
Complicated Relationships between Anterior and Condylar Guidance and Their Clinical Implications—Comparison by Cone Beam Computed Tomography and Electronic Axiography—An Observational Cohort Cross-Sectional Study



Abstract
1. Introduction
1.1. Objectives
- The protrusive movement of the mandible does correlate with the TMJ anatomy.
- The protrusive movement of the mandible does not correlate with the incisal features.
- The position and relationship of upper and lower permanent incisors do not have a direct and significant effect on the TMJ morphology in young adults.
1.2. Clinical Implications
2. Materials and Methods
2.1. Study Participants
2.2. Study Protocol
2.3. Statistical Analysis
2.4. Limitations
3. Results
4. Discussion
5. Conclusions
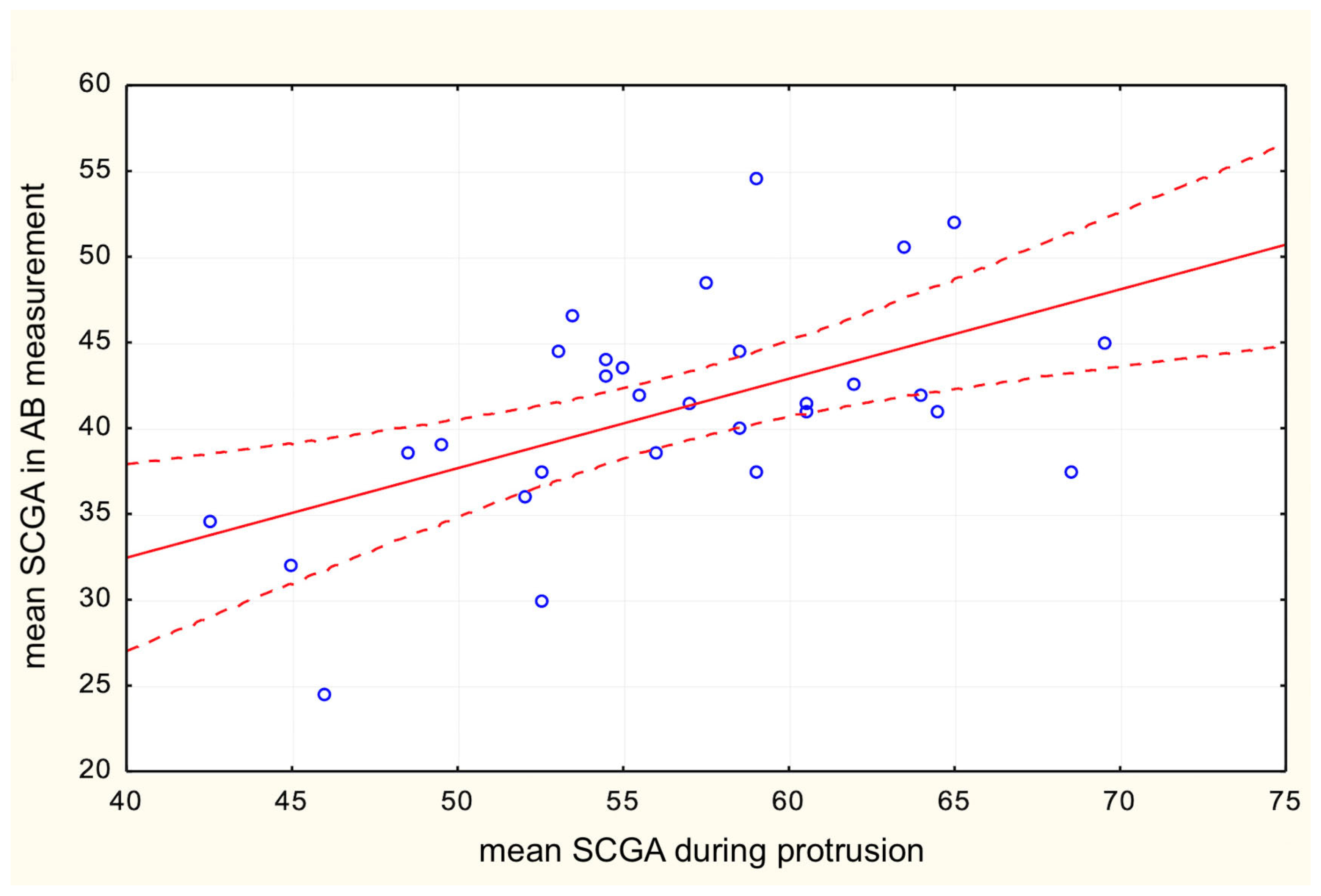
- The SCGA, during the protrusive movement recorded by the axiograph, is correlated with the features of the articular fossa, such as the height and inclination angle of the articular tubercle, suggesting that the TMJ anatomy dictates its function.
