
Impact of Obesity on Clinical Outcomes of Patients with Intra-Abdominal Hypertension and Abdominal Compartment Syndrome



Abstract
1. Introduction
2. Materials and Methods
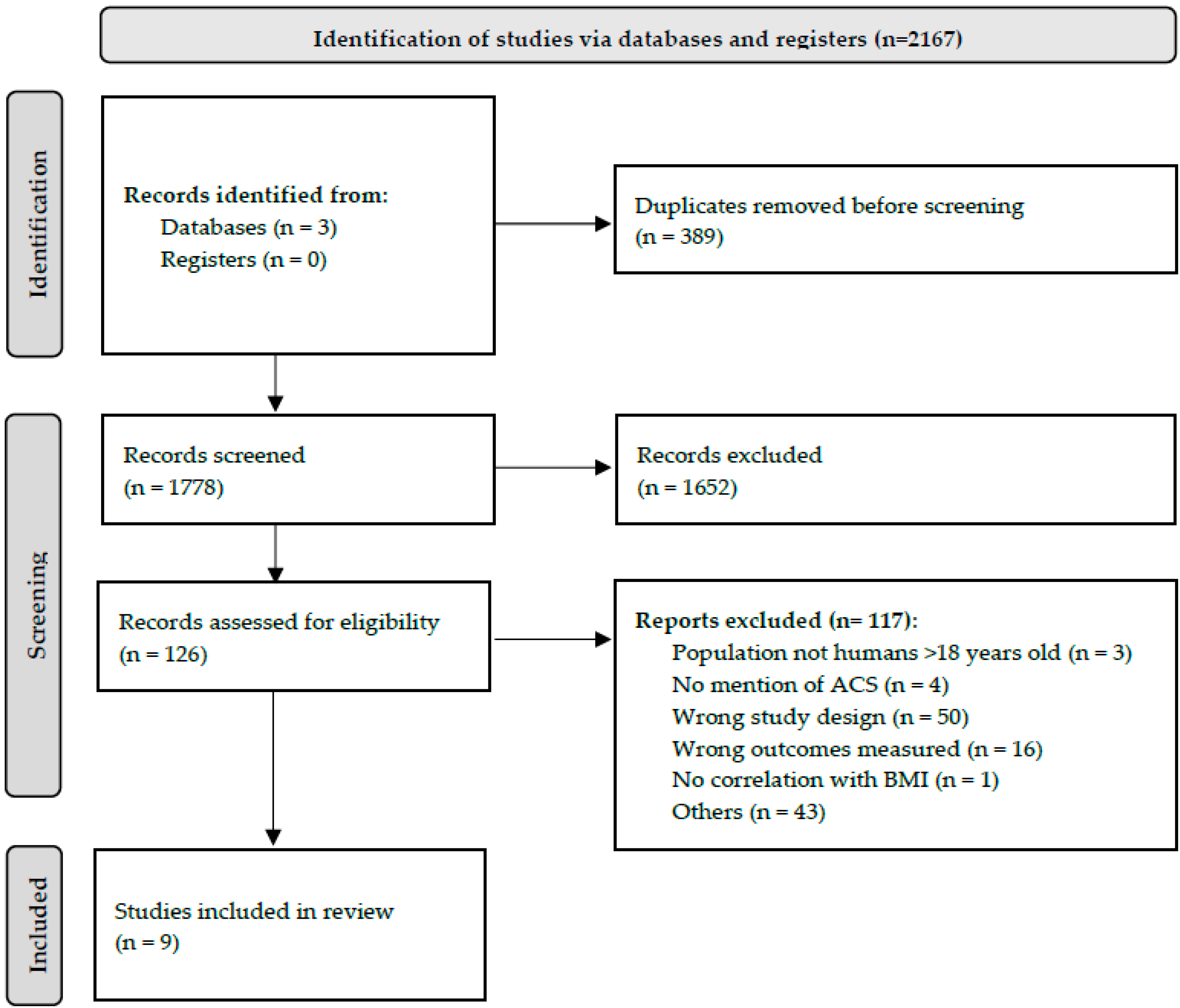
2.1. Study Selection and Search Strategy
2.2. Data Extraction and Synthesis
2.3. Risk of Bias Assessment
3. Results
3.1. Study Characteristics
3.2. Obesity and Impact on IAP
3.3. Clinical Outcomes of Patients with IAH Or ACS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fietsam, R.; Villalba, M.; Glover, J.L.; Clark, K. Intra-abdominal compartment syndrome as a complication of ruptured abdominal aortic aneurysm repair. Ann. Surg. 1989, 55, 396–402. [Google Scholar]
- Kron, I.L.; Harman, P.K.; Nolan, S.P. The measurement of intra-abdominal pressure as a criterion for abdominal re-exploration. Ann Surg. 1984, 199, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Kimball, E.J.; Kim, W.; Cheatham, M.L.; Malbrain, M.L.N.G. Clinical awareness of intra-abdominal hypertension and abdominal compartment syndrome in 2007. Acta Clin. Belg. 2007, 62 (Suppl. 1), 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, A.W.; Roberts, D.J.; De Waele, J.; Jaeschke, R.; Malbrain, M.L.N.G.; De Keulenaer, B.; Duchesne, J.; Bjorck, M.; Leppaniemi, A.; Ejike, J.C.; et al. Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013, 39, 1190–1206. [Google Scholar] [CrossRef] [PubMed]
- Socea, B.; Nica, A.A.; Smaranda, A.; Bratu, O.G.; Diaconu, C.C.; Carap, A.C.; Neagu, T.P.; Badiu, C.D.; Constantin, V.D. Abdominal Compartment Syndrome—A Surgical Emergency. Mod. Med. 2018, 25, 187–191. [Google Scholar] [CrossRef]
- Walker, J.; Criddle, L.M. Pathophysiology and management of abdominal compartment syndrome. Am. J. Crit. Care 2003, 12, 367–371, quiz 372–373. [Google Scholar] [CrossRef]
- Smith, K.B.; Smith, M.S. Obesity Statistics. Prim. Care 2016, 43, 121–135. [Google Scholar] [CrossRef]
- Varela, J.E.; Hinojosa, M.; Nguyen, N. Correlations between intra-abdominal pressure and obesity-related co-morbidities. Surg. Obes. Relat. Dis. 2009, 5, 524–528. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Kim, I.B.; Prowle, J.; Baldwin, I.; Bellomo, R. Incidence, risk factors and outcome associations of intra-abdominal hypertension in critically ill patients. Anaesth. Intensive Care 2012, 40, 79–89. [Google Scholar] [CrossRef]
- Lambert, D.M.; Marceau, S.; Forse, R.A. Intra-abdominal pressure in the morbidly obese. Obes. Surg. 2005, 15, 1225–1232. [Google Scholar] [CrossRef]
- Paolini, J.B.M.; Mancini, J.; Genestal, M.; Gonzalez, H.; McKay, R.E.; Samii, K.; Fourcade, O.A. Predictive value of abdominal obesity vs. body mass index for determining risk of intensive care unit mortality. Crit. Care Med. 2010, 38, 1308–1314. [Google Scholar] [CrossRef]
- Pãduraru, D.N.; Nica, A.; Stoian, R.V.; Oprescu, S.M.; Ionescu, O.A.; Andronic, O.; Ion, D. Obesity—Risk Factor for Abdominal Compartment Syndrome in Patients with Acute Pancreatits. Arch. Balk. Med. Union 2016, 51, 153–156. [Google Scholar]
