


Psilocybin and Eugenol Reduce Inflammation in Human 3D EpiIntestinal Tissue

 ,
,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. EpiIntestinal 3D Model and Inflammation Induction
2.2. Treatment of EpiIntestinal 3D Tissue
2.3. Multiplex Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Whole Cellular Lysate Preparation and Western Blot Analysis
2.5. Statistical Analysis
3. Results
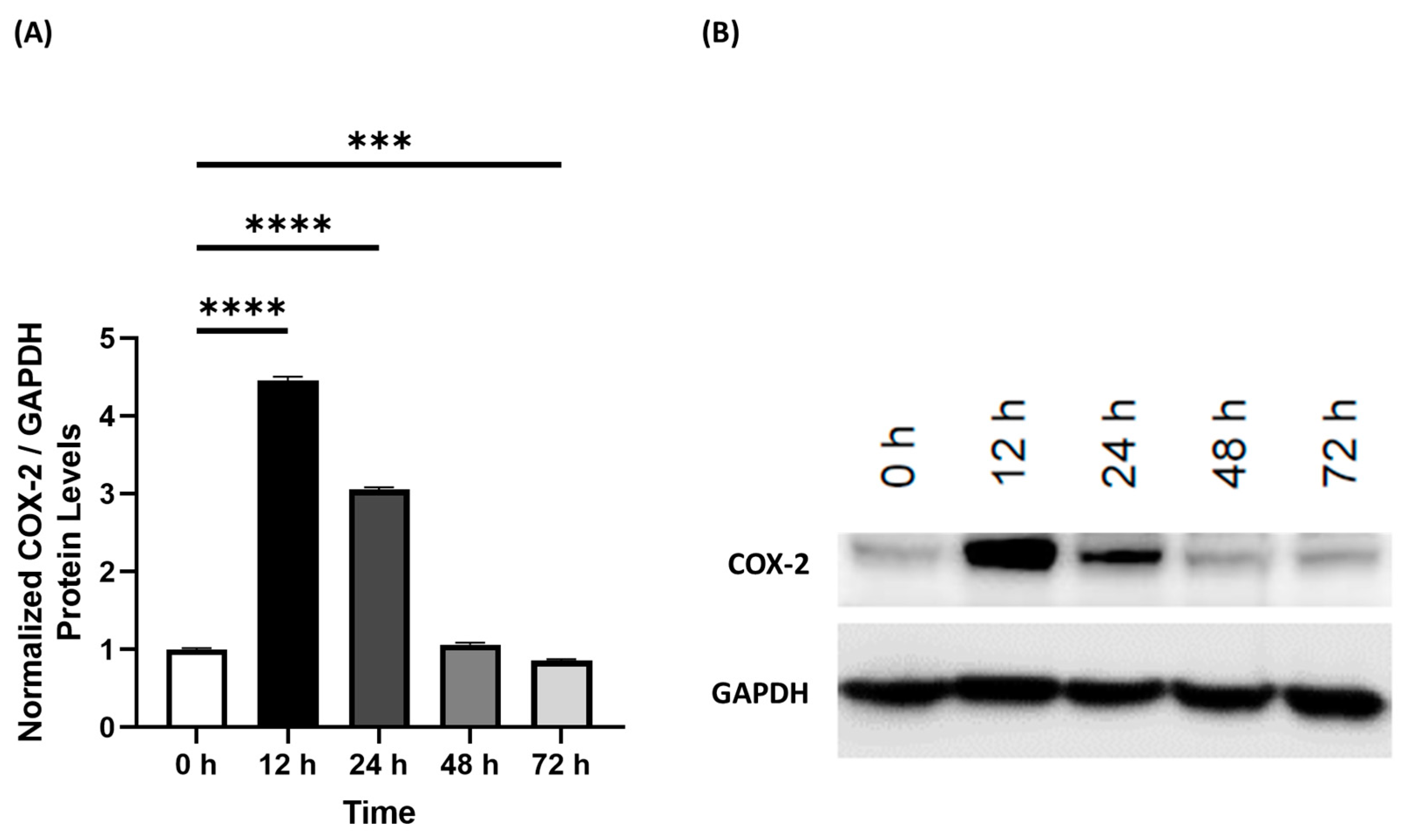
3.1. Human 3D EpiIntestinal Tissue Exhibits Inflammation Characteristic of Inflammatory Bowel Disease
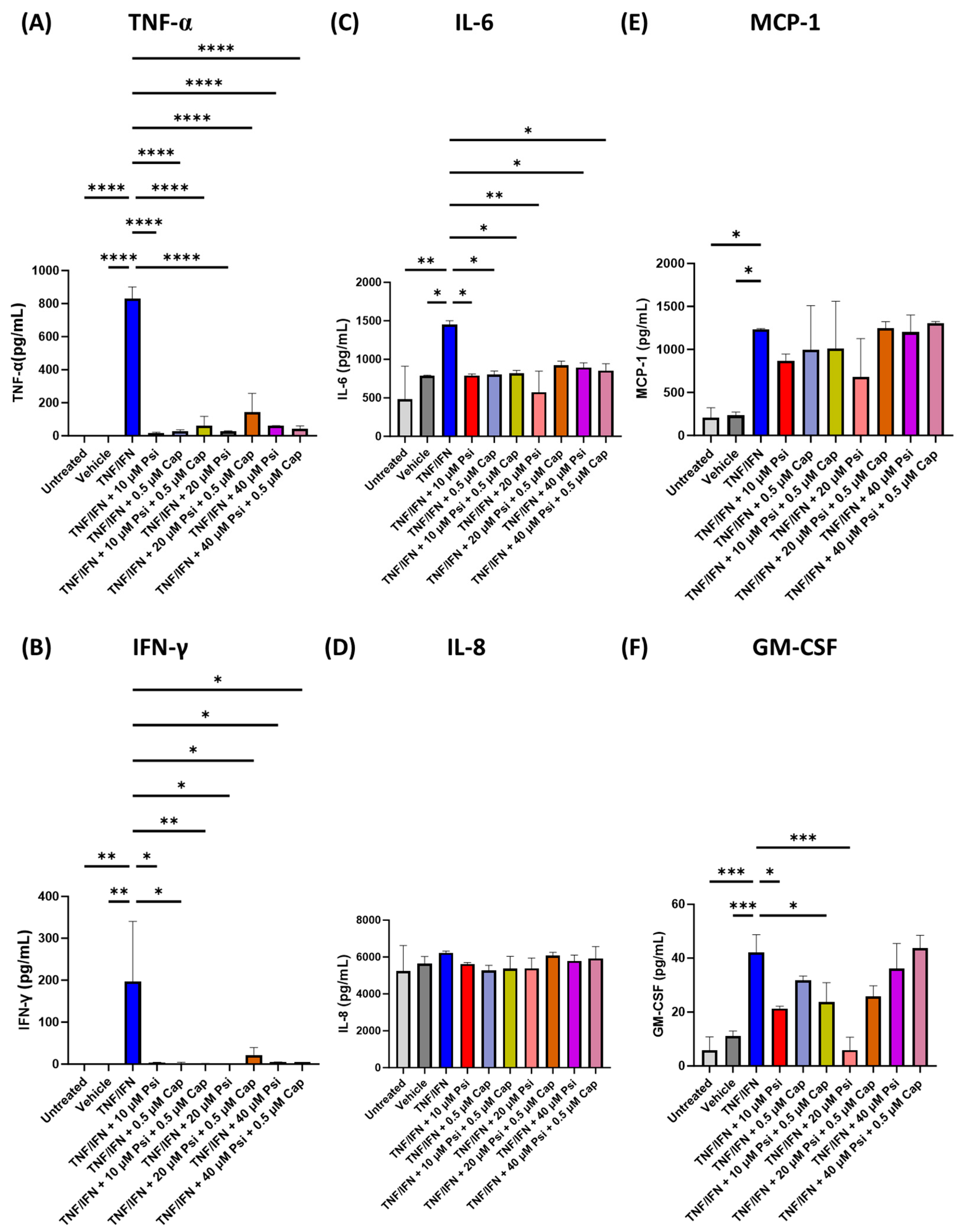
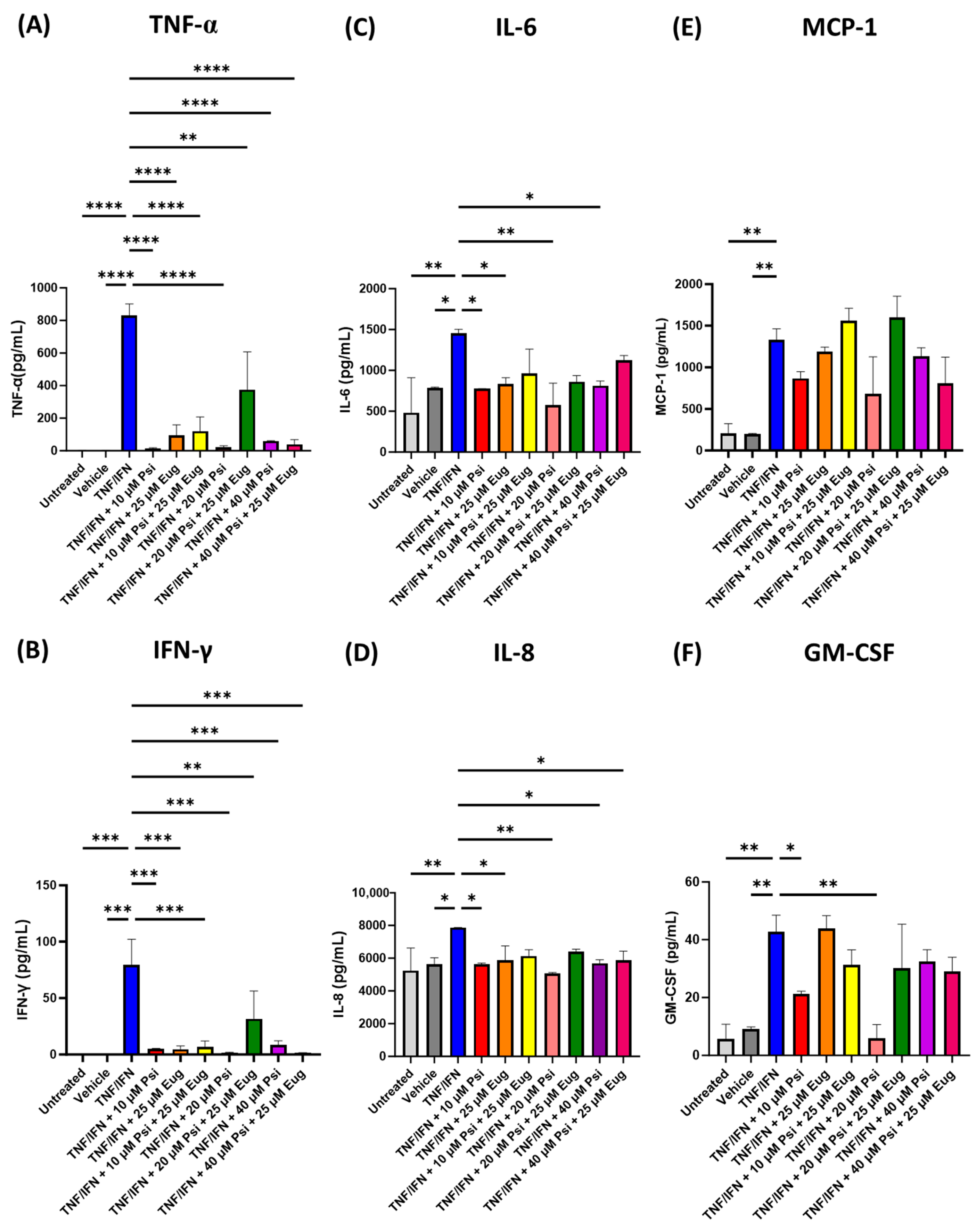
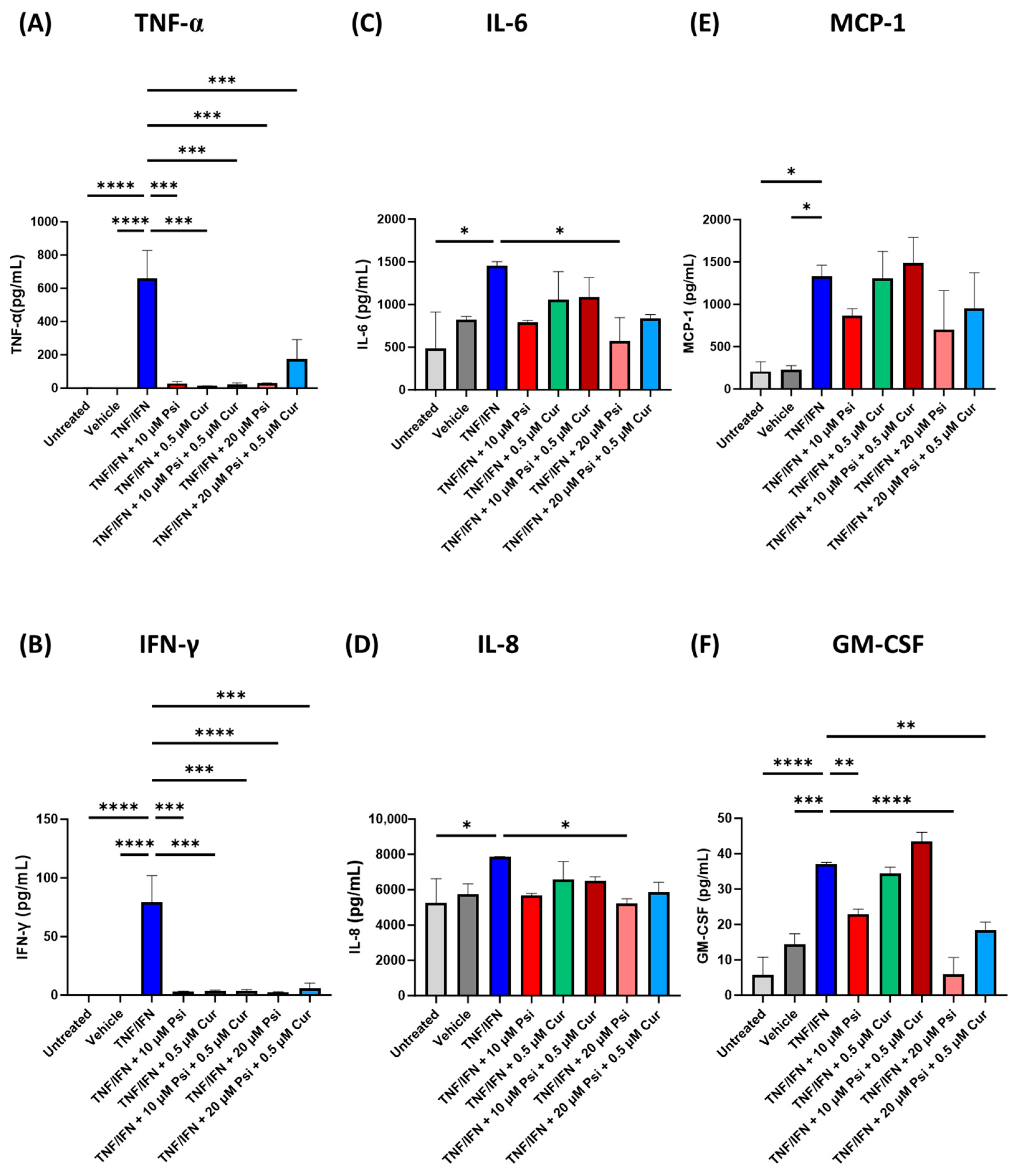
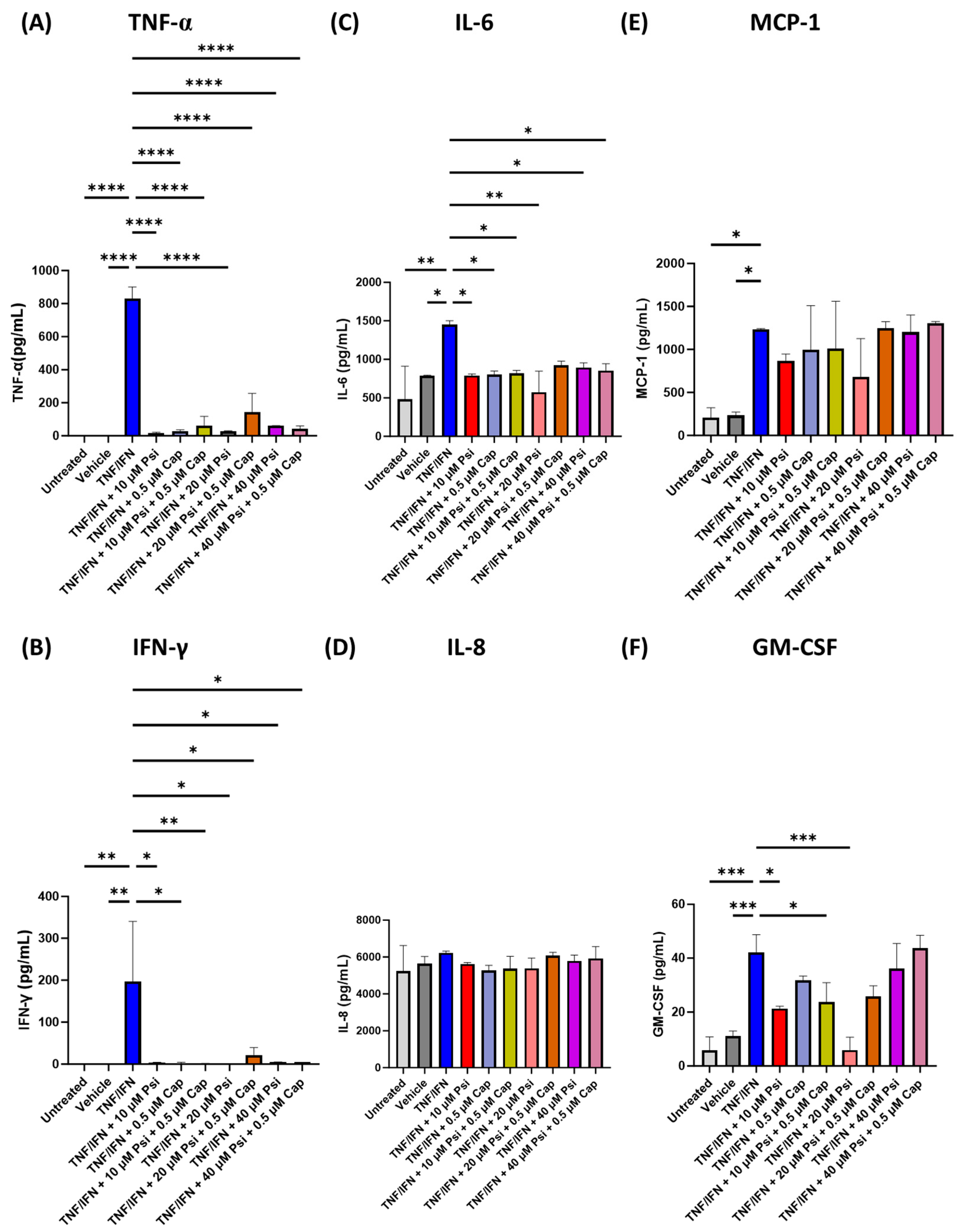
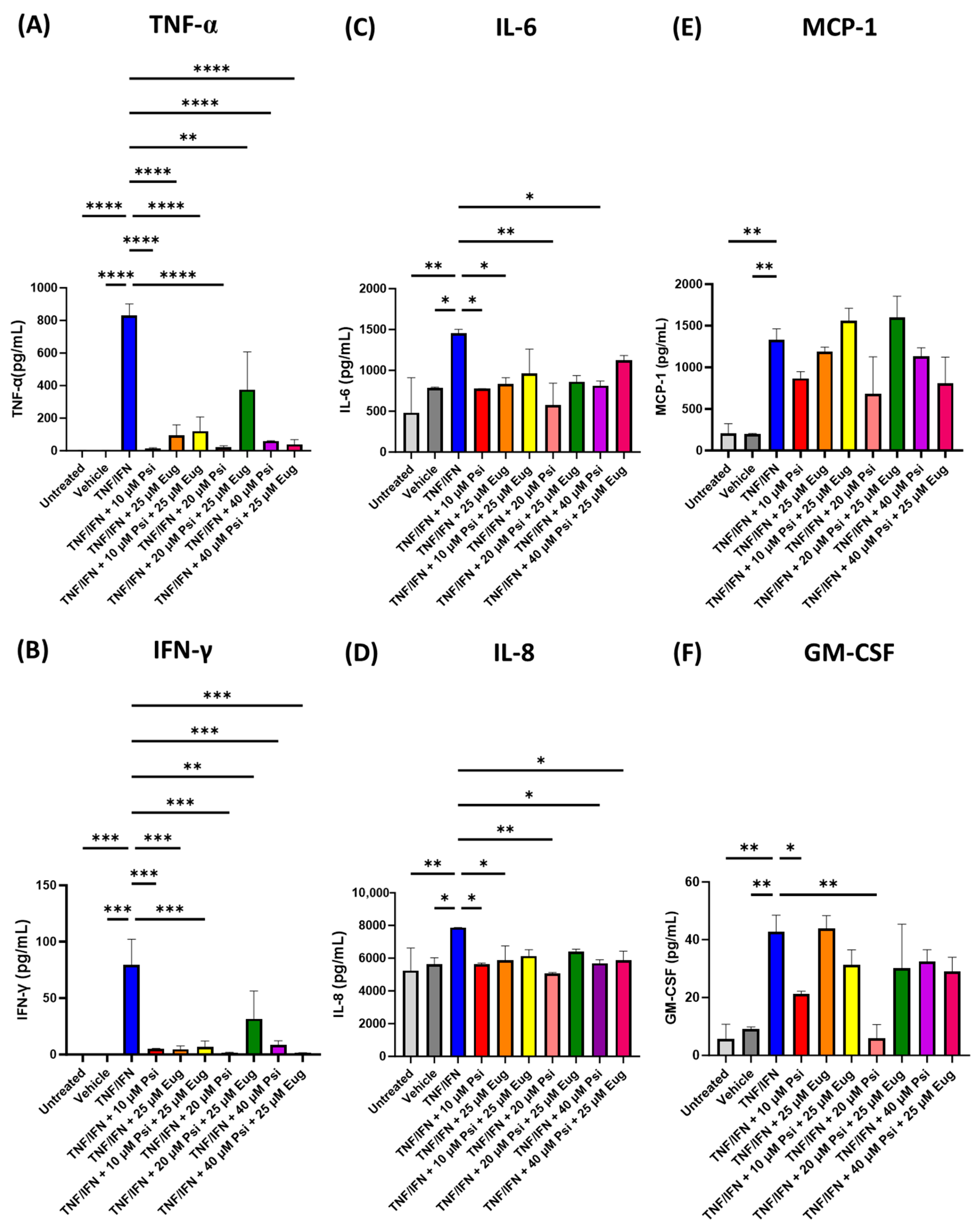
3.2. Psilocybin and Transient Receptor Potential Channel Agonists Decrease Inflammation in Human 3D EpiIntestinal Tissue
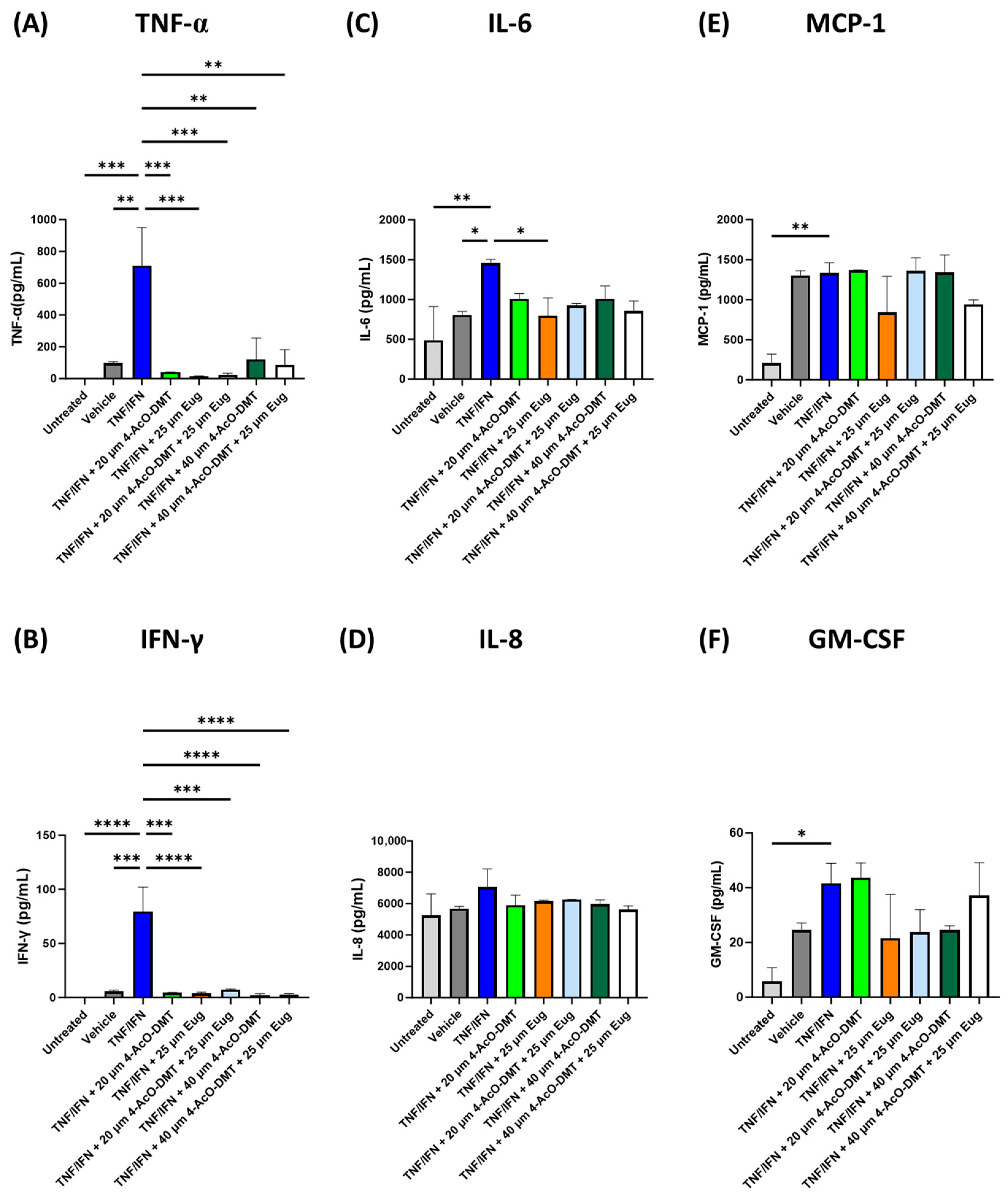
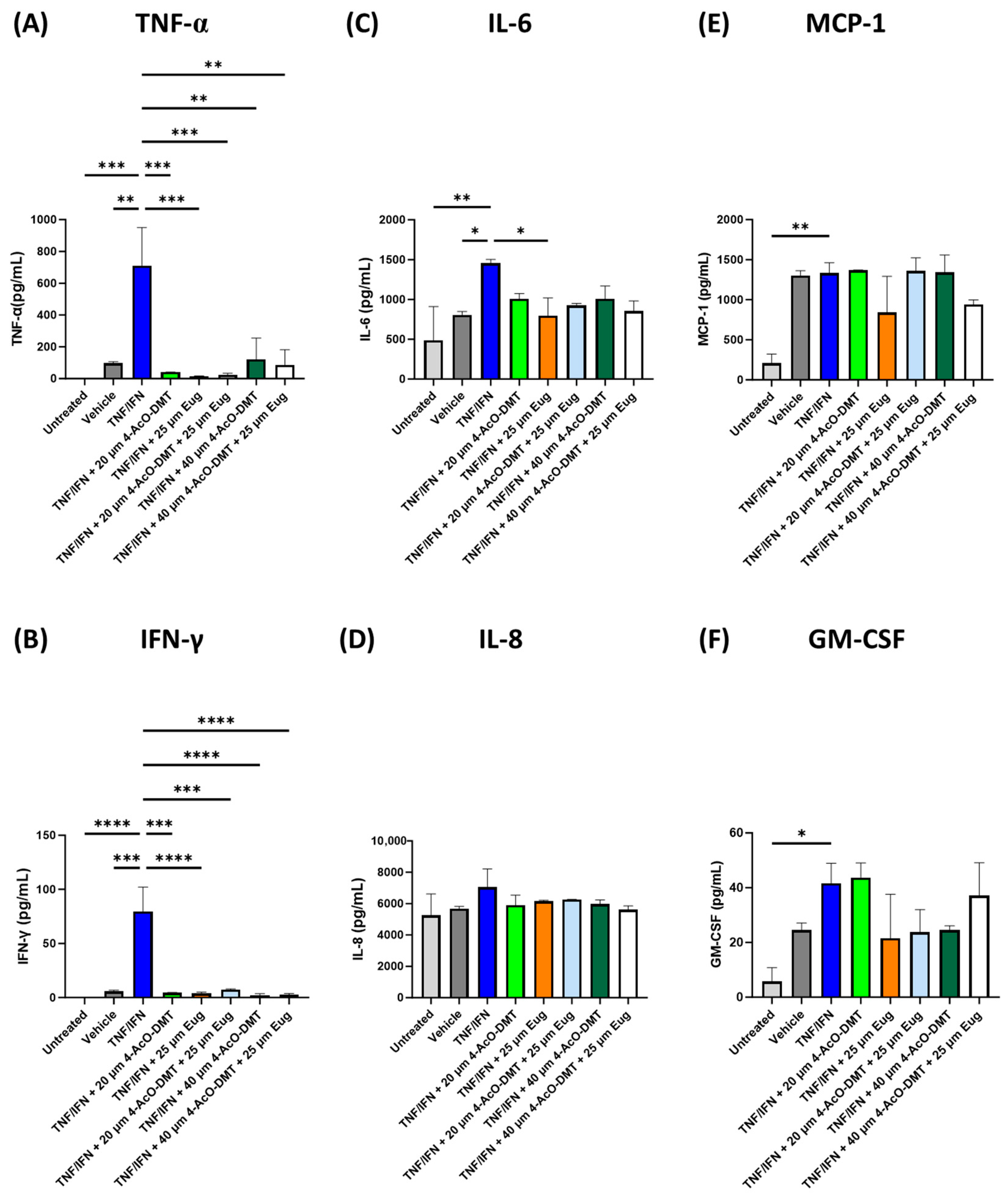
3.3. 4-AcO-DMT and Eugenol Decrease Inflammation in Human 3D EpiIntestinal Tissue
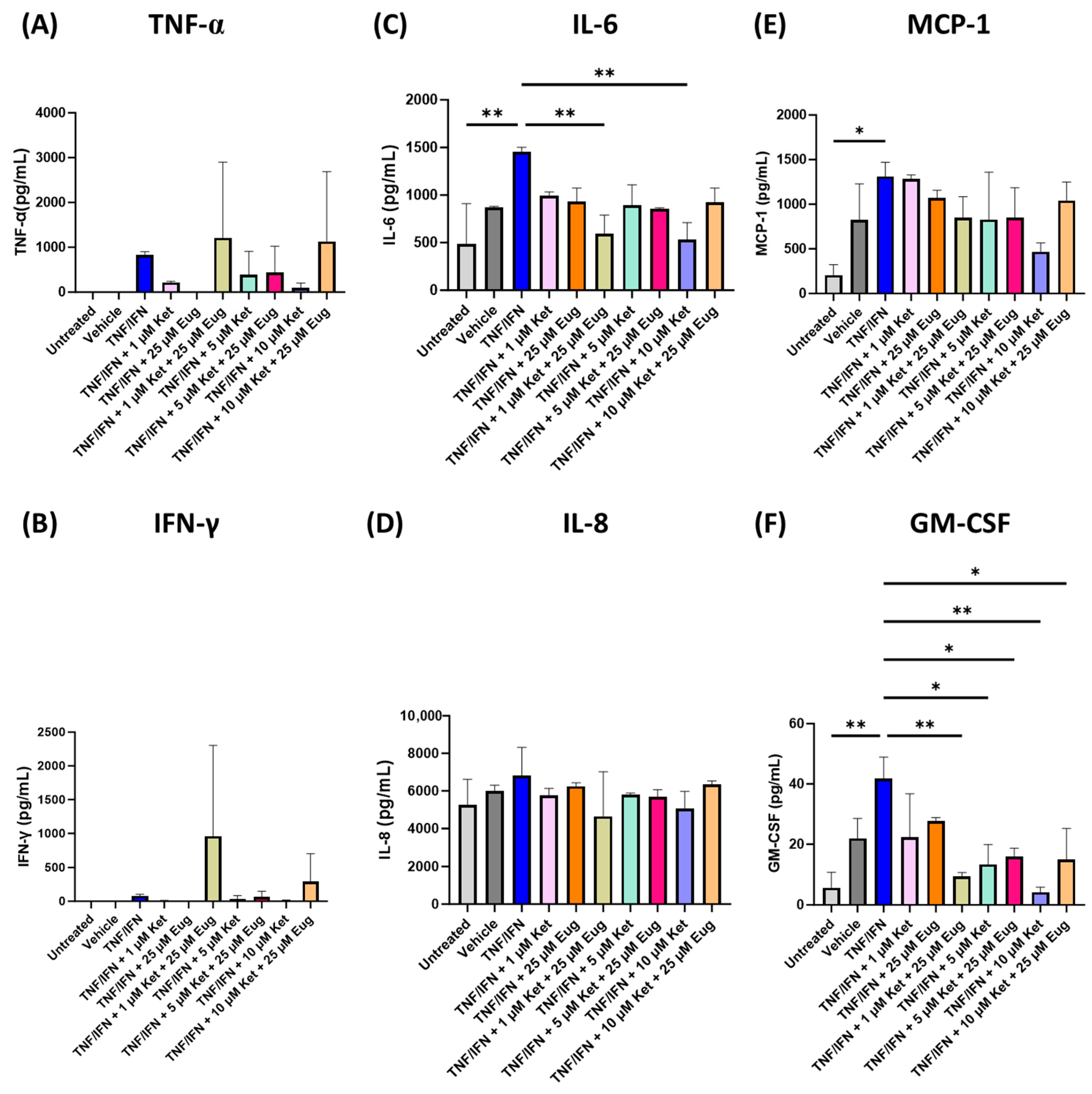
3.4. Ketanserin and Eugenol Decrease Inflammation in Human 3D EpiIntestinal Tissue
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, J.Y.; Wasinger, V.C.; Yau, Y.Y.; Chuang, E.; Yajnik, V.; Leong, R.W. Molecular Pathophysiology of Epithelial Barrier Dysfunction in Inflammatory Bowel Diseases. Proteomes 2018, 6, 17. [Google Scholar] [CrossRef]
- Laukoetter, M.G.; Nava, P.; Nusrat, A. Role of the intestinal barrier in inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Abdulla, M.; Mohammed, N. A Review on Inflammatory Bowel Diseases: Recent Molecular Pathophysiology Advances. Biol. Targets Ther. 2022, 16, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Wang, S.; Li, J. Treatment of Inflammatory Bowel Disease: A Comprehensive Review. Front. Med. 2021, 8, 765474. [Google Scholar] [CrossRef] [PubMed]
- Alatab, S.; Sepanlou, S.G.; Ikuta, K.; Vahedi, H.; Bisignano, C.; Safiri, S.; Sadeghi, A.; Nixon, M.R.; Abdoli, A.; Abolhassani, H.; et al. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef]
- Mak, W.Y.; Zhao, M.; Ng, S.C.; Burisch, J. The epidemiology of inflammatory bowel disease: East meets west. J. Gastroenterol. Hepatol. 2020, 35, 380–389. [Google Scholar] [CrossRef]
- Nkadimeng, S.M.; Nabatanzi, A.; Steinmann, C.M.L.; Eloff, J.N. Phytochemical, Cytotoxicity, Antioxidant and Anti-Inflammatory Effects of Psilocybe Natalensis Magic Mushroom. Plants 2020, 9, 1127. [Google Scholar] [CrossRef]
- Nkadimeng, S.M.; Steinmann, C.M.L.; Eloff, J.N. Anti-Inflammatory Effects of Four Psilocybin-Containing Magic Mushroom Water Extracts in vitro on 15-Lipoxygenase Activity and on Lipopolysaccharide-Induced Cyclooxygenase-2 and Inflammatory Cytokines in Human U937 Macrophage Cells. J. Inflamm. Res. 2021, 14, 3729–3738. [Google Scholar] [CrossRef]
- Flanagan, T.W.; Nichols, C.D. Psychedelics as anti-inflammatory agents. Int. Rev. Psychiatry Abingdon Engl. 2018, 30, 363–375. [Google Scholar] [CrossRef]
- Kalkman, H.O. Inhibition of Microglial GSK3β Activity Is Common to Different Kinds of Antidepressants: A Proposal for an In Vitro Screen to Detect Novel Antidepressant Principles. Biomedicines 2023, 11, 806. [Google Scholar] [CrossRef]
- Klein, A.K.; Chatha, M.; Laskowski, L.J.; Anderson, E.I.; Brandt, S.D.; Chapman, S.J.; McCorvy, J.D.; Halberstadt, A.L. Investigation of the Structure-Activity Relationships of Psilocybin Analogues. ACS Pharmacol. Transl. Sci. 2021, 4, 533–542. [Google Scholar] [CrossRef]
- Robinson, G.I.; Li, D.; Wang, B.; Zahoruiko, Y.; Gerasymchuk, M.; Hudson, D.; Kovalchuk, O.; Kovalchuk, I. Anti-Inflammatory Effects of Serotonin Receptor and Transient Receptor Potential Channel Ligands in Human Small Intestinal Epithelial Cells. Curr. Issues Mol. Biol. 2023, 45, 6743–6774. [Google Scholar] [CrossRef] [PubMed]