- The SCGA, during the protrusive movement, is not correlated with the relations between the incisors, pointing towards the conclusion that the TMJ function does not depend on the incisal features (IGA, interincisal angle, overbite, and overjet).
- Incisal relationships of permanent teeth such as overbite, overjet, IGA, and interincisal angle do not correlate with TMJ anatomy; therefore, they do not affect TMJ formation in young adults in regard to analyzed study group.
- The AB line is the most reliable reference for measuring the SCGA on CBCT.
- While processed foods contributed significantly to the change in the bite, neither a soft diet nor a change in the bite modified the structure of the temporomandibular joint, either now or in antiquity.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| TMJ | Temporomandibular joint |
| TMD | Temporomandibular disorders |
| IGA | Incisal guidance angle |
| CBCT | Cone beam computed tomography |
| SCGA | Sagittal condylar guidance angle |
| SCG | Sagittal condylar guidance |
| IG | Incisal guidance |
| MIP | Maximum intercuspation position |
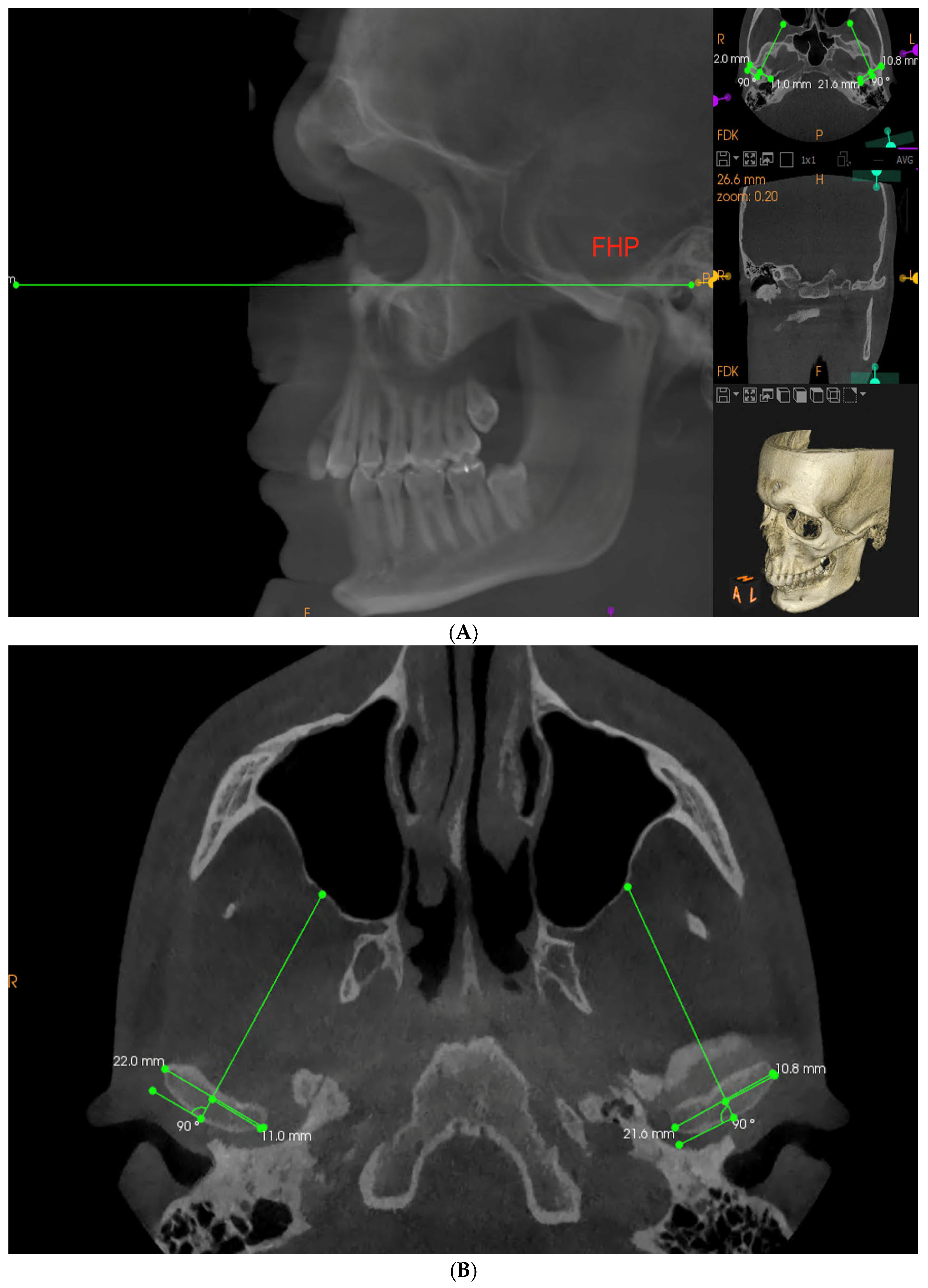
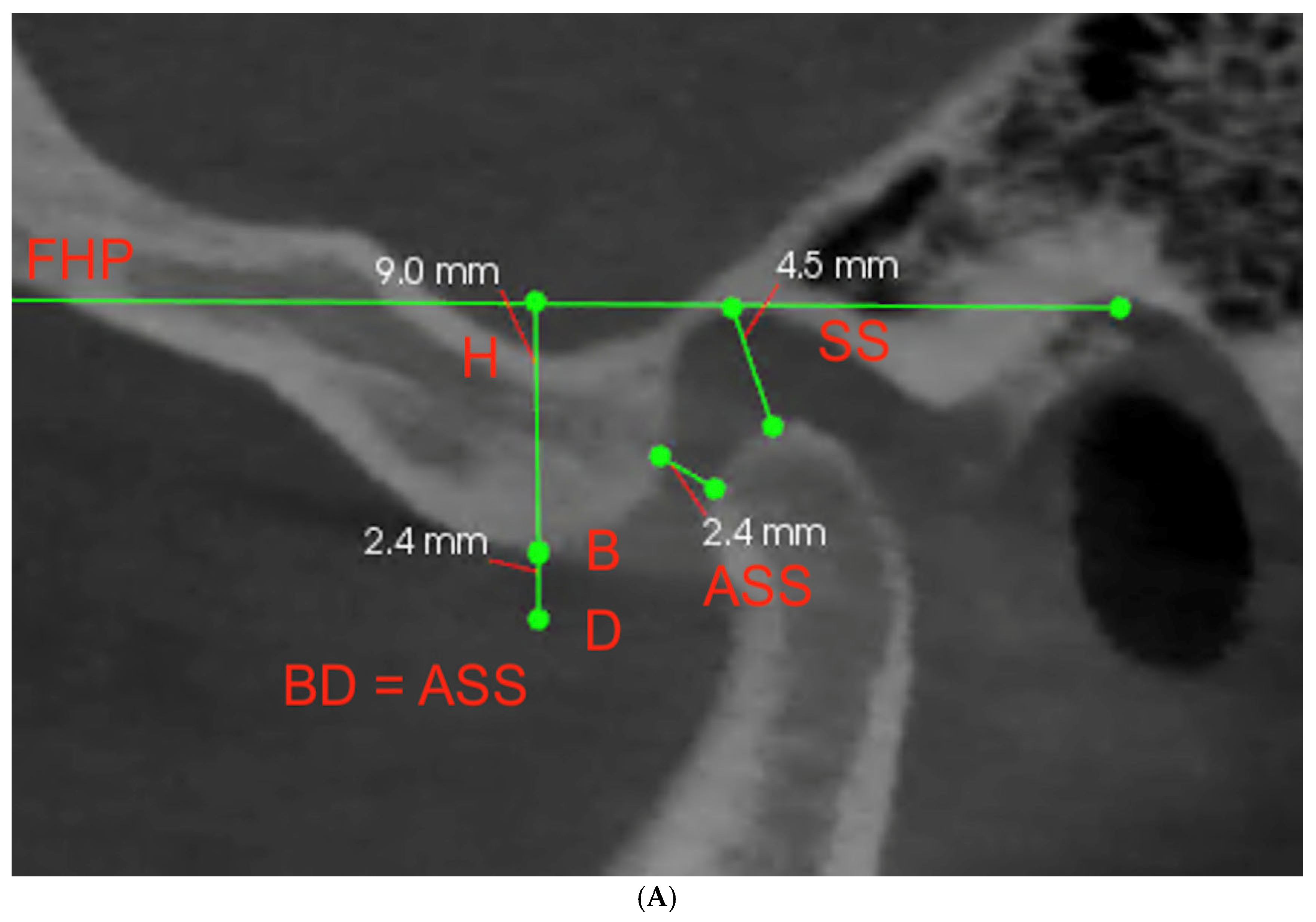
| FHP | Frankfort horizontal plane |
| ASS | Antero-superior space |
| SS | Superior space |
References
- Kubein-Meesenburg, D.; Fanghänel, J.; Ihlow, D.; Lotzmann, U.; Hahn, W.; Thieme, K.M.; Proff, P.; Gedrange, T.; Nägerl, H. Functional state of the mandible and rolling–gliding characteristics in the TMJ. Ann. Anat. Anat. Anz. 2007, 189, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Gilboa, I.; Cardash, H.S.; Kaffe, I.; Gross, M.D. Condylar guidance: Correlation between articular morphology and panoramic radiographic images in dry human skulls. J. Prosthet. Dent. 2008, 99, 477–482. [Google Scholar] [CrossRef]
- Shreshta, P.; Jain, V.; Bhalla, A.; Pruthi, G. A comparative study to measure the condylar guidance by the radiographic and clinical methods. J. Adv. Prosthodont. 2012, 4, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Tannamala, P.K.; Pulagam, M.; Pottem, S.R.; Swapna, B. Condylar Guidance: Correlation between Protrusive Interocclusal Record and Panoramic Radiographic Image: A Pilot Study. J. Prosthodont. 2012, 21, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Muddugangadhar, B.C.; Mawani, D.; Das, A.; Mukhopadhyay, A. Comparative evaluation of condylar inclination in dentulous subjects as determined by two radiographic methods: Orthopantomograph and cone-beam computed tomography—An in vivo study. J. Indian Prosthodont. Soc. 2019, 19, 113–119. [Google Scholar] [CrossRef]
