
Exploring the Interplay of Muscular Endurance, Functional Balance, and Limits of Stability: A Comparative Study in Individuals with Lumbar Spondylosis Using a Computerized Stabilometric Force Platform


 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Settings, and Ethics
2.2. Participants
2.3. Outcome Measures
2.3.1. Lumbar Extensor Endurance
2.3.2. Functional Balance
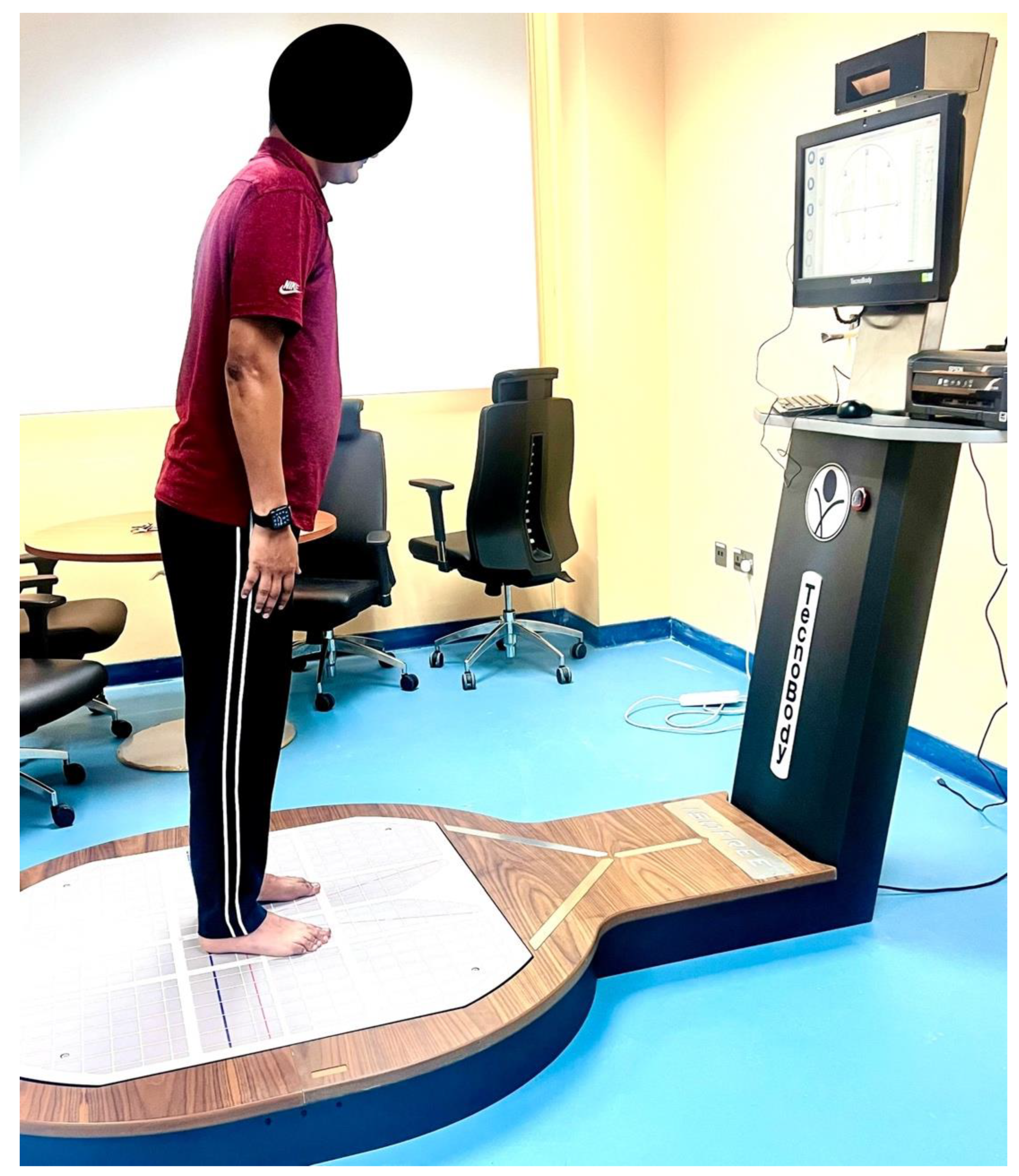
2.3.3. Limits of Stability Assessment
- Ellipse Area (mm2): This metric quantifies the area enclosed by the trajectory of the COP during the limits of stability test. It reflects how effectively an individual can shift their body weight within their base of support. Larger Ellipse Area values indicate greater COP displacement and signify challenges in maintaining postural stability.
