
Prognostic Impact and Predictors of New-Onset Atrial Fibrillation in Heart Failure

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Cox Regression Analysis for NOAF and Score Development
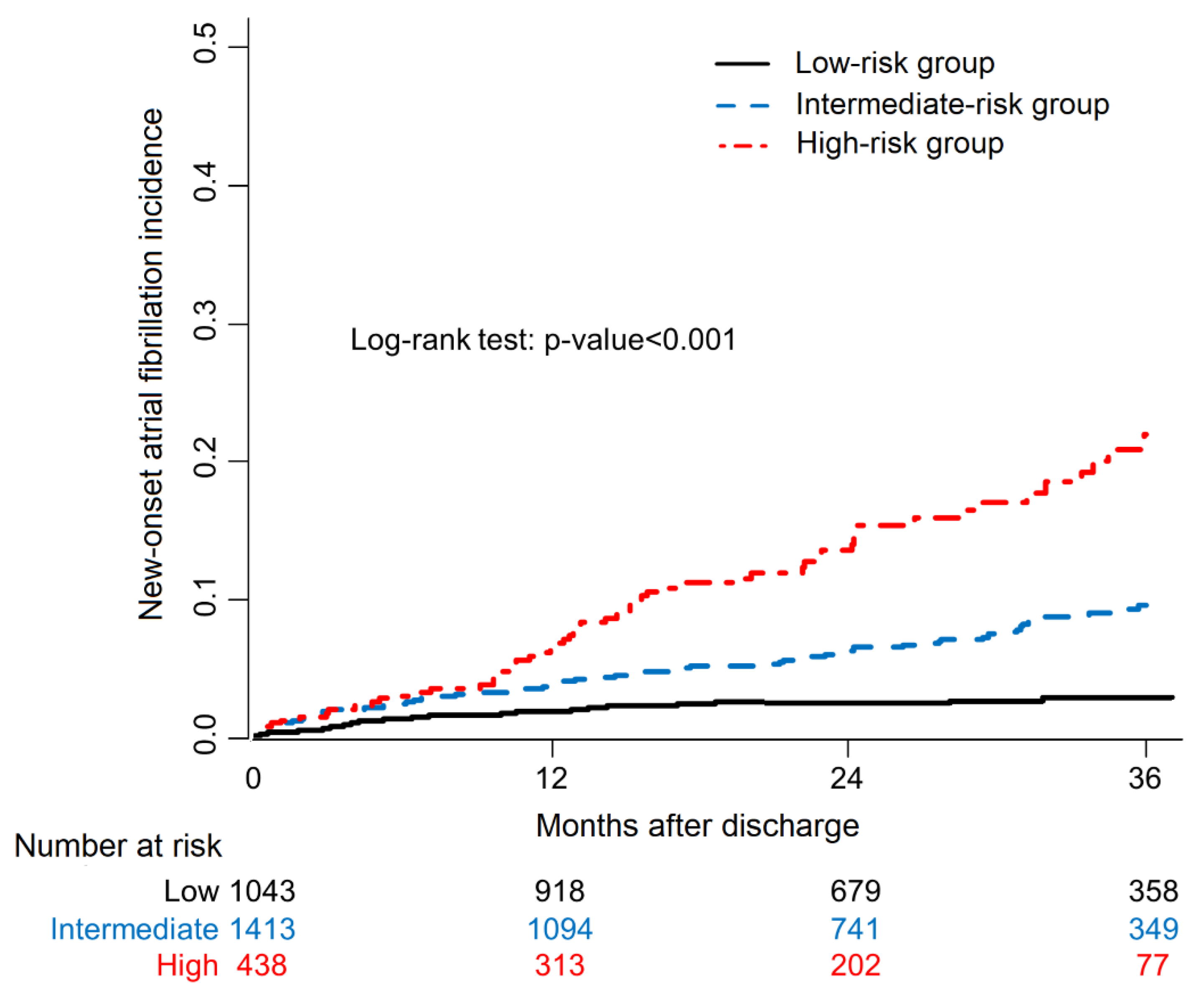
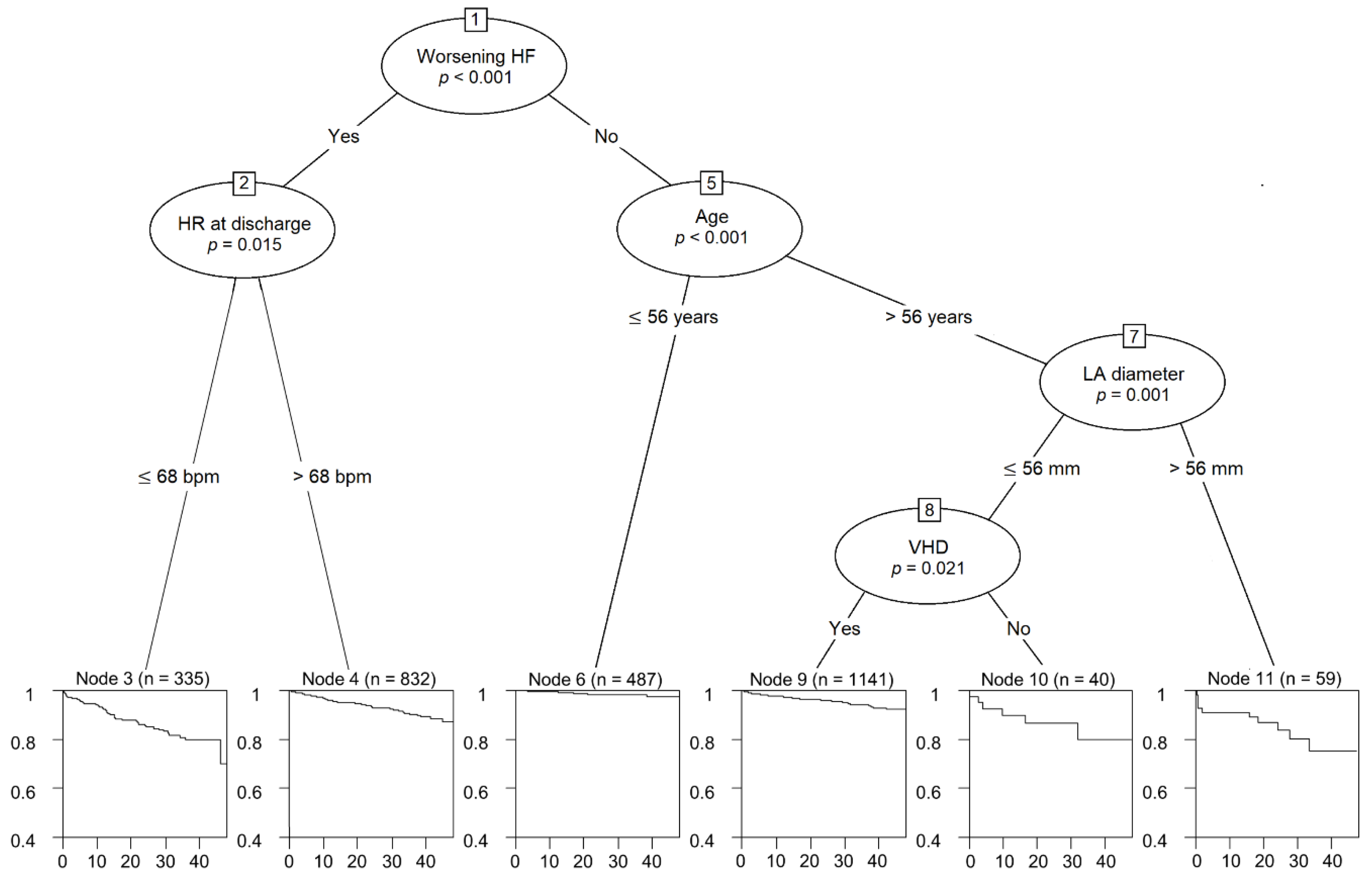
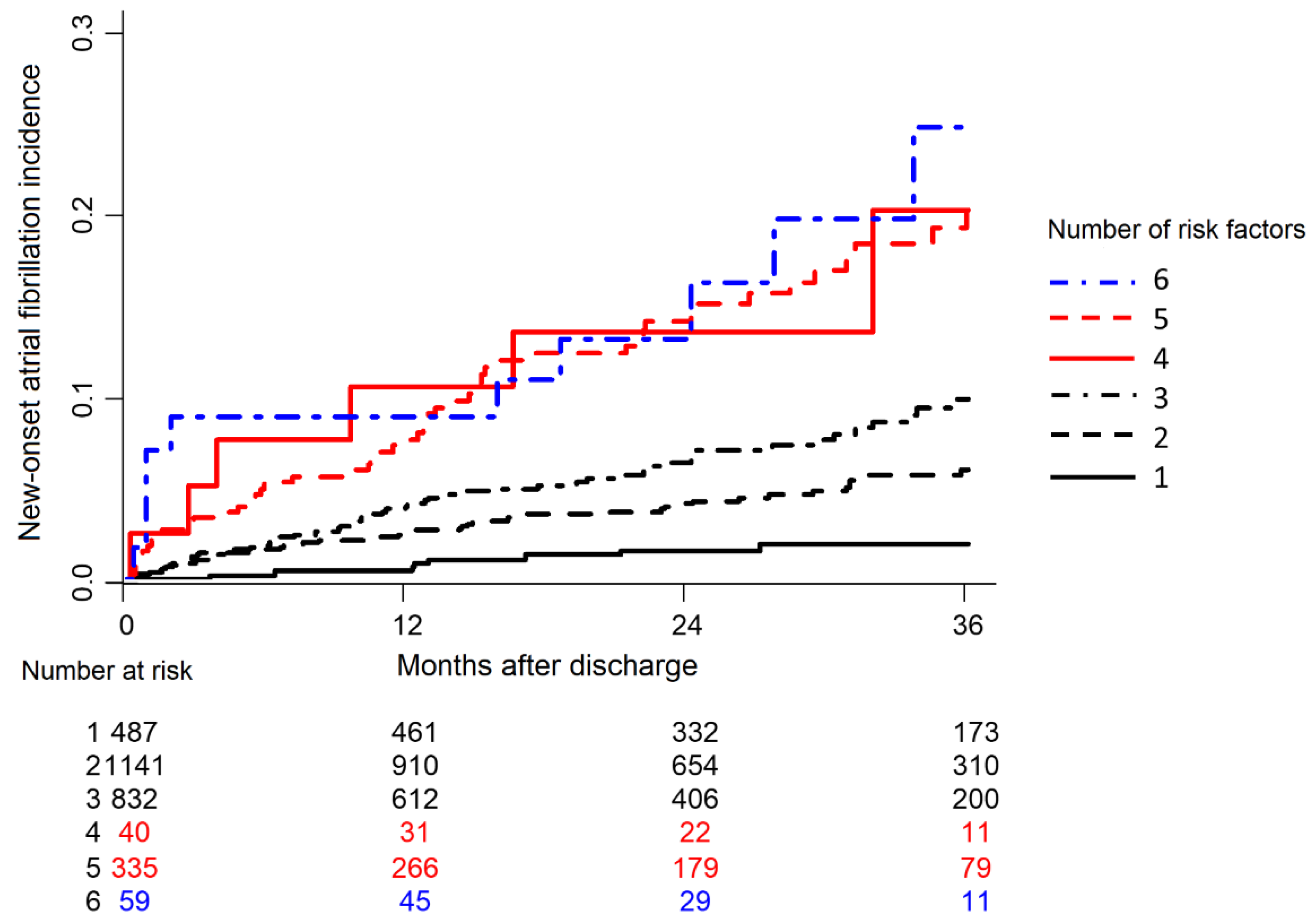
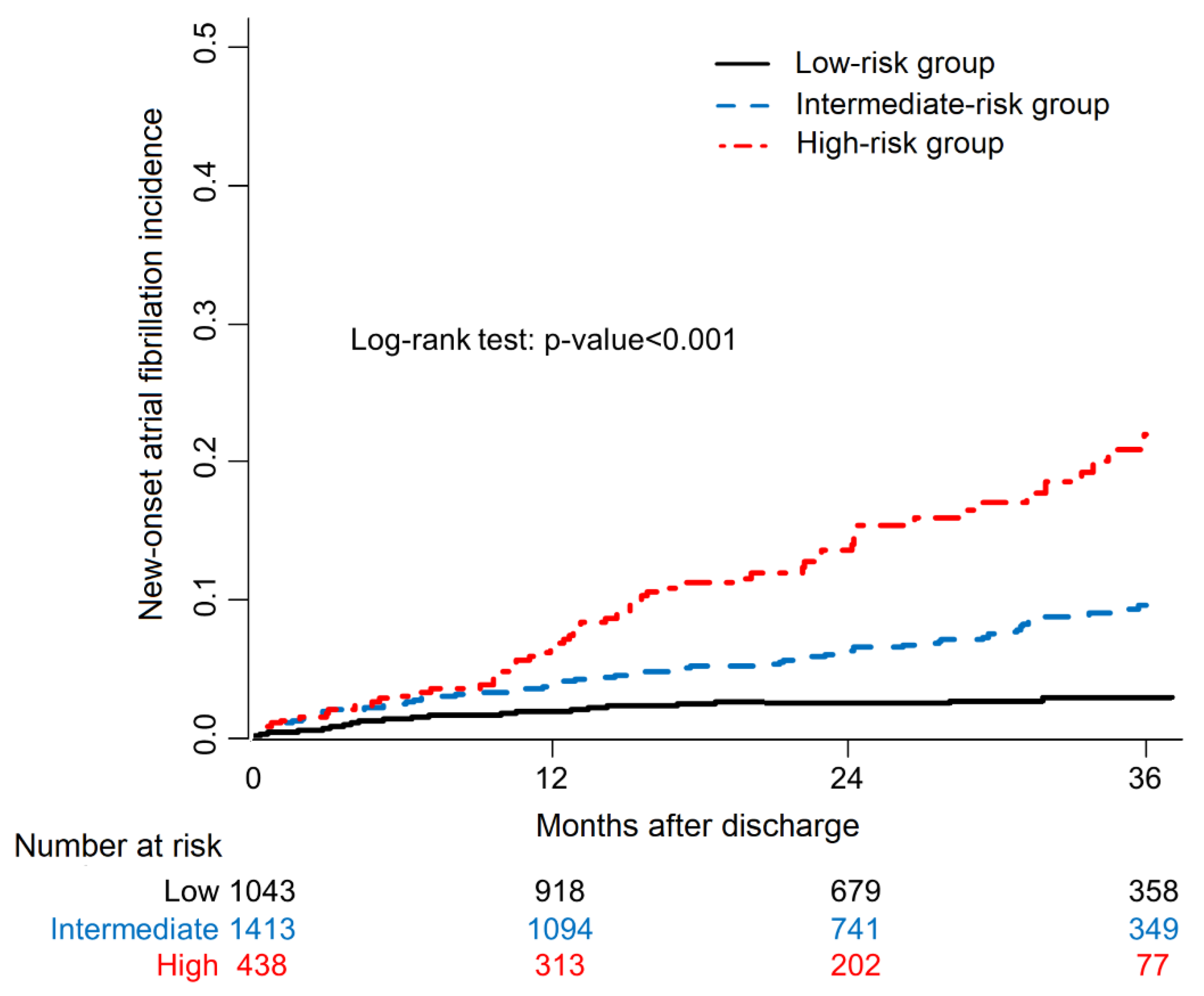
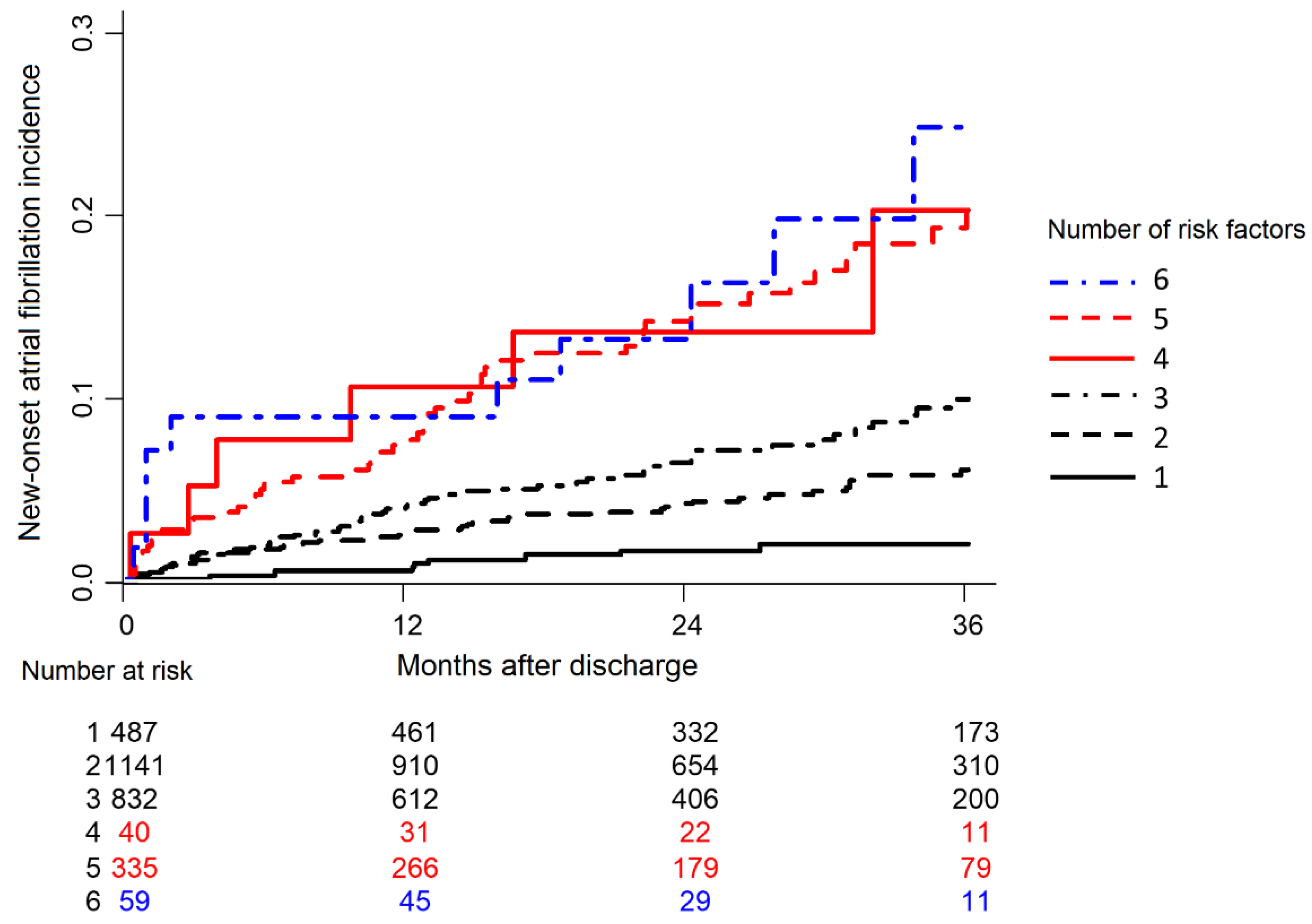
3.3. Survival Tree Analysis for NOAF
3.4. Prognostic Impact of NOAF on Patient Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chamberlain, A.M.; Redfield, M.M.; Alonso, A.; Weston, S.A.; Roger, V.L. Atrial Fibrillation and Mortality in Heart Failure. Circ. Heart Fail. 2011, 4, 740–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsigkas, G.; Apostolos, A.; Despotopoulos, S.; Vasilagkos, G.; Kallergis, E.; Leventopoulos, G.; Mplani, V.; Davlouros, P. Heart failure and atrial fibrillation: New concepts in pathophysiology, management, and future directions. Heart Fail. Rev. 2021. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Heijman, J.; Linz, D.; Schotten, U. Dynamics of Atrial Fibrillation Mechanisms and Comorbidities. Annu. Rev. Physiol. 2021, 83, 83–106. [Google Scholar] [CrossRef] [PubMed]
- Huizar, J.F.; Ellenbogen, K.A.; Tan, A.Y.; Kaszala, K. Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2328–2344. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, U.M.; Jhund, P.; Abraham, W.T.; Desai, A.S.; Dickstein, K.; Packer, M.; Rouleau, J.L.; Solomon, S.D.; Swedberg, K.; Zile, M.; et al. Type of Atrial Fibrillation and Outcomes in Patients With Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2017, 70, 2490–2500. [Google Scholar] [CrossRef]