- Ramser, M.; Glauser, P.M.; Glass, T.R.; Weixler, B.; Grapow, M.T.R.; Hoffmann, H.; Kirchhoff, P. Abdominal Decompression after Cardiac Surgery: Outcome of 42 Patients with Abdominal Compartment Syndrome. World J. Surg. 2021, 45, 1242–1251. [Google Scholar] [CrossRef]
- Smit, M.; Werner, M.J.M.; Lansink-Hartgring, A.O.; Dieperink, W.; Zijlstra, J.G.; van Meurs, M. How central obesity influences intra-abdominal pressure: A prospective, observational study in cardiothoracic surgical patients. Ann. Intensive Care 2016, 6, 99. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5056912/ (accessed on 26 November 2022). [CrossRef]
- Sugerman, H.; Windsor, A.; Bessos, M.; Wolfe, L. Intra-abdominal pressure, sagittal abdominal diameter and obesity comorbidity. J. Intern. Med. 1997, 241, 71–79. [Google Scholar] [CrossRef]
- Wacharasint, P.; Fuengfoo, P.; Rangsin, R.; Morakul, S.; Chittawattanarat, K.; Chaiwat, O. Prevalence and Impact of Overweight and Obesity in Critically Ill Surgical Patients: Analysis of THAI-SICU Study. J. Med. Assoc. Thail. 2016, 99 (Suppl. 6), S55–S62. [Google Scholar]
- Malbrain, M. Relationship of body mass index (BMI), lactate and intra-abdominal pressure (IAP) to subsequent mortality in ICU patients. Crit. Care 1999, 3 (Suppl. 1), P039. [Google Scholar] [CrossRef]
- Jacobs, R.; Wise, R.D.; Myatchin, I.; Vanhonacker, D.; Minini, A.; Mekeirele, M.; Kirkpatrick, A.W.; Pereira, B.M.; Sugrue, M.; De Keulenaer, B.; et al. Fluid Management, Intra-Abdominal Hypertension and the Abdominal Compartment Syndrome: A Narrative Review. Life 2022, 12, 1390. [Google Scholar] [CrossRef]
- Frezza, E.E.; Shebani, K.O.; Robertson, J.; Wachtel, M.S. Morbid Obesity Causes Chronic Increase of Intraabdominal Pressure. Dig. Dis. Sci. 2007, 52, 1038–1041. [Google Scholar] [CrossRef]
- Malbrain, M.L.N.G.; De Keulenaer, B.L.; Khanna, A.K. Continuous intra-abdominal pressure: Is it ready for prime time? Intensive Care Med. 2022, 48, 1501–1504. [Google Scholar] [CrossRef] [PubMed]
- Akinnusi, M.E.; Pineda, L.A.; El Solh, A.A. Effect of obesity on intensive care morbidity and mortality: A meta-analysis. Crit. Care Med. 2008, 36, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Minet, C.; Potton, L.; Bonadona, A.; Hamidfar-Roy, R.; Somohano, C.A.; Lugosi, M.; Cartier, J.-C.; Ferretti, G.; Schwebel, C.; Timsit, J.-F. Venous thromboembolism in the ICU: Main characteristics, diagnosis and thromboprophylaxis. Crit. Care 2015, 19, 287. [Google Scholar] [CrossRef] [PubMed]
- Weststrate, J.T.; Bruining, H.A. Pressure sores in an intensive care unit and related variables: A descriptive study. Intensive Crit. Care Nurs. 1996, 12, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Ak, A.K.; Anjum, F. Ventilator-Induced Lung Injury (VILI). StatPearls. StatPearls Publishing. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563244/ (accessed on 27 November 2022).
