
Imaging Inflammation in Atherosclerosis with CXCR4-Directed [68Ga]PentixaFor PET/MRI—Compared with [18F]FDG PET/MRI
 ,
,  ,
,  ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Imaging Procedures
2.3. Imaging Analysis
2.4. Statistical Analysis
3. Results
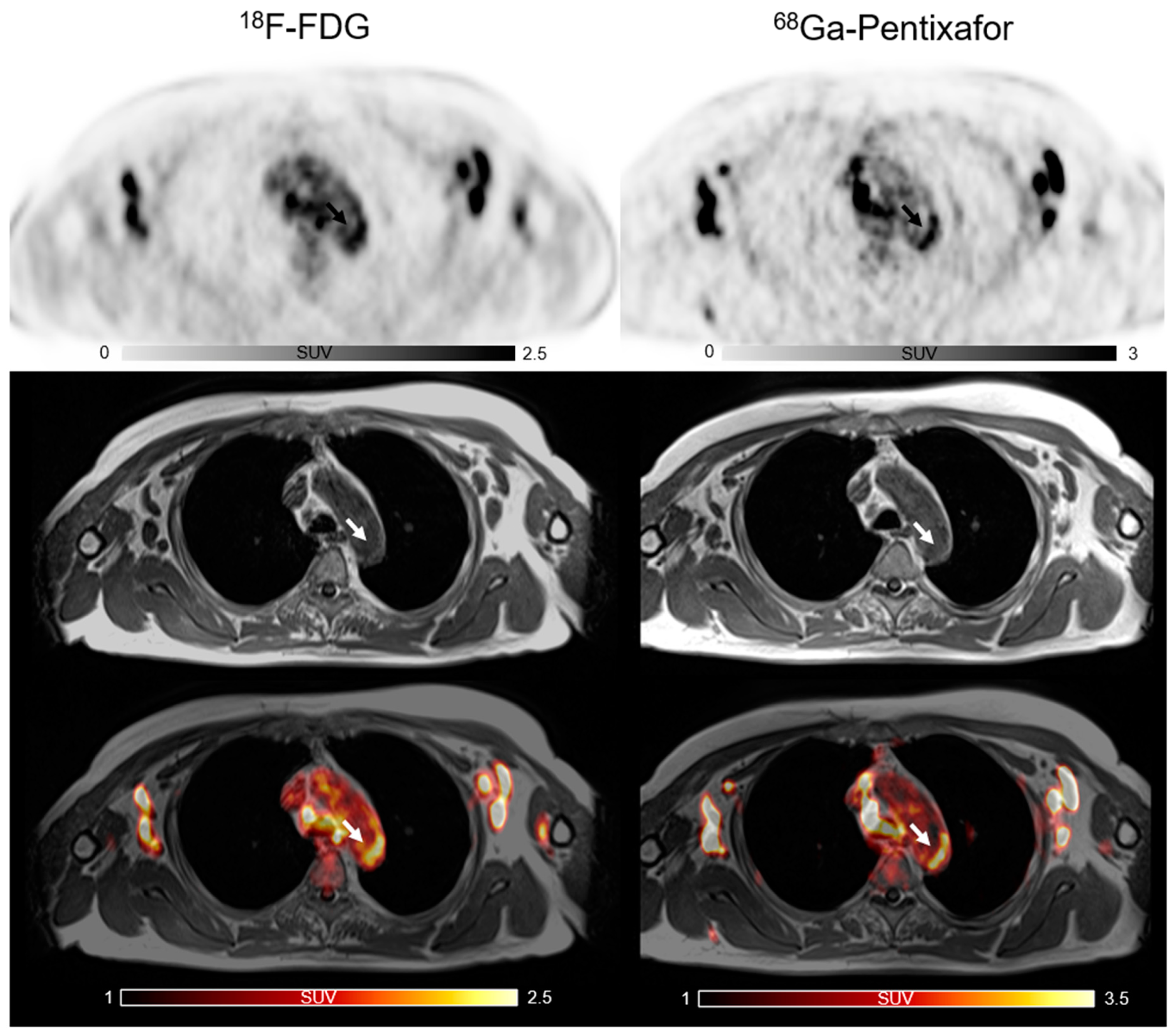
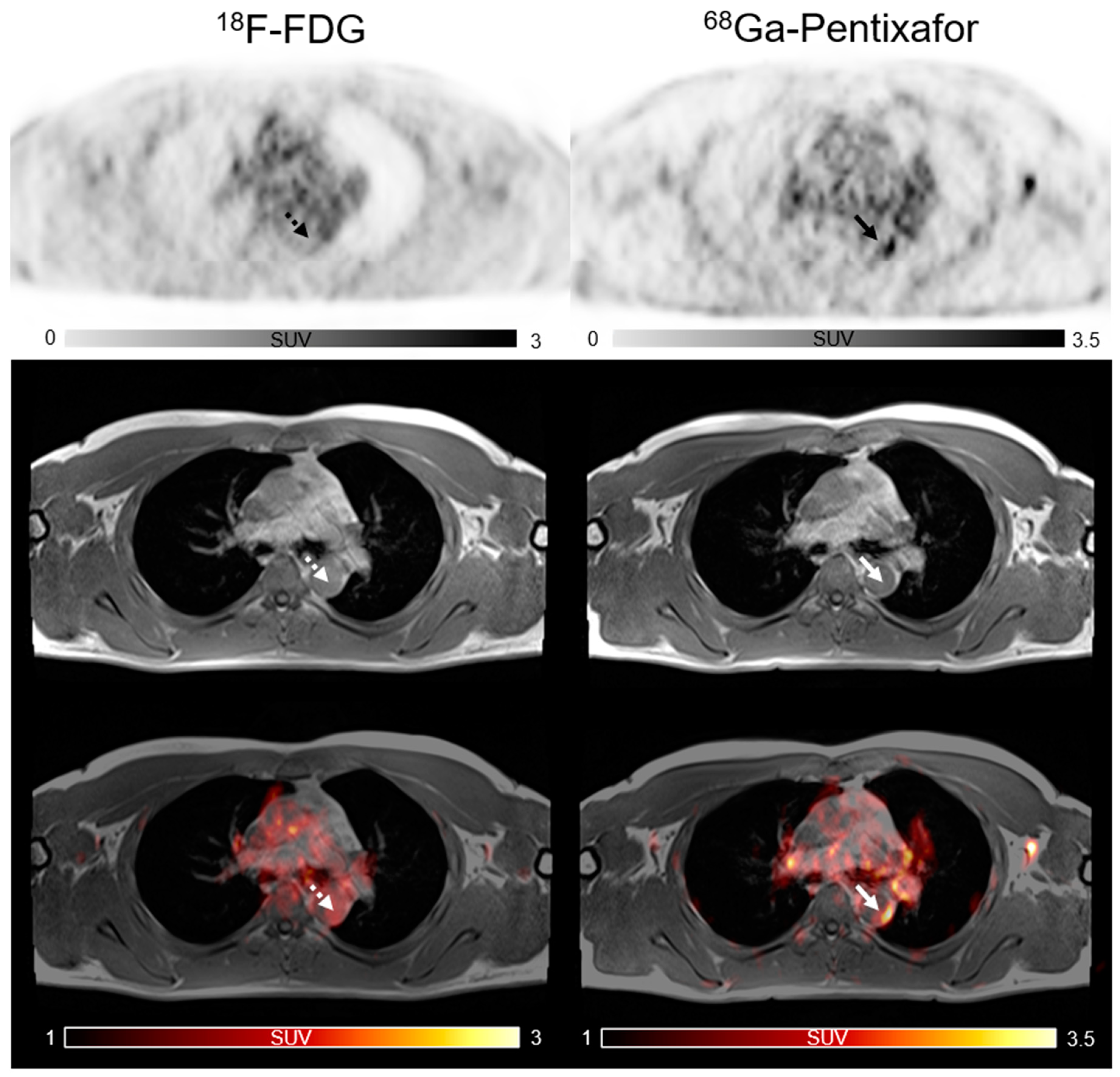
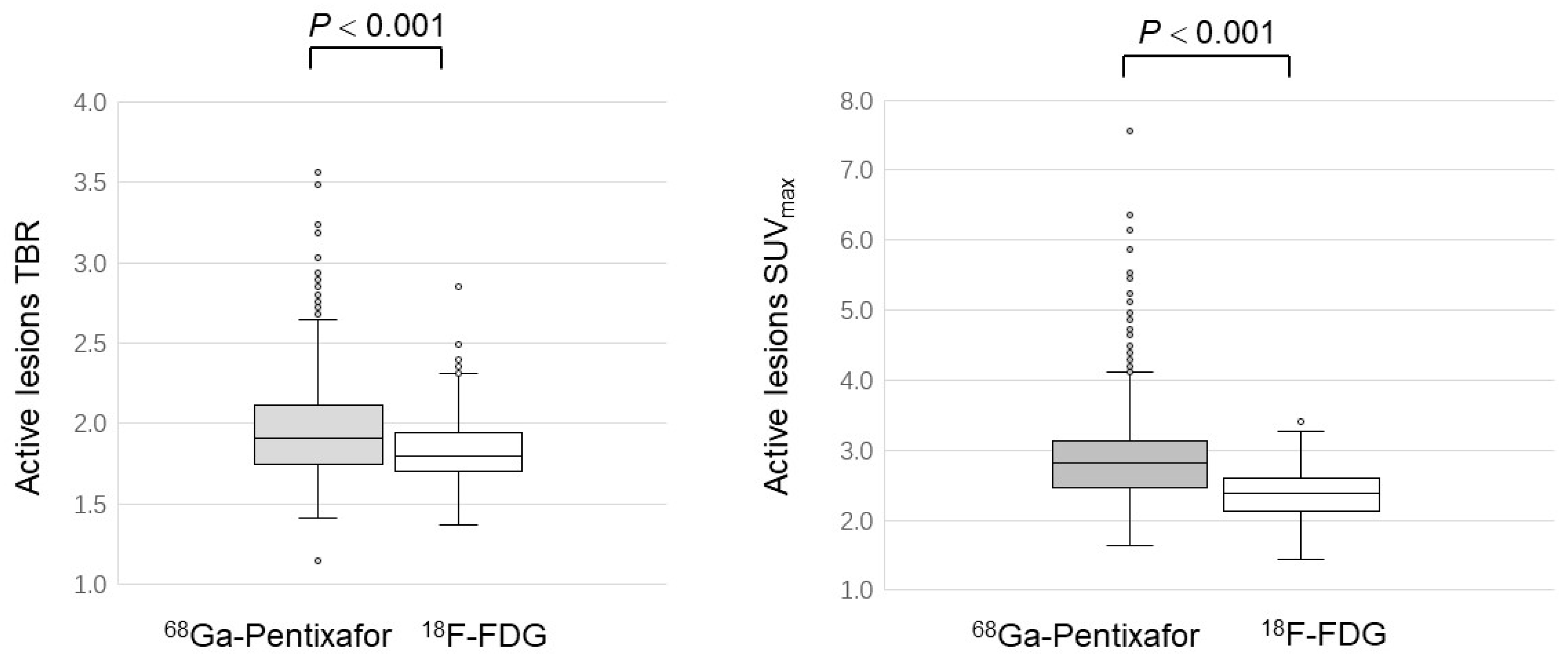
3.1. Comparison of [68Ga]PentixaFor and [18F]FDG Uptake: Lesion-Based Analysis
3.2. Comparison of [68Ga]PentixaFor and [18F]FDG Uptake: Patient-Based Analysis
3.3. Pearson Correlation between Tracer Uptake of Plaques and Myocardial CXCR4 Expression
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Herrington, W.; Lacey, B.; Sherliker, P.; Armitage, J.; Lewington., S. Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease. Circ. Res. 2016, 118, 535–546. [Google Scholar] [CrossRef]
- Vaina, S.; Stefanadis, C. Detection of the vulnerable coronary atheromatous plaque. Where are we now? Int. J. Cardiovasc. Interv. 2005, 7, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Romero, J.R.; Beiser, A.; Seshadri, S.; Benjamin, E.J.; Polak, J.F.; Vasan, R.S.; Au, R.; DeCarli, C.; Wolf, P.A. Carotid artery atherosclerosis, MRI indices of brain ischemia, aging, and cognitive impairment: The Framingham study. Stroke 2009, 40, 1590–1596. [Google Scholar] [CrossRef] [Green Version]
- Adams, M.R.; Celermajer, D.S. Detection of presymptomatic atherosclerosis: A current perspective. Clin. Sci. 1999, 97, 615–624. [Google Scholar] [CrossRef]
- Moore, K.J.; Sheedy, F.J.; Fisher, E.A. Macrophages in atherosclerosis: A dynamic balance. Nat. Rev. Immunol. 