- A–P Sway (mm): A–P sway measures anterior–posterior COP and body sway. It assesses an individual’s control over forward and backward movements. Increased A–P sway values indicate heightened instability along the sagittal plane.
- M–L Sway (mm): M–L sway quantifies medial–lateral COP and body sway, evaluating control over lateral movements. Elevated M–L sway values denote increased instability along the frontal plane.
2.4. Sample Size Calculation
2.5. Data Analysis
3. Results
4. Discussion
4.1. Limitations of the Study
4.2. Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Theodore, N. Degenerative cervical spondylosis. N. Engl. J. Med. 2020, 383, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Ashinsky, B.; Smith, H.; Mauck, R.; Gullbrand, S. Intervertebral disc degeneration and regeneration: A motion segment perspective. Eur. Cells Mater. 2021, 41, 370. [Google Scholar] [CrossRef] [PubMed]
- Badhiwala, J.H.; Ahuja, C.S.; Akbar, M.A.; Witiw, C.D.; Nassiri, F.; Furlan, J.C.; Curt, A.; Wilson, J.R.; Fehlings, M.G. Degenerative cervical myelopathy—Update and future directions. Nat. Rev. Neurol. 2020, 16, 108–124. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, K.A.; Rengaramanujam, K.; Reddy, R.S.; Samuel, P.S.; Tedla, J.S.; Kakaraparthi, V.N.; Ahmad, I. The immediate and short-term effects of dynamic taping on pain, endurance, disability, mobility and kinesiophobia in individuals with chronic non-specific low back pain: A randomized controlled trial. PloS ONE 2020, 15, e0239505. [Google Scholar] [CrossRef]
- ALMohiza, M.A.; Reddy, R.S.; Asiri, F.; Alshahrani, A.; Tedla, J.S.; Dixit, S.; Gular, K.; Kakaraparthi, V.N. The Mediation Effect of Pain on the Relationship between Kinesiophobia and Lumbar Joint Position Sense in Chronic Low Back Pain Individuals: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 5193. [Google Scholar] [CrossRef]
- Reddy, R.S.; Alahmari, K.A.; Samuel, P.S.; Tedla, J.S.; Kakaraparthi, V.N.; Rengaramanujam, K. Intra-rater and inter-rater reliability of neutral and target lumbar positioning tests in subjects with and without non-specific lower back pain. J. Back Musculoskelet. Rehabil. 2021, 34, 289–299. [Google Scholar] [CrossRef]
- Samanta, A.; Lufkin, T.; Kraus, P. Intervertebral disc degeneration—Current therapeutic options and challenges. Front. Public Health 2023, 11, 1156749. [Google Scholar] [CrossRef]
- Zahari, Z.; Azan, S.A.S.; Imran, N.F.A. Effectiveness of Lumbar Stabilization Exercise on Pain, Disability and Functional Performance among Older People with Low Back Pain: A Systematic Review. Malays. J. Med. Health Sci. 2023, 19, 307–314. [Google Scholar] [CrossRef]
- Fallahasady, E.; Rahmanloo, N.; Seidi, F.; Rajabi, R.; Bayattork, M. The relationship between core muscle endurance and functional movement screen scores in females with lumbar hyperlordosis: A cross-sectional study. BMC Sport. Sci. Med. Rehabil. 2022, 14, 182. [Google Scholar] [CrossRef]
- Alahmari, K.A.; Reddy, R.S.; Silvian, P.; Ahmad, I.; Kakarparthi, V.N.; Rengaramanujam, K. Intra and inter-rater reliability for deep neck flexor and neck extensor muscle endurance tests in subjects with and without subclinical neck pain. Phys. Med. Rehabil. Kurortmed. 2019, 58, 310–316. [Google Scholar] [CrossRef]
