
Predicting Early Loss of Lateral Spread Response before Decompression in Hemifacial Spasm Surgery


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Inclusion Criteria
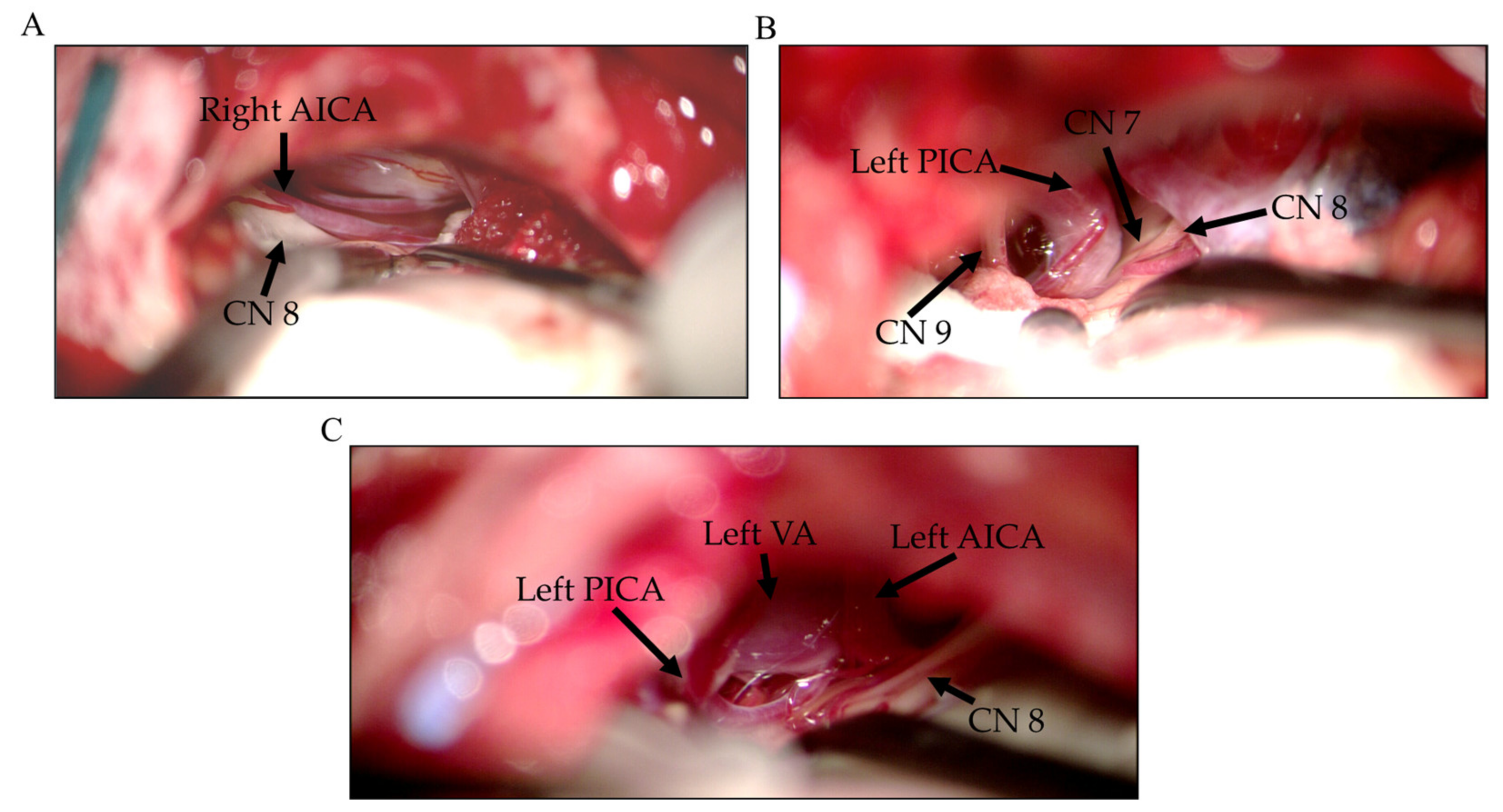
2.2. Surgery
2.3. Intraoperative Monitoring (IOM)
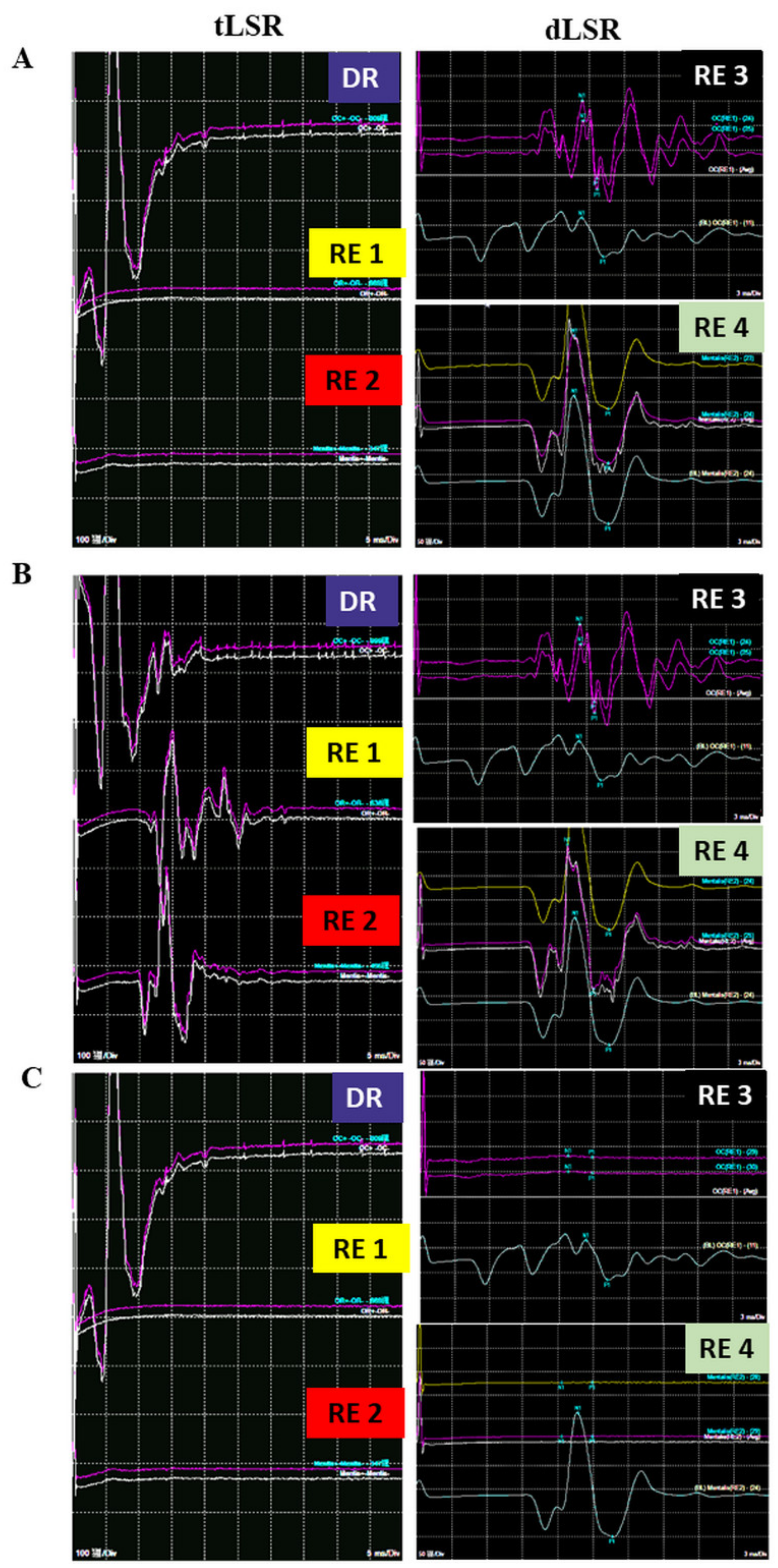
2.3.1. tLSR Measurement
2.3.2. dLSR Measurement
2.4. Outcome Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenstengel, C.; Matthes, M.; Baldauf, J.; Fleck, S.; Schroeder, H. Hemifacial spasm: Conservative and surgical treatment options. Dtsch. Arztebl. Int. 2012, 109, 667–673. [Google Scholar]
- Hughes, M.; Branstetter, B.; Taylor, C.; Fakhran, S.; Delfyett, W.; Frederickson, A.; Sekula, R. MRI Findings in Patients with a History of Failed Prior Microvascular Decompression for Hemifacial Spasm: How to Image and Where to Look. Am. J. Neuroradiol. 2014, 36, 768–773. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, V.K. Pathophysiology of hemifacial spasm: II. Lateral spread of the supraorbital nerve reflex. Neurology 1984, 34, 427. [Google Scholar] [CrossRef] [PubMed]
- Kameyama, S.; Masuda, H.; Shirozu, H.; Ito, Y.; Sonoda, M.; Kimura, J. Ephaptic transmission is the origin of the abnormal muscle response seen in hemifacial spasm. Clin. Neurophysiol. 2016, 127, 2240–2245. [Google Scholar] [CrossRef] [PubMed]
- Mooij, J.J.A.; Mustafa, M.K.; van Weerden, T.W. Hemifacial Spasm: Intraoperative Electromyographic Monitoring as a Guide for Microvascular Decompression. Neurosurgery 2001, 49, 1365–1371. [Google Scholar] [CrossRef]
- Kim, C.-H.; Kong, D.-S.; Lee, J.A.; Park, K. The Potential Value of the Disappearance of the Lateral Spread Response During Microvascular Decompression for Predicting the Clinical Outcome of Hemifacial Spasms: A Prospective Study. Neurosurgery 2010, 67, 1581–1588. [Google Scholar] [CrossRef]
- Yamashita, S.; Kawaguchi, T.; Fukuda, M.; Watanabè, M.; Tanaka, R.; Kameyama, S. Abnormal muscle response monitoring during microvascular decompression for hemifacial spasm. Acta Neurochir. 2005, 147, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Xu, W.; Dai, Y.; Lu, T.; Jin, W.; Liang, W. Early permanent disappearance of abnormal muscle response during microvascular decompression for hemifacial spasm: A retrospective clinical study. Neurosurg. Rev. 2016, 40, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Møller, A.R.; Jannetta, P.J. Monitoring facial EMG responses during microvascular decompression operations for hemifacial spasm. J. Neurosurg. 1987, 66, 681–685. [Google Scholar] [CrossRef]