2013, 13, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Silvestre-Roig, C.; de Winther, M.P.; Weber, C.; Daemen, M.J.; Lutgens, E.; Soehnlein, O. Atherosclerotic plaque destabilization: Mechanisms, models, and therapeutic strategies. Circ. Res. 2014, 114, 214–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavurma, M.M.; Rayner, K.J.; Karunakaran, D. The walking dead: Macrophage inflammation and death in atherosclerosis. Curr. Opin. Lipidol. 2017, 28, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Roa, P.M.; Rees, J.I.; Bartley, L.; Marshall, C. Systemic atherosclerotic plaque vulnerability in patients with coronary artery disease with a single whole body FDG PET-CT scan. Asia Ocean. J. Nucl. Med. Biol. 2020, 8, 18–26. [Google Scholar]
- Noh, T.S.; Moon, S.H.; Cho, Y.S.; Hong, S.P.; Lee, E.J.; Choi, J.Y.; Kim, B.T.; Lee, K.H. Relation of carotid artery [18F]FDG uptake to C-reactive protein and Framingham risk score in a large cohort of asymptomatic adults. J. Nucl. Med. 2013, 54, 2070–2076. [Google Scholar] [CrossRef] [Green Version]
- Shinde, S.S.; Maschauer, S.; Prante, O. Sweetening pharmaceutical radiochemistry by 18F-fluoroglycosylation: Recent progress and future prospects. Pharmaceuticals 2021, 14, 1175–1197. [Google Scholar] [CrossRef]
- Kung, B.T.; Seraj, S.M.; Zadeh, M.Z.; Rojulpote, C.; Kothekar, E.; Ayubcha, C.; Ng, K.S.; Ng, K.K.; Au-Yong, T.K.; Werner, T.J.; et al. An update on the role of [18F]FDG-PET/CT in major infectious and inflammatory diseases. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 255–273. [Google Scholar] [PubMed]
- Weber, C.; Noels, H. Atherosclerosis: Current pathogenesis and therapeutic options. Nat. Med. 2011, 17, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Hyafil, F.; Pelisek, J.; Laitinen, I.; Schottelius, M.; Mohring, M.; Döring, Y.; van der Vorst, E.P.; Kallmayer, M.; Steiger, K.; Poschenrieder, A.; et al. Imaging the cytokine receptor CXCR4 in atherosclerotic plaques with the radiotracer [68Ga]PentixaFor for positron emission tomography. J. Nucl. Med. 