- Mujović, N.; Marinković, M.; Mihajlović, M.; Mujović, N.; Potpara, T.S. Risk factor modification for the primary and secondary prevention of atrial fibrillation. Part 1. Kardiol. Pol. 2020, 78, 181–191. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.S.; Di Tullio, M.R.; Qian, M.; Wu, M.; Thompson, J.L.; Mann, D.L.; Sacco, R.L.; Pullicino, P.M.; Freudenberger, R.S.; Teerlink, J.R.; et al. Clinical and Echocardiographic Factors Associated With New-Onset Atrial Fibrillation in Heart Failure—Subanalysis of the WARCEF Trial. Circ. J. 2016, 80, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Campbell, N.G.; Cantor, E.J.; Sawhney, V.; Duncan, E.R.; DeMartini, C.; Baker, V.; Diab, I.G.; Dhinoja, M.; Earley, M.J.; Sporton, S.; et al. Predictors of new onset atrial fibrillation in patients with heart failure. Int. J. Cardiol. 2014, 175, 328–332. [Google Scholar] [CrossRef]
- Lee, S.E.; Cho, H.-J.; Lee, H.-Y.; Yang, H.-M.; Choi, J.-O.; Jeon, E.-S.; Kim, M.-S.; Kim, J.-J.; Hwang, K.-K.; Chae, S.C.; et al. A multicentre cohort study of acute heart failure syndromes in Korea: Rationale, design, and interim observations of the Korean Acute Heart Failure (KorAHF) registry. Eur. J. Heart Fail. 2014, 16, 700–708. [Google Scholar] [CrossRef]
- Simon, R.; Makuch, R.W. A non-parametric graphical representation of the relationship between survival and the occurrence of an event: Application to responder versus non-responder bias. Stat. Med. 1984, 3, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Ó’Hartaigh, B.; Janszky, I.; Romundstad, P.R.; Tonstad, S.; Vatten, L.J. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality—A systematic review and dose-response meta-analysis of prospective studies. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 504–517. [Google Scholar] [CrossRef] [PubMed]