- Rapalli, A.; Bertoni, S.; Arcaro, V.; Saccani, F.; Grandi, A.; Vivo, V.; Cantoni, A.M.; Barocelli, E. Dual Role of Endogenous Serotonin in 2,4,6-Trinitrobenzene Sulfonic Acid-Induced Colitis. Front. Pharmacol. 2016, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Shao, L.; Shen, J.; Jiang, W.; Feng, Y.; Zheng, P.; Liu, F. Effects of ketanserin on experimental colitis in mice and macrophage function. Int. J. Mol. Med. 2016, 37, 659–668. [Google Scholar] [CrossRef]
- Tang, Q.; Li, Z.-Q.; Li, W.; Guo, J.; Sun, H.-Y.; Zhang, X.-H.; Lau, C.-P.; Tse, H.-F.; Zhang, S.; Li, G.-R. The 5-HT2 antagonist ketanserin is an open channel blocker of human cardiac ether-à-go-go-related gene (hERG) potassium channels. Br. J. Pharmacol. 2008, 155, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Aronson, J.K. (Ed.) Ketanserin. In Meyler’s Side Effects of Drugs (Sixteenth Edition); Elsevier: Oxford, UK, 2016; p. 413. ISBN 978-0-444-53716-4. [Google Scholar]
- Pope, J.; Fenlon, D.; Thompson, A.; Shea, B.; Furst, D.; Wells, G.A.; Silman, A. Ketanserin for Raynaud’s phenomenon in progressive systemic sclerosis. Cochrane Database Syst. Rev. 1998, 1998, CD000954. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, Z.; Deng, Y.; Lu, X.; Luo, C.; Mu, X.; Zhang, T.; Liu, Q.; Tang, S.; Li, J.; et al. Function of TRP channels in monocytes/macrophages. Front. Immunol. 2023, 14, 1187890. [Google Scholar] [CrossRef]
- Parenti, A.; De Logu, F.; Geppetti, P.; Benemei, S. What is the evidence for the role of TRP channels in inflammatory and immune cells? Br. J. Pharmacol. 2016, 173, 953–969. [Google Scholar] [CrossRef]
- Horikawa, R.; Oe, Y.; Fujii, R.; Kasuga, R.; Yoshimura, R.; Miyata, S. Effects of peripheral administration of lipopolysaccharide on chronic sickness responses in TRPM8-deficient mice. Neurosci. Lett. 2022, 790, 136895. [Google Scholar] [CrossRef]
- Piciu, F.; Balas, M.; Badea, M.A.; Cucu, D. TRP Channels in Tumoral Processes Mediated by Oxidative Stress and Inflammation. Antioxidants 2023, 12, 1327. [Google Scholar] [CrossRef]
- Zanikov, T.; Gerasymchuk, M.; Ghasemi Gojani, E.; Robinson, G.I.; Asghari, S.; Groves, A.; Haselhorst, L.; Nandakumar, S.; Stahl, C.; Cameron, M.; et al. The Effect of Combined Treatment of Psilocybin and Eugenol on Lipopolysaccharide-Induced Brain Inflammation in Mice. Molecules 2023, 28, 2624. [Google Scholar] [CrossRef] [PubMed]
- Nisar, M.F.; Khadim, M.; Rafiq, M.; Chen, J.; Yang, Y.; Wan, C.C. Pharmacological Properties and Health Benefits of Eugenol: A Comprehensive Review. Oxid. Med. Cell. Longev. 2021, 2021, 2497354. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zheng, Y.; Luo, Y.; Du, Y.; Zhang, X.; Fu, J. Curcumin inhibits LPS-induced neuroinflammation by promoting microglial M2 polarization via TREM2/TLR4/NF-κB pathways in BV2 cells. Mol. Immunol. 2019, 116, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Karthikeyan, A.; Young, K.N.; Moniruzzaman, M.; Beyene, A.M.; Do, K.; Kalaiselvi, S.; Min, T. Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook. Pharmaceutics 2021, 13, 484. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Panel on Food Additives and Nutrient Sources added to Food (ANS) Scientific Opinion on the re-evaluation of curcumin (E 100) as a food additive. EFSA J. 2010, 8, 1679. [Google Scholar] [CrossRef]
- Csekő, K.; Beckers, B.; Keszthelyi, D.; Helyes, Z. Role of TRPV1 and TRPA1 Ion Channels in Inflammatory Bowel Diseases: Potential Therapeutic Targets? Pharmaceutics 2019, 12, 48. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, E.A.; Alvarez-Leite, J.I. Capsaicin: A Potential Therapy Adjuvant for Intestinal Bowel Disease. J. Dig. Disord. Diagn. 2019, 2, 8–16. [Google Scholar] [CrossRef]
