
Primary Extracranial Meningiomas of the Head and Neck

 ,
,  ,
, 

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Data Extraction
3. Results
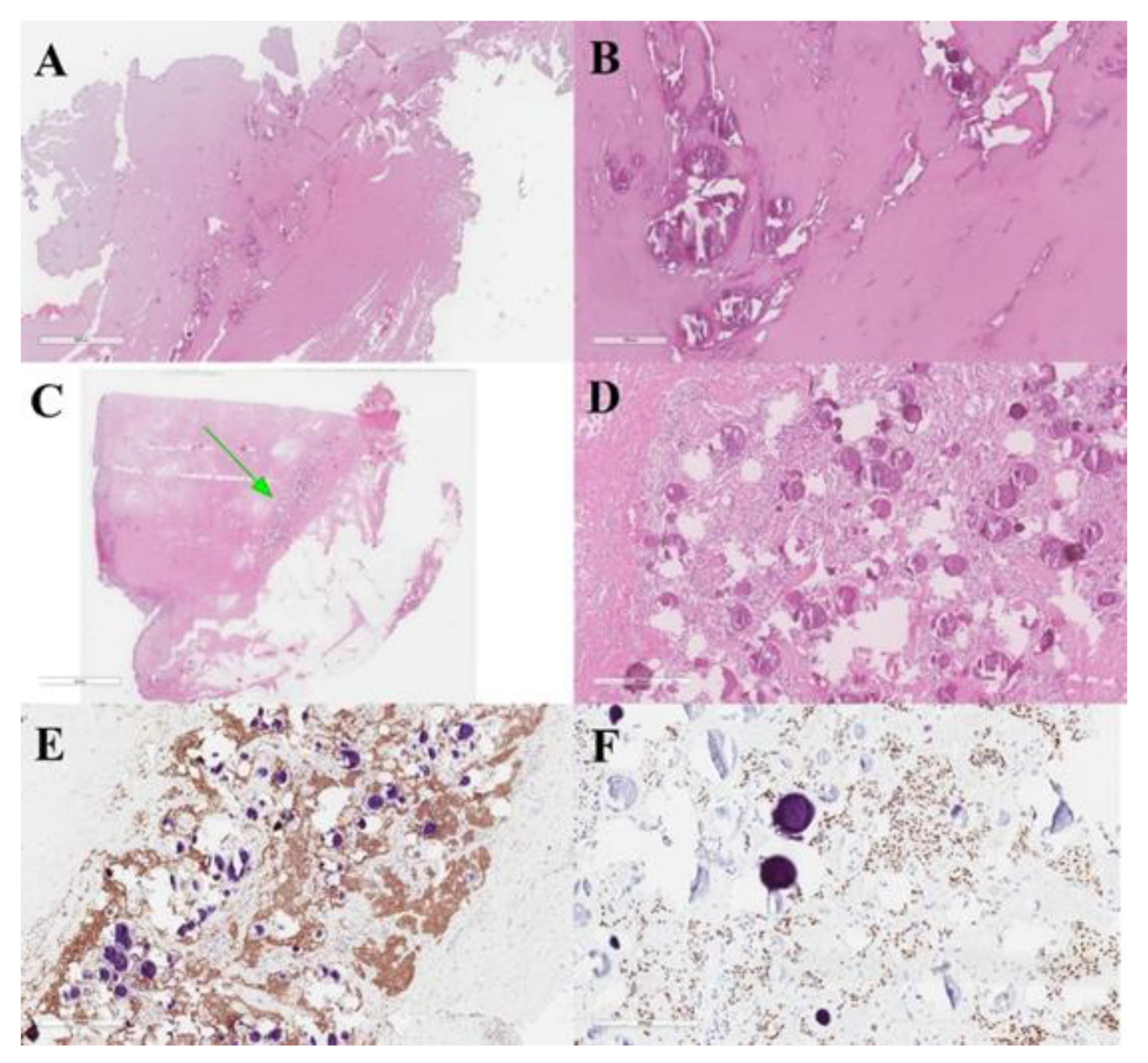
Case Illustration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rege, I.C.C.; Garcia, R.R.; Mendonça, E.F. Primary Extracranial Meningioma: A Rare Location. Head Neck Pathol. 2017, 11, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Simpson, M.; Sneddon, K. Extracranial meningioma of the oral cavity. Br. J. Oral Maxillofac. Surg. 1987, 25, 520–525. [Google Scholar] [CrossRef]
- Landini, G.; Kitano, M. Meningioma of the mandible. Cancer 1992, 69, 2917–2920. [Google Scholar] [CrossRef]
- Agaimy, A.; Buslei, R.; Coras, R.; Rubin, B.P.; Mentzel, T. Comparative study of soft tissue perineurioma and meningioma using a five-marker immunohistochemical panel. Histopathology 2014, 65, 60–70. [Google Scholar] [CrossRef]
- Koutlas, I.G.; Scheithauer, B.W.; Folpe, A.L. Intraoral Perineurioma, Soft Tissue Type: Report of Five Cases, Including 3 Intraosseous Examples, and Review of the Literature. Head Neck Pathol. 2010, 4, 113–120. [Google Scholar] [CrossRef][Green Version]
- Michel, R.G.; Woodard, B.H. Extracranial Meningioma. Ann. Otol. Rhinol. Laryngol. 1979, 88, 407–412. [Google Scholar] [CrossRef]
- Weinberger, J.M.; Birt, B.D.; Lewis, A.J.; Nedzelski, J.M. Primary meningioma of the nasopharynx: Case report and review of ectopic meningioma. J. Otolaryngol. 1985, 14, 317–322. [Google Scholar]
- Friedman, C.D.; Costantino, P.D.; Teitelbaum, B.; Berktold, R.E.; Sisson, G.A. Primary Extracranial Meningiomas of the Head and Neck. Laryngoscope 1990, 100, 41–48. [Google Scholar] [CrossRef]
- Miyamoto, T.; Mihara, M.; Hagari, Y.; Shimao, S. Primary Cutaneous Meningioma on the Scalp: Report of Two Siblings. J. Dermatol. 1995, 22, 611–619. [Google Scholar] [CrossRef]
- O’Reilly, R.C.; Kapadia, S.B.; Kamerer, D.B. Primary Extracranial Meningioma of the Temporal Bone. Otolaryngol. Head Neck Surg. 1998, 118, 690–694. [Google Scholar] [CrossRef]
- Jabor, M.A.; Amedee, R.G.; Gianoli, G.J. Primary meningioma of the fallopian canal. South Med. J. 2000, 93, 717–720. [Google Scholar] [CrossRef]
- Kishore, A.; Roy, D.; Irvine, B.W.H. Primary extracranial meningioma of the soft palate. J. Laryngol. Otol. 2000, 114, 149–150. [Google Scholar] [CrossRef]
- Sen, S.; Saha, S. A rare case of primary extracranial meningioma of the Paranasal Sinuses. Indian J. Otolaryngol. Head Neck Surg. 2001, 53, 318–320. [Google Scholar] [CrossRef]
- Hameed, A.; Gokden, M.; Hanna, E.Y. Fine-needle aspiration cytology of a primary ectopic meningioma. Diagn. Cytopathol. 2002, 26, 297–300. [Google Scholar] [CrossRef]
- Thompson, L.D.R.; Bouffard, J.-P.; Sandberg, G.D.; Mena, H. Primary Ear and Temporal Bone Meningiomas: A Clinicopathologic Study of 36 Cases with a Review of the Literature. Mod. Pathol. 2003, 16, 236–245. [Google Scholar] [CrossRef]