- Maramattom, B.V.; Wijdicks, E.F.M. Acute neuromuscular weakness in the intensive care unit. Crit. Care Med. 2006, 34, 2835–2841. [Google Scholar] [CrossRef]
- Desai, S.V.; Law, T.J.; Needham, D.M. Long-term complications of critical care. Crit. Care Med. 2011, 39, 371–379. [Google Scholar] [CrossRef]
- Lin, W.T.; Lai, C.C.; Chang, S.P.; Wang, J.J. Effects of early dialysis on the outcomes of critically ill patients with acute kidney injury: A systematic review and meta-analysis of randomized controlled trials. Sci. Rep. 2019, 9, 18283. [Google Scholar] [CrossRef]
- Parham, W.A.; Mehdirad, A.A.; Biermann, K.M.; Fredman, C.S. Hyperkalemia Revisited. Tex. Heart Inst. J. 2006, 33, 40–47. [Google Scholar]
- Lapinsky, S.E.; Mount, D.B.; Mackey, D.; Grossman, R.F. Management of acute respiratory failure due to pulmonary edema with nasal positive pressure support. Chest 1994, 105, 229–231. [Google Scholar] [CrossRef]
- van Santvoort, H.C.; Bakker, O.J.; Bollen, T.L.; Besselink, M.G.; Ahmed Ali, U.; Schrijver, A.M.; Boermeester, M.A.; van Goor, H.; Dejong, C.H.; van Eijck, C.H.; et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011, 141, 1254–1263. [Google Scholar] [CrossRef]
- van Brunschot, S.; Schut, A.J.; Bouwense, S.A.; Besselink, M.G.; Bakker, O.J.; van Goor, H.; Hofker, S.; Gooszen, H.G.; Boermeester, M.A.; van Santvoort, H.C.; et al. Abdominal Compartment Syndrome in Acute Pancreatitis: A Systematic Review. Pancreas 2014, 43, 665–674. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Regli, A.; De Keulenaer, B.; Kimball, E.J.; Starkopf, L.; Davis, W.A.; Greiffenstein, P.; Starkopf, J. Incidence, Risk Factors, and Outcomes of Intra-Abdominal (IROI) Study Investigators. Incidence, Risk Factors, and Outcomes of Intra-Abdominal Hypertension in Critically Ill Patients—A Prospective Multicenter Study (IROI Study). Crit. Care Med. 2019, 47, 535–542. [Google Scholar] [CrossRef]
- Bochicchio, G.V.; Joshi, M.; Bochicchio, K.; Nehman, S.; Tracy, J.K.; Scalea, T.M. Impact of obesity in the critically ill trauma patient: A prospective study. J. Am. Coll. Surg. 2006, 203, 533–538. [Google Scholar] [CrossRef]
- Siegelaar, S.E.; Hoekstra, J.B.L.; DeVries, J.H. Special considerations for the diabetic patient in the ICU; targets for treatment and risks of hypoglycaemia. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 825–834. [Google Scholar] [CrossRef]
- Goh, S.S.N.; Chan, K.S.; Tay, W.M. The impact of obesity on Singaporean trauma patients and their venous thromboembolism risk. ANZ J. Surg. 2022, 92, 1706–1713. [Google Scholar] [CrossRef]
- Trivedi, V.; Jean, R.E.; Genese, F.; Fuhrmann, K.A.; Saini, A.K.; Mangulabnan, V.D.; Bavishi, C. Impact of Obesity on Outcomes in a Multiethnic Cohort of Medical Intensive Care Unit Patients. J. Intensive Care Med. 2018, 33, 97–103. [Google Scholar] [CrossRef]