- Zhang, Q.; Luo, P.; Xia, F.; Tang, H.; Chen, J.; Zhang, J.; Liu, D.; Zhu, Y.; Liu, Y.; Gu, L.; et al. Capsaicin ameliorates inflammation in a TRPV1-independent mechanism by inhibiting PKM2-LDHA-mediated Warburg effect in sepsis. Cell Chem. Biol. 2022, 29, 1248–1259.e6. [Google Scholar] [CrossRef]
- Kang, C.; Wang, B.; Kaliannan, K.; Wang, X.; Lang, H.; Hui, S.; Huang, L.; Zhang, Y.; Zhou, M.; Chen, M.; et al. Gut Microbiota Mediates the Protective Effects of Dietary Capsaicin against Chronic Low-Grade Inflammation and Associated Obesity Induced by High-Fat Diet. mBio 2017, 8, e00470-17. [Google Scholar] [CrossRef]
- Arnold, J.T.; Stewart, S.B.-L.; Sammut, L. Oral Capsaicin Ingestion: A Brief Update Dose, Tolerance and Side Effects. Res. Rev. J. Herb. Sci. 2018, 5, 1–5. [Google Scholar]
- Berg, K.A.; Maayani, S.; Goldfarb, J.; Clarke, W.P. Pleiotropic behavior of 5-HT2A and 5-HT2C receptor agonists. Ann. N. Y. Acad. Sci. 1998, 861, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Markus, J.; Landry, T.; Stevens, Z.; Scott, H.; Llanos, P.; Debatis, M.; Armento, A.; Klausner, M.; Ayehunie, S. Human small intestinal organotypic culture model for drug permeation, inflammation, and toxicity assays. In Vitro Cell. Dev. Biol. Anim. 2021, 57, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Kovalchuk, A.; Wang, B.; Li, D.; Rodriguez-Juarez, R.; Ilnytskyy, S.; Kovalchuk, I.; Kovalchuk, O. Fighting the storm: Could novel anti-TNFα and anti-IL-6 C. sativa cultivars tame cytokine storm in COVID-19? Aging 2021, 13, 1571–1590. [Google Scholar] [CrossRef]
- Woznicki, J.A.; Saini, N.; Flood, P.; Rajaram, S.; Lee, C.M.; Stamou, P.; Skowyra, A.; Bustamante-Garrido, M.; Regazzoni, K.; Crawford, N.; et al. TNF-α synergises with IFN-γ to induce caspase-8-JAK1/2-STAT1-dependent death of intestinal epithelial cells. Cell Death Dis. 2021, 12, 864. [Google Scholar] [CrossRef] [PubMed]
- Chen, C. COX-2′s new role in inflammation. Nat. Chem. Biol. 2010, 6, 401–402. [Google Scholar] [CrossRef]
- Ricciotti, E.; FitzGerald, G.A. Prostaglandins and Inflammation. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 986–1000. [Google Scholar] [CrossRef]
- Kontoyiannis, D.; Pasparakis, M.; Pizarro, T.T.; Cominelli, F.; Kollias, G. Impaired On/Off Regulation of TNF Biosynthesis in Mice Lacking TNF AU-Rich Elements: Implications for Joint and Gut-Associated Immunopathologies. Immunity 1999, 10, 387–398. [Google Scholar] [CrossRef]
- Schmitt, H.; Billmeier, U.; Dieterich, W.; Rath, T.; Sonnewald, S.; Reid, S.; Hirschmann, S.; Hildner, K.; Waldner, M.J.; Mudter, J.; et al. Expansion of IL-23 receptor bearing TNFR2+ T cells is associated with molecular resistance to anti-TNF therapy in Crohn’s disease. Gut 2019, 68, 814–828. [Google Scholar] [CrossRef]
- Ivashkiv, L.B. IFNγ: Signalling, epigenetics and roles in immunity, metabolism, disease and cancer immunotherapy. Nat. Rev. Immunol. 2018, 18, 545–558. [Google Scholar] [CrossRef]
- Thapa, R.J.; Basagoudanavar, S.H.; Nogusa, S.; Irrinki, K.; Mallilankaraman, K.; Slifker, M.J.; Beg, A.A.; Madesh, M.; Balachandran, S. NF-kappaB protects cells from gamma interferon-induced RIP1-dependent necroptosis. Mol. Cell. Biol. 2011, 31, 2934–2946. [Google Scholar] [CrossRef]
- Thapa, R.J.; Nogusa, S.; Chen, P.; Maki, J.L.; Lerro, A.; Andrake, M.; Rall, G.F.; Degterev, A.; Balachandran, S. Interferon-induced RIP1/RIP3-mediated necrosis requires PKR and is licensed by FADD and caspases. Proc. Natl. Acad. Sci. USA 2013, 110, E3109–E3118. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.P.; Thapa, R.J.; Fisher, A.; Tummers, B.; Zhang, T.; Yin, C.; Rodriguez, D.A.; Guo, H.; Lane, R.; Williams, R.; et al. ZBP1/DAI Drives RIPK3-Mediated Cell Death Induced by IFNs in the Absence of RIPK1. J. Immunol. 2019, 203, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Fuss, I.J.; Neurath, M.; Boirivant, M.; Klein, J.S.; de la Motte, C.; Strong, S.A.; Fiocchi, C.; Strober, W. Disparate CD4+ lamina propria (LP) lymphokine secretion profiles in inflammatory bowel disease. Crohn’s disease LP cells manifest increased secretion of IFN-gamma, whereas ulcerative colitis LP cells manifest increased secretion of IL-5. J. Immunol. 1996, 157, 1261–1270. [Google Scholar] [CrossRef]