- Keshavarzi, F.; Azadinia, F.; Talebian, S.; Rasouli, O. Impairments in trunk muscles performance and proprioception in older adults with hyperkyphosis. J. Man. Manip. Ther. 2022, 30, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Studnicka, K.; Ampat, G. Lumbar Stabilization. In StatPearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2021. [Google Scholar]
- Justine, M. Prevalence and Factors Associated with Sarcopenia in Older Adults with Low Back Pain: A Scoping Review. Aging Med. Healthc. 2022, in press. [Google Scholar]
- Shah, A.; Lemans, J.V.; Zavatsky, J.; Agarwal, A.; Kruyt, M.C.; Matsumoto, K.; Serhan, H.; Agarwal, A.; Goel, V.K. Spinal balance/alignment—Clinical relevance and biomechanics. J. Biomech. Eng. 2019, 141, 070805. [Google Scholar] [CrossRef]
- Ito, T.; Sakai, Y.; Ito, Y.; Yamazaki, K.; Morita, Y. Association between back muscle strength and proprioception or mechanoreceptor control strategy in postural balance in elderly adults with lumbar spondylosis. Healthcare 2020, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.; Niu, W.-X.; Zeng, Z.-L.; Tong, J.-H.; Zhen, Z.-W.; Zhou, S.; Yu, Y.; Cheng, L.-M. The effects of muscle weakness on degenerative spondylolisthesis: A finite element study. Clin. Biomech. 2017, 41, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Hellesnes, J.; Brox, J.I. Reliability of the isokinetic trunk extensor test, Biering-Sørensen test, and Åstrand bicycle test: Assessment of intraclass correlation coefficient and critical difference in patients with chronic low back pain and healthy individuals. Spine 2001, 26, 771–777. [Google Scholar] [CrossRef]
- Kothapalli, M. The Biering–Sorensen test as a screening tool to observe lower back muscle strength and sub-clinical back strain in computer users: A cross sectional study. Health Sport. Rehabil. Med. 2023, 24, 78–81. [Google Scholar] [CrossRef]
- Thomas, E.; Battaglia, G.; Patti, A.; Brusa, J.; Leonardi, V.; Palma, A.; Bellafiore, M. Physical activity programs for balance and fall prevention in elderly: A systematic review. Medicine 2019, 98, e16218. [Google Scholar] [CrossRef]
- Дідo, Ю.; Дулo, О.; Гoтoвський, Р.; Григус, І. Effect of the goal-oriented physical therapy and ergotherapy tasks and dual task activities on the Berg balance scale and balance indicators in patients with the unilateral neglect. J. Phys. Educ. Sport 2021, 21, 1234–1241. [Google Scholar]
- Johansson, J.; Jarocka, E.; Westling, G.; Nordström, A.; Nordström, P. Predicting incident falls: Relationship between postural sway and limits of stability in older adults. Hum. Mov. Sci. 2019, 66, 117–123. [Google Scholar] [CrossRef]
- Alahmari, K.A.; Kakaraparthi, V.N.; Reddy, R.S.; Silvian, P.; Tedla, J.S.; Rengaramanujam, K.; Ahmad, I. Combined effects of strengthening and proprioceptive training on stability, balance, and proprioception among subjects with chronic ankle instability in different age groups: Evaluation of clinical outcome measures. Indian J. Orthop. 2021, 55, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Hollick, R.J.; Stelfox, K.; Dean, L.E.; Shim, J.; Walker-Bone, K.; Macfarlane, G.J. Outcomes and treatment responses, including work productivity, among people with axial spondyloarthritis living in urban and rural areas: A mixed-methods study within a national register. Ann. Rheum. Dis. 2020, 79, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ferrante, S.; Teli, M.; Rocca, B.; Foti, C.; Lovi, A.; Brayda Bruno, M. Management of catastrophising and kinesiophobia improves rehabilitation after fusion for lumbar spondylolisthesis and stenosis. A randomised controlled trial. Eur. Spine J. 2014, 23, 87–95. [Google Scholar] [CrossRef]