- Hai, J.; Chan, P.-H.; Tse, H.-F.; Siu, C.-W. Slow Heart Rate Predicts New Occurrence of Atrial Fibrillation. Heart Lung Circ. 2015, 24, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Skov, M.W.; Bachmann, T.N.; Rasmussen, P.V.; Olesen, M.S.; Pietersen, A.; Graff, C.; Lind, B.; Struijk, J.J.; Køber, L.; Haunsø, S.; et al. Association Between Heart Rate at Rest and Incident Atrial Fibrillation (from the Copenhagen Electrocardiographic Study). Am. J. Cardiol. 2016, 118, 708–713. [Google Scholar] [CrossRef]
- O’Neal, W.T.; AlMahmoud, M.F.; Soliman, E.Z. Resting Heart Rate and Incident Atrial Fibrillation in the Elderly. Pacing Clin. Electrophysiol. 2015, 38, 591–597. [Google Scholar] [CrossRef]
- Choi, Y.W.; Park, M.; Lim, Y.-H.; Myung, J.; Kim, B.S.; Lee, Y.; Shin, J.-H.; Park, H.-C.; Shin, J.; Kim, C.K.; et al. Independent effect of physical activity and resting heart rate on the incidence of atrial fibrillation in the general population. Sci. Rep. 2019, 9, 11228. [Google Scholar] [CrossRef]
- Yu, Z.; Zhang, D.; Ji, Q.; Yi, F. Inhibition of the renin-angiotensin-aldosterone system prevents and cures atrial fibrillation: An overview of systematic reviews. Medicine 2021, 100, e25559. [Google Scholar] [CrossRef]
