
Psoriasis Management Challenges Regarding Difficult-to-Treat Areas: Therapeutic Decision and Effectiveness

 , , ,
, , ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
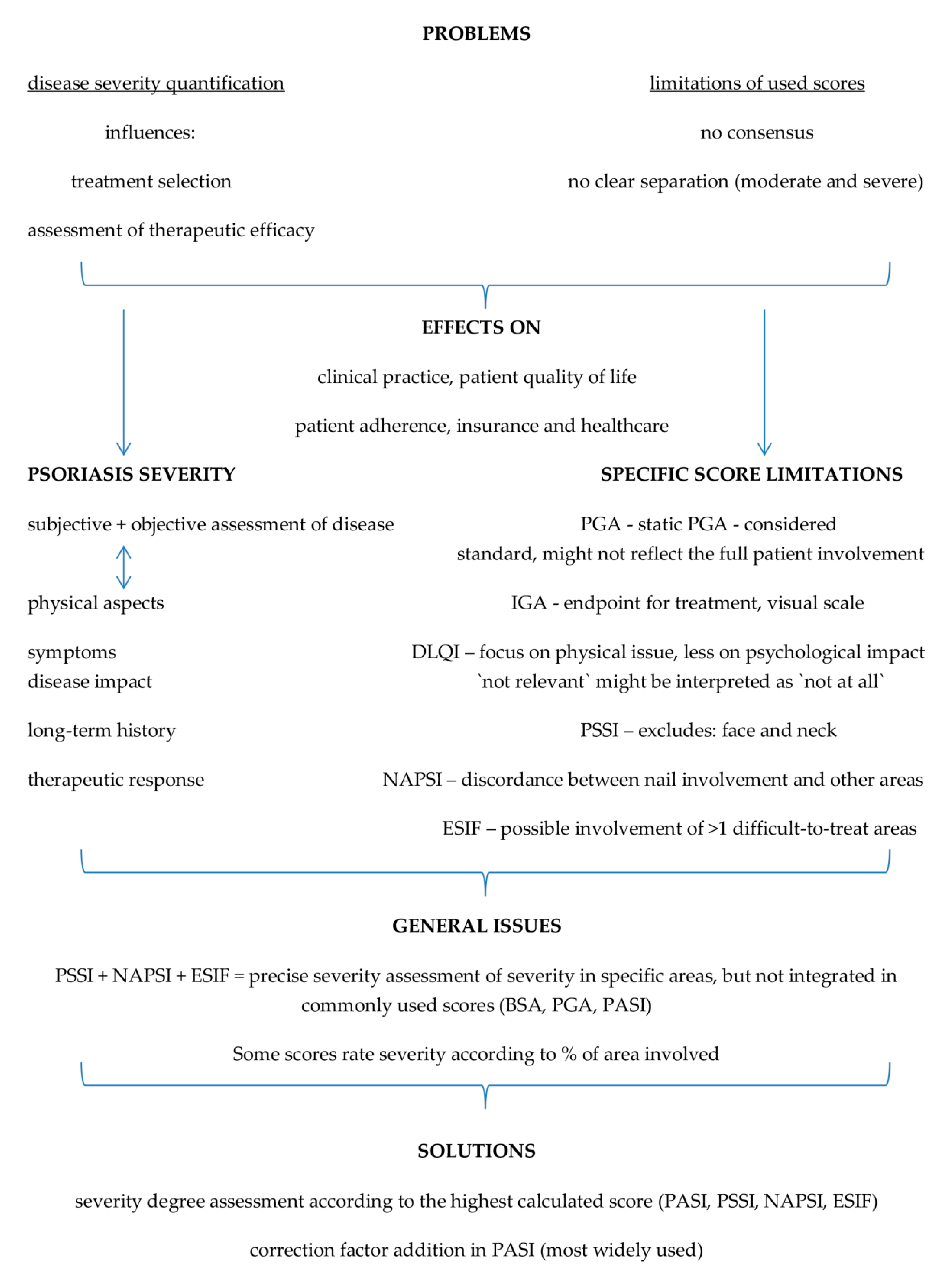
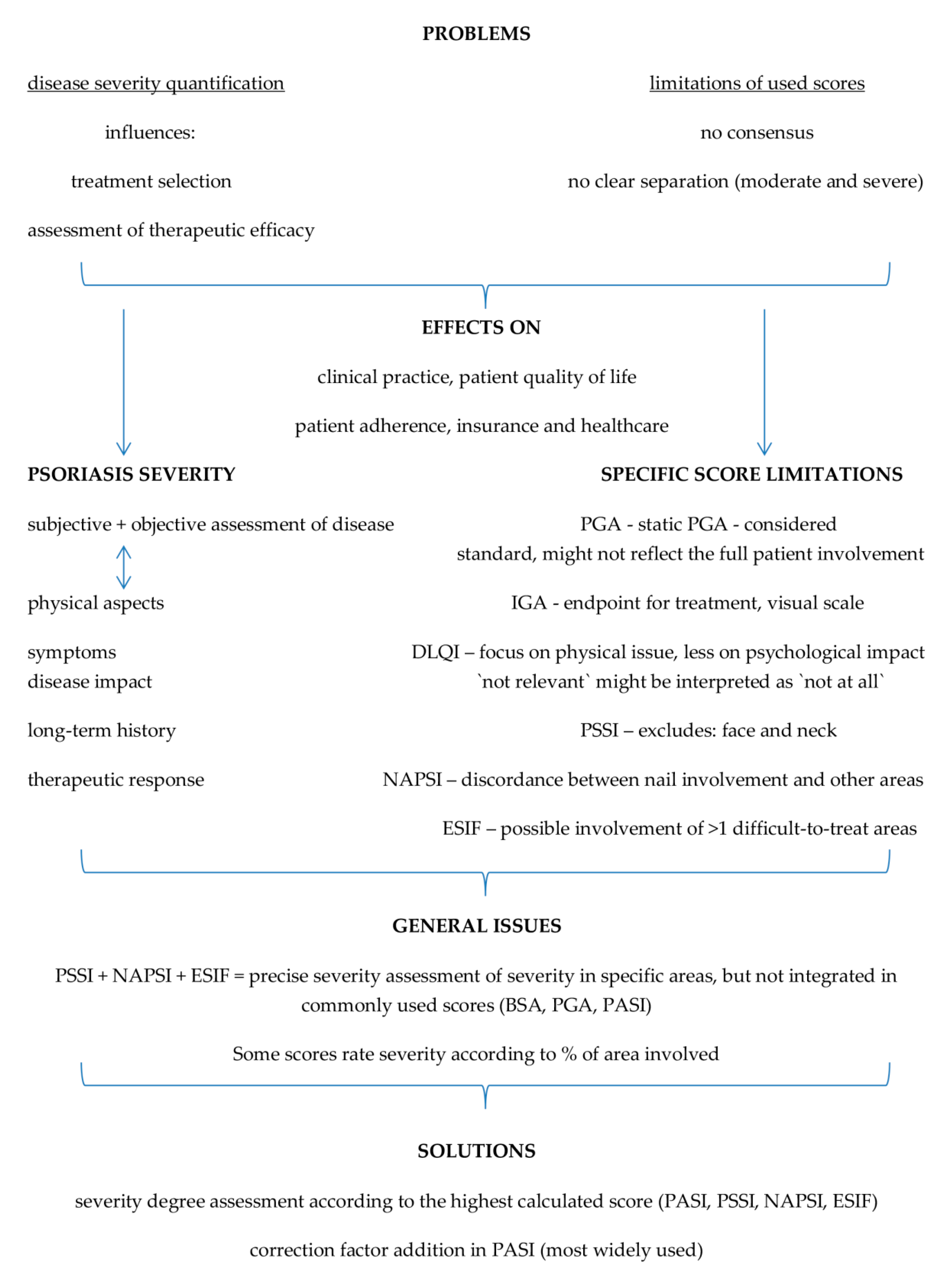
3. Current Challenges in Disease Severity and Treatment Goals
3.1. Body Surface Area (BSA)
3.2. Physician‘s Global Assessment (PGA)