2017, 58, 499–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kircher, M.; Tran-Gia, J.; Kemmer, L.; Zhang, X.L.; Schirbel, A.; Werner, R.A.; Buck, A.K.; Wester, H.J.; Hacker, M.; Lapa, C.; et al. Imaging Inflammation in Atherosclerosis with CXCR4-directed [68Ga]PentixaFor PET/CT-Correlation with [18F]FDG PET/CT. J. Nucl. Med. 2020, 61, 751–756. [Google Scholar] [CrossRef]
- Ishiguchi, H.; Ito, S.; Kato, K.; Sakurai, Y.; Kawai, H.; Fujita, N.; Abe, S.; Narita, A.; Nishio, N.; Muramatsu, H.; et al. Diagnostic performance of (18)F-FDG PET/CT and whole-body diffusion-weighted imaging with background body suppression (DWIBS) in detection of lymph node and bone metastases from pediatric neuroblastoma. Ann. Nucl. Med. 2018, 32, 348–362. [Google Scholar] [CrossRef]
- Maggialetti, N.; Ferrari, C.; Minoia, C.; Asabella, A.N.; Ficco, M.; Loseto, G.; De Tullio, G.; de Fazio, V.; Calabrese, A.; Guarini, A.; et al. Role of WB-MR/DWIBS compared to [18F]FDG PET/CT in the therapy response assessment of lymphoma. Radiol. Med. 2016, 121, 132–143. [Google Scholar] [CrossRef]
- Tudisca, C.; Nasoodi, A.; Fraioli, F. PET-MRI: Clinical application of the new hybrid technology. Nucl. Med. Commun. 2015, 36, 666–678. [Google Scholar] [CrossRef]
- Zernecke, A.; Weber, C. Chemokines in atherosclerosis: Proceedings resumed. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 742–750. [Google Scholar] [CrossRef]
- Altaf, N.; Daniels, L.; Morgan, P.S.; Auer, D.; MacSweeney, S.T.; Moody, A.R.; Gladman, J.R. Detection of intraplaque hemorrhage by magnetic resonance imaging in symptomatic patients with mild to moderate carotid stenosis predicts recurrent neurological events. J. Vasc. Surg. 2008, 47, 337–342. [Google Scholar] [CrossRef] [Green Version]