- Seth, V.; Kamath, P.; Vaidya, N. Cone beam computed tomography: Third eye in diagnosis and treatment planning. Int. J. Orthod. 2012, 23, 17–22. [Google Scholar]
- Utz, K.-H.; Muller, F.; Luckerath, W.; Fuss, E.; Koeck, B. Accuracy of check-bite registration and centric condylar position. J. Oral Rehabil. 2002, 29, 458–466. [Google Scholar] [CrossRef]
- Shah, N.; Hegde, C.; Prasad, K.D. A clinico-radiographic analysis of sagittal condylar guidance determined by protrusive interocclusal registration and panoramic radiographic images in humans. Contemp. Clin. Dent. 2012, 3, 383–387. [Google Scholar] [CrossRef]
- Price, R.B.; Kolling, J.N.; Clayton, J.A. Effects of changes in articulator settings on generated occlusal tracings. Part I: Condylar inclination and progressive side shift settings. J. Prosthet. Dent. 1991, 65, 237–243. [Google Scholar] [CrossRef]
- Lundeen, H.C.; Shryock, E.F.; Gibbs, C.H. An evaluation of mandibular border movements: Their character and significance. J. Prosthet. Dent. 1978, 40, 442–452. [Google Scholar] [CrossRef]
- Brose, M.O.; Tanquist, R.A. The influence of anterior coupling on mandibular movement. J. Prosthet. Dent. 1987, 57, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Zoghby, A.E.; Ré, J.-P.; Perez, C. Functional harmony between the sagittal condylar path inclination and the anterior guidance inclination. Int. J. Stomatol. Occlusion Med. 2009, 2, 131–136. [Google Scholar] [CrossRef]
- Broderson, S.P. Anterior guidance—The key to successful occlusal treatment. J. Prosthet. Dent. 1978, 39, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, L.B.; Campbell, S.D. Evaluation of the relationship between anterior and posterior functionally disclusive angles. Part I: Literature review, instrumentation, and reproducibility. J. Prosthet. Dent. 1990, 63, 395–403. [Google Scholar] [CrossRef]
- Pelletier, L.B.; Campbell, S.D. Evaluation of the relationship between anterior and posterior functionally disclusive angles. Part II: Study of a population. J. Prosthet. Dent. 1990, 63, 536–540. [Google Scholar] [CrossRef]
- E Dawson, P. Determining the determinants of occlusion. Int. J. Periodontics Restor. Dent. 1983, 3, 8–21. [Google Scholar]
- Kepron, D. Experiences with Modern Occlusal Concepts. Dent. Clin. North Am. 1971, 15, 595–610. [Google Scholar] [CrossRef]
- Thompson, J.R. Abnormal function of the temporomandibular joints and related musculature. Orthodontic implications. Part II. Angle Orthod. 1986, 56, 181–195. [Google Scholar]
