1. Introduction
With an incidence of over 1.5 million worldwide per annum, breast cancer continues to be the most common cancer affecting the female population [
1,
2]. The prime and most effective treatment in most cases is surgery, and a neoplasm resection is in fact the primary treatment option in over 40% of patients [
3]. Moreover, while it is true that breast-conserving surgery (BSC) and sentinel lymph node biopsy are widely used, radical mastectomy is the standard surgical treatment for female patients who have contraindications for BSC or who have a positive sentinel lymph node biopsy [
4]. Although general anaesthesia (GA), often in association with loco-regional procedures, is the most commonly used anaesthetic technique for radical mastectomy surgery, its complications and side effects, such as nausea, vomiting, and considerable postoperative pain, increase postoperative morbidity [
5]. A growing body of research has been dedicated to investigating the use of loco-regional anaesthesia either in association with or, in some cases, in substitution of GA during breast surgery [
6,
7]. Those studies have shown that these techniques can reduce postoperative complications and provide the optimal control of postoperative pain, thus minimising the need for the use of opioids.
The regional anaesthetic techniques most commonly used for breast surgery are: a thoracic epidural block, thoracic paravertebral block, erector spinae plane block, deep and superficial serratus anterior blocks, as well as interpectoral plane (IPP) and pectoserratus plane (PSP) blocks [
7]. The high risk of pneumothorax, haemorrhage, dural penetration, and hypotension linked to these techniques needs, nevertheless, to be taken into consideration [
8]. First described by Blanco et al. in 2012, the Pectoralis II (PECS II) fascial block is an inter-fascial plane block between the pectoralis major and minor muscles and between the pectoralis minor and serratus anterior muscles at the levels of the third and fourth ribs along the mid-axillary line. The low incidence of complications seemingly connected to the novel approach to breast cancer surgery is at least in part due to ultrasound imaging guidance [
9]. Moreover, a recent international consensus study involving experts using a three-round Delphi method produced a standardised nomenclature of regional anaesthetic techniques for the abdominal wall, paraspinal, and chest wall [
10]. Based on the consensus study’s recommendations, the original PECS II block should now be referred to as a combination of IPP and PSP [
10].
The current work describes the case of an elderly patient who underwent a left radical mastectomy due to breast cancer and a positive sentinel lymph node biopsy under ultrasound-guided IPP and PSP blocks anaesthesia.
2. Case Report
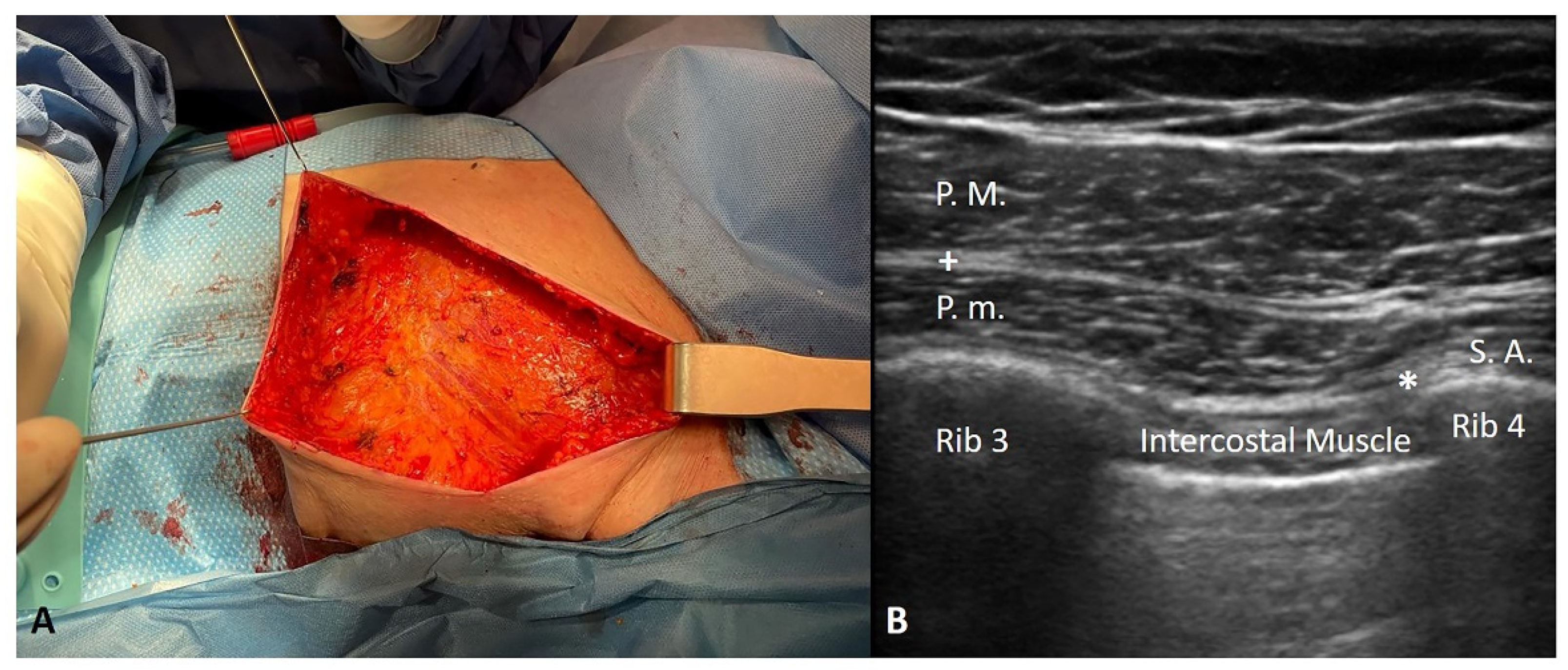