3.3. The Psoriasis Area and Severity Index (PASI)
3.4. The Investigator Global Assessment (IGA) Scale
3.5. The Dermatology Life Quality Index (DLQI)
3.6. The Psoriasis Scalp Severity Index (PSSI)
3.7. The Nail Psoriasis Severity Index (NAPSI)
3.8. The Erythema, Scaling, Induration, and Fissuring (ESIF)
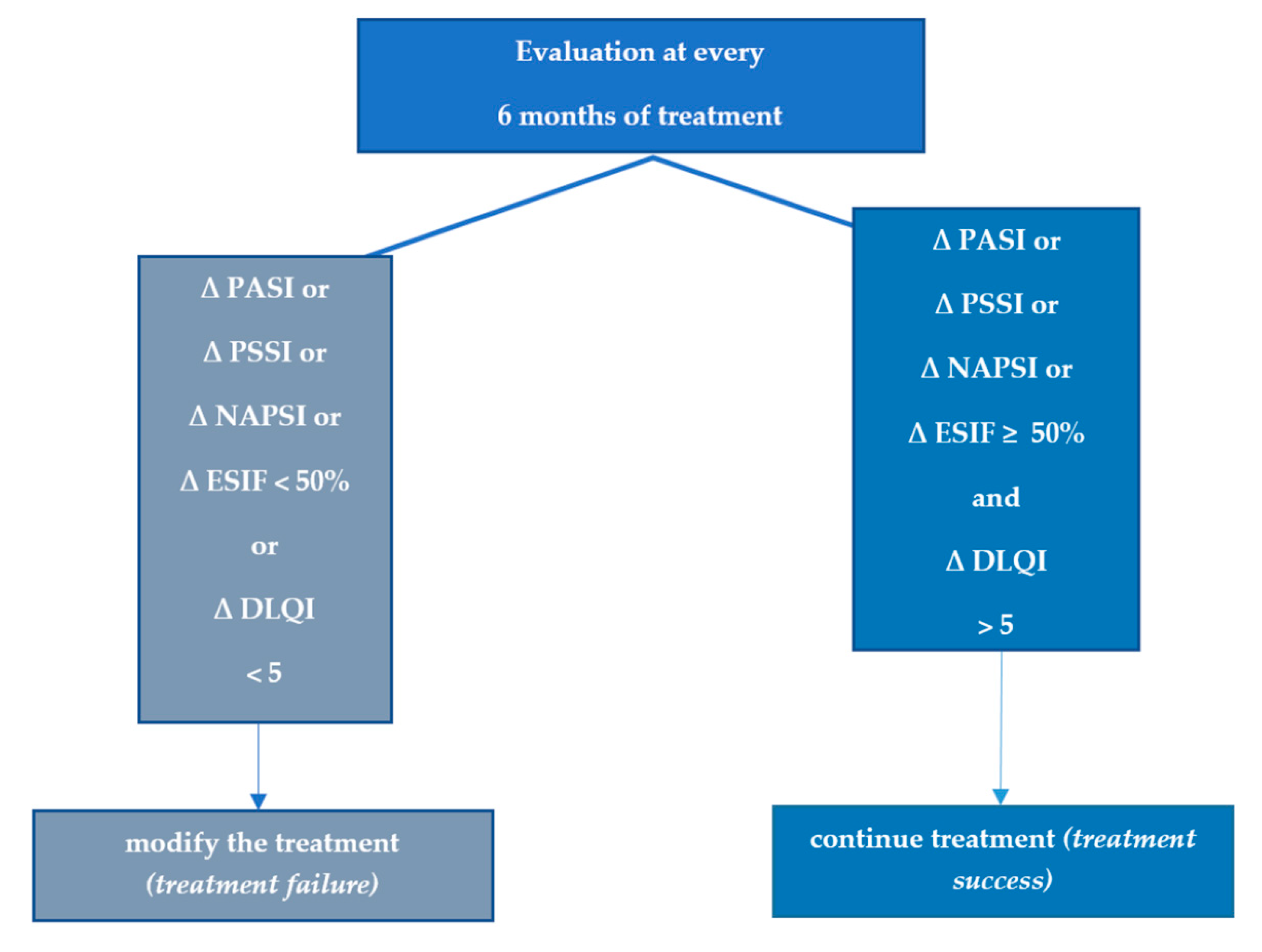
4. The Challenges of Individualized Treatment and Evaluating the Treatment Success
5. Treatment Goals and Treat-to-Target
6. Treatment Success or Failure for Patients with Difficult-to-Treat Areas
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Study 2010 (GBD 2010) Results by Cause 1990–2010. Available online: https://ghdx.healthdata.org/record/ihme-data/gbd-2010-results-cause-1990-2010 (accessed on 10 October 2022).