- Han, S.; Shin, S.M.; Choi, Y.-S.; Kim, S.Y.; Ko, C.-C.; Kim, Y.-I. Morphometric analysis for evaluating the relation between incisal guidance angle, occlusal plane angle, and functional temporomandibular joint shape variation. Acta Odontol. Scand. 2018, 76, 287–293. [Google Scholar] [CrossRef]
- Luca, L.; Manfredini, D.; Arveda, N.; Rossi, L.; Siciliani, G. A cone-beam computerized tomography assessment of the relationship between upper incisors inclination and articular eminence features in orthodontically untreated patients with different facial type. J. World Fed. Orthod. 2016, 5, 56–63. [Google Scholar] [CrossRef]
- Li, Y.; Zhou, W.; Wu, Y.; Dai, H.; Zhou, J. The relation between incisal guidance angle and the growth and development of tem-poromandibular joint: A multi-cross-sectional retrospective study. BMC Oral Health 2021, 21, 380. [Google Scholar] [CrossRef]
- Laplanche, O.; Orthlieb, J.D.; Laurent, M.; Vyslozil, O.; Dutour, O. Evolution of the incisal relationship in a Central European population (1870/1970). Int. J. Stomatol. Occlusion Med. 2010, 3, 2–9. [Google Scholar] [CrossRef]
- Kaifu, Y.; Kasai, K.; Townsend, G.C.; Richards, L.C. Tooth wear and the design of the human dentition: A perspective from evolutionary medicine. Am. J. Phys. Anthr. 2003, 122, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Brace, C.L. Egg on the Face, f in the Mouth, and the Overbite. Am. Anthropol. 1986, 88, 695–697. [Google Scholar] [CrossRef]
- Sülün, T.; Cemgil, T.; Duc, J.-M.P.; Rammelsberg, P.; Jäger, L.; Gernet, W. Morphology of the mandibular fossa and inclination of the articular eminence in patients with internal derangement and in symptom-free volunteers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 98–107. [Google Scholar] [CrossRef]
- Lei, J.; Liu, M.-Q.; Yap, A.U.J.; Fu, K.-Y. Condylar subchondral formation of cortical bone in adolescents and young adults. Br. J. Oral Maxillofac. Surg. 2013, 51, 63–68. [Google Scholar] [CrossRef]
- Osiewicz, M.A.; Lobbezoo, F.; Loster, B.W.; Wilkosz, M.; Naeije, M.; Ohrbach, R. Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD)—The Polish version of a dual-axis system for the diagnosis of TMD. RDC/TMD Form. J. Stomatol. 2013, 66, 576–649. [Google Scholar] [CrossRef]
- Chae, J.-M.; Park, J.H.; Tai, K.; Mizutani, K.; Uzuka, S.; Miyashita, W.; Seo, H.Y. Evaluation of condyle-fossa relationships in adolescents with various skeletal patterns using cone-beam computed tomography. Angle Orthod. 2020, 90, 224–232. [Google Scholar] [CrossRef]