- Chen, S.; Acou, W.J.; Kiuchi, M.G.; Meyer, C.; Sommer, P.; Martinek, M.; Schratter, A.; Andrea, B.R.; Ling, Z.; Liu, S.; et al. Association of Preoperative Renin-Angiotensin System Inhibitors With Prevention of Postoperative Atrial Fibrillation and Adverse Events: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e194934. [Google Scholar] [CrossRef] [Green Version]
- Neefs, J.; van den Berg, N.W.E.; Limpens, J.; Berger, W.R.; Boekholdt, S.M.; Sanders, P.; de Groot, J.R. Aldosterone Pathway Blockade to Prevent Atrial Fibrillation: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2017, 231, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Filippatos, G.; Bakris, G.L.; Pitt, B.; Agarwal, R.; Rossing, P.; Ruilope, L.M.; Butler, J.; Lam, C.S.; Kolkhof, P.; Roberts, L.; et al. Finerenone Reduces New-Onset Atrial Fibrillation in Patients With Chronic Kidney Disease and Type 2 Diabetes. J. Am. Coll. Cardiol. 2021, 78, 142–152. [Google Scholar] [CrossRef]
- Ziff, O.J.; Samra, M.; Howard, J.P.; Bromage, D.; Ruschitzka, F.; Francis, D.P.; Kotecha, D. Beta-blocker efficacy across different cardiovascular indications: An umbrella review and meta-analytic assessment. BMC Med. 2020, 18, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Sai, C.; Li, J.; Ruiyan, M.; Yingbin, X. Atorvastatin prevents postoperative atrial fibrillation in patients undergoing cardiac surgery. Hell. J. Cardiol. 2019, 60, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Jong, G.-P.; Chen, H.-Y.; Li, S.-Y.; Liou, Y.-S. Long-term effect of antihypertensive drugs on the risk of new-onset atrial fibrillation: A longitudinal cohort study. Hypertens. Res. 2014, 37, 950–953. [Google Scholar] [CrossRef] [PubMed]
- Pfenniger, A.; Geist, G.E.; Arora, R. Autonomic Dysfunction and Neurohormonal Disorders in Atrial Fibrillation. Card. Electrophysiol. Clin. 2021, 13, 183–190. [Google Scholar] [CrossRef]