- Reich, K.; Krüger, K.; Mössner, R.; Augustin, M. Epidemiology and clinical pattern of psoriatic arthritis in Germany: A prospective interdisciplinary epidemiological study of 1511 patients with plaque-type psoriasis. Br. J. Dermatol. 2009, 160, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Harden, J.L.; Krueger, J.G.; Bowcock, A.M. The immunogenetics of psoriasis: A comprehensive review. J. Autoimmun. 2015, 64, 66–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niculet, E.; Radaschin, D.S.; Nastase, F.; Draganescu, M.; Baroiu, L.; Miulescu, M.; Arbune, M.; Tatu, A.L. Influence of phytochemicals in induced psoriasis. Exp. Ther. Med. 2020, 20, 3421–3424. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Kishimoto, M.; Sugai, J.; Komine, M.; Ohtsuki, M. Risk factors for the development of psoriasis. Int. J. Mol. Sci. 2019, 20, 4347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.K.; Del Rosso, J.Q. Drug-provoked psoriasis: Is it drug induced or drug aggravated?: Understanding pathophysiology and clinical relevance. J. Clin. Aesthetic Dermatol. 2010, 3, 32–38. [Google Scholar]
- International Federation of Psoriasis Associations. World Psoriasis Day. 2015. Available online: https://ifpa-pso.com/our-actions/worldpsoriasis-day (accessed on 19 September 2022).
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M.; Global Psoriasis Atlas. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modelling study. BMJ 2020, 369, 1590. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.M.; Ashcroft, D.M. Identification and management of psoriasis and associated comorbidity (IMPACT) project team. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [Green Version]
- AlQassimi, S.; AlBrashdi, S.; Galadari, H.; Hashim, M.J. Global burden of psoriasis—Comparison of regional and global epidemiology, 1990 to 2017. Int. J. Dermatol. 2020, 59, 566–571. [Google Scholar] [CrossRef]
- Enamandram, M.; Kimball, A.B. Psoriasis epidemiology: The interplay of genes and the environment. J. Investig. Dermatol. 2013, 133, 287–289. [Google Scholar] [CrossRef] [Green Version]
- Nicolescu, A.C.; Bucur, Ș.; Giurcăneanu, C.; Gheucă-Solovăstru, L.; Constantin, T.; Furtunescu, F.; Ancuța, I.; Constantin, M.M. Prevalence and characteristics of psoriasis in Romania—First study in overall population. J. Pers. Med. 2021, 11, 523. [Google Scholar] [CrossRef]
- Boca, A.N.; Ilies, R.F.; Vesa, S.; Pop, R.; Tataru, A.D.; Buzoianu, A.D. The first nation-wide study revealing epidemiologic data and life quality aspects of psoriasis in Romania. Exp. Ther. Med. 2019, 18, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Krueger, G.G.; Feldman, S.R.; Camisa, C.; Duvic, M.; Elder, J.T.; Gottlieb, A.B.; Koo, J.; Krueger, J.G.; Lebwohl, M.; Lowe, N.; et al. Two considerations for patients with psoriasis and their clinicians. J. Am. Acad. Dermatol. 2000, 43, 281–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pariser, D.M.; Bagel, J.; Gelfand, J.M.; Korman, N.J.; Ritchlin, C.T.; Strober, B.E.; Van Voorhees, A.S.; Young, M.; Rittenberg, S.; Lebwohl, M.G.; et al. National psoriasis foundation. national psoriasis foundation clinical consensus on disease severity. Arch. Dermatol. 2007, 143, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Rider, P.; Carmi, Y.; Cohen, I. Biologics for targeting inflammatory cytokines, clinical uses, and limitations. Int. J. Cell Biol. 2016, 2016, 9259646. [Google Scholar] [CrossRef] [Green Version]