- Celebic, A.; Alajbeg, Z.I.; Kraljevic-Simunkovic, S.; Valentic-Peruzovic, M. Influence of different condylar and incisal guidance ratios to the activity of anterior and posterior temporal muscle. Arch. Oral Biol. 2007, 52, 142–148. [Google Scholar] [CrossRef]
- Bapelle, M.; Dubromez, J.; Savoldelli, C.; Tillier, Y.; Ehrmann, E. Modjaw® device: Analysis of mandibular kinematics recorded for a group of asymptomatic subjects. Cranio® 2021, 1–7. [Google Scholar] [CrossRef]
- Mongini, F. Remodelling of the mandibular condyle in the adult and its relationship to the condition of the dental arches. Cells Tissues Organs 1972, 82, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Mongini, F. Dental abrasion as a factor in remodeling of the mandibular condyle. Cells Tissues Organs 1975, 92, 292–300. [Google Scholar] [CrossRef]
- Katsavrias, E.G.; Halazonetis, D. Condyle and fossa shape in Class II and Class III skeletal patterns: A morphometric tomographic study. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Tanne, K.; Tanaka, E.; Sakuda, M. Stress distributions in the TMJ during clenching in patients with vertical discrepancies of the craniofacial complex. J. Orofac. Pain 1995, 9, 153–160. [Google Scholar] [PubMed]
- Nickel, J.C.; McLachlan, K.R.; Smith, D.M. Eminence Development of the Postnatal Human Temporomandibular Joint. J. Dent. Res. 1988, 67, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Blasi, D.E.; Moran, S.; Moisik, S.R.; Widmer, P.; Dediu, D.; Bickel, B. Human sound systems are shaped by post-Neolithic changes in bite configuration. Science 2019, 363, 6432. [Google Scholar] [CrossRef]
- Kranjčić, J.; Hunt, D.; Peršić Kiršić, S.; Kovačić, I.; Vukšić, J.; Vojvodić, D. Articular Eminence Morphology of American Historic and Contemporary Populations. Acta Stomatol. Croat. 2021, 55, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, C.; John, M.T.; Drangsholt, M.T.; A Mancl, L. Relationship between overbite/overjet and clicking or crepitus of the temporomandibular joint. J. Orofac. Pain 2005, 19, 218–225. [Google Scholar]
- Manfredini, D.; Lombardo, L.; Siciliani, G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: End of an era? J. Oral Rehabil. 2017, 44, 908–923. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, Ł.; Pollis, M.; Żółtowska, A.; Manfredini, D. Gut Bless Your Pain—Roles of the Gut Microbiota, Sleep, and Melatonin in Chronic Orofacial Pain and Depression. Biomedicines 2022, 10, 1528. [Google Scholar] [CrossRef] [PubMed]
