. J. Physiol. Renal. Physiol. 2018, 314, F462–F470. [Google Scholar] [CrossRef]
- Jeon, H.J.; Shin, D.H.; Oh, J.; Kee, Y.K.; Park, J.Y.; Ko, K.; Lee, S. Urinary retinol-binding protein 4 is associated with renal function and rapid renal function decline in kidney transplant recipients. Transplant. Proc. 2022, 54, 362–366. [Google Scholar] [CrossRef]
- Tsai, Y.-L.; Liu, C.-W.; Huang, S.-F.; Yang, Y.-Y.; Lin, M.-W.; Huang, C.-C.; Li, T.-H.; Huang, Y.-H.; Hou, M.-C.; Lin, H.-C. Urinary fatty acid and retinol binding protein-4 predict CKD progression in severe NAFLD patients with hypertension: 4-year study with clinical and experimental approaches. Medicine 2020, 99, e18626. [Google Scholar] [CrossRef] [PubMed]
- Rivarola, E.W.; Moyses-Neto, M.; Dantas, M.; Da-Silva, C.G.; Volpini, R.; Coimbra, T.M. Transforming growth factor beta activity in urine of patients with type 2 diabetes and diabetic nephropathy. Braz. J. Med. Biol. Res. 1999, 32, 1525–1528. [Google Scholar] [CrossRef] [PubMed]
- Bondar’, I.A.; Klimontov, V.V.; Nadeev, A.P. Urinary excretion of proinflammatory cytokines and transforming growth factor beta at early stages of diabetic nephropathy. Ter. Arkhiv 2008, 80, 52–56. [Google Scholar]
- Bondar’, I.A.; Klimontov, V.V.; Parfent’eva, E.M.; Romanov, V.V.; Nadeev, A.P. Urinary excretion of fibrogenic and antifibrotic growth factors in type 1 diabetic patients: The interrelationship with diabetic nephropathy. Ter. Arkhiv 2012, 84, 36–40. [Google Scholar]
- Sato, H.; Iwano, M.; Akai, Y.; Kurioka, H.; Kubo, A.; Yamaguchi, T.; Hirata, E.; Kanauchi, M.; Dohi, K. Increased excretion of urinary transforming growth factor beta 1 in patients with diabetic nephropathy. Am. J. Nephrol. 1998, 18, 490–494. [Google Scholar] [CrossRef]
- Monteiro de Freitas, A.S.; Coimbra, T.M.; Costa, R.S.; Baroni, E.A. Urinary transforming growth factor-beta (TGF-beta) excretion and renal production of TGF-beta in rats with subtotal renal ablation: Effect of enalapril and nifedipine. Nephron 1998, 78, 302–309. [Google Scholar] [CrossRef]
- Esmatjes, E.; Flores, L.; Iñigo, P.; Lario, S.; Ruilope, L.M.; Campistol, J.M. Effect of losartan on TGF-Beta1 and urinary albumin excretion in patients with type 2 diabetes mellitus and microalbuminuria. Nephrol. Dial. Transplant. 2001, 16, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Houlihan, C.A.; Akdeniz, A.; Tsalamandris, C.; Cooper, M.E.; Jerums, G.; Gilbert, R.E. Urinary transforming growth factor-beta excretion in patients with hypertension, type 2 diabetes, and elevated albumin excretion rate: Effects of angiotensin receptor blockade and sodium restriction. Diabetes Care 2002, 25, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Inukai, T.; Fujiwara, Y.; Tayama, K.; Aso, Y.; Takemura, Y. Serum levels of carboxy-terminal propeptide of human type I procollagen are an indicator for the progression of diabetic nephropathy in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2000, 48, 23–28. [Google Scholar] [CrossRef]
- Klimontov, V.V.; Eremenko, N.V.; Myakina, N.E.; Fazullina, O.N. Cystatin C and collagen type IV in diagnostics of chronic kidney disease in type 2 diabetic patients. Diabetes Mellit. 2015, 18, 87–93. [Google Scholar] [CrossRef]
- Nakamura, T.; Ushiyama, C.; Suzuki, S.; Shimada, N.; Sekizuka, K.; Ebihara, L.; Koide, H. Effect of troglitazone on urinary albumin excretion and serum type IV collagen concentrations in type 2 diabetic patients with microalbuminuria or macroalbuminuria. Diabet. Med. 2001, 18, 308–313. [Google Scholar] [CrossRef]