- O’Brien, J.M.; Philips, G.S.; Ali, N.A.; Aberegg, S.K.; Marsh, C.B.; Lemeshow, S. The association between body mass index, processes of care, and outcomes from mechanical ventilation: A prospective cohort study. Crit. Care Med. 2012, 40, 1456–1463. [Google Scholar] [CrossRef]
- Robinson, K.; Prins, J.; Venkatesh, B. Clinical review: Adiponectin biology and its role in inflammation and critical illness. Crit. Care 2011, 15, 221. [Google Scholar] [CrossRef]
- Stapleton, R.D.; Dixon, A.E.; Parsons, P.E.; Ware, L.B.; Suratt, B.T. NHLBI Acute Respiratory Distress Syndrome Network. The association between BMI and plasma cytokine levels in patients with acute lung injury. Chest 2010, 138, 568–577. [Google Scholar] [CrossRef]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Pischon, T.; Boeing, H.; Hoffmann, K.; Bergmann, M.; Schulze, M.B.; Overvad, K.; van der Schouw, Y.T.; Spencer, E.; Moons, K.G.M.; Tjønneland, A.; et al. General and abdominal adiposity and risk of death in Europe. N. Engl. J. Med. 2008, 359, 2105–2120. [Google Scholar] [CrossRef]
- Seidell, J.C. Waist circumference and waist/hip ratio in relation to all-cause mortality, cancer and sleep apnea. Eur. J. Clin. Nutr. 2010, 64, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Gupta, H.P.; Khichar, P.R.; Porwal, R.; Singh, A.; Sharma, A.K.; Beniwal, M.; Singh, S. The Duration of Intra-abdominal Hypertension and Increased Serum Lactate Level are Important Prognostic Markers in Critically Ill Surgical Patient’s Outcome: A Prospective, Observational Study. Niger. J. Surg. 2019, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kyoung, K.H.; Hong, S.K. The duration of intra-abdominal hypertension strongly predicts outcomes for the critically ill surgical patients: A prospective observational study. World J. Emerg. Surg. WJES 2015, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Akavipat, P.; Thinkhamrop, J.; Thinkhamrop, B.; Sriraj, W. Acute Physiology and Chronic Health Evaluation (APAHCE) II Score—The Clinical Predictor in Neurosurgical Intensive Care Unit. Acta Clin. Croat. 2019, 58, 50–56. [Google Scholar]


{kind=link}
| No. | First Author | Year | Study Design | Sample Size | Patient Population | Outcomes Reported |
|---|---|---|---|---|---|---|
| 1 | I. B. Kim [10] | 2012 | Prospective | 100 | ICU patients > 18 yo | Survival |
| 2 | D. M. Lambert [11] | 2005 | Prospective | 49 | Morbidly obese undergoing open Roux-en-Y gastric bypass | Osteoarthropathy, Gallbladder disease, OSA, GERD, HTN, Abdominal hernia, T2DM, HLD, Heart disease |
| 3 | J. M. Paolini [12] | 2010 | Prospective | 403 | ICU patients | Septic shock, Sepsis, CVS pathology, Neurologic pathology, Haemorrhagic shock, Trauma, ARDS, ICU mortality, RRT, ICU-acquired infection, Acute coronary syndrome, Thrombophlebitis or PE |
| 4 | D.N. Pãduraru [13] | 2016 | Retrospective | 269 | Acute pancreatitis adult patients | Length of Stay, Mortality |