- Nowak, Z.; Chęciński, M.; Nitecka-Buchta, A.; Bulanda, S.; Ilczuk-Rypuła, D.; Postek-Stefańska, L.; Baron, S. Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 9552. [Google Scholar] [CrossRef] [PubMed]
- Chęciński, M.; Chęcińska, K.; Turosz, N.; Kamińska, M.; Nowak, Z.; Sikora, M.; Chlubek, D. Autologous Stem Cells Transplants in the Treatment of Temporomandibular Joints Disorders: A Systematic Review and Meta-Analysis of Clinical Trials. Cells 2022, 11, 2709. [Google Scholar] [CrossRef]
- Turosz, N.; Chęcińska, K.; Chęciński, M.; Kamińska, M.; Nowak, Z.; Sikora, M.; Chlubek, D. A Scoping Review of the Use of Pioglitazone in the Treatment of Temporo-Mandibular Joint Arthritis. Int. J. Environ. Res. Public Health 2022, 19, 16518. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.D.; Del Mondo, D.D.; Russo, D.D.; Cervino, G.D.; D’Amico, C.D.; Fiorillo, L.D. Stem Cells in Temporomandibular Joint Engineering: State of Art and Future Persectives. J. Craniofacial Surg. 2022, 33, 2181–2187. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Nucci, L.; Giudice, A.; Calafiore, D.; Marotta, N.; Minervini, G.; D’Apuzzo, F.; Ammendolia, A.; Perillo, L.; de Sire, A. Efficacy of conservative approaches on pain relief in patients with temporomandibular joint disorders: A systematic review with network meta-analysis. Cranio® 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Tinastepe, N.; Oral, K. Investigation of the Relationship between Increased Vertical Overlap with Minimum Horizontal Overlap and the Signs of Temporomandibular Disorders. J. Prosthodont. 2015, 24, 463–468. [Google Scholar] [CrossRef]
- Williamson, E.; Lundquist, D. Anterior guidance: Its effect on electromyographic activity of the temporal and masseter muscles. J. Prosthet. Dent. 1983, 49, 816–823. [Google Scholar] [CrossRef]
- Lukic, N.; Saxer, T.; Hou, M.; Wojczyńska, A.Z.; Gallo, L.M.; Colombo, V. Short-term effects of NTI-tss and Michigan splint on nocturnal jaw muscle activity: A pilot study. Clin. Exp. Dent. Res. 2021, 7, 323–330. [Google Scholar] [CrossRef]
- MacDonald, J.W.C.; Hannam, A.G. Relationship between occlusal contacts and jaw-closing muscle activity during tooth clenching: Part I. J. Prosthet. Dent. 1984, 52, 718–729. [Google Scholar] [CrossRef]
- Kahn, J.; Tallents, R.H.; Katzberg, R.W.; Ross, M.E.; Murphy, W.C. Prevalence of dental occlusal variables and intraarticular temporomandibular disorders: Molar relationship, lateral guidance, and nonworking side contacts. J. Prosthet. Dent. 1999, 82, 410–415. [Google Scholar] [CrossRef]