- Nie, J.-M.; Li, H.-F. Therapeutic effects of salvia miltiorrhiza injection combined with telmisartan in patients with diabetic nephropathy by influencing collagen IV and fibronectin: A case-control study. Exp. Ther. Med. 2018, 16, 3405–3412. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, N.; Abe, H.; Tominaga, T.; Nakahara, K.; Ito, Y.; Okumoto, Y.; Kim, J.; Kitakaze, M.; Doi, T. Risk factors for chronic kidney disease in Japan: A community-based study. BMC Nephrol. 2009, 10, 34. [Google Scholar] [CrossRef]
- Kishi, F.; Nagai, K.; Takamatsu, N.; Tominaga, T.; Tamaki, M.; Shibata, E.; Murakami, T.; Kishi, S.; Abe, H.; Koezuka, Y.; et al. Urinary type IV collagen excretion is involved in the decline in estimated glomerular filtration rate in the Japanese general population without diabetes: A 5-year observational study. PLoS ONE 2018, 13, e0195523. [Google Scholar] [CrossRef]
- Hung, P.-H.; Hsu, Y.-C.; Chen, T.-H.; Lin, C.-L. Recent advances in diabetic kidney diseases: From kidney injury to kidney fibrosis. Int. J. Mol. Sci. 2021, 22, 11857. [Google Scholar] [CrossRef]
- Koye, D.N.; Magliano, D.J.; Reid, C.M.; Jepson, C.; Feldman, H.I.; Herman, W.H.; Shaw, J.E. Risk of progression of nonalbuminuric CKD to end-stage kidney disease in people with diabetes: The CRIC (Chronic Renal Insufficiency Cohort) study. Am. J. Kidney Dis. 2018, 72, 653–661. [Google Scholar] [CrossRef]
- Go, A.S.; Yang, J.; Tan, T.C.; Cabrera, C.S.; Stefansson, B.V.; Greasley, P.J.; Ordonez, J.D.; Kaiser Permanente Northern California. CKD outcomes study contemporary rates and predictors of fast progression of chronic kidney disease in adults with and without diabetes mellitus. BMC Nephrol. 2018, 19, 146. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, Y.; Yan, R.; Liang, L.; Zhou, X.; Liu, H.; Zhang, X.; Mao, Y.; Peng, W.; Xiao, Y.; et al. BMP-7 inhibits renal fibrosis in diabetic nephropathy via MiR-21 downregulation. Life Sci. 2019, 238, 116957. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.-M.; Chung, A.C.K.; Lan, H.Y. Role of the TGF-β/BMP-7/Smad pathways in renal diseases. Clin. Sci. 2013, 124, 243–254. [Google Scholar] [CrossRef]
- Lv, W.; Booz, G.W.; Wang, Y.; Fan, F.; Roman, R.J. Inflammation and renal fibrosis: Recent developments on key signaling molecules as potential therapeutic targets. Eur. J. Pharmacol. 2018, 820, 65–76. [Google Scholar] [CrossRef]
- Lim, A.I.; Chan, L.Y.Y.; Tang, S.C.W.; Yiu, W.H.; Li, R.; Lai, K.N.; Leung, J.C.K. BMP-7 Represses albumin-induced chemokine synthesis in kidney tubular epithelial cells through destabilization of NF-ΚB-inducing kinase. Immunol. Cell Biol. 2014, 92, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.H.; Chang, C.K.; Cheng, M.F.; Lin, H.J.; Cheng, J.T. Decrease of bone morphogenetic protein-7 (BMP-7) and its type II receptor (BMP-RII) in kidney of type 1-like diabetic rats. Horm. Metab. Res. 2009, 41, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Jin, M.-Y.; Liu, D.-W.; Wei, L. Bone morphogenetic protein (BMP) 7 expression is regulated by the E3 ligase UBE4A in diabetic nephropathy. Arch. Physiol. Biochem. 2020, 126, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Ivanac-Janković, R.; Ćorić, M.; Furić-Čunko, V.; Lovičić, V.; Bašić-Jukić, N.; Kes, P. BMP-7 protein expression is downregulated in human diabetic nephropathy. Acta Clin. Croat. 2015, 54, 164–168. [Google Scholar]