- Raychaudhuri, S.P.; Raychaudhuri, S.K. Biologics: Target-specific treatment of systemic and cutaneous autoimmune diseases. Indian J. Dermatol. 2009, 54, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Feldman, S.R.; Goffe, B.; Rice, G.; Mitchell, M.; Kaur, M.; Robertson, D.; Sierka, D.; Bourret, J.A.; Evans, T.S.; Gottlieb, A. The challenge of managing psoriasis: Unmet medical needs and stakeholder perspectives. Am. Health Drug Benefits 2016, 9, 504–513. [Google Scholar]
- Rhodes, J.; Clay, C.; Phillips, M. The surface area of the hand and the palm for estimating percentage of total body surface area: Results of a meta-analysis. Br. J. Dermatol. 2013, 169, 76–84. [Google Scholar] [CrossRef]
- Weisman, S.; Pollack, C.R.; Gottschalk, R.W. Psoriasis disease severity measures: Comparing efficacy of treatments for severe psoriasis. J. Dermatol. Treat. 2003, 14, 158–165. [Google Scholar] [CrossRef]
- Feldman, S.R.; Krueger, G.G. Psoriasis assessment tools in clinical trials. Ann. Rheum. Dis. 2005, 64, ii65–ii68. [Google Scholar] [CrossRef]
- Salgado-Boquete, L.; Carrascosa, J.M.; Llamas-Velasco, M.; Ruiz-Villaverde, R.; de la Cueva, P.; Belinchón, I. A new classification of the severity of psoriasis: What’s moderate psoriasis? Life 2021, 11, 627. [Google Scholar] [CrossRef] [PubMed]
- Long, C.C.; Finlay, A.Y.; Averill, R.W. The rule of hand: 4 hand areas = 2 FTU = 1 g. Arch. Dermatol. 1992, 128, 1129–1130. [Google Scholar] [CrossRef] [PubMed]
- Langley, R.G.; Ellis, C.N. Evaluating psoriasis with psoriasis area and severity index, psoriasis global assessment, and lattice system physician’s global assessment. J. Am. Acad. Dermatol. 2004, 51, 563–569. [Google Scholar] [CrossRef]
- Kirsten, N.; Rustenbach, S.; von Kiedrowski, R.; Sorbe, C.; Reich, K.; Augustin, M. Which PASI outcome is most relevant to the patients in real-world care? Life 2021, 11, 1151. [Google Scholar] [CrossRef]
- Twiss, J.; Meads, D.M.; Preston, E.P.; Crawford, S.R.; McKenna, S.P. Can we rely on the dermatology life quality index as a measure of the impact of psoriasis or atopic dermatitis? J. Investig. Dermatol. 2012, 132, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langebruch, A.; Radtke, M.A.; Gutknecht, M.; Augustin, M. Does the dermatology life quaslity index (DLQI) underestimate the disease-specific burden of psoriasis patients? J. Eur. Acad. Dermatol. Venereol. 2019, 33, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Rencz, F.; Poór, A.K.; Péntek, M.; Holló, P.; Kárpáti, S.; Gulácsi, L.; Szegedi, A.; Remenyik, É.; Hidvégi, B.; Herszényi, K.; et al. A detailed analysis of ‘not relevant’ responses on the DLQI in psoriasis: Potential biases in treatment decisions. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belinchón Romero, I.; Dauden, E.; Ferrándiz Foraster, C.; González-Cantero, Á.; Carrascosa Carrillo, J.M. Therapeutic goals and treatment response evaluation in moderate to severe psoriasis: An expert’s opinion document. Ann. Med. 2021, 53, 1727–1736. [Google Scholar] [CrossRef]
- Smith, C.H.; Jabbar-Lopez, Z.K.; Yiu, Z.Z.; Bale, T.; Burden, A.D.; Coates, L.C.; Cruickshank, M.; Hadoke, T.; MacMahon, E.; Murphy, R.; et al. British association of dermatologists guidelines for biologic therapy for psoriasis 2017. Br. J. Dermatol. 2017, 177, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Mrowietz, U. Implementing treatment goals for successful long-term management of psoriasis. JEADV 2012, 26 (Suppl. S2), 12–20. [Google Scholar] [CrossRef]