- Rompré, P.; Daigle-Landry, D.; Guitard, F.; Montplaisir, J.; Lavigne, G. Identification of a Sleep Bruxism Subgroup with a Higher Risk of Pain. J. Dent. Res. 2007, 86, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Olliver, S.; Broadbent, J.; Thomson, W.; Farella, M. Occlusal Features and TMJ Clicking: A 30-Year Evaluation from a Cohort Study. J. Dent. Res. 2020, 99, 1245–1251. [Google Scholar] [CrossRef]
- Mohlin, B.O.; Derweduwen, K.; Pilley, R.; Kingdon, A.; Shaw, W.C.; Kenealy, P. Malocclusion and temporomandibular disorder: A comparison of adolescents with moderate to severe dysfunction with those without signs and symptoms of temporoman-dibular disorder and their further development to 30 years of age. Angle Orthod. 2004, 74, 319–327. [Google Scholar] [PubMed]
- Ma, Q.; Bimal, P.; Mei, L.; Olliver, S.; Farella, M.; Li, H. Temporomandibular condylar morphology in diverse maxillary-mandibular skeletal patterns: A 3-dimensional cone-beam computed tomography study. J. Am. Dent. Assoc. 2018, 149, 589–598. [Google Scholar] [CrossRef]
- Nickel, J.; Iwasaki, L.; Gonzalez, Y.; Gallo, L.; Yao, H. Mechanobehavior and Ontogenesis of the Temporomandibular Joint. J. Dent. Res. 2018, 97, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Segù, M.; Arveda, N.; Lombardo, L.; Siciliani, G.; Rossi, A.; Guarda-Nardini, L. Temporomandibular Joint Disorders in Patients With Different Facial Morphology. A Systematic Review of the Literature. J. Oral Maxillofac. Surg. 2015, 74, 29–46. [Google Scholar] [CrossRef] [PubMed]
- Rowlerson, A.; Raoul, G.; Daniel, Y.; Close, J.; Maurage, C.-A.; Ferri, J.; Sciote, J.J. Fiber-type differences in masseter muscle associated with different facial morphologies. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Cifter, E.D. Effects of Occlusal Plane Inclination on the Temporomandibular Joint Stress Distribution: A Three-Dimensional Finite Element Analysis. Int. J. Clin. Pract. 2022, 2022, 2171049. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n | Mean | SD | r (X, Y) | r2 | p |
|---|---|---|---|---|---|---|
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | 0.496253 | 0.246267 | 0.005285 |
| Mean vertical height of the TMJ fossa | 8.2467 | 0.8467 | ||||
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | 0.551815 | 0.304500 | 0.001571 |
| Mean SCGA in AB measurement | 41.1167 | 6.2694 | ||||
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | 0.532373 | 0.283421 | 0.002459 |
| Mean SCGA in AT measurement | 52.4167 | 7.9525 | ||||
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | 0.449854 | 0.202368 | 0.012623 |
| Mean SCGA in CD measurement | 36.4833 | 5.8509 |