- Tan, B.Y.; Ho, J.S.Y.; Sia, C.-H.; Boi, Y.; Foo, A.S.; Dalakoti, M.; Chan, M.Y.; Ho, A.F.; Leow, A.S.; Chan, B.P.; et al. Left Atrial Volume Index Predicts New-Onset Atrial Fibrillation and Stroke Recurrence in Patients with Embolic Stroke of Undetermined Source. Cerebrovasc. Dis. 2020, 49, 285–291. [Google Scholar] [CrossRef]
- Kiuchi, K.; Shirakabe, A.; Kobayashi, N.; Okazaki, H.; Matsushita, M.; Shibata, Y.; Goda, H.; Shigihara, S.; Asano, K.; Tani, K.; et al. Prognostic impact of new-onset atrial fibrillation associated with worsening heart failure in aging patients with severely decompensated acute heart failure. Int. J. Cardiol. 2019, 302, 88–94. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SR Group (N = 2707) | NOAF Group (N = 187) | p Value | |
|---|---|---|---|
| Age, year | 66.2 ± 15.5 | 70.8 ± 13.2 | <0.001 |
| Male (%). | 1475 (54.5) | 92 (49.2) | 0.18 |
| BMI, kg/m2 | 23.4 ± 3.93 | 23.8 ± 3.65 | 0.19 |
| Current smoking (%) | 588 (21.7) | 27 (14.4) | 0.01 |
| Hypertension (%) | 1655 (61.1) | 133 (71.1) | 0.008 |
| Diabetes mellitus (%) | 1159 (42.8) | 89 (47.6) | 0.23 |
| Chronic kidney disease (%) | 397 (14.7) | 36 (19.3) | 0.11 |
| Chronic obstructive lung disease (%) | 266 (9.8) | 20 (10.7) | 0.80 |
| Cerebrovascular accident (%) | 353 (13.0) | 32 (17.1) | 0.14 |
| Implantable cardioverter defibrillator (%) | 73 (2.7) | 7 (3.7) | 0.54 |
| Cardiac resynchronization therapy (%) | 46 (1.7) | 4 (2.1) | 0.88 |
| Percutaneous coronary intervention (%) | 527 (19.5) | 49 (26.2) | 0.03 |