- Shaw, R.; Kissun, D.; Boyle, M.; Triantafyllou, A. Primary meningioma of the scalp as a late complication of skull fracture: Case report and literature review. Int. J. Oral Maxillofac. Surg. 2004, 33, 509–511. [Google Scholar] [CrossRef]
- Eshete, M.; Schneider, J. Extracranial meningioma of the scalp: Case report. Ethiop. Med. J. 2005, 43, 119–122. [Google Scholar]
- Jian, X.-C.; Wang, C.-X.; Jiang, C.-H. Surgical management of primary and secondary tumors in the pterygopalatine fossa. Otolaryngol. Neck Surg. 2005, 132, 90–94. [Google Scholar] [CrossRef]
- Ouazzani, A.; De Fontaine, S.; Berthe, J.-V. Extracranial meningioma and pregnancy: A rare diagnosis. J. Plast. Reconstr. Aesthetic Surg. 2007, 60, 622–625. [Google Scholar] [CrossRef]
- Rushing, E.J.; Bouffard, J.-P.; McCall, S.; Olsen, C.; Mena, H.; Sandberg, G.D.; Thompson, L.D.R. Primary Extracranial Meningiomas: An Analysis of 146 Cases. Head Neck Pathol. 2009, 3, 116–130. [Google Scholar] [CrossRef]
- Rutt, A.L.; Chen, X.; Sataloff, R.T. Jugular Fossa Meningioma: Presentation and Treatment Options. Ear Nose Throat J. 2009, 88, 1169–1172. [Google Scholar] [CrossRef] [PubMed]
- Alzarae, A.H.; Hussein, M.R.; Amri, D.; Mokarbesh, H.M. Primary Meningioma of the Nasal Septum. Appl. Immunohistochem. Mol. Morphol. 2010, 18, 296–298. [Google Scholar] [CrossRef] [PubMed]
- George, M.; Ikonomidis, C.; Pusztaszeri, M.; Monnier, P. Primary meningioma of the middle ear: Case report. J. Laryngol. Otol. 2009, 124, 572–574. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Deshmukh, S.D.; Rokade, V.V.; Pathak, G.S.; Nemade, S.V.; Ashturkar, A.V. Primary extra-cranial meningioma in the right submandibular region of an 18-year-old woman: A case report. J. Med. Case Rep. 2011, 5, 271. [Google Scholar] [CrossRef]
- Aiyer, R.G.; Prashanth, V.; Ambani, K.; Bhat, S.; Soni, G.B. Primary Extracranial Meningioma of Paranasal Sinuses. Indian J. Otolaryngol. Head Neck Surg. 2012, 65, 384–387. [Google Scholar] [CrossRef]
- Baek, B.J.; Shin, J.; Lee, C.K.; Lee, J.H.; Lee, K.H. Atypical primary meningioma in the nasal septum with malignant transformation and distant metastasis. BMC Cancer 2012, 12, 275. [Google Scholar] [CrossRef]
- Possanzini, P.; Pipolo, C.; Romagnoli, S.; Falleni, M.; Moneghini, L.; Braidotti, P.; Salvatori, P.; Paradisi, S.; Felisati, G. Primary extra-cranial meningioma of head and neck: Clinical, histopathological and immunohistochemical study of three cases. Acta Otorhinolaryngol. Ital. 2012, 32, 336–338. [Google Scholar]
- Zulkiflee, A.B.; Prepageran, N.; Rahmat, O.; Jayalaskhmi, P.; Sharizal, T. Hypoglossal nerve tumor: A rare primary extracranial meningioma of the neck. Ear Nose Throat J. 2012, 91, E26–E29. [Google Scholar]
- Maeng, J.W.; Kim, Y.H.; Seo, J.; Kim, S.W. Primary Extracranial Meningioma Presenting as a Cheek Mass. Clin. Exp. Otorhinolaryngol. 2013, 6, 266–268. [Google Scholar] [CrossRef]
- Ocque, R.; Khalbuss, W.E.; Monaco, S.E.; Michelow, P.M.; Pantanowitz, L. Cytopathology of Extracranial Ectopic and Metastatic Meningiomas. Acta Cytol. 2014, 58, 1–8. [Google Scholar] [CrossRef]