- Wozel, G. Psoriasis treatment in difficult locations: Scalp, nails, and intertriginous areas. Clin. Dermatol. 2008, 26, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Van de Kerkhof, P.C.; Franssen, M.E. Psoriasis of the scalp. Diagnosis and management. Am. J. Clin. Dermatol. 2001, 2, 159–165. [Google Scholar] [CrossRef]
- Farley, E.; Masrour, S.; McKey, J.; Menter, A. Palmoplantar psoriasis: A phenotypical and clinical review with introduction of a new quality-of-life assessment tool. J. Am. Acad. Dermatol. 2009, 60, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Reich, A.; Szepietowski, J.C. Health-related quality of life in patients with nail disorders. Am. J. Clin. Dermatol. 2011, 12, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Sadlier, M.; De Vol, E.; Patel, M.; Lloyd, A.A.; Day, A.; Lally, A.; Kirby, B.; Menter, A. Genital psoriasis is associated with significant impairment in quality of life and sexual functioning. J. Am. Acad. Dermatol. 2015, 72, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Sarma, N. Evidence and suggested therapeutic approach in psoriasis of difficult-to-treat areas: Palmoplantar psoriasis, nail psoriasis, scalp psoriasis, and Intertriginous psoriasis. Indian J. Dermatol. 2017, 62, 113–122. [Google Scholar] [CrossRef]
- Egeberg, A.; See, K.; Garrelts, A.; Burge, R. Epidemiology of psoriasis in hard-to-treat body locations: Data from the Danish skin cohort. BMC Dermatol. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed]
- Callis Duffin, K.; Mason, M.A.; Gordon, K.; Harrison, R.W.; Crabtree, M.M.; Guana, A.; Germino, R.; Lebwohl, M. Characterization of patients with psoriasis in challenging-to-treat body areas in the Corrona Psoriasis Registry. Dermatology 2021, 237, 46–55. [Google Scholar] [CrossRef]
- Callis-Duffin, K.; Karki, C.; Mason, M.A.; Gordon, K.; Harrison, R.W.; Guana, A.; Gilloteau, I.; Herrra, V.; Lebwohl, M. Describing the clinical and patient reported outcomes of patients with scalp psoriasis enrolled in the Corrona Psoriasis Registry. J. Am. Acad. Dermatol. 2018, 79, AB105. [Google Scholar]
- Callis-Duffin, K.; Karki, C.; Mason, M.A.; Gordon, K.; Harrison, R.W.; Guana, A.; Gilloteau, I.; Herrra, V.; Lebwohl, M. The burden of nail psoriasis: A real-world analysis from the Corrona Psoriasis Registry. J. Am. Acad. Dermatol. 2018, 79, AB283. [Google Scholar]
- Duffin, K.C.; Herrera, V.; Mason, M.A.; Gordon, K.; Harrison, R.W.; Guana, A.; Gilloteau, I.; Karki, C.; Lebwohl, M. Impact of palmoplantar psoriasis on clinical and patient reported outcomes: Results from the Corrona Registry. J. Am. Acad. Dermatol. 2018, 79, AB159. [Google Scholar]
- Mosca, M.; Hong, J.; Hadeler, E.; Brownstone, N.; Bhutani, T.; Liao, W. Scalp psoriasis: A literature review of effective therapies and updated recommendations for practical management. Dermatol. Ther. 2021, 11, 769–797. [Google Scholar] [CrossRef]
- Arif, A.; Mahadi, I.D.R.; Yosi, A. Correlation between nail psoriasis severity index score with quality of life in nail psoriasis. Bali Med. J. 2021, 10, 256–260. [Google Scholar] [CrossRef]