| 5 | M. Ramser [14] | 2021 | Prospective | 4128 | Post-cardiac surgery | HTN, Smoking, Dyslipidaemia, Units of blood transfused, Units of FFP transfused, Units of platelets transfused, Mortality |
| 6 | M. Smit [15] | 2016 | Prospective | 186 | Cardiothoracic surgery patients | COPD, Chronic cardiovascular insufficiency, Immunological insufficiency, Metastasized neoplasm, Respiratory insufficiency, New AKI, Haematological malignancy, New confirmed infection, Vasopressor in first 24 h of ICU, APACHE IV score, LOS in ICU, Reintubation rate |
| 7 | H. Sugerman [16] | 1997 | Prospective | 89 | 84 Bariatric surgery, 5 colectomy w/ ileoanal anastomosis for ulcerative colitis | Hypoventilation, GERD, Venous stasis, Stress incontinence, Incisional hernia, HTN, T2DM |
| 8 | J. E. Varela [8] | 2009 | Prospective | 62 | Morbidly obese patients who underwent laparoscopic gastric bypass or adjustable gastric banding | Systemic HTN, T2DM, OSA, GERD, Urinary stress incontinence, Lower extremity edema, Abdominal wall hernia |
| 9 | P. Wacharasint [17] | 2016 | Retrospective | 4652 | SICUs in Thailand | SIRS, New Infection, ARDS, 28-Day Mortality |
| Selection | Comparability | Outcome | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Year of Study | First Author | Representation of the Exposed Cohort | Selection of Non Exposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest was Not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis (2 Points) | Assessment of Outcome | Was Follow Up Long Enough for Outcomes to Occur? | Adequacy of Follow Up Cohorts | Total Score* |
| 1 | 2012 | I. B. Kim [10] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 2 | 2005 | D. M. Lambert [11] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 3 | 2010 | J. M. Paolini [12] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 4 | 2016 | D.N. Pãduraru [13] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 5 | 2021 | M. Ramser [14] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 6 | 2016 | M. Smit [15] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 7 | 1997 | H. Sugerman [16] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 8 | 2009 | J. E. Varela [8] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| 9 | 2016 | P. Wacharasint [17] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| No. | First Author | Year | Definition of obesity | Sample size | Mean BMI (kg/m2) | Incidence of IAH | Mean IAP (cmH2O) |
|---|---|---|---|---|---|---|---|
| 1 | I. B. Kim [10] | 2012 | Overweight: BMI ≥ 25 Obese: BMI ≥ 30 | Overweight/Obese: 55/100 (55) Non-overweight/Obese: 45/100 (45) | Survivors: BMI 27.7 ± 8.1 Non-survivors: BMI 26.6 ± 7.2 p = 0.61 | Overweight/Obese: 30/42 (71.4) Non-overweight/Obese: 33/58 (56.9) Obesity on IAH: OR 8.5 (2.7–31.9), p < 0.001 | Maximum IAP: Survivors: 11.2 ± 5.7 Non-survivors: 11.9 ± 3.7 p = 0.60 Mean IAP: Survivors: 10.3 ± 5.5 Non-survivors: 10.6 ± 3.6 p = 0.79 |