- Ohigashi, M.; Kobara, M.; Takahashi, T.; Toba, H.; Wada, T.; Nakata, T. Pitavastatin suppresses hyperglycaemia-induced podocyte injury via bone morphogenetic protein-7 preservation. Clin. Exp. Pharmacol. Physiol. 2017, 44, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Ohigashi, M.; Imai, N.; Toba, H.; Kobara, M.; Nakata, T. Pitavastatin exhibits protective effects on podocytes accompanied by BMP-7 up-regulation and rho suppression. Pharmacology 2016, 97, 265–276. [Google Scholar] [CrossRef]
- Mizuno, S.; Nakamura, T. Suppressions of chronic glomerular injuries and TGF-beta 1 production by HGF in attenuation of murine diabetic nephropathy. Am. J. Physiol. Renal. Physiol. 2004, 286, F134–F143. [Google Scholar] [CrossRef]
- Zhang, C.; Hou, B.; Yu, S.; Chen, Q.; Zhang, N.; Li, H. HGF alleviates high glucose-induced injury in podocytes by GSK3β inhibition and autophagy restoration. Biochim. Biophys. Acta 2016, 1863, 2690–2699. [Google Scholar] [CrossRef]
- Hou, B.; Li, Y.; Li, X.; Zhang, C.; Zhao, Z.; Chen, Q.; Zhang, N.; Li, H. HGF protected against diabetic nephropathy via autophagy-lysosome pathway in podocyte by modulating PI3K/Akt-GSK3β-TFEB axis. Cell. Signal. 2020, 75, 109744. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, T.; Karasawa, K.; Nitta, K. The role of caveolae on albumin passage through glomerular endothelial and epithelial cells: The new etiology of urinary albumin excretion. Contrib. Nephrol. 2018, 195, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Molitoris, B.A.; Sandoval, R.M.; Yadav, S.P.S.; Wagner, M.C. Albumin uptake and processing by the proximal tubule: Physiological, pathological, and therapeutic implications. Physiol. Rev. 2022, 102, 1625–1667. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.; Blomhoff, R. Retinol, retinoic acid, and retinol-binding protein 4 are differentially associated with cardiovascular disease, type 2 diabetes, and obesity: An overview of human studies. Adv. Nutr. 2020, 11, 644–666. [Google Scholar] [CrossRef]
- Ren, H.; Ma, X.; Shao, Y.; Han, J.; Yang, M.; Wang, Q. Correlation between serum MiR-154-5p and osteocalcin in males and postmenopausal females of type 2 diabetes with different urinary albumin creatinine ratios. Front. Endocrinol. 2019, 10, 542. [Google Scholar] [CrossRef]
- Okonogi, H.; Nishimura, M.; Utsunomiya, Y.; Hamaguchi, K.; Tsuchida, H.; Miura, Y.; Suzuki, S.; Kawamura, T.; Hosoya, T.; Yamada, K. Urinary type IV collagen excretion reflects renal morphological alterations and type IV collagen expression in patients with type 2 diabetes mellitus. Clin. Nephrol. 2001, 55, 357–364. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Group | eGFR | UACR | N |
|---|---|---|---|
| NRF/NA | ≥60 mL/min/1.73 m2 | <3.0 mg/mmol | 35 |
| DRF/NA | <60 mL/min/1.73 m2 | ≥3.0 mg/mmol | 35 |
| NRF/EA | ≥60 mL/min/1.73 m2 | <3.0 mg/mmol | 35 |
| DRF/EA | <60 mL/min/1.73 m2 | ≥3.0 mg/mmol | 35 |
| Parameter | NRF/NA | DRF/NA | NRF/EA | DRF/EA |
|---|---|---|---|---|
| N | 35 | 35 | 35 | 35 |
| Age, years | 64 (58–71) | 65 (58–67) | 64 (58–68) | 66 (58–72) |
| Sex, m/f (n, %) | 12/23 (34.3/65.7) | 12/23 (34.3/65.7) | 13/22 (37.1/62.9) | 12/23 (34.3/65.7) |
| Body weight, kg | 88 (75–98) | 95 (80–104) | 95 (80–108) | 88 (73–100) |
| BMI, kg/m2 | 34.4 (28.1–38) | 34.1 (30.1–37.5) | 33.3 (30.8–39.6) | 32.2 (28.8–36.2) |
| Obesity, n (%) | 23 (65.7) | 26 (74.3) | 27 (77.1) | 25 (71.4) |