| Coronary artery bypass surgery (%) | 145 (5.4) | 17 (9.1) | 0.04 |
| Ischemic heart disease (%) | 1387 (51.2) | 98 (52.4) | 0.82 |
| Dilated cardiomyopathy (%) | 214 (7.9) | 23 (12.3) | 0.05 |
| Valvular heart disease (%) | 195 (7.2) | 29 (15.5) | <0.001 |
| Heart failure category | <0.001 | ||
| De novo heart failure | 1648 (60.9) | 79 (42.2) | |
| Acute decompensated heart failure | 1059 (39.1) | 108 (57.8) | |
| Systolic BP, mmHg | 134.0 ± 31.3 | 133.2 ± 31.11 | 0.76 |
| Diastolic BP, mmHg | 79.4 ± 18.8 | 78.6 ± 17.1 | 0.56 |
| Heart rate, beats/min | 91.0 ± 22.2 | 85.6 ± 22.8 | 0.001 |
| NYHA class (%) | 0.28 | ||
| II | 459 (17.0) | 24 (12.8) | |
| III | 952 (35.2) | 73 (39.0) | |
| IV | 1296 (47.9) | 90 (48.1) | |
| Discharge medication | |||
| RAS blocker (%) | 1971 (72.8) | 129 (69.0) | 0.29 |
| Beta-blocker (%) | 1490 (55.0) | 100 (53.5) | 0.73 |
| Aldosterone antagonist (%) | 1215 (44.9) | 79 (42.2) | 0.53 |
| Nitrates (%) | 695 (25.7) | 54 (28.9) | 0.38 |
| Loop diuretics (%) | 1887 (69.7) | 148 (79.1) | 0.008 |
| Thiazide (%) | 206 (7.6) | 12 (6.4) | 0.65 |
| Statin (%) | 1342 (49.6) | 92 (49.2) | 0.98 |
| Clinical status on discharge | |||
| BMI, kg/m2 | 22.5 ± 3.8 | 22.8 ± 3.7 | 0.39 |
| Systolic BP, mmHg | 115.2 ± 18.4 | 115.6 ± 19.6 | 0.78 |
| Diastolic BP, mmHg | 67.3 ± 11.6 | 65.3 ± 10.3 | 0.02 |
| Heart rate, beats/min | 77.6 ± 13.4 | 73.5 ± 13.2 | <0.001 |
| NYHA class (%) | 0.26 | ||
| I | 522 (20.0) | 29 (16.1) | |
| II | 1786 (68.5) | 136 (75.6) | |
| III | 178 (6.8) | 9 (5.0) | |
| IV | 121 (4.6) | 6 (3.3) | |
| SR Group (N = 2707) | NOAF Group (N = 187) | p Value | |
|---|---|---|---|