- Haines, S.; Torres, F. Intraoperative monitoring of the facial nerve during decompressive surgery for hemifacial spasm. J. Neurosurg. 1991, 74, 254–257. [Google Scholar] [CrossRef]
- Wei, Y.; Yang, W.; Zhao, W.; Pu, C.; Li, N.; Cai, Y.; Shang, H. Microvascular decompression for hemifacial spasm: Can intraoperative lateral spread response monitoring improve surgical efficacy? J. Neurosurg. 2018, 128, 885–890. [Google Scholar] [CrossRef] [Green Version]
- Hirono, S.; Yamakami, I.; Sato, M.; Kado, K.; Fukuda, K.; Nakamura, T.; Higuchi, Y.; Saeki, N. Continuous intraoperative monitoring of abnormal muscle response in microvascular decompression for hemifacial spasm; a real-time navigator for complete relief. Neurosurg. Rev. 2013, 37, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zheng, X.; Ying, T.; Zhu, J.; Zhang, W.; Yang, X.; Li, S. Combined intraoperative monitoring of abnormal muscle response and Z-L response for hemifacial spasm with tandem compression type. Acta Neurochir. 2014, 156, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhao, H.; Ying, T.-T.; Tang, Y.-D.; Zhu, J.; Li, S.-T. The Effects of Dual Abnormal Muscle Response Monitoring on Microvascular Decompression in Patients with Hemifacial Spasm. World Neurosurg. 2017, 101, 93–98. [Google Scholar] [CrossRef]
- Xia, Y.F.; Zhou, W.P.; Zhang, Y.; Li, Y.Z.; Wang, X.H.; Li, S.T.; Zhao, H. How to Improve the Effect of Microvascular Decompression for Hemifacial Spasm: A Retrospective Study of 32 Cases with Unsuccessful First Time MVD. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2021. [Google Scholar] [CrossRef]
- Shin, J.C.; Kim, Y.C.; Park, C.I.; Chung, U.H. Intraoperative monitoring of microvascular decompression in hemifacial spasm. Yonsei Med. J. 1996, 37, 209–213. [Google Scholar] [CrossRef] [Green Version]
- Sekula, R.F.; Bhatia, S.; Frederickson, A.M.; Jannetta, P.J.; Quigley, M.R.; Small, G.A.; Breisinger, R. Utility of intraoperative electromyography in microvascular decompression for hemifacial spasm: A meta-analysis. Neurosurg. Focus 2009, 27, E10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, D.-S.; Park, K.; Shin, B.-G.; Lee, J.A.; Eum, D.-O. Prognostic value of the lateral spread response for intraoperative electromyography monitoring of the facial musculature during microvascular decompression for hemifacial spasm. J. Neurosurg. 2007, 106, 384–387. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.-R.; Chang, C.-N.; Hsu, J.-C. Intraoperative electrophysiological monitoring in microvascular decompression for hemifacial spasm. J. Clin. Neurosci. 2009, 16, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Neves, D.O.; Lefaucheur, J.-P.; de Andrade, D.C.; Hattou, M.; Ahdab, R.; Ayache, S.S.; Le Guerinel, C.; Keravel, Y. A reappraisal of the value of lateral spread response monitoring in the treatment of hemifacial spasm by microvascular decompression. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1375–1380. [Google Scholar] [CrossRef] [Green Version]
- Hatem, J.; Sindou, M.; Vial, C. Intraoperative monitoring of facial EMG responses during microvascular decompression for hemifacial spasm. Prognostic value for long-term outcome: A study in a 33-patient series. Br. J. Neurosurg. 2001, 15, 496–499. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Y.; Zhu, H.; Li, Y. Prognostic value of intra-operative abnormal muscle response monitoring during microvascular decompression for long-term outcome of hemifacial spasm. J. Clin. Neurosci. 2012, 19, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Von Eckardstein, K.L.; Link, M.J. The Significance of Intraoperative Electromyographic “Lateral Spread” in Predicting Outcome of Microvascular Decompression for Hemifacial Spasm. J. Neurol. Surg. Part B Skull Base 2012, 73, A387. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, B.J.; Shin, H.S.; Park, C.K.; Rhee, B.A.; Lim, Y.J. Prognostic ability of intraoperative electromyographic monitoring during microvascular decompression for hemifacial spasm to predict lateral spread response outcome. J. Neurosurg. 2017, 126, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Li, Z.-H.; Wang, J.-F.; Chen, Y.-H.; Wang, N.; Wang, Y. Prognostic Value of Abnormal Muscle Response during Microvascular Decompression for Hemifacial Spasm: A Meta-Analysis. World Neurosurg. 2020, 137, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Nugroho, S.W.; Perkasa, S.A.H.; Gunawan, K.; Manuhutu, Y.N.; Rahman, M.A.; Rizky, A. Predicting outcome of hemifacial spasm after microvascular decompression with intraoperative monitoring: A systematic review. Heliyon 2021, 7, e06115. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Kong, D.-S.; Lee, J.-A.; Park, K. Hemifacial spasm: Neurovascular compressive patterns and surgical significance. Acta Neurochir. 2008, 150, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Park, J.S. Hemifacial Spasm: A Comprehensive Guide, 1st ed.; Springer: Singapore, 2020; p. 154. [Google Scholar]