- Breese, E.; Braegger, C.P.; Corrigan, C.J.; Walker-Smith, J.A.; MacDonald, T.T. Interleukin-2- and interferon-gamma-secreting T cells in normal and diseased human intestinal mucosa. Immunology 1993, 78, 127–131. [Google Scholar] [PubMed]
- Camoglio, L.; Te Velde, A.A.; Tigges, A.J.; Das, P.K.; Van Deventer, S.J. Altered expression of interferon-gamma and interleukin-4 in inflammatory bowel disease. Inflamm. Bowel Dis. 1998, 4, 285–290. [Google Scholar] [CrossRef]
- Deem, R.L.; Shanahan, F.; Targan, S.R. Triggered human mucosal T cells release tumour necrosis factor-alpha and interferon-gamma which kill human colonic epithelial cells. Clin. Exp. Immunol. 1991, 83, 79–84. [Google Scholar] [CrossRef]
- Bruewer, M.; Luegering, A.; Kucharzik, T.; Parkos, C.A.; Madara, J.L.; Hopkins, A.M.; Nusrat, A. Proinflammatory cytokines disrupt epithelial barrier function by apoptosis-independent mechanisms. J. Immunol. 2003, 171, 6164–6172. [Google Scholar] [CrossRef]
- Mitsuyama, K.; Toyonaga, A.; Sasaki, E.; Ishida, O.; Ikeda, H.; Tsuruta, O.; Harada, K.; Tateishi, H.; Nishiyama, T.; Tanikawa, K. Soluble interleukin-6 receptors in inflammatory bowel disease: Relation to circulating interleukin-6. Gut 1995, 36, 45–49. [Google Scholar] [CrossRef]
- Atreya, R.; Mudter, J.; Finotto, S.; Müllberg, J.; Jostock, T.; Wirtz, S.; Schütz, M.; Bartsch, B.; Holtmann, M.; Becker, C.; et al. Blockade of interleukin 6 trans signaling suppresses T-cell resistance against apoptosis in chronic intestinal inflammation: Evidence in Crohn disease and experimental colitis in vivo. Nat. Med. 2000, 6, 583–588. [Google Scholar] [CrossRef]
- Ghandadi, M.; Sahebkar, A. Curcumin: An Effective Inhibitor of Interleukin-6. Curr. Pharm. Des. 2017, 23, 921–931. [Google Scholar] [CrossRef]
- Gorabi, A.M.; Razi, B.; Aslani, S.; Abbasifard, M.; Imani, D.; Sathyapalan, T.; Sahebkar, A. Effect of curcumin on proinflammatory cytokines: A meta-analysis of randomized controlled trials. Cytokine 2021, 143, 155541. [Google Scholar] [CrossRef]
- Takada, Y.; Hisamatsu, T.; Kamada, N.; Kitazume, M.T.; Honda, H.; Oshima, Y.; Saito, R.; Takayama, T.; Kobayashi, T.; Chinen, H.; et al. Monocyte Chemoattractant Protein-1 Contributes to Gut Homeostasis and Intestinal Inflammation by Composition of IL-10–Producing Regulatory Macrophage Subset. J. Immunol. 2010, 184, 2671–2676. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Kwon, T.K. Curcumin inhibits phorbol myristate acetate (PMA)-induced MCP-1 expression by inhibiting ERK and NF-kappaB transcriptional activity. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2010, 48, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Karimian, M.S.; Pirro, M.; Majeed, M.; Sahebkar, A. Curcumin as a natural regulator of monocyte chemoattractant protein-1. Cytokine Growth Factor Rev. 2017, 33, 55–63. [Google Scholar] [CrossRef]
- Ariki, S.; Ozaka, S.; Sachi, N.; Chalalai, T.; Soga, Y.; Fukuda, C.; Kagoshima, Y.; Ekronarongchai, S.; Mizukami, K.; Kamiyama, N.; et al. GM-CSF-producing CCR2+ CCR6+ Th17 cells are pathogenic in dextran sodium sulfate-induced colitis model in mice. Genes Cells 2023, 28, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Ebbo, M.; Crinier, A.; Vély, F.; Vivier, E. Innate lymphoid cells: Major players in inflammatory diseases. Nat. Rev. Immunol. 2017, 17, 665–678. [Google Scholar] [CrossRef] [PubMed]