- Willey, J.S.; Britten, R.A.; Blaber, E.; Tahimic, C.G.; Chancellor, J.; Mortreux, M.; Sanford, L.D.; Kubik, A.J.; Delp, M.D.; Mao, X.W. The individual and combined effects of spaceflight radiation and microgravity on biologic systems and functional outcomes. J. Environ. Sci. Health Part C 2021, 39, 129–179. [Google Scholar] [CrossRef] [PubMed]
- Tufail, M.; Lee, H.; Moon, Y.; Kim, H.; Kim, K. Interdisciplinary Co-Design Research Practice in the Rehabilitation of Elderly Individuals with Chronic Low Back Pain from a Senior Care Center in South Korea. Appl. Sci. 2022, 12, 4687. [Google Scholar] [CrossRef]
- Das, P.; Haldar, R.; Santhanam, S.; Ravindran, V. Therapeutic exercises and rehabilitation in axial spondyloarthropathy: Balancing benefits with unique challenges in the Asia-Pacific countries. Int. J. Rheum. Dis. 2021, 24, 170–182. [Google Scholar] [CrossRef]
- Reddy, R.S.; Tedla, J.S.; Dixit, S.; Raizah, A.; Al-Otaibi, M.L.; Gular, K.; Ahmad, I.; Sirajudeen, M.S. Cervical joint position sense and its correlations with postural stability in subjects with fibromyalgia syndrome. Life 2022, 12, 1817. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Wang, Z.; Chen, G.; Liu, W. Predictive effect of cervical spinal cord compression and corresponding segmental paravertebral muscle degeneration on the severity of symptoms in patients with cervical spondylotic myelopathy. Spine J. 2021, 21, 1099–1109. [Google Scholar] [CrossRef]
- Pye, S.R.; Reid, D.M.; Lunt, M.; Adams, J.E.; Silman, A.J.; O’Neill, T.W. Lumbar disc degeneration: Association between osteophytes, end-plate sclerosis and disc space narrowing. Ann. Rheum. Dis. 2007, 66, 330–333. [Google Scholar] [CrossRef]
- Middleton, K.; Fish, D.E. Lumbar spondylosis: Clinical presentation and treatment approaches. Curr. Rev. Musculoskelet. Med. 2009, 2, 94–104. [Google Scholar] [CrossRef]
- Moreau, C.E.; Green, B.N.; Johnson, C.D.; Moreau, S.R. Isometric back extension endurance tests: A review of the literature. J. Manip. Physiol. Ther. 2001, 24, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Demoulin, C.; Vanderthommen, M.; Duysens, C.; Crielaard, J.-M. Spinal muscle evaluation using the Sorensen test: A critical appraisal of the literature. Jt. Bone Spine 2006, 73, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Vlažná, D.; Krkoška, P.; Kuhn, M.; Dosbaba, F.; Batalik, L.; Vlčková, E.; Voháňka, S.; Adamová, B. Assessment of lumbar extensor muscles in the context of trunk function, a pilot study in healthy individuals. Appl. Sci. 2021, 11, 9518. [Google Scholar] [CrossRef]
- Shaw, J.; Jacobs, J.V.; Van Dillen, L.R.; Beneck, G.J.; Armour Smith, J. Understanding the Biering-Sorensen test: Contributors to extensor endurance in young adults with and without low back pain. medRxiv 2023. [Google Scholar] [CrossRef]