A 94-year-old woman with breast cancer and a positive sentinel lymph node biopsy was scheduled for a left radical mastectomy (
Figure 1A). The patient’s medical history included pathologies such as dementia, hypertension, Mobitz I type BAV, hypothyroidism (the patient was receiving replacement therapy), osteoporosis, megaloblastic anaemia, recent interstitial pneumonia, and METS > 4 < 10. According to the classification of the American Society of Anesthesiologists (ASA), she was an ASA III, thus a patient with a severe systemic disease that was not life threatening.
The surgical team decided against using GA, orotracheal intubation, and intra or postoperative opioids because of the complications (delirium, disrupted psychomotor performance, cardio-respiratory depression, and ileus) linked to their use, and they hoped to discharge her as soon as possible after surgery in view of her age (94 years), clinical complexity, and comorbidities. The team opted for performing combined IPP and PSP blocks in the recovery room. This was carried out using an ultrasound linear probe (high frequency) and an ultrasound Sonosite Edge II machine in the following manner: a 50 mm Pajunk echogenic needle was used to inject ropivacaine 0.5% 10 mL (in the inter-fascial plane between the major and minor pectoralis muscles) +20 mL (in the inter-fascial plane between the pectoralis minor and serratus anterior muscles) (
Figure 1B).
The patient was transferred to the operating room 20 min after the block was performed; at the time the incision was carried out, the Numerical Rating Scale (NRS) was equal to 0. As the patient seemed uncomfortable in the unfamiliar environment, a low dose propofol infusion (1.4 mg/kg/h) was begun.
The patient’s Richmond Agitation-Sedation Scale (RASS) was equal to -1. Her ECG, non-invasive blood pressure (NIBP), oxygen saturation (SpO2), end-tidal CO2 (EtCO2), and Bispectral Index (BIS) were all being monitored.
The patient’s BIS was between 80 and 65; moreover, she maintained spontaneous breathing with a nasal cannula O2 3 lt/min, maintaining a saturation between 94 and 98% (saturation in ambient air 93%) and had no episodes of apnoea. The patient was haemodynamically stable throughout the surgery. There was a single hypertensive peak of 150/90 mmHg thirty minutes after the incision was made; it was treated with 10 mg of urapidil. During surgery, 70 mg of ketamine was administered in boluses (30 mg pre-incision, 20 mg 10 min post-incision, and 20 mg 30 min post-incision). Before suturing and inserting the drainage, the surgeon infiltrated the surgical wound with 200 mg of lidocaine. Throughout the procedure, the patient’s numeric rating scale (NRS) was between 0 and 3 (required for awake patients). At the end of the surgery, the patient was transferred to the recovery room; her vital parameters were stable and pain control was good. An hour later, she was transferred to the ward with an NRS = 0.