- Önal, H.T.; Yetkin, D.; Ayaz, F. Immunostimulatory activity of fluoxetine in macrophages via regulation of the PI3K and P38 signaling pathways. Immunol. Res. 2023, 71, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Dong, B.; Friesen, M.; Liu, S.; Zhu, C.; Yang, C. Capsaicin Attenuates Lipopolysaccharide-Induced Inflammation and Barrier Dysfunction in Intestinal Porcine Epithelial Cell Line-J2. Front. Physiol. 2021, 12, 715469. [Google Scholar] [CrossRef]
- Azimirad, M.; Noori, M.; Azimirad, F.; Gholami, F.; Naseri, K.; Yadegar, A.; Asadzadeh Aghdaei, H.; Zali, M.R. Curcumin and capsaicin regulate apoptosis and alleviate intestinal inflammation induced by Clostridioides difficile in vitro. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 41. [Google Scholar] [CrossRef]
- Cione, E.; Plastina, P.; Pingitore, A.; Perri, M.; Caroleo, M.C.; Fazio, A.; Witkamp, R.; Meijerink, J. Capsaicin Analogues Derived from n-3 Polyunsaturated Fatty Acids (PUFAs) Reduce Inflammatory Activity of Macrophages and Stimulate Insulin Secretion by β-Cells In Vitro. Nutrients 2019, 11, 915. [Google Scholar] [CrossRef]
- Kunde, D.A.; Yingchoncharoen, J.; Jurković, S.; Geraghty, D.P. TRPV1 mediates capsaicin-stimulated metabolic activity but not cell death or inhibition of interleukin-1β release in human THP-1 monocytes. Toxicol. Appl. Pharmacol. 2018, 360, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Calzetta, L.; Pistocchini, E.; Cito, G.; Ritondo, B.L.; Verri, S.; Rogliani, P. Inflammatory and contractile profile in LPS-challenged equine isolated bronchi: Evidence for IL-6 as a potential target against AHR in equine asthma. Pulm. Pharmacol. Ther. 2022, 73–74, 102125. [Google Scholar] [CrossRef] [PubMed]
- Rodriguiz, R.M.; Nadkarni, V.; Means, C.R.; Pogorelov, V.M.; Chiu, Y.-T.; Roth, B.L.; Wetsel, W.C. LSD-stimulated behaviors in mice require β-arrestin 2 but not β-arrestin 1. Sci. Rep. 2021, 11, 17690. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Parameswaran, N. Multifaceted role of β-arrestins in inflammation and disease. Genes Immun. 2015, 16, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Cheshmehkani, A.; Senatorov, I.S.; Dhuguru, J.; Ghoneim, O.; Moniri, N.H. Free-fatty acid receptor-4 (FFA4) modulates ROS generation and COX-2 expression via the C-terminal β-arrestin phosphosensor in Raw 264.7 macrophages. Biochem. Pharmacol. 2017, 146, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Chen, X.; Chen, D.; Yu, B.; He, J.; Yan, H.; Luo, Y.; Zheng, P.; Chen, H.; Huang, Z. Eugenol promotes appetite through TRP channels mediated-CaMKK2/AMPK signaling pathway. Phytother. Res. 2023, 37, 2759–2770. [Google Scholar] [CrossRef]
- Racioppi, L.; Nelson, E.R.; Huang, W.; Mukherjee, D.; Lawrence, S.A.; Lento, W.; Masci, A.M.; Jiao, Y.; Park, S.; York, B.; et al. CaMKK2 in myeloid cells is a key regulator of the immune-suppressive microenvironment in breast cancer. Nat. Commun. 2019, 10, 2450. [Google Scholar] [CrossRef]
- Fedi, A.; Vitale, C.; Ponschin, G.; Ayehunie, S.; Fato, M.; Scaglione, S. In vitro models replicating the human intestinal epithelium for absorption and metabolism studies: A systematic review. J. Control. Release 2021, 335, 247–268. [Google Scholar] [CrossRef]
- Cao, D.; Yu, J.; Wang, H.; Luo, Z.; Liu, X.; He, L.; Qi, J.; Fan, L.; Tang, L.; Chen, Z.; et al. Structure-based discovery of nonhallucinogenic psychedelic analogs. Science 2022, 375, 403–411. [Google Scholar] [CrossRef]
- González-Maeso, J.; Weisstaub, N.V.; Zhou, M.; Chan, P.; Ivic, L.; Ang, R.; Lira, A.; Bradley-Moore, M.; Ge, Y.; Zhou, Q.; et al. Hallucinogens recruit specific cortical 5-HT(2A) receptor-mediated signaling pathways to affect behavior. Neuron 2007, 53, 439–452. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, X.; Zhou, J.-X.; Wei, W.; Liu, D.-H.; Ke, P.; Zhang, G.-F.; Cai, G.-J.; Su, D.-F. The protective action of ketanserin against lipopolysaccharide-induced shock in mice is mediated by inhibiting inducible NO synthase expression via the MEK/ERK pathway. Free Radic. Biol. Med. 2013, 65, 658–666. [Google Scholar] [CrossRef]