- Godi, M.; Franchignoni, F.; Caligari, M.; Giordano, A.; Turcato, A.M.; Nardone, A. Comparison of reliability, validity, and responsiveness of the mini-BESTest and Berg Balance Scale in patients with balance disorders. Phys. Ther. 2013, 93, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.; Ricci, N.; Nogueira, E.; Perracini, M.R. The Berg Balance Scale as a clinical screening tool to predict fall risk in older adults: A systematic review. Physiotherapy 2018, 104, 383–394. [Google Scholar] [CrossRef]
- Reddy, R.S.; Alkhamis, B.A.; Kirmani, J.A.; Uddin, S.; Ahamed, W.M.; Ahmad, F.; Ahmad, I.; Raizah, A. Age-Related Decline in Cervical Proprioception and Its Correlation with Functional Mobility and Limits of Stability Assessed Using Computerized Posturography: A Cross-Sectional Study Comparing Older (65+ Years) and Younger Adults. Healthcare 2023, 11, 1924. [Google Scholar] [CrossRef]
- Pickerill, M.L.; Harter, R.A. Validity and reliability of limits-of-stability testing: A comparison of 2 postural stability evaluation devices. J. Athl. Train. 2011, 46, 600–606. [Google Scholar] [CrossRef]
- Raizah, A.; Reddy, R.S.; Alshahrani, M.S.; Tedla, J.S.; Dixit, S.; Gular, K.; Gautam, A.P.; Ahmad, I.; Kandakurti, P.K. Investigating Knee Joint Proprioception and Its Impact on Limits of Stability Using Dynamic Posturography in Individuals with Bilateral Knee Osteoarthritis—A Cross-Sectional Study of Comparisons and Correlations. J. Clin. Med. 2023, 12, 2764. [Google Scholar] [CrossRef]
- Behennah, J.; Conway, R.; Fisher, J.; Osborne, N.; Steele, J. The relationship between balance performance, lumbar extension strength, trunk extension endurance, and pain in participants with chronic low back pain, and those without. Clin. Biomech. 2018, 53, 22–30. [Google Scholar] [CrossRef]
- McGill, S. Low Back Disorders: Evidence-Based Prevention and Rehabilitation; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Hodges, P.W.; Danneels, L. Changes in structure and function of the back muscles in low back pain: Different time points, observations, and mechanisms. J. Orthop. Sport. Phys. Ther. 2019, 49, 464–476. [Google Scholar] [CrossRef] [PubMed]
- Pranata, A.; Perraton, L.; El-Ansary, D.; Clark, R.; Fortin, K.; Dettmann, T.; Brandham, R.; Bryant, A. Lumbar extensor muscle force control is associated with disability in people with chronic low back pain. Clin. Biomech. 2017, 46, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Holmes, B.; Leggett, S.; Mooney, V.; Nichols, J.; Negri, S.; Hoeyberghs, A. Comparison of female geriatric lumbar-extension strength: Asymptotic versus chronic low back pain patients and their response to active rehabilitation. Clin. Spine Surg. 1996, 9, 17–22. [Google Scholar] [CrossRef]
- Bayramoglu, M.; Akman, M.N.; Klnç, S.; Çetin, N.; Yavuz, N.; Özker, R. Isokinetic measurement of trunk muscle strength in women with chronic low-back pain. Am. J. Phys. Med. Rehabil. 2001, 80, 650–655. [Google Scholar] [CrossRef]
- Suh, J.H.; Kim, H.; Jung, G.P.; Ko, J.Y.; Ryu, J.S. The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine 2019, 98, e16173. [Google Scholar] [CrossRef]
- Ringheim, I.; Indahl, A.; Roeleveld, K. Reduced muscle activity variability in lumbar extensor muscles during sustained sitting in individuals with chronic low back pain. PLoS ONE 2019, 14, e0213778. [Google Scholar] [CrossRef]
- Rhajib, M.A.N.; Islam, M.W.; Hossain, M.A.; Haque, M.O.; Fazal, A.I.A. Evidence based Physiotherapy Intervention of Lumbar Spondylolisthesis: A Narrative Review. J. Spine Res. Surg. 2022, 4, 72–79. [Google Scholar]