- Lüscher, T.F. Inflammation and features of the vulnerable plaque: From mechanisms and imaging to outcomes. Eur. Heart J. 2020, 41, 2923–2927. [Google Scholar] [CrossRef]
- Schäfer, J.F.; Gatidis, S.; Schmidt, H.; Gückel, B.; Bezrukov, I.; Pfannenberg, C.A.; Reimold, M.; Ebinger, M.; Fuchs, J.; Claussen, C.D.; et al. Simultaneous whole-body PET/MR imaging in comparison to PET/CT in pediatric oncology: Initial results. Radiology 2014, 273, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Ponisio, M.R.; McConathy, J.; Laforest, R.; Khanna, G. Evaluation of diagnostic performance of whole-body simultaneous PET/MRI in pediatric lymphoma. Pediatr. Radiol. 2016, 46, 1258–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klenk, C.; Gawande, R.; Uslu, L.; Khurana, A.; Qiu, D.Q.; Quon, A.; Doing, J.; Rosenberg, J.; Fineman, S.L.; Moseley, M.; et al. Ionising radiation-free wholebody MRI versus F-18 fluorodeoxyglucose PET/CT scans for children and young adults with cancer: A prospective, non-randomised, single-centre study. Lancet Oncol. 2014, 15, 275–285. [Google Scholar] [CrossRef]
- Osam, B.; Huang, L.H.; Elvington, A.; Szpakowska, M.; Sultan, D.; Heo, G.S.; Zhang, X.; Luehmann, H.; Detering, L.; Chevigne, A.; et al. CXCR4-Binding Positron Emission Tomography Tracers Link Monocyte Recruitment and Endothelial Injury in Murine Atherosclerosis. Arter. Thromb. Vasc. Biol. 2021, 41, 822–836. [Google Scholar]
- Li, X.; Heber, D.; Rausch, I.; Beitzke, D.; Mayerhoefer, M.E.; Rasul, S.; Kreissl, M.; Mitthauser, M.; Wadsak, W.; Hartenbach, M.; et al. Quantitative assessment of atherosclerotic plaques on (18)F-FDG PET/MRI: Comparison with a PET/CT hybrid system. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1503–1512. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Yu, W.; Wollenweber, T.; Lu, X.; Wei, Y.; Beitzke, D.; Wadsak, W.; Kropf, S.; Wester, H.J.; Haug, A.R.; et al. [(68)Ga]Pentixafor PET/MR imaging of chemokine receptor 4 expression in the human carotid artery. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1616–1625. [Google Scholar] [CrossRef] [Green Version]