- Sengupta, T.K.; Talbot, E.S.; Scherle, P.A.; Ivashkiv, L.B. Rapid inhibition of interleukin-6 signaling and Stat3 activation mediated by mitogen-activated protein kinases. Proc. Natl. Acad. Sci. USA 1998, 95, 11107–11112. [Google Scholar] [CrossRef]
- Seidel, M.F.; Fiebich, B.L.; Ulrich-Merzenich, G.; Candelario-Jalil, E.; Koch, F.-W.; Vetter, H. Serotonin mediates PGE2 overexpression through 5-HT2A and 5-HT3 receptor subtypes in serum-free tissue culture of macrophage-like synovial cells. Rheumatol. Int. 2008, 28, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Cloëz-Tayarani, I.; Petit-Bertron, A.-F.; Venters, H.D.; Cavaillon, J.-M. Differential effect of serotonin on cytokine production in lipopolysaccharide-stimulated human peripheral blood mononuclear cells: Involvement of 5-hydroxytryptamine2A receptors. Int. Immunol. 2003, 15, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Srikiatkhachorn, A.; Anthony, M.; Chong, B.H. Serotonin stimulates megakaryocytopoiesis via the 5-HT2 receptor. Blood Coagul. Fibrinolysis 1996, 7, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Sviridova, A.; Rogovskii, V.; Kudrin, V.; Pashenkov, M.; Boyko, A.; Melnikov, M. The role of 5-HT2B-receptors in fluoxetine-mediated modulation of Th17- and Th1-cells in multiple sclerosis. J. Neuroimmunol. 2021, 356, 577608. [Google Scholar] [CrossRef] [PubMed]
- Tylš, F.; Páleníček, T.; Horáček, J. Psilocybin—Summary of knowledge and new perspectives. Eur. Neuropsychopharmacol. 2014, 24, 342–356. [Google Scholar] [CrossRef]
- Jones, N.T.; Zahid, Z.; Grady, S.M.; Sultan, Z.W.; Zheng, Z.; Razidlo, J.; Banks, M.I.; Wenthur, C.J. Transient Elevation of Plasma Glucocorticoids Supports Psilocybin-Induced Anxiolysis in Mice. ACS Pharmacol. Transl. Sci. 2023, 6, 1221–1231. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Sun, S.; Wang, P.; Sun, Y.; Hu, Q.; Wang, X. The Mechanism of Secretion and Metabolism of Gut-Derived 5-Hydroxytryptamine. Int. J. Mol. Sci. 2021, 22, 7931. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Barbara, G.; Buurman, W.; Ockhuizen, T.; Schulzke, J.-D.; Serino, M.; Tilg, H.; Watson, A.; Wells, J.M. Intestinal permeability—A new target for disease prevention and therapy. BMC Gastroenterol. 2014, 14, 189. [Google Scholar] [CrossRef]
- Wang, B.; Sun, S.; Liu, M.; Chen, H.; Liu, N.; Wu, Z.; Wu, G.; Dai, Z. Dietary L-Tryptophan Regulates Colonic Serotonin Homeostasis in Mice with Dextran Sodium Sulfate-Induced Colitis. J. Nutr. 2020, 150, 1966–1976. [Google Scholar] [CrossRef] [PubMed]
- Koopman, N.; Katsavelis, D.; ten Hove, A.S.; Brul, S.; de Jonge, W.J.; Seppen, J. The Multifaceted Role of Serotonin in Intestinal Homeostasis. Int. J. Mol. Sci. 2021, 22, 9487. [Google Scholar] [CrossRef] [PubMed]
- Nau, F.; Yu, B.; Martin, D.; Nichols, C.D. Serotonin 5-HT2A Receptor Activation Blocks TNF-α Mediated Inflammation In Vivo. PLoS ONE 2013, 8, e75426. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Xin, F.; Ren, J.; Xu, S.; Huang, H.; Zha, X.; Wen, X.; Gu, G.; Yang, G.; Cheng, Y.; et al. 5-HT2B-mediated serotonin activation in enterocytes suppresses colitis-associated cancer initiation and promotes cancer progression. Theranostics 2022, 12, 3928–3945. [Google Scholar] [CrossRef]
- Lee, S.H.; eun Kwon, J.; Cho, M.-L. Immunological pathogenesis of inflammatory bowel disease. Intest. Res. 2018, 16, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Zinberg, N.E. Drug, Set, and Setting: The Basis for Controlled Intoxicant Use; Yale University Press: New Haven, CT, USA, 1986; ISBN 978-0-300-03634-3. [Google Scholar]
- Schlag, A.K.; Aday, J.; Salam, I.; Neill, J.C.; Nutt, D.J. Adverse effects of psychedelics: From anecdotes and misinformation to systematic science. J. Psychopharmacol. Oxf. Engl. 2022, 36, 258–272. [Google Scholar] [CrossRef]