- Matheve, T.; Hodges, P.; Danneels, L. The Role of Back Muscle Dysfunctions in Chronic Low Back Pain: State-of-the-Art and Clinical Implications. J. Clin. Med. 2023, 12, 5510. [Google Scholar] [CrossRef]
- Noonan, A.M.; Brown, S.H. Paraspinal muscle pathophysiology associated with low back pain and spine degenerative disorders. JOR Spine 2021, 4, e1171. [Google Scholar] [CrossRef]
- Kim, D.-J.; Choi, I.-R.; Lee, J.-H. Effect of balance taping on trunk stabilizer muscles for back extensor muscle endurance: A randomized controlled study. J. Musculoskelet. Neuronal Interact. 2020, 20, 541. [Google Scholar]
- Jahandideh, L.; Letafatkar, A.; Khanzadeh, R.; Kashani, F.O. Comparing the Effect of Exercises with Different Gluteal-to-Tensor Fasciae Latae Activation Index in Patients With Chronic Low Back Pain. J. Sport Rehabil. 2023, 32, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Karagül, S.; Kartaloğlu, I.F. The effect of single and dual-task balance exercises on balance performance in older adult patients with degenerative lumbar spondylosis: A randomized controlled trial. Geriatr. Nurs. 2023, 49, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, S.; Uyar Köylü, S. Comparison of spinopelvic parameters among older adults with lumbar spondylosis, lumbar fractures and lumbar spinal stabilization. Turk. J. Geriatr./Türk Geriatr. Derg. 2022, 25, 351–357. [Google Scholar] [CrossRef]
- Murena, L.; Canton, G.; Giraldi, G.; Bassini, S. Spine pain: Clinical features. In Pain Imaging: A Clinical-Radiological Approach to Pain Diagnosis; Springer: Berlin/Heidelberg, Germany, 2019; pp. 119–133. [Google Scholar]
- Mazurek, M.; Kulesza, B.; Gołębiowska, N.; Tyzo, B.; Kura, K.; Szczepanek, D. Factors Predisposing to The Formation of Degenerative Spondylolisthesis—A Narrative Review. Medicina 2023, 59, 1430. [Google Scholar] [CrossRef]
- Jafarabadi, M.A. Effects of Mcgill Stabilization Exercise on Pain and Disability, Range of Motion and Dynamic Balance Indices in Patients with Chronic Nonspecific Low Back Pain. Pain 2017, 16, 19–21. [Google Scholar]
- Gheitasi, M.; Bayattork, M.; Miri, H.; Afshar, H. Comparing the effect of suspended and non-suspended core stability exercises on static and dynamic balance and muscular endurance in young males with Down syndrome. Phys. Treat.-Specif. Phys. Ther. J. 2019, 9, 153–160. [Google Scholar] [CrossRef]
- Overstreet, D.S.; Michl, A.N.; Penn, T.M.; Rumble, D.D.; Aroke, E.N.; Sims, A.M.; King, A.L.; Hasan, F.N.; Quinn, T.L.; Long, D.L. Temporal summation of mechanical pain prospectively predicts movement-evoked pain severity in adults with chronic low back pain. BMC Musculoskelet. Disord. 2021, 22, 429. [Google Scholar] [CrossRef]
- Yang, H.-C.; Xiao, W.-W.; Guan, Y.-X.; Mao, H.-A.; Hao, Z.-M.; Wang, C.-H. Effect of Cognitive Load on Anticipatory Postural Adjustment Latency and its Relationship with Pain-Related Dysfunction in Non-specific Chronic Low Back Pain: A Cross-Sectional Study. Pain Ther. 2023, 12, 723–735. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, Y.; Li, T.; Ma, J.; He, R.; Han, X.; Wu, W.; Wang, C. Relationship between Abnormal Spontaneous Brain Activity and Altered Neuromuscular Activation of Lumbar Paraspinal Muscles in Chronic Low Back Pain. Res. Sq. 2023. preprint. [Google Scholar]