- Fabiano, S.; Mancino, S.; Stefanini, M.; Chiocchi, M.; Mauriello, A.; Spagnoli, L.G.; Simonetti, G. High resolution multi contrast-weighted MR imaging from human carotid endarterectomy specimens to assess carotid plaque components. Eur. Radiol. 2008, 18, 2912–2921. [Google Scholar] [CrossRef]
- Bot, I.; Daissormont, I.T.; Zernecke, A.; van Puijvelde, G.H.; Kramp, B.; de Jager, S.C.; Sluimer, J.C.; Manca, M.; Hérias, V.; Westra, M.M.; et al. CXCR4 blockade induces atherosclerosis by affecting neutrophil function. J. Mol. Cell. Cardiol. 2014, 74, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Döring, Y.; Pawig, L.; Weber, C.; Noels, H. The CXCL12/CXCR4 chemokine ligand/receptor axis in cardiovascular disease. Front. Physiol. 2014, 5, 212. [Google Scholar]
- Segret, A.; Rücker-Martin, C.; Pavoine, C.; Flavigny, J.; Deroubaix, E.; Châtel, M.A.; Lombet, A.; Renaud, J.F. Structural localization and expression of CXCL12 and CXCR4 in rat heart and isolated cardiac myocytes. J. Histochem. Cytochem. 2007, 55, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Nasser, M.I.; Zhu, S.J.; Huang, H.L.; Zhao, M.; Wang, B.; Ping, H.; Geng, Q.; Zhu, P. Macrophages: First guards in the prevention of cardiovascular diseases. Life Sci. 2020, 250, 117559. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Crespo, A. Comparison of Gallium-68 and Fluorine-18 imaging characteristics in positron emission tomography. Appl. Radiat. Isot. 2013, 76, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Bucerius, J.; Hyafil, F.; Verberne, H.J.; Slart, R.H.; Lindner, O.; Sciagra, R.; Agostini, D.; Übleis, C.; Gimelli, A.; Hacker, M.; et al. Cardiovascular Committee