- Albsoul, N.; Rawashdeh, B.; Albsoul, A.; Abdullah, M.; Golestani, S.; Rawshdeh, A.; Mohammad, A.; Alzoubi, M. A rare case of extracranial meningioma in parapharyngeal space presented as a neck mass. Int. J. Surg. Case Rep. 2015, 11, 40–43. [Google Scholar] [CrossRef]
- Asil, K.; Aksoy, Y.E.; Yaldiz, C.; Kahyaoğlu, Z. Primary intraosseous meningiomas mimicking osteosarcoma: Case report. Turk. Neurosurg. 2014, 25, 174–176. [Google Scholar] [CrossRef]
- Janakiram, T.N.; Parekh, P.; Subramaniam, V. Primary Extracranial Meningioma: The Royal Pearl Experience. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 120–123. [Google Scholar] [CrossRef]
- Mondal, D.; Jana, M.; Sur, P.K.; Khan, E.M. Primary Sinonasal Meningioma in a Child. Ear Nose Throat J. 2015, 94, E7–E13. [Google Scholar] [CrossRef]
- Yang, X.-H.; Liu, L.; Zhang, P.; Hu, Y.-J. An Ectopic Meningioma in Nasal Floor. J. Craniofacial Surg. 2015, 26, e88–e90. [Google Scholar] [CrossRef]
- Ma, C.; Li, X.; Li, Y.; Qu, X. Primary Ectopic Meningioma of the Tongue: Case Report and Review of the Literature. J. Oral Maxillofac. Surg. 2016, 74, 2216–2228. [Google Scholar] [CrossRef]
- Lee, D.H.; Sim, H.S.; Hwang, J.H.; Kim, K.S.; Lee, S.Y. Extracranial Meningioma Presenting as an Eyebrow Mass. J. Craniofacial Surg. 2017, 28, e305–e307. [Google Scholar] [CrossRef]
- Radke, P.M.; Herreid, P.A.; Sires, B.S. Primary Extracranial Meningioma of the Lacrimal Sac Fossa. Ophthalmic Plast. Reconstr. Surg. 2018, 34, e147–e148. [Google Scholar] [CrossRef]
- Petrulionis, M.; Valeviciene, N.; Paulauskiene, I.; Bruzaite, J. Primary extracranial meningioma of the sinonasal tract. Acta Radiol. 2005, 46, 415–418. [Google Scholar] [CrossRef]
- Jones, A.C.; Freedman, P.D. Primary extracranial meningioma of the mandible: A report of 2 cases and a review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 91, 338–341. [Google Scholar] [CrossRef]
- Serry, P.; Rombaux, P.; Ledeghen, S.; Collet, S.; Eloy, P.; Hamoir, M.; Bertrand, B. Extracranial sinonasal tract meningioma: A case report. Acta Oto-Rhino-Laryngol. Belg. 2004, 58, 151–155. [Google Scholar]
- Hoye, S.J.; Hoar, C.S.; Murray, J.E. Extracranial meningioma presenting as a tumor of the neck. Am. J. Surg. 1960, 100, 486–489. [Google Scholar] [CrossRef]
- Burger, P.C.; Scheithauer, B.W. Tumors of meningothelial cells. In Tumors of the Central Nervous System, 3rd ed.; Armed Forces institute of Pathology: Washington, DC, USA, 1994; pp. 259–286. [Google Scholar]
- Dominguez-Malagon, H.; Ordòñez, N.G. Malignant Meningioma of the Parapharyngeal Space: A Case Report. Ultrastruct. Pathol. 1996, 20, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Huszar, M.; Fanburg, J.C.; Dickersin, G.R.; Kirshner, J.J.; Rosenberg, A.E. Retroperitoneal Malignant Meningioma. Am. J. Surg. Pathol. 1996, 20, 492–499. [Google Scholar] [CrossRef]