| Waist circumference, cm | 110 (99–130) | 115 (106–123) | 110 (105–124) | 107 (104–112) |
| WHR | 0.97 (0.93–1.10) | 1.05 (0.90–1.10) | 1.00 (0.93–1.09) | 1.00 (0.91–1.07) |
| Current smokers, n (%) | 3 (8.6) | 4 (11.4) | 5 (14.3) | 3 (8.6) |
| Duration of T2D, years | 12 (10–17) | 13 (10–20) | 14 (10–17) | 14.5(11–18) |
| Insulin, n (%) | 23 (65.7) | 23 (65.7) | 23 (65.7) | 26 (74.8) |
| Metformin, n (%) | 28 (80.0) | 22 (62.8) | 24 (68.6) | 20 (57.1) |
| SU, n (%) | 9 (25.7) | 14 (40.8) | 14 (40.0) | 11 (31.4) |
| ACE inhibitors or ARBs, n (%) | 24 (68.6) | 29 (82.9) | 28 (80.0) | 30 (85.7) |
| Statins, n (%) | 14 (40.0) | 26 (74.3) | 17 (48.6) | 19 (54.3) |
| HbA1C, % | 8.48 (7.5–10.3) | 8.8 (7.88–9.81) | 9.37 (8.17–11.8) § | 8.39 (7.46–9.53) |
| HbA1C, mmol/mol | 69.2 (58.5–88.8) | 72.7 (62.6–83.7) | 78.9 (65.8–105) § | 68.1 (58–80.6) |
| CKD G1/G2/G3a/G3b, n (%) | 10/25/0/0 (28.6/71.4/0/0) | 0/0/23/12 (0/0/65.7/34.3) | 3/32/0/0 (8.6/91.4/0/0) | 0/0/23/12 (0/0/65.7/34.3) |
| eGFR, mL/min/1.73 m2 | 84 (71–94) | 51 (45–55) *** | 70 (65–78) | 51 (43–54) *** |
| UACR, mg/mmol | 0.6 (0.3–0.9) | 0.65 (0.45–0.9) | 10.5 (6.3–36.7) ### | 12.0 (6.3–80.6) ### |
| CKD A1/A2/A3, n (%) | 35/0/0 (100/0/0) | 35/0/0 (100/0/0) | 0/23/12 (0/65.7/34.3) | 0/25/10 (0/71.4/28.6) |
| Protein excretion, g/day | 0.07 (0.05–0.1) | 0.07 (0.05–0.15) | 0.17 (0.09–0.53) ### | 0.2 (0.13–0.52) ### |
| Diabetic retinopathy, n (%) | 19 (54.3) | 19 (54.3) | 23 (65.7) | 24 (65.7) |
| Arterial hypertension, n (%) | 33 (94.3) | 35 (100) | 34 (97.1) | 35 (100) |
| Myocardial infarction in medical history, n (%) | 4 (11.4) | 7 (20.0) | 5 (14.3) | 11 (31.4) |
| Chronic heart failure NYHA class III/IV, n (%) | 0 (0) | 2 (5.7) | 5 (14.3) | 1 (2.9) |
| Cerebrovascular event in medical history, n (%) | 1 (2.9) | 7 (20.0) | 3 (8.6) | 3 (8.6) |
| Peripheral artery disease, n (%) | 19 (54.3) | 25 (71.4) | 22 (62.9) | 25 (71.4) |
| Parameter | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| Urinary RBP-4, μg/mmol | 1.11 | 1.02–1.21 | 0.02 |
| Urinary Col1, pg/mmol | 1.16 | 1.01–1.32 | 0.03 |
| Urinary HGF, ng/mmol | 1.08 | 1.01–1.15 | 0.03 |
| Parameter | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| NRF/EA | |||
| Urinary RBP-4, μg/mmol | 1.54 | 1.07–2.22 | 0.02 |
| DRF/EA | |||
| Urinary RBP-4, μg/mmol | 1.36 | 1.02–1.83 | 0.04 |
| Urinary Col1, pg/mmol | 1.43 | 1.03–2.00 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korbut, A.I.; Romanov, V.V.; Klimontov, V.V. Urinary Markers of Tubular Injury and Renal Fibrosis in Patients with Type 2 Diabetes and Different Phenotypes of Chronic Kidney Disease. Life 2023, 13, 343. https://doi.org/10.3390/life13020343
Korbut AI, Romanov VV, Klimontov VV. Urinary Markers of Tubular Injury and Renal Fibrosis in Patients with Type 2 Diabetes and Different Phenotypes of Chronic Kidney Disease. Life. 2023; 13(2):343. https://doi.org/10.3390/life13020343
Chicago/Turabian StyleKorbut, Anton I., Vyacheslav V. Romanov, and Vadim V. Klimontov. 2023. "Urinary Markers of Tubular Injury and Renal Fibrosis in Patients with Type 2 Diabetes and Different Phenotypes of Chronic Kidney Disease" Life 13, no. 2: 343. https://doi.org/10.3390/life13020343
APA StyleKorbut, A. I., Romanov, V. V., & Klimontov, V. V. (2023). Urinary Markers of Tubular Injury and Renal Fibrosis in Patients with Type 2 Diabetes and Different Phenotypes of Chronic Kidney Disease. Life, 13(2), 343. https://doi.org/10.3390/life13020343