During the post-operative period, a 1 g paracetamol solution for infusion was administered 3 h after surgery (1 h after she arrived in the ward), 8 h later, and 16 h after that. The patient did not require rescue analgesia, and she was discharged from hospital 24 h after the surgery.
3. Discussion
In the case described above, analgesia of a complex elderly patient’s pectoral, mammary, inframammary and axillary regions during a mastectomy was provided by IPP and PSP blocks. The fourth, fifth, and sixth intercostal nerves supply the mammary region, whereas the medial (C8-T1) and lateral (C5-C7) pectoral nerves innervate the pectoralis major and minor muscles and the overlying fasciae [
9].
The local anaesthetic spread between the clavipectoral fascia and the superficial border of the serratus anterior muscles anaesthetising the anterior cutaneous branches of the intercostal nerves situated between the thoracic spinal nerve (T4-6), the intercostobrachial and the long thoracic nerve [
10]. To reduce the risk of a vascular and pleural puncture during the procedure, the direction in which the needle was inserted was medial to lateral. In addition to its relative simplicity, the procedure described carries a minimal risk of injuries to the pleura and blood vessels and more reliably provides analgesia with respect to the infiltration of the surgical wound with a local anaesthetic [
1]. Indeed, Torre et al. reported that PECS II could potentially provide analgesia for lateral incisions involving minimally invasive cardiac surgery [
11].
At the current time, IPP and PSP blocks are commonly used as part of multimodal analgesia for breast surgery, for which they were originally developed. Several studies have demonstrated that they are effective in reducing nausea, vomiting, postoperative narcotic consumption, and the length of the hospital stay [
12]. In the case described here, ultrasound-guided IPP and PSP blocks were used to avoid GA in an elderly, complicated patient. This was done to circumvent the side effects and complications of GA which, of course, include nausea, vomiting, considerable postoperative pain, and increased morbidity in many breast surgery patients and, in particular, in elderly, complex ones [
4]. It goes without saying that the surgical team wanted to avoid, if possible, an orotracheal intubation as well as intra and post-operative opioids in view of their complications (delirium, worse psychomotor performance, cardio-respiratory depression, and ileus). At the same time, they sought to discharge the patient as soon as possible to avoid their disorientation in an unfamiliar place and aggravating her comorbidities.
As a final note, we would like to point out that the fibrous component of the fascial tissues increases with aging [
13,
14]; this could explain their capacity to contain an anaesthetic for a longer time, thus prolonging its effect. In other words, the analgesic effect may last longer because the fascial tissues of an elderly person absorb and spread those drugs in a different manner, with respect to younger individuals.
4. Conclusions
In conclusion, ultrasound-guided IPP and PSP blocks were found to be a simple, safe, and effective technique to anaesthetise a difficult, elderly patient undergoing a mastectomy. Further studies will be able to confirm its safety and efficacy in patients of all ages with a complex medical history and confirm that it has no or minimal complications and side effects.