- Fraioli, M.F.; Marciani, M.G.; Umana, G.E.; Fraioli, B. Anterior Microsurgical Approach to Ventral Lower Cervical Spine Meningiomas: Indications, Surgical Technique and Long Term Outcome. Technol. Cancer Res. Treat. 2015, 14, 505–510. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Patients (n) | Age/Sex | Localization | Histology and Grading | Treatment | Recurrence | Outcome |
|---|---|---|---|---|---|---|---|
| Michel et al., 1979 [6] | 1 | 64F | Neck at parotid (associated with a synchronous intracranial syncytial meningioma of the frontal lobe) | Fibrous meningioma | Resection of the intracranial tumor only and biopsy of the neck tumor | No recurrence and stability of the neck tumor | Transient right arm weakness |
| Weinberger et al., 1985 [7] | 1 | Not available | Nasopharynx | Meningioma | Transpalatal flap | Not available | Not available |
| Friedman et al., 1990 [8] | 5 | 4M, 1F, 17–53 years | 2 infratemporal, 2 parapharyngeal, 1 nasal cavity | 1 syncytial, 4 transitional. (1 final diagnosis of nf ii associated with transitional meningioma in the 17-year-old male patient) | 2 transmandibular, 2 infratemporal, 1 facial degloving | 1 recurrence at less than 1 year, 1 recurrence at 3 years | Complete recovery |
| Miyamoto et al., 1995 [9] | 2 | 15F, 13M | 2 occipital scalp | 1 meningothelial, 1 fibroblastic | Surgical resection | No recurrence | Complete recovery |
| O’Reilly et al., 1998 [10] | 1 | 59M | Mesotympanum | Meningioma | Mastoidectomy | No recurrence at 6 months | Complete recovery |
| Jabor et al., 2000 [11] | 1 | 7F | Facial nerve in the fallopian canal | Meningioma | Not available | Not available | Not available |
| Kishore et al., 2000 [12] | 1 | 44F | Soft palate | Hyalinized and vascular meningioma | Excisional biopsy | No recurrence | Complete recovery |
| Sen and Saha, 2001 [13] | 1 | 8F | Right maxillary antrum, right nasal cavity, nasopharynx | Psammomatous | Surgical resection | No recurrence | Complete recovery |
| Hameed et al., 2002 [14] | 1 | 22F | Sublingual | Meningioma | Surgical resection | Not reported | Not reported |
| Thompson et al., 2003 [15] | 36 | 24F, 12M, 10–80 years | Ear and temporal bone | Meningothelial (n = 33), psammomatous (n = 2), and atypical (n = 1) | Surgical resection | 10 patients developed a recurrencefrom 5 months to 2 years later | Five patients died with recurrent disease (mean, 3.5 years), and the remaining 30 patients lived (n 25, mean: 19.0 years) or died (n 5, mean: 9.5 years) ofunrelated causes without evidence of disease |
| Shaw et al., 2004 [16] | 1 | 29M | Occipital scalp | Meningothelial meningioma | Surgical resection | No recurrence at 12 months | Complete recovery |
| Eshete et al., 2005 [17] | 1 | 70M | Parietal scalp | Meningothelial meningioma | Surgical resection | No recurrence | Not available |
| Jian et al., 2005 [18] | 1 | 19F | Pterygopalatine fossa | Meningioma | Surgical resection | No recurrence | Not reported |
| Ouazzani et al., 2007 [19] | 1 | 27F | Parietal scalp | Lymphoplasmacyte-rich meningioma | Surgical resection | No recurrence | Complete recovery |