- Timotijević, Z.S.; Trajković, G.; Jankovic, J.; Relić, M.; Đorić, D.; Vukićević, D.; Relić, G.; Rašić, D.; Filipović, M.; Janković, S. How frequently does palmoplantar psoriasis affect the palms and/or soles? A systematic review and meta-analysis. Adv. Dermatol. Allergol. 2019, 36, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.; Saraswat, A.; Kaur, I. Palmoplantar lesions in psoriasis: A study of 3065 patients. Acta Derm. Venereol. 2002, 82, 192–195. [Google Scholar] [CrossRef] [Green Version]
- Nast, A.; Smith, C.; Spuls, P.I.; Avila Valle, G.; Bata-Csörgö, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris–Part 1: Treatment and monitoring recommendations. JEADV 2020, 34, 2461–2498. [Google Scholar] [CrossRef]
- Mrowietz, U.; Steinz, K.; Gerdes, S. Psoriasis: To treat or to manage? Exp. Dermatol. 2014, 23, 705–709. [Google Scholar] [CrossRef]
- Merola, J.F.; Abrar Qureshi, M.; Husni, E. Underdiagnosed and undertreated psoriasis: Nuances of treating psoriasis affecting the scalp, face, intertriginous areas, genitals, hands, feet, and nails. Dermatol. Ther. 2018, 31, e12589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakuta, P.; Marcinkiewicz, K.; Bergler-Czop, B.; Brzezinska-Wcislo, L.; Slomian, A. Associations between site of skin lesions and depression, social anxiety, body-related emotions and feelings of stigmatization in psoriasis patients. Postepy Dermatol. Allergol. 2018, 35, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Dopytalska, K.; Sobolewski, P.; Blaszczak, A.; Szymanska, E.; Walecka, I. Psoriasis in special localizations. Reumatologia 2018, 56, 392–398. [Google Scholar] [CrossRef] [Green Version]
- Gordon, K.B.; Strober, B.; Lebwohl, M.; Augustin, M.; Blauvelt, A.; Poulin, Y.; Papp, K.A.; Sofen, H.; Puig, L.; Foley, P.; et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): Results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet 2018, 392, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.; Thaçi, D.; Reich, K.; Riedl, E.; Langley, R.G.; Krueger, J.G.; Gottlieb, A.B.; Nakagawa, H.; Bowman, E.P.; Mehta, A.; et al. Tildrakizumab (MK3222), an anti-interleukin-23p19 monoclonal antibody, improves psoriasis in a phase IIb randomized placebo-controlled trial. Br. J. Dermatol. 2015, 173, 930–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blauvelt, A.; Papp, K.A.; Griffiths, C.E.; Randazzo, B.; Wasfi, Y.; Shen, Y.K.; Li, S.; Kimball, A.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: Results from the phase III, double-blinded, placebo- and active comparator controlled VOYAGE 1 trial. J. Am. Acad. Dermatol. 2017, 76, 405–417. [Google Scholar] [PubMed] [Green Version]
- Elewski, B.E.; Puig, L.; Mordin, M.; Gilloteau, I.; Sherif, B.; Fox, T.; Gnanasakthy, A.; Papavassilis, C.; Strober, B.E. Psoriasis patients with psoriasis Area and Severity Index (PASI) 90 response achieve greater health-related quality-of-life improvements than those with PASI 75-89 response: Results from two phase 3 studies of secukinumab. J. Dermatol. Treat. 2017, 28, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Carretero, G.; Puig, L.; Carrascosa, J.M.; Ferrándiz, L.; Ruiz-Villaverde, R.; de la Cueva, P.; Belinchon, I.; Vilarrasa, E.; Del Rio, R.; Spanish Group of Psoriasis; et al. Redefining the therapeutic objective in psoriatic patients’ candidates for biological therapy. J. Dermatol. Treat. 2018, 29, 334–346. [Google Scholar] [CrossRef]
- Lista Protocoalelor Terapeutice Aprobate Prin ORDINUL MS/CNAS NR 1462/347/2022—Valabila cu IUNIE 2022. Available online: https://cnas.ro/wp-content/uploads/2022/06/iunie.pdf (accessed on 10 October 2022).