Author Contributions
Conceptualization, C.P. and D.E.T.; methodology, C.P.; software, C.P.; validation, C.P., D.E.T. and C.S.; formal analysis, C.P.; investigation, D.E.T.; resources, C.P., D.E.T. and C.S.; data curation, C.P.; writing—original draft preparation, C.P.; writing—review and editing, C.P., D.E.T. and C.S.; visualization, A.U.B. and R.D.C.; supervision, C.P.; project administration, C.P. and D.E.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the University of Padua.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Acknowledgments
The authors thank the Institute of Human Anatomy of the University of Padua.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Holly, E.; Elizabeth, D.; Farah, M.; Erin, P.; Joanne, C.; Rebecca, R.; Charlene, S. Breast cancer surgical treatment choices in Newfoundland and Labrador, Canada: Patient and surgeon perspectives. J. Public Health Res. 2017, 6, 867–1867. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Tyczynski, J.E.; Bray, F.; Parkin, D.M. Breast cancer in Europe—ENCR cancer fact sheet. Eur. Netw. Cancer Regist. 2002, 2, 1–4. [Google Scholar]
- Wesmiller, S.W.; Bender, C.M.; Conley, Y.P.; Bovbjerg, D.H.; Ahrendt, G.; Bonaventura, M.; Sereika, S.M. A prospective study of nausea and vomiting after breast cancer surgery. J. PeriAnesthesia Nurs. 2017, 32, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Reihnér, E.; Grunditz, R.; Giesecke, K.; Gustafsson, L.L. Postoperative nausea and vomiting after breast surgery: Efficacy of prophylactic ondansetron and droperidol in a randomized placebo-controlled study. Eur. J. Anaesthesiol 2000, 17, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, A.; Yamasaki, M.; Yokota, I.; Mori, M.; Matsuda, M.; Yamaguchi, Y.; Yamakita, S.; Ueno, H.; Sawa, T.; Taguchi, T.; et al. Classification of acute pain trajectory after breast cancer surgery identifies patients at risk for persistent pain: A prospective observational study. J. Pain Res. 2018, 11, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Senapathi, T.G.A.; Widnyana, I.M.G.; Aribawa, I.G.N.M.; Jaya, A.A.G.P.S.; Junaedi, I.M.D. Combined ultrasound-guided Pecs II block and general anesthesia are effective for reducing pain from modified radical mastectomy. J. Pain Res. 2019, 12, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Liu, X.; Li, F.; Xue, Z.; Li, Y.; Qian, B. Anesthetic effect of ultrasound-guided multiple-nerve blockade in modified radical mastectomy in patients with breast cancer. Medicine 2021, 100, e24786. [Google Scholar] [CrossRef] [PubMed]
- Blanco, R.; Fajardo, M.; Parras Maldonado, T. Ultrasound description of Pecs II (modified Pecs I): A novel approach to breast surgery. Rev. Esp. Anestesiol. Reanim. 2012, 59, 470–475. [Google Scholar] [CrossRef] [PubMed]
- El-Boghdadly, K.; Wolmarans, M.; Stengel, A.D.; Albrecht, E.; Chin, K.J.; Elsharkawy, H.; Kopp, S.; Mariano, E.R.; Xu, J.L.; Adhikary, S.; et al. Standardizing nomenclature in regional anesthesia: An ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Reg. Anesth. Pain Med. 2021, 46, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Torre, D.E.; Pirri, C.; Contristano, M.; Behr, A.U.; De Caro, R.; Stecco, C. Ultrasound-Guided PECS II + Serratus Plane Fascial Blocks Are Associated with Reduced Opioid Consumption and Lengths of Stay for Minimally Invasive Cardiac Surgery: An Observational Retrospective Study. Life 2022, 12, 805. [Google Scholar] [CrossRef] [PubMed]
- Bashandy, G.M.; Abbas, D.N. Pectoral nerves I and II blocks in multimodal analgesia for breast cancer surgery: A randomized clinical trial. Reg. Anesth. Pain Med. 2015, 40, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Petrelli, L.; Pérez-Bellmunt, A.; Ortiz-Miguel, S.; Fede, C.; De Caro, R.; Miguel-Pérez, M.; Stecco, C. Fetal Fascial Reinforcement Development: From “a White Tablet” to a Sculpted Precise Organization by Movement. Biology 2022, 11, 735. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Pirri, C.; Fede, C.; Guidolin, D.; Biz, C.; Petrelli, L.; Porzionato, A.; Macchi, V.; De Caro, R.; Stecco, C. Age-Related Alterations of Hyaluronan and Collagen in Extracellular Matrix of the Muscle Spindles. J. Clin. Med. 2021, 11, 86. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