| Rushing et al., 2009 [20] | 146 | 74F, 72M; 0.3–88 years | Scalp skin (40.4%), ear and temporal bone (26%), and sinonasal tract (24%). | Meningothelial (77.4%), followed by atypical (7.5%), psammomatous (4.1%), and anaplastic (2.7%) | Surgical resection | Recurrences were noted in 26 (23.6%) patients | Recurrent disease was persistent in 15 patients (mean, 7.7 years): 13 patients died with disease and two lived; the remaining patients were disease-free (alive 60, mean 19.0 years, dead 35, mean 9.6 years) |
| Rutt et al., 2009 [21] | 1 | 45M | Jugular fossa | Meningioma | Surgical resection | No recurrence at 1 year | Complete recovery |
| Alzarae et al., 2010 [22] | 1 | 60M | Nasal septum | Meningioma | Surgical resection | No recurrence at 4 years | Complete recovery |
| George et al., 2010 [23] | 1 | 35F | Middle-ear mass | Meningothelial meningioma | Surgical resection, tympanoplasty | No recurrence at 3 months | Complete recovery |
| Deshmukh et al., 2011 [24] | 1 | 18F | Right submandibular | Meningothelial meningioma | Surgical resection | No recurrence at 2 years | Complete recovery |
| Aiyer et al., 2012 [25] | 3 | 13F, 45F, 23F | Paranasal sinuses | Meningioma, meningioma, fibroblastic meningioma | Frontoethmoidectomy, left lateral rhinotomy approach | No recurrence at 1 year, 8 months, 6 months | Complete recovery |
| Baek et al., 2012 [26] | 1 | 44M | Nasal cavity | Meningioma WHO III | Surgical resection | Recurrence 2 years after surgery, treated with local external radiotherapy (6840 cgy in 38 fractions); after 2 more months, the patient developed malignant chest meningiomas (WHO III), surgically removed, and then developed multiple cutaneous tumors addressed to palliative treatment | Died 3 months after the last surgery |
| Possanzini et al., 2012 [27] | 3 | 38F, 69F, 34F | Temporal muscle, parapharyngeal, nasal mass | Epithelioid, s-100 positive, negative for gliofibrillary protein, cd31, cytokeratin Pool, cd34, smooth muscle actin, chromogranin a, Synaptophysin and melanocytic antigen. Immunoreactive Ki-67 cells were less than 5% | Surgical resection | Disease-free at 3 years | Complete recovery |
| Zulkiflee et al., 2012 [28] | 1 | 54M | Bifurcation of the left common carotid artery | Meningioma of the hypoglossal nerve | Transcervical excision | No recurrence at 2 years | Complete recovery |
| Maeng et al., 2013 [29] | 1 | 66F | Right cheek | Meningothelial meningioma | Lateral rhinotomy | No recurrence at 18 months | Complete recovery |
| Ocque et al., 2014 [30] | 8 | 26–64/3M–5F | 1 ear, 2 orbit,1 neck, 2 sphenoid sinus, 1 sella tuberculum, 1 parapharyngeal | Meningioma | Surgical resection | Not reported | Not reported |
| Albsoul et al., 2015 [31] | 1 | 55F | Neck | Meningothelial meningioma | Right cervical exploration for excisional biopsy and, because of the encasement of the right internal jugular vein, partial excision of the mass. | Stable after 8-month follow-up | Stable |
| Asil et al., 2015 [32] | 1 | 64M | Right frontotemporal | Intradiploic meningioma | Surgical resection | No recurrence at 2 months | No deficits |