| Laboratory tests at admission | |||
| Sodium, mmol/L | 137.7 ± 4.5 | 137.3 ± 4.3 | 0.17 |
| Creatinine, mg/dL | 1.5 ± 1.6 | 1.7 ± 1.7 | 0.12 |
| BUN, mg/dL | 25.3 ± 16.0 | 28.6 ± 17.3 | 0.006 |
| BNP, pg/mL | 1445 ± 1335 | 1844 ± 1624 | 0.02 |
| NT-proBNP, pg/mL | 9208 ± 10,875 | 11,474 ± 16,883 | 0.05 |
| Electrocardiographic parameters | |||
| RBBB (%) | 171 (6.3) | 8 (4.3) | 0.34 |
| LBBB (%) | 186 (6.9) | 13 (7.0) | 1.00 |
| Interventricular conduction disturbance (%) | 129 (4.8) | 10 (5.4) | 0.84 |
| Q wave (%) | 392 (14.5) | 30 (16.1) | 0.61 |
| PR interval, msec | 167.3 ± 32.9 | 179.3 ± 49.5 | <0.001 |
| QRS width, msec | 107.1 ± 28.6 | 110.0 ± 31.1 | 0.18 |
| QT interval, msec | 396.2 ± 58.9 | 408.7 ± 68.3 | 0.006 |
| Corrected QT interval, msec | 476.2 ± 43.7 | 475.8 ± 49.2 | 0.90 |
| Heart rate, beats/min | 90.9 ± 22.4 | 85.9 ± 23.1 | 0.003 |
| Echocardiographic parameters | |||
| LV end-diastolic dimension, mm | 58.3 ± 10.2 | 59.0 ± 10.2 | 0.37 |
| LV end-systolic dimension, mm | 46.5 ± 12.5 | 46.5 ± 12.4 | 0.999 |
| LV EF, % | 36.3 ± 15.2 | 36.8 ± 16.0 | 0.63 |
| LA diameter, mm | 44.9 ± 8.2 | 47.7 ± 8.4 | <0.001 |
| Peak TR velocity, m/sec | 2.9 ± 0.6 | 2.9 ± 0.6 | 0.94 |
| Estimated RV systolic pressure, mmHg | 43.3 ± 15.6 | 45.9 ± 17.1 | 0.07 |
| Laboratory tests at discharge | |||
| Sodium, mmol/L | 138.0 ± 3.8 | 137.8 ± 3.7 | 0.49 |
| Creatinine, mg/dL | 1.4 ± 1.5 | 1.7 ± 1.8 | 0.03 |
| BUN, mg/dL | 23.8 ± 14.9 | 27.3 ± 18.3 | 0.002 |
| BNP, pg/mL | 1261 ± 1277 | 1605 ± 1440 | 0.03 |
| NT-proBNP, pg/mL | 8555 ± 10,668 | 10,426 ± 16,667 | 0.10 |
| Multivariable | ||||
|---|---|---|---|---|