- Irizarry, R.; Winczura, A.; Dimassi, O.; Dhillon, N.; Minhas, A.; Larice, J. Psilocybin as a Treatment for Psychiatric Illness: A Meta-Analysis. Cureus 2022, 14, e31796. [Google Scholar] [CrossRef]
- Ona, G.; Bouso, J.C. Potential safety, benefits, and influence of the placebo effect in microdosing psychedelic drugs: A systematic review. Neurosci. Biobehav. Rev. 2020, 119, 194–203. [Google Scholar] [CrossRef]
- Kuypers, K.P.C. The therapeutic potential of microdosing psychedelics in depression. Ther. Adv. Psychopharmacol. 2020, 10, 2045125320950567. [Google Scholar] [CrossRef]
- Mortensen, J.K.; Andersen, G. Safety considerations for prescribing SSRI antidepressants to patients at increased cardiovascular risk. Expert Opin. Drug Saf. 2022, 21, 467–475. [Google Scholar] [CrossRef]
- Ledwos, N.; Rosenblat, J.D.; Blumberger, D.M.; Castle, D.J.; McIntyre, R.S.; Mulsant, B.H.; Husain, M.I. A Critical Appraisal of Evidence on the Efficacy and Safety of Serotonergic Psychedelic Drugs as Emerging Antidepressants: Mind the Evidence Gap. J. Clin. Psychopharmacol. 2022, 42, 581–588. [Google Scholar] [CrossRef]
- Rosenblat, J.D.; Husain, M.I.; Lee, Y.; McIntyre, R.S.; Mansur, R.B.; Castle, D.; Offman, H.; Parikh, S.V.; Frey, B.N.; Schaffer, A.; et al. The Canadian Network for Mood and Anxiety Treatments (CANMAT) Task Force Report: Serotonergic Psychedelic Treatments for Major Depressive Disorder. Can. J. Psychiatry 2023, 68, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Leon, A.; Escamilla-Orozco, R.I.; Tabal-Robles, A.R.; Martínez-Vargas, D.; Romero-Bautista, L.; Escamilla-Soto, G.; González-Romero, O.S.; Torres-Valencia, M.; González-Trujano, M.E. Antidepressant- and anxiolytic-like activities and acute toxicity evaluation of the Psilocybe cubensis mushroom in experimental models in mice. J. Ethnopharmacol. 2024, 320, 117415. [Google Scholar] [CrossRef] [PubMed]
- Lam, N.T.; Balachandran, K. The mechanobiology of drug-induced cardiac valve disease. J. Long. Term Eff. Med. Implants 2015, 25, 27–40. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S. Serotonin 5-HT2B receptor agonism and valvular heart disease: Implications for the development of psilocybin and related agents. Expert Opin. Drug Saf. 2023, 22, 881–883. [Google Scholar] [CrossRef] [PubMed]
- Rickli, A.; Moning, O.D.; Hoener, M.C.; Liechti, M.E. Receptor interaction profiles of novel psychoactive tryptamines compared with classic hallucinogens. Eur. Neuropsychopharmacol. 2016, 26, 1327–1337. [Google Scholar] [CrossRef] [PubMed]
- Glatfelter, G.C.; Pham, D.N.K.; Walther, D.; Golen, J.A.; Chadeayne, A.R.; Baumann, M.H.; Manke, D.R. Synthesis, Structural Characterization, and Pharmacological Activity of Novel Quaternary Salts of 4-Substituted Tryptamines. ACS Omega 2022, 7, 24888–24894. [Google Scholar] [CrossRef] [PubMed]
- Dahmane, E.; Hutson, P.R.; Gobburu, J.V.S. Exposure-Response Analysis to Assess the Concentration-QTc Relationship of Psilocybin/Psilocin. Clin. Pharmacol. Drug Dev. 2021, 10, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Mawe, G.M.; Hoffman, J.M. Serotonin Signaling in the Gastrointestinal Tract: Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 473–486. [Google Scholar] [CrossRef]
- Fiorica-Howells, E.; Hen, R.; Gingrich, J.; Li, Z.; Gershon, M.D. 5-HT2A receptors: Location and functional analysis in intestines of wild-type and 5-HT2A knockout mice. Am. J. Physiol.-Gastrointest. Liver Physiol. 2002, 282, G877–G893. [Google Scholar] [CrossRef]