| Janakiram et al., 2015 [33] | 2 | 40M, 36M | Nasal cavity, frontal sinus | Meningothelial pattern. Psammoma bodies were seen in between. There was no nuclear atypia or mitotic activity. Immunohistochemistry was positive for epithelial membrane antigen (ema) | Endoscopic endonasal approach | No recurrence at 2 years | Complete recovery |
| Mondal et al., 2015 [34] | 1 | 2M | Mass in the ethmoid sinus | Meningioma | Resection | No recurrence at 3 months | Complete recovery |
| Yang et al., 2015 [35] | 1 | 16M | Nasal floor | Meningioma | Surgical resection | No recurrence at 6 months | Complete recovery at 1 week |
| Ma et al., 2016 [36] | 1 | 18M | Left side of the tongue | Atypical meningioma | Lip-split mandibulotomy approach | No recurrence at 21 months | Progressive recovery and good functional speech and swallowing |
| Lee et al., 2017 [37] | 1 | 77F | Left eyebrow | Meningothelial meningioma | Trans-eyebrow removal | No recurrence at 10 months | Not reported |
| Rege et al., 2017 [1] | 1 | 35M | Right retromolar | Meningioma, antibodies against ema, vimentin, and Cd34 were positive | Partial resection of the mandible and reconstruction with autogenous iliac tricortical bone | No recurrence at 5 years | Complete recovery |
| Radke et al., 2018 [38] | 1 | 54F | Nasolacrimal sac/fossa | Epithelioid meningioma | Dacryocystorhinostomy with exploration | No recurrence at 3 months | Tearing persisted, conjunctivodacryocystorhinostomy was planned after 1 year to ensure the tumor did not recur |
| Umana et al., 2021 | 1 | 45M | Occipital scalp | Psammomatous meningioma | Surgical resection | No recurrence at 6 months | Complete recovery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umana, G.E.; Scalia, G.; Vats, A.; Pompili, G.; Barone, F.; Passanisi, M.; Graziano, F.; Maugeri, R.; Tranchina, M.G.; Cosentino, S.; et al. Primary Extracranial Meningiomas of the Head and Neck. Life 2021, 11, 942. https://doi.org/10.3390/life11090942
Umana GE, Scalia G, Vats A, Pompili G, Barone F, Passanisi M, Graziano F, Maugeri R, Tranchina MG, Cosentino S, et al. Primary Extracranial Meningiomas of the Head and Neck. Life. 2021; 11(9):942. https://doi.org/10.3390/life11090942
Chicago/Turabian StyleUmana, Giuseppe Emmanuele, Gianluca Scalia, Atul Vats, Gianluca Pompili, Fabio Barone, Maurizio Passanisi, Francesca Graziano, Rosario Maugeri, Maria Grazia Tranchina, Sebastiano Cosentino, and et al. 2021. "Primary Extracranial Meningiomas of the Head and Neck" Life 11, no. 9: 942. https://doi.org/10.3390/life11090942
APA StyleUmana, G. E., Scalia, G., Vats, A., Pompili, G., Barone, F., Passanisi, M., Graziano, F., Maugeri, R., Tranchina, M. G., Cosentino, S., Ippolito, M., Tomasi, S. O., Raudino, G., Chaurasia, B., Iacopino, D. G., Nicoletti, G. F., Cicero, S., Strigari, L., & Perrotta, R. E. (2021). Primary Extracranial Meningiomas of the Head and Neck. Life, 11(9), 942. https://doi.org/10.3390/life11090942