- Machado-Pinto, J.; Diniz Mdos, S.; Bavoso, N.C. Psoriasis: New comorbidities. An. Bras. Dermatol. 2016, 91, 8–16. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Guideline | Moderate to Severe Psoriasis Treatment Aim Definitions | Treatment Response and/or Failure Definitions, with Changes in Those Suffering from Moderate to Severe Psoriasis |
|---|---|---|
| European guideline of systemic therapy | Any psoriasis treatment should aim at eliminating all symptoms of skin inflammation.Necessary: minimum improvement and particular drug analysis times. | Throughout the phases of induction and maintenance:
|
| French guideline of systemic therapy | Factors when establishing treatment goals for systemic therapy:
| An adequate treatment response: PASI 75 (from the baseline), or PASI 50 with DLQI ≤ 5. |
| British guideline of systemic therapy | Treatment choice according to the patient and other factors:
|
|
| Spanish consensus of systemic therapy | The ideal outcome is to achieve: PASI 90 and a PGA ≤ 1, or as an alternative, a minimal, topical treatment controllable localized disease (PGA ≤ 2 and PASI < 5), DLQI ≤ 1, prolonged remissions without loss of efficacy, no worsening of comorbidities. Criteria for an appropriate response initially and in the long term (more than 6 months), 1 of: PASI 75, PASI < 5, PGA ≤ 1 and DLQI < 5. Criteria for the minimum efficacy required: PASI 50, PASI < 5. | Therapeutic failure during initiation of the treatment:
|
| Difficult-to-Treat Areas | % of Patients with Mild Psoriasis | % of Patients with Moderate Psoriasis | % of Patients with Severe Psoriasis |
|---|---|---|---|
| scalp | 48.1% | 57.8% | 66.1% |
| face | 27.6% | 41.8% | 53.3% |
| palms | 13.5% | 22.9% | 19.5% |
| nails | 25.6% | 31.1% | 42.4% |
| genitals | 12.5% | 18.1% | 27.2% |
| soles | 16.7% | 24.7% | 22.1% |
| Main Area | Additional Areas | Severity Assessment |
|---|---|---|
| trunk BSA less than < 10% severity 4 for erythema, induration and scaling PASI = 3.6 | scalp >70% severity 4 for erythema, induration and scaling | PASI = 8 → PSO moderate or PSSI = 48 → PSO severe |
| nails matrix and nail bed completely affected 10 nails | PASI = 6 → PSO moderate or NAPSI = 80 → PSO severe | |
| palmo-plantar both hands or both soles severity 4 for erythema, induration, scaling, fissuring | PASI = 8 → PSO moderate or ESIF = 24 → PSO severe |
| Severity Scores to Achieve | Quality of Life | |
|---|---|---|
| Treatment goals (assessed after 10–16 weeks and then every 8 weeks treatment goals | PASI 90 or PASI ≤ 2 PGA clear or almost clear | DLQI < 2 |
| minimum efficacy (lowest hurdle for treatment modification) | PASI 50 | DLQI < 5 or DLQI improvement ≥ 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolescu, A.C.; Ionescu, M.-A.; Constantin, M.M.; Ancuta, I.; Ionescu, S.; Niculet, E.; Tatu, A.L.; Zirpel, H.; Thaçi, D. Psoriasis Management Challenges Regarding Difficult-to-Treat Areas: Therapeutic Decision and Effectiveness. Life 2022, 12, 2050. https://doi.org/10.3390/life12122050
Nicolescu AC, Ionescu M-A, Constantin MM, Ancuta I, Ionescu S, Niculet E, Tatu AL, Zirpel H, Thaçi D. Psoriasis Management Challenges Regarding Difficult-to-Treat Areas: Therapeutic Decision and Effectiveness. Life. 2022; 12(12):2050. https://doi.org/10.3390/life12122050
Chicago/Turabian StyleNicolescu, Alin Codrut, Marius-Anton Ionescu, Maria Magdalena Constantin, Ioan Ancuta, Sinziana Ionescu, Elena Niculet, Alin Laurentiu Tatu, Henner Zirpel, and Diamant Thaçi. 2022. "Psoriasis Management Challenges Regarding Difficult-to-Treat Areas: Therapeutic Decision and Effectiveness" Life 12, no. 12: 2050. https://doi.org/10.3390/life12122050