- Porwal, S.; Rizvi, M.R.; Sharma, A.; Ahmad, F.; Alshahrani, M.S.; Raizah, A.; Shaik, A.R.; Seyam, M.K.; Miraj, M.; Alkhamis, B.A. Enhancing Functional Ability in Chronic Nonspecific Lower Back Pain: The Impact of EMG-Guided Trunk Stabilization Exercises. Healthcare 2023, 11, 2153. [Google Scholar] [CrossRef]
- Del Din, S.; Galna, B.; Lord, S.; Nieuwboer, A.; Bekkers, E.M.; Pelosin, E.; Avanzino, L.; Bloem, B.R.; Olde Rikkert, M.G.; Nieuwhof, F. Falls risk in relation to activity exposure in high-risk older adults. J. Gerontol. Ser. A 2020, 75, 1198–1205. [Google Scholar] [CrossRef] [PubMed]
- Bezold, J.; Krell-Roesch, J.; Eckert, T.; Jekauc, D.; Woll, A. Sensor-based fall risk assessment in older adults with or without cognitive impairment: A systematic review. Eur. Rev. Aging Phys. Act. 2021, 18, 15. [Google Scholar] [CrossRef]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Hodges, P.W. Are the changes in postural control associated with low back pain caused by pain interference? Clin. J. Pain 2005, 21, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Brumagne, S.; Janssens, L.; Janssens, E.; Goddyn, L. Altered postural control in anticipation of postural instability in persons with recurrent low back pain. Gait Posture 2008, 28, 657–662. [Google Scholar] [CrossRef]
- Thakkar, H.H.; Kumar, S. Static and dynamic postural stability in subjects with and without chronic low back pain. Int. J. Res. Med. Sci. 2015, 3, 2405–2409. [Google Scholar] [CrossRef]
- Brumagne, S.; Janssens, L.; Knapen, S.; Claeys, K.; Suuden-Johanson, E. Persons with recurrent low back pain exhibit a rigid postural control strategy. Eur. Spine J. 2008, 17, 1177–1184. [Google Scholar] [CrossRef]
- Soliman, E.S.; Shousha, T.M.; Alayat, M.S. The effect of pain severity on postural stability and dynamic limits of stability in chronic low back pain. J. Back Musculoskelet. Rehabil. 2017, 30, 1023–1029. [Google Scholar] [CrossRef]
- Hlaing, S.S.; Puntumetakul, R.; Khine, E.E.; Boucaut, R. Effects of core stabilization exercise and strengthening exercise on proprioception, balance, muscle thickness and pain related outcomes in patients with subacute nonspecific low back pain: A randomized controlled trial. BMC Musculoskelet. Disord. 2021, 22, 998. [Google Scholar] [CrossRef]
- Alshahrani, M.S.; Reddy, R.S. Mediation Effect of Kinesiophobia on the Relationship between Cervical Joint Position Sense and Limits of Stability in Individuals with Fibromyalgia Syndrome: A Cross-Sectional Study Using Mediation Analysis. J. Clin. Med. 2023, 12, 2791. [Google Scholar] [CrossRef]
- Özkal, Ö.; Kara, M.; Topuz, S.; Kaymak, B.; Bakı, A.; Özçakar, L. Assessment of core and lower limb muscles for static/dynamic balance in the older people: An ultrasonographic study. Age Ageing 2019, 48, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Pope, M.H.; Goh, K.L.; Magnusson, M.L. Spine ergonomics. Annu. Rev. Biomed. Eng. 2002, 4, 49–68. [Google Scholar] [CrossRef] [PubMed]
- Unger, M.; Jelsma, J.; Stark, C. Effect of a trunk-targeted intervention using vibration on posture and gait in children with spastic type cerebral palsy: A randomized control trial. Dev. Neurorehabilit. 2013, 16, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Standaert, C.J.; Weinstein, S.M.; Rumpeltes, J. Evidence-informed management of chronic low back pain with lumbar stabilization exercises. Spine J. 2008, 8, 114–120. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics | Lumbar Spondylosis Group (n = 60) | Healthy Control Group (n = 60) | p-Value |