| 2 | D. M. Lambert [11] | 2005 | Morbidly obese: BMI ≥ 35 | Morbidly obese: 91.8 (45/49) Control: 8.1 (4/49) | Morbidly obese: 55 ± 2 Control: 26 ± 3 p < 0.0001 | NR | Morbidly obese: 12 ± 0.7 Control: 0 ± 1.2 p < 0.001 |
| 3 | J. M. Paolini [12] | 2010 | Overweight: BMI ≥ 30 Underweight: BMI < 18.5 Abdominally obese: Upper quartile of SAD (>26 cm) | Underweight: 4.22 (17/403) Control: 68.7 (277/403) Abdominally obese: 27.0 (109/403) | NR | Underweight*: 0/17 (0) Control*: 1/277 (0.4) Abdominally obese*: 8/109 (7.3) p < 0.01 BMI ≤ 30 + SAD ≤ 26 cm*: 0/247 (0) BMI ≤ 30 + SAD ≥ 26 cm*: 4/44 (9.1) | NR |
| 4 | D.N. Pãduraru [13] | 2016 | NR | NR | NR | 102/269 (37.9) | NR |
| 5 | M. Ramser [14] | 2021 | NR | NR | NR | 42/4086 (1.0)* | |
| 6 | M. Smit [15] | 2016 | Normal weight: BMI < 25 Overweight: BMI 25–29.9 Obese: BMI ≥ 30 | Obese: 38/186 (20.4) Non-obese: 148/186 (79.6) | NR | Obese: 15/38 (39.5) Non-obese: 35/148 (23.6) | NR |
| 7 | H. Sugerman [16] | 1997 | Morbidly obese: BMI ≥ 35 | Morbidly obese: 84/89 (94.4) Non-obese: 5/89 (5.6) | NR | NR | Morbidly obese: 18 ± 0.7 Non-obese: 7 ± 1.6 p < 0.001 |
| 8 | J. E. Varela [8] | 2009 | NR | Morbidly obese: 62/62 (100) | 49 ± 10 | IAP ≥ 9 cmH2O: 48/62 (77) | NR |
| 9 | P. Wacharasint [17] | 2016 | Underweight: BMI < 18.5 Normal: BMI 18.5–24.9 Overweight: BMI 25–29.9 Obese: BMI ≥30 | Underweight: 768/4652 (16.8) Normal: 2624/4652 (57.3) Overweight: 858/4652 (18.7) Obese: 329/4652 (7.2) | NR | Underweight: 6/768 (0.7) Normal: 12/2624 (1.4) Overweight: 20/858 (2.3) Obese: 8/329 (2.4) p = 0.030 | NR |
| Type of Co-Morbidity | Study Included | Incidence of Co-Morbidity | p-Value |
|---|---|---|---|
| Osteoarthropathy | Lambert et al. [11] | Obese: 31/45 (68.9) Non-obese: 0/4 (0) | NR |
| Gallbladder Disease | Lambert et al. [11] | Obese: 25/45 (55.6) Non-obese: 0/4 (0) | NR |
| OSA | Lambert et al. [11] | Obese: 25/45 (55.6) Non-obese: 0/4 (0) | NR |
| GERD | Lambert et al. [11] | Obese: 19/45 (42.2) Non-obese: 0/4 (0) | NR |
| HTN | Lambert et al. [11] | Obese: 17/45 (37.8) Non-obese: 0/4 (0) | NR |
| Abdo Hernia | Lambert et al. [11] | Obese: 8/45 (17.8) Non-obese: 0/4 (0) | NR |
| T2DM | Lambert et al. [11] | Obese: 7/45 (15.6) Non-obese: 0/4 (0) | NR |
| HLD | Lambert et al. [11] | Obese: 6/45 (13.3) Non-obese: 0/4 (0) | NR |
| Heart Disease | Lambert et al. [11] | Obese: 5/45 (11.1) Non-obese: 0/4 (0) | NR |
| Septic Shock | Paolini et al. [12] | Obese: 69/109 (63.3) Non-obese: 210/294 (71.4) | >0.05 |
| Sepsis | Paolini et al. [12] | Obese: 15/109 (13.8) Non-obese: 53/294 (18.0) | >0.05 |
| Cardiovascular Patho | Lambert et al. [11], Paolini et al. [12], Smit et al. [15] | Obese: 27/192 (14.1) Non-obese: 47/346 (13.6) | >0.05 |
| Neurologic Patho | Paolini et al. [12] | Obese: 5/109 (4.6) Non-obese: 28/294 (9.5) | >0.05 |