- Tan, E.K.; Chan, L.L. Young onset hemifacial spasm. Acta Neurol. Scand. 2006, 114, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Engh, J.A.; Horowitz, M.; Burkhart, L.; Chang, Y.-F.; Kassam, A. Repeat microvascular decompression for hemifacial spasm. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1574–1580. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Group A (n = 14) | Group B (n = 35) | p-Value | |
|---|---|---|---|
| Gender (M/F) | 3/11 | 18/17 | 0.0552 |
| Side (L/R) | 7/7 | 21/14 | 0.5228 |
| Mean age (years) | 47.8 ± 8.6 | 53.9 ± 10.6 | 0.0393 |
| Mean duration (years) (mean ± SD) | 5.7 ± 3.0 | 6.2 ± 4.4 | 0.9911 |
| No. of operation (1st/2nd) | 14/0 | 30/5 | 0.3032 |
| Offending vessels | |||
| AICA | 11 (78.57%) | 10 (28.57%) | 0.0205 |
| PICA | 1 (7.14%) | 8 (22.86%) | |
| VA involved | 1 (7.14%) | 9 (25.71%) | |
| AICA + PICA | 1 (7.14%) | 8 (22.86%) | |
| Indentation of the facial nerve | 1 | 2 | 1 |
| Post-Operative | Long-Term | |||
|---|---|---|---|---|
| Group A | Group B | Group A | Group B | |
| Cured | 12 | 24 | 14 | 29 |
| Uncured | 2 | 11 | 0 | 6 |
| p-value | 0.2969 | 0.1639 | ||
| Complications | ||
|---|---|---|
| Group A | Group B | |
| Delayed facial palsy | 0 | 2 |
| Tinnitus | 0 | 2 |
| Abducens palsy | 0 | 2 |
| Subdural hematoma | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, R.W.-Y.; Chiang, Y.-H.; Chen, Y.-Y.; Chen, Y.-C.; Lin, J.-H.; Tsou, Y.-S. Predicting Early Loss of Lateral Spread Response before Decompression in Hemifacial Spasm Surgery. Life 2022, 12, 40. https://doi.org/10.3390/life12010040
Chan RW-Y, Chiang Y-H, Chen Y-Y, Chen Y-C, Lin J-H, Tsou Y-S. Predicting Early Loss of Lateral Spread Response before Decompression in Hemifacial Spasm Surgery. Life. 2022; 12(1):40. https://doi.org/10.3390/life12010040
Chicago/Turabian StyleChan, Ryan Wing-Yuk, Yung-Hsiao Chiang, Yi-Yu Chen, Yi-Chen Chen, Jiann-Her Lin, and Yi-Syue Tsou. 2022. "Predicting Early Loss of Lateral Spread Response before Decompression in Hemifacial Spasm Surgery" Life 12, no. 1: 40. https://doi.org/10.3390/life12010040
APA StyleChan, R. W.-Y., Chiang, Y.-H., Chen, Y.-Y., Chen, Y.-C., Lin, J.-H., & Tsou, Y.-S. (2022). Predicting Early Loss of Lateral Spread Response before Decompression in Hemifacial Spasm Surgery. Life, 12(1), 40. https://doi.org/10.3390/life12010040