- Panpetch, W.; Visitchanakun, P.; Saisorn, W.; Sawatpanich, A.; Chatthanathon, P.; Somboonna, N.; Tumwasorn, S.; Leelahavanichkul, A. Lactobacillus rhamnosus attenuates Thai chili extracts induced gut inflammation and dysbiosis despite capsaicin bactericidal effect against the probiotics, a possible toxicity of high dose capsaicin. PLoS ONE 2021, 16, e0261189. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.; Blesso, C.N.; Barreto, G.E.; Banach, M.; Majeed, M.; Sahebkar, A. Macrophage plasticity, polarization and function in response to curcumin, a diet-derived polyphenol, as an immunomodulatory agent. J. Nutr. Biochem. 2019, 66, 1–16. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | TNF-α | IFN-γ | IL-6 | IL-8 | MCP-1 | GM-CSF |
|---|---|---|---|---|---|---|
| TNF/IFN + 10 μM Psi | −55.0× **** | −16.7× * | −1.9× * | −1.4× * | −1.5× | −2.0× * |
| TNF/IFN + 25 μM Eug | −8.8× **** | −17.0× * | −1.7× * | −1.3× * | −1.1× | 1.0× |
| TNF/IFN + 10 μM Psi + 25 μM Eug | −6.9× **** | −11.5× ** | −1.5× | −1.3× | 1.2× | −1.4× |
| TNF/IFN + 0.5 μM Cur | −48.2× *** | −23.2× *** | −1.4× | −1.2× | −1.0× | −1.1× |
| TNF/IFN + 10 μM Psi + 0.5 μM Cur | −30.7× *** | −21.7× *** | −1.3× | −1.2× | 1.1× | 1.2× |
| TNF/IFN + 0.5 μM Cap | −28.8× **** | −74.9× * | −1.8× * | −1.2× | −1.2× | −1.3× |
| TNF/IFN + 10 μM Psi + 0.5 μM Cap | −13.2× **** | −196.9× ** | −1.8× * | −1.2× | 1.2× | −1.8× * |
| TNF/IFN + 20 μM Psi | −39.2× **** | −55.9× * | −2.5× ** | −1.6× ** | −2.0× | −7.2× *** |
| TNF/IFN + 20 μM Psi + 25 μM Eug | −2.2× **** | −2.5× * | −1.7× | −1.2× | 1.2× | −1.4× |
| TNF/IFN + 20 μM Psi + 0.5 μM Cur | −3.8× *** | −13.6× *** | −1.7× | −1.3× | −1.4× | −2.0× ** |
| TNF/IFN + 20 μM Psi + 0.5 μM Cap | −5.8× **** | −9.0× * | −1.6× * | −1.0× | −1.0× | −1.6× |
| TNF/IFN + 40 μM Psi | −13.7× **** | −9.5× * | −1.8× * | −1.4× * | −1.2× | −1.3× |
| TNF/IFN + 40 μM Psi + 25 μM Eug | −21.0× **** | −62.5× * | −1.3× | −1.3× * | −1.6× | −1.5× |
| TNF/IFN + 40 μM Psi + 0.5 μM Cap | −20.0× **** | −36.7× * | −1.7× * | −1.1× | 1.1× | 1.0× |
| TNF/IFN + 20 μm 4-AcO-DMT | −17.5× *** | −17.9× *** | −1.4× | −1.2× | −1.0× | 1.1× |
| TNF/IFN + 25 μM Eug | −49.7× *** | −20.8× **** | −1.8× * | −1.1× | −1.6× | −1.9× |
| TNF/IFN + 20 μm 4-AcO-DMT + 25 μm Eug | −30.0× *** | −10.6× *** | −1.6× | −1.1× | 1.0× | −1.8× |
| TNF/IFN + 40 μm 4-AcO-DMT | −5.9× ** | −36.0× **** | −1.4× | −1.2× | 1.0× | −1.7× |
| TNF/IFN + 40 μm 4-AcO-DMT + 25 μm Eug | −8.8× ** | −30.6× **** | −1.7× | −1.3× | −1.4× | −1.1× |
| TNF/IFN + 1 μM Ket | −3.6× | −9.7× | −1.5× | −1.2× | −1.0× | −1.9× |
| TNF/IFN + 25 μM Eug | −37.3× | −55.6× | −1.6× | −1.1× | −1.2× | −1.5× |
| TNF/IFN + 1 μM Ket + 25 µM Eug | 1.5× | 12.6× | −2.5× ** | −1.5× | 1.5× | −4.4× ** |
| TNF/IFN + 5 μM Ket | −2.1× | −2.2× | −1.6× | −1.2× | −1.6× | −3.1× * |
| TNF/IFN + 5 μM Ket + 25 µM Eug | −1.9× | −1.2× | −1.7× | −1.2× | −1.5× | −2.6× * |
| TNF/IFN + 10 μM Ket | −8.8× | −7.8× | −2.7× ** | −1.3× | −2.8× | −9.9× ** |
| TNF/IFN + 10 μM Ket + 25 µM Eug | 1.4× | 3.7× | −1.6× | −1.1× | −1.3× | −2.8× * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robinson, G.I.; Li, D.; Wang, B.; Rahman, T.; Gerasymchuk, M.; Hudson, D.; Kovalchuk, O.; Kovalchuk, I. Psilocybin and Eugenol Reduce Inflammation in Human 3D EpiIntestinal Tissue. Life 2023, 13, 2345. https://doi.org/10.3390/life13122345
Robinson GI, Li D, Wang B, Rahman T, Gerasymchuk M, Hudson D, Kovalchuk O, Kovalchuk I. Psilocybin and Eugenol Reduce Inflammation in Human 3D EpiIntestinal Tissue. Life. 2023; 13(12):2345. https://doi.org/10.3390/life13122345
Chicago/Turabian StyleRobinson, Gregory Ian, Dongping Li, Bo Wang, Tahiat Rahman, Marta Gerasymchuk, Darryl Hudson, Olga Kovalchuk, and Igor Kovalchuk. 2023. "Psilocybin and Eugenol Reduce Inflammation in Human 3D EpiIntestinal Tissue" Life 13, no. 12: 2345. https://doi.org/10.3390/life13122345
APA StyleRobinson, G. I., Li, D., Wang, B., Rahman, T., Gerasymchuk, M., Hudson, D., Kovalchuk, O., & Kovalchuk, I. (2023). Psilocybin and Eugenol Reduce Inflammation in Human 3D EpiIntestinal Tissue. Life, 13(12), 2345. https://doi.org/10.3390/life13122345