| Variables | n | Mean | SD | r (X, Y) | r2 | p |
|---|---|---|---|---|---|---|
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | −0.173606 | 0.030139 | 0.358898 |
| Overbite | 3.5400 | 1.2544 | ||||
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | 0.022152 | 0.000491 | 0.907500 |
| Overjet | 2.4067 | 0.7701 | ||||
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | −0.183319 | 0.033606 | 0.332212 |
| Interincisal angle | 134.6000 | 11.7403 | ||||
| Mean SCGA during protrusion | 30 | 56.6000 | 6.6299 | −0.173343 | 0.030048 | 0.359636 |
| Incisal guidance angle | 53.1333 | 12.1789 |
| Variables | n | Mean | SD | r (X, Y) | r2 | p |
|---|---|---|---|---|---|---|
| Incisal guidance angle | 30 | 53.13333 | 12.17893 | −0.069985 | 0.004898 | 0.713254 |
| Mean SCGA in AB measurement | 41.11667 | 6.26936 | ||||
| Incisal guidance angle | 30 | 53.13333 | 12.17893 | −0.062899 | 0.003956 | 0.741250 |
| Mean SCGA in AT measurement | 52.41667 | 7.95254 | ||||
| Incisal guidance angle | 30 | 53.13333 | 12.17893 | −0.129900 | 0.016874 | 0.493869 |
| Mean SCGA in CD measurement | 36.48333 | 5.85085 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lassmann, Ł.; Nowak, Z.; Orthlieb, J.-D.; Żółtowska, A. Complicated Relationships between Anterior and Condylar Guidance and Their Clinical Implications—Comparison by Cone Beam Computed Tomography and Electronic Axiography—An Observational Cohort Cross-Sectional Study. Life 2023, 13, 335. https://doi.org/10.3390/life13020335
Lassmann Ł, Nowak Z, Orthlieb J-D, Żółtowska A. Complicated Relationships between Anterior and Condylar Guidance and Their Clinical Implications—Comparison by Cone Beam Computed Tomography and Electronic Axiography—An Observational Cohort Cross-Sectional Study. Life. 2023; 13(2):335. https://doi.org/10.3390/life13020335
Chicago/Turabian StyleLassmann, Łukasz, Zuzanna Nowak, Jean-Daniel Orthlieb, and Agata Żółtowska. 2023. "Complicated Relationships between Anterior and Condylar Guidance and Their Clinical Implications—Comparison by Cone Beam Computed Tomography and Electronic Axiography—An Observational Cohort Cross-Sectional Study" Life 13, no. 2: 335. https://doi.org/10.3390/life13020335
APA StyleLassmann, Ł., Nowak, Z., Orthlieb, J.-D., & Żółtowska, A. (2023). Complicated Relationships between Anterior and Condylar Guidance and Their Clinical Implications—Comparison by Cone Beam Computed Tomography and Electronic Axiography—An Observational Cohort Cross-Sectional Study. Life, 13(2), 335. https://doi.org/10.3390/life13020335