|---|---|---|---|
| Age (years) (mean ± SD) | 59.73 ± 10.08 | 58.98 ± 8.67 | 0.826 |
| Sex, (male: female) | 32:28 | 33:27 | 0.975 |
| BMI (kg/m2) (mean ± SD) | 24.64 ± 3.24 | 23.83 ± 2.32 | 0.416 |
| Duration of symptoms (months) | 12.33 ± 4.56 | - | - |
| Pain intensity (VAS scale) 0–100 mm | 57.66 ± 22.11 | - | - |
| Functional disability (ODI score) 0–50 | 22.63 ± 8.09 | - | - |
| Characteristics | Lumbar Spondylosis Group (n = 60) (mean ± SD) | Healthy Control Group (n = 60) (mean ± SD) | p-Value |
|---|---|---|---|
| Lumbar extensor endurance (seconds) | 23.06 ± 8.38 | 52.45 ± 11.48 | <0.001 |
| Functional balance (BBS scores, 0 to 56) | 48.36 ± 3.26 | 53.34 ± 2.48 | <0.001 |
| Limits of stability variables—Eyes open | <0.001 | ||
| 337.07 ± 128.12 | 176.94 ± 63.87 | |
| 6.43 ± 2.16 | 4.23 ± 1.01 | ||
| 3.38 ± 0.89 | 2.12 ± 0.32 | ||
| Limits of stability variables—Eyes closed | <0.001 | ||
| 512.38 ± 110.26 | 256.12 ± 98.87 | |
| 8.32 ± 2.92 | 5.12 ± 2.08 | ||
| 5.23 ± 1.96 | 3.99 ± 1.98 |
| Characteristics | Lumbar Extensor Endurance (seconds) (r) |
|---|---|
| Functional balance (BBS scores, 0 to 56) | 0.46 ** |
| Limits of stability variables—Eyes open | |
| −0.38 ** |
| −0.41 ** | |
| −0.43 ** | |
| Limits of stability variables—Eyes closed | |
| −0.49 ** |
| −0.47 ** | |
| −0.45 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfaya, F.F.; Reddy, R.S.; Alshahrani, M.S.; Gautam, A.P.; Mukherjee, D.; Al Salim, Z.A.; Alqhtani, R.S.; Ghulam, H.S.H.; Alyami, A.M.; Al Adal, S.; et al. Exploring the Interplay of Muscular Endurance, Functional Balance, and Limits of Stability: A Comparative Study in Individuals with Lumbar Spondylosis Using a Computerized Stabilometric Force Platform. Life 2023, 13, 2104. https://doi.org/10.3390/life13102104
Alfaya FF, Reddy RS, Alshahrani MS, Gautam AP, Mukherjee D, Al Salim ZA, Alqhtani RS, Ghulam HSH, Alyami AM, Al Adal S, et al. Exploring the Interplay of Muscular Endurance, Functional Balance, and Limits of Stability: A Comparative Study in Individuals with Lumbar Spondylosis Using a Computerized Stabilometric Force Platform. Life. 2023; 13(10):2104. https://doi.org/10.3390/life13102104
Chicago/Turabian StyleAlfaya, Fareed F., Ravi Shankar Reddy, Mastour Saeed Alshahrani, Ajay Prashad Gautam, Debjani Mukherjee, Zuhair A. Al Salim, Raee S. Alqhtani, Hussain Saleh H. Ghulam, Abdullah Mohammed Alyami, Saeed Al Adal, and et al. 2023. "Exploring the Interplay of Muscular Endurance, Functional Balance, and Limits of Stability: A Comparative Study in Individuals with Lumbar Spondylosis Using a Computerized Stabilometric Force Platform" Life 13, no. 10: 2104. https://doi.org/10.3390/life13102104
APA StyleAlfaya, F. F., Reddy, R. S., Alshahrani, M. S., Gautam, A. P., Mukherjee, D., Al Salim, Z. A., Alqhtani, R. S., Ghulam, H. S. H., Alyami, A. M., Al Adal, S., & Jabour, A. A. (2023). Exploring the Interplay of Muscular Endurance, Functional Balance, and Limits of Stability: A Comparative Study in Individuals with Lumbar Spondylosis Using a Computerized Stabilometric Force Platform. Life, 13(10), 2104. https://doi.org/10.3390/life13102104