| Hemorrhagic Shock | Paolini et al. [12] | Obese: 7/109 (6.4) Non-obese: 9/294 (3.1) | >0.05 |
| Trauma | Paolini et al. [12] | Obese: 11/109 (10.1) Non-obese: 44/294 (15.0) | >0.05 |
| ARDS | Paolini et al. [12] | Obese: 3/109 (2.8) Non-obese: 10/294 (3.4) | >0.05 |
| COPD | Smit et al. [15] | Obese: 0/38 (0) Non-obese: 1/148 (0.7) | NR |
| Immunological Insufficiency | Smit et al. [15] | Obese: 4/38 (10.5) Non-obese: 4/148 (2.7) | 0.034 |
| Metastasized Neoplasm | Smit et al. [15] | Obese: 1/38 (2.6) Non-obese: 2/148 (1.4) | >0.05 |
| Respiratory Insufficiency | Smit et al. [15] | Obese: 0/38 (0) Non-obese: 1/148 (0.7) | NR |
| Hematological Malignancy | Smit et al. [15] | Obese: 0/38 (0) Non-obese: 1/148 (0.7) | NR |
| Morbidity | Study Included | Patient Demographics | p-Value |
|---|---|---|---|
| Need for RRT | Paolini et al. [12] | Obese: 40/109 (36.7) Non-obese: 294 (10.5) | <0.01 |
| ICU-acquired infection | Paolini et al. [12], Smit et al. [15], Wacharasint et al. [17] | Obese: 105/476 (22.1) Non-obese: 1124/4592 (24.5) | Wacharasint et al. p = 0.047 |
| Acute coronary syndrome | Paolini et al. [12] | Obese: 6/109 (5.5) Non-obese: 7/294 (2.4) | NR |
| Thrombophlebitis or PE | Paolini et al. [12] | Obese: 10/109 (9.2) Non-obese: 13/294 (4.4) | NR |
| New-onset AKI | Smit et al. [15] | Obese: 0/38 (0) Non-obese: 1/148 (0.7) | NR |
| Length of stay, days | Smit et al. [15] | Obese: 0.94 (5.2) Obese: 0.91 (19.4) | 0.060 |
| Need for vasopressors | Smit et al. [15] | Obese: 32/38 (84.2) Non-obese: 132/148 (89.2) | 0.571 |
| Reintubation | Smit et al. [15] | Obese: 0/38 (0) Non-obese: 0/148 (0) | NR |
| SIRS | Wacharasint et al. [17] | Obese: 97/329 (29.5) Non-obese: 1545/4250 (36.4) | 0.001 |
| ARDS | Wacharasint et al. [17] | Obese: 14/329 (4.3) Non-obese: 159/4250 (3.7) | 0.048 |
| Mortality | Paolini et al. [12] | Obese: 48/109 (44.0) Non-obese: 78/294 (26.5) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohan, S.; Lim, Z.Y.; Chan, K.S.; Shelat, V.G. Impact of Obesity on Clinical Outcomes of Patients with Intra-Abdominal Hypertension and Abdominal Compartment Syndrome. Life 2023, 13, 330. https://doi.org/10.3390/life13020330
Mohan S, Lim ZY, Chan KS, Shelat VG. Impact of Obesity on Clinical Outcomes of Patients with Intra-Abdominal Hypertension and Abdominal Compartment Syndrome. Life. 2023; 13(2):330. https://doi.org/10.3390/life13020330
Chicago/Turabian StyleMohan, Swetha, Zavier Yongxuan Lim, Kai Siang Chan, and Vishal G. Shelat. 2023. "Impact of Obesity on Clinical Outcomes of Patients with Intra-Abdominal Hypertension and Abdominal Compartment Syndrome" Life 13, no. 2: 330. https://doi.org/10.3390/life13020330
APA StyleMohan, S., Lim, Z. Y., Chan, K. S., & Shelat, V. G. (2023). Impact of Obesity on Clinical Outcomes of Patients with Intra-Abdominal Hypertension and Abdominal Compartment Syndrome. Life, 13(2), 330. https://doi.org/10.3390/life13020330