| Variable | HR | 95% CI | p Value | |
| Age | 1.03 | 1.01 | 1.04 | <0.001 |
| Worsening heart failure | 1.66 | 1.22 | 2.24 | 0.001 |
| Valvular heart disease | 1.67 | 1.11 | 2.51 | 0.01 |
| LA diameter | 1.03 | 1.01 | 1.05 | <0.001 |
| Use of loop diuretics at discharge | 1.61 | 1.12 | 2.32 | 0.01 |
| Heart rate at discharge | 0.98 | 0.97 | 1.00 | 0.01 |
| Creatinine | 1.11 | 1.03 | 1.20 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.-I.; Lee, S.E.; Kim, M.-S.; Lee, H.-Y.; Cho, H.-J.; Choi, J.O.; Jeon, E.-S.; Hwang, K.-K.; Chae, S.C.; Baek, S.H.; et al. Prognostic Impact and Predictors of New-Onset Atrial Fibrillation in Heart Failure. Life 2022, 12, 579. https://doi.org/10.3390/life12040579
Choi H-I, Lee SE, Kim M-S, Lee H-Y, Cho H-J, Choi JO, Jeon E-S, Hwang K-K, Chae SC, Baek SH, et al. Prognostic Impact and Predictors of New-Onset Atrial Fibrillation in Heart Failure. Life. 2022; 12(4):579. https://doi.org/10.3390/life12040579
Chicago/Turabian StyleChoi, Hyo-In, Sang Eun Lee, Min-Seok Kim, Hae-Young Lee, Hyun-Jai Cho, Jin Oh Choi, Eun-Seok Jeon, Kyung-Kuk Hwang, Shung Chull Chae, Sang Hong Baek, and et al. 2022. "Prognostic Impact and Predictors of New-Onset Atrial Fibrillation in Heart Failure" Life 12, no. 4: 579. https://doi.org/10.3390/life12040579
APA StyleChoi, H.-I., Lee, S. E., Kim, M.-S., Lee, H.-Y., Cho, H.-J., Choi, J. O., Jeon, E.-S., Hwang, K.-K., Chae, S. C., Baek, S. H., Kang, S.-M., Choi, D.-J., Yoo, B.-S., Kim, K. H., Cho, M.-C., Oh, B.-H., & Kim, J.-J. (2022). Prognostic Impact and Predictors of New-Onset Atrial Fibrillation in Heart Failure. Life, 12(4), 579. https://doi.org/10.3390/life12040579