of the European Association of Nuclear Medicine (EANM). Position paper of the Cardiovascular Committee of the European Association of Nuclear Medicine (EANM) on PET imaging of atherosclerosis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 780–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics (n = 19) | |
| Age (y) | 68 ± 10 |
| Gender | 11 male/8 female |
| BMI (kg/m2) | 27.1 |
| Cardiovascular Risk Factors (n, %) | |
| Hypertension | 4 (21%) |
| Dyslipidemia | 4 (21%) |
| Diabetes | 2 (11%) |
| Smoking | 5 (26%) |
| CRP (≥3 mg/L) | 2 (11%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, X.; Calabretta, R.; Wadsak, W.; Haug, A.R.; Mayerhöfer, M.; Raderer, M.; Zhang, X.; Li, J.; Hacker, M.; Li, X. Imaging Inflammation in Atherosclerosis with CXCR4-Directed [68Ga]PentixaFor PET/MRI—Compared with [18F]FDG PET/MRI. Life 2022, 12, 1039. https://doi.org/10.3390/life12071039
Lu X, Calabretta R, Wadsak W, Haug AR, Mayerhöfer M, Raderer M, Zhang X, Li J, Hacker M, Li X. Imaging Inflammation in Atherosclerosis with CXCR4-Directed [68Ga]PentixaFor PET/MRI—Compared with [18F]FDG PET/MRI. Life. 2022; 12(7):1039. https://doi.org/10.3390/life12071039
Chicago/Turabian StyleLu, Xia, Raffaella Calabretta, Wolfgang Wadsak, Alexander R. Haug, Marius Mayerhöfer, Markus Raderer, Xiaoli Zhang, Jingle Li, Marcus Hacker, and Xiang Li. 2022. "Imaging Inflammation in Atherosclerosis with CXCR4-Directed [68Ga]PentixaFor PET/MRI—Compared with [18F]FDG PET/MRI" Life 12, no. 7: 1039. https://doi.org/10.3390/life12071039
APA StyleLu, X., Calabretta, R., Wadsak, W., Haug, A. R., Mayerhöfer, M., Raderer, M., Zhang, X., Li, J., Hacker, M., & Li, X. (2022). Imaging Inflammation in Atherosclerosis with CXCR4-Directed [68Ga]PentixaFor PET/MRI—Compared with [18F]FDG PET/MRI. Life, 12(7), 1039. https://doi